
Abstract
Background
Work-related stress negatively impacts employee wellbeing. Stress-management interventions that reduce workplace stress can be challenging. Immersive technologies, such as virtual reality (VR), may provide an alternative.
Aims
This systematic review aimed to evaluate feasibility, acceptability, and effectiveness of immersive technologies to promote workplace wellbeing (PROSPERO 268460).
Methods
Databases MEDLINE, Web of Science, PsycINFO and Embase were searched until 22nd July 2021. Studies were included if they tested a workforce or were designed for a workplace. Effective Public Health Practice Project quality assessment tool (EPHPP) was used for quality ratings.
Results
There were 17 studies (N = 1270), published 2011–2021. Over half were conducted in Europe. Eight studies were controlled trials. Most studies involved brief, single sessions of immersive VR and provided evidence of feasibility, acceptability, and effectiveness when measuring wellbeing-related variables such as stress, relaxation, and restoration. VR environments included relaxation tasks such as meditation or breathing exercises, and nature-based stimuli, such as forests, beaches, and water. Studies tested office workers, healthcare professionals, social workers, teachers, and military personnel. EPHPP ratings were “strong” (N = 1), “moderate” (N = 13), and “weak” (N = 3).
Conclusions
VR relaxation appears helpful for workplaces. However, limited longer-term data, controlled trials, and naturalistic studies mean conclusions must be drawn cautiously.
Introduction
Work-related stress is a leading cause of common mental health problems, such as anxiety, depression, and burnout, which impacts one in six working adults (Harvey et al., Citation2017; Seymour, Citation2010). It can also result in serious physical health consequences, such as cancer, diabetes, and cardiovascular disease (Wiegner et al., Citation2015). Organisations suffer the impact of work stress with 17.9 million workdays lost in 2019 in Great Britain (HSE., Citation2020b), costing the economy £5 billion (HSE, Citation2020a), with similar costs incurred worldwide (WHO., Citation2017). “Presenteeism”, in which poor mental health impacts employees’ workplace productivity, is considered to be similarly damaging to organisations as absenteeism (Kirkham et al., Citation2015). COVID-19 has further amplified pressure faced by many workers, with increased staff absences and limited face-to-face contact, which has exacerbated rates of stress-related illness (Horesh & Brown, Citation2020; Mezzina et al., Citation2020).
Stress management interventions are increasingly being implemented in workplaces and can be used as an effective breaktime activity during the working day (Tetrick & Winslow, Citation2015). These interventions can either target employees currently experiencing stress or take a preventative approach by targeting all employees (Quick & Tetrick, Citation2011). Interventions, such as psychoeducational stress management workshops, yoga, mindfulness, and deep breathing techniques, have increased positive wellbeing and relaxation, and reduced physiological symptoms, such as high blood pressure and heart rate (Balaji et al., Citation2012; Edwards & Burnard, Citation2003; Li et al., Citation2020). Short daily mindfulness sessions can reduce stress and improve sleep quality and job satisfaction (Klatt et al., Citation2009; Michel et al., Citation2014; Wolever et al., Citation2012). However, many of these interventions can be incompatible with fast-paced working environments, or workers can find them difficult to engage with (Nahar & Gurav, Citation2018), so there is need for novel workplace stress management interventions.
Immersive technologies, such as virtual reality (VR), multi-sensory rooms, cave automated virtual environments, spatialised audio environments, and role-playing games, employ virtual, immersive, and interactive elements to promote workplace wellbeing and optimise workplace conditions (Barton et al., Citation2020; Michalos et al., Citation2018; Rajguru et al., Citation2020; Riches & Smith, Citation2022). VR-based relaxation is a common immersive technology for stress reduction, typically using a head-mounted display (HMD), with immersive, interactive three-dimensional images of relaxing virtual environments (Slater et al., Citation1994; Villani et al., Citation2007). VR relaxation has been found to significantly reduce stress in clinical and non-clinical populations (Gorini & Riva, Citation2008; Riches et al., Citation2021; Veling et al., Citation2021); while, more generally, VR and other immersive technologies have been used to reduce pain (Nordgård & Låg, Citation2021), anxiety, and improve mood (Yu et al., Citation2018). Such immersive technologies have potential to be cost- and time-efficient tools that are engaging, promote wellbeing, and offer brief respite from the workplace without workers needing to physically leave their working location (Liberatore & Wagner, Citation2021; Riches et al., Citation2021). A recent scoping review concluded VR may have potential as a stress management tool in workplaces (Naylor et al., Citation2020); however, there is no systematic review assessing broader applications of VR and other immersive technologies to promote employee wellbeing and optimise workplace conditions to mitigate against work-related stress. This systematic review aims to narratively synthesise evidence of feasibility, acceptability, and effectiveness of VR and immersive technologies to promote workplace wellbeing.
Methods
This review is registered on the PROSPERO database (268460).
Search strategy
This review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) (Moher et al., Citation2009). A systematic search of published articles on MEDLINE, Web of Science, PsycINFO and Embase databases was carried out on 22nd July 2021. Search terms focused on the concepts of virtual reality and immersive technologies, workforces and workplaces, breaktimes and relaxation, and wellbeing. Truncations were used to search the roots of words and alternative endings. See for the full list of search terms and search strategy. Database searches targeted keywords, title, and abstract information and were restricted to English language publications. Categories of “virtual reality”, “occupations”, “leisure time” and “wellbeing” were ‘exploded’ for MEDLINE, PsychInfo, and Embase, and results were combined with results generated from search terms. Searches and screening using Endnote were carried out by two reviewers (LT, PJ), under the supervision of another researcher (SR). This screening included abstract, article title, and full-text screening. Studies screened and included in this study were also found through other sources, which included reference lists of other publications and independent searching. This search strategy included an initial pilot phase that was carried out by the same research team before the formal search was conducted.
Table 1. Full list of search terms and Boolean operators.
Studies were included if they were published in a peer-reviewed journal; written in English; used an experimental design; presented original data; N ≥ 5; tested virtual, immersive, or interactive environments that promote workplace wellbeing; and tested members of a workforce, or tested an intervention designed for a workforce, or tested an intervention in a workplace. Studies using mixed samples, e.g., participants who were employed, unemployed, or students, were included in the review if the primary study aim was investigating workplace wellbeing. Studies were excluded if they were conference proceedings, abstracts, books, book sections, grey literature, or dissertations; or if the immersive technology was used for staff training or for employees to carry out their work duties. Non-peer-reviewed journal publications were excluded to ensure that the review was methodologically robust.
Two researchers (SR, LT) led on the narrative synthesis, in collaboration with the wider research team. A structure of feasibility, acceptability, and effectiveness was used as a framework for the narrative synthesis because investigation of these issues was the main aim of the review. The review defined ‘feasibility’ as whether interventions were practical and delivered as intended; ‘acceptability’ as whether participants found the intervention acceptable and that there were no adverse experiences; and ‘effectiveness’ as whether the intervention improved wellbeing outcomes.
Quality assessment
The Effective Public Health Practice Project quality assessment tool for quantitative studies (EPHPP) (EPHPP, Citation2010) was used for quality ratings. EPHPP rates studies ‘weak’, ‘moderate’ or ‘strong’ on six methodological domains: selection bias, study design, confounders, blinding, data collection and withdrawals. Studies are given a Global Rating of ‘weak’ for two or more weak methodological domains, ‘moderate’ for only one weak methodological domain, and ‘strong’ for no weak methodological domains. The tool reclassifies randomised controlled trials (RCTs) as controlled clinical trials (CCTs) if no method of randomisation is reported.
The EPHPP was selected for this review because it can provide consistent quality ratings for a range of study designs. One researcher (LT) conducted quality ratings for all studies. A second researcher (PJ) rated a third of studies. Quality ratings were regularly discussed with another researcher (SR) who oversaw quality ratings. The research team met regularly to discuss any differences in quality ratings between researchers and studies were re-evaluated until consensus was reached.
Results
Study characteristics
In total, 10,563 articles were identified (Web of Science = 5,108; Embase = 3,106; MEDLINE = 1,942; PsychINFO = 394; other sources = 13). Thirty-nine full texts were retrieved and assessed for eligibility and 17 studies, published between 2011 and 2021, met inclusion criteria and were included in this review. See for PRISMA flowchart and for study characteristics. Nine studies were conducted in Europe (Germany, N = 3; Finland, N = 1; Ireland, N = 1; Italy, N = 1; The Netherlands, N = 1; Spain, N = 1; United Kingdom, N = 1), four in North America (United States, N = 3; Canada, N = 1), three in Asia (China, N = 2; South Korea, N = 1), and one in Australia (Australia, N = 1). Studies used VR HMDs (N = 13), immersive 2D audio-visual interventions (N = 3), or multi-sensory rooms (N = 1).
Figure 1. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of studies of virtual reality and immersive technologies to promote workplace wellbeing.
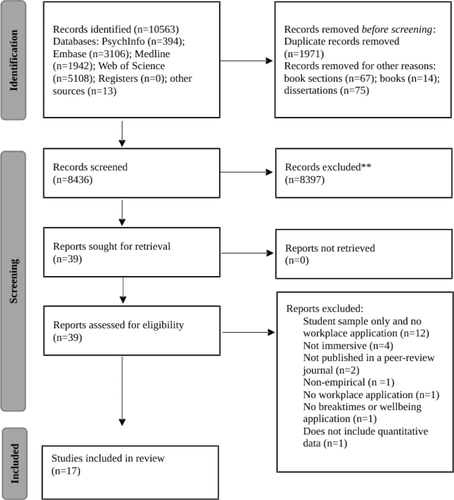
Table 2. Characteristics of studies of virtual reality and immersive technologies to promote workplace wellbeing.
In total, 1,270 people participated in the studies, with 859 experiencing an immersive technology intervention. One study did not record the number of participants experiencing an experimental intervention (Karacan et al., Citation2021). Studies ranged from having eight to 219 participants, with five studies including 100 or more participants (Gaggioli et al., Citation2014; Karacan et al., Citation2021; Maarsingh et al., Citation2019; Mattila et al., Citation2020; Putrino et al., Citation2020). Thirteen studies included part-time or full-time employees, of which three were conducted in employees’ workplaces (Karacan et al., Citation2021; Mattila et al., Citation2020; Palanica et al., Citation2019). Three studies included samples of healthcare professionals (Cikajlo et al., Citation2017; Gaggioli et al., Citation2014; Putrino et al., Citation2020), with one of them also including patients (Cikajlo et al., Citation2017) and one also including teachers (Gaggioli et al., Citation2014). Other studies included a mixed sample of social workers and students (Wang et al., Citation2019), university staff and students (Abdalrahman & Galbrun, Citation2020), employees of a large, German logistics company (Karacan et al., Citation2021), employees of a marketing and research company in the health sector (Palanica et al., Citation2019), and military personnel (Stetz et al., Citation2011). Five studies provided limited information about participant occupations; these participants were either employees from local companies (Blum et al., Citation2019; Maarsingh et al., Citation2019), mixed samples of employees and students (Mattila et al., Citation2020; Rockstroh et al., Citation2019), or students, employees, and unemployed participants (Chung et al., Citation2018). Another four studies included student or general population samples but explicitly stated a workplace application to the intervention (Anderson et al., Citation2017; Ma & Shu, Citation2018; Naylor et al., Citation2019; Vaquero-Blasco et al., Citation2021).
Fourteen studies included a single session, one included three sessions (Stetz et al., Citation2011), and two included eight sessions (Cikajlo et al., Citation2017; Gaggioli et al., Citation2014). Session length ranged from four minutes to one hour. Twelve studies used sessions of under 20 minutes. One study reported follow-up data, after an eight-session intervention (Gaggioli et al., Citation2014). Numerous psychological measures were used across studies. In several studies, stress, anxiety, and mood were measured with self-report measures, such as Perceived Stress Scale (PSS), Profile of Mood States (POMS), and State-Trait Anxiety Inventory (STAI). One study measured creativity with an Alternative Uses Test (AUT) (Palanica et al., Citation2019). Some studies employed physiological measures, such as heart rate variability (HRV) and electroencephalogram (EEG) to assess stress pre- and post-intervention sessions.
There were 13 head-mounted display VR studies. Twelve used immersive nature-based VR with ambient music or nature sounds, and one used a VR graphical ‘void of colourful lights and sounds’ as experimental stimuli (Naylor et al., Citation2019). Seven of the 12 nature-based studies involved participants viewing 360-degree high-definition video footage of real-life geographical locations, such as Irish countryside, Australian coastlines, Aurora Borealis, African safari with wild animals for office workers in the logistic sector, and waterfalls and pools in enclosed forests in Beijing. The other five studies used computer-programmed natural environments to immerse participants in interactive virtual scenes, such as beaches at sunset, tropical islands, or mountain tops with panoramic views. Four of the 12 nature-based studies incorporated elements such as fireworks (Chung et al., Citation2018), urban cityscapes (Palanica et al., Citation2019), fireplaces (Cikajlo et al., Citation2017), and helicopter rides (Karacan et al., Citation2021). Nine studies included specific relaxation tasks that were carried out while participants were exposed to the natural imagery. Four studies used a biofeedback task which involved participants trying to control physiological biomarkers of stress, such as HRV, that were being fed back to them in real-time (Blum et al., Citation2019; Gaggioli et al., Citation2014; Maarsingh et al., Citation2019; Rockstroh et al., Citation2019); and five studies incorporated guided meditation or breathing exercises with a real-life facilitator, audio-guided instruction, or a mixture of audio-guide and real-life facilitation.
Five studies measured perceived stress or stress-related mindset as the primary outcome (Gaggioli et al., Citation2014; Maarsingh et al., Citation2019; Rockstroh et al., Citation2019; Vaquero-Blasco et al., Citation2021; Wang et al., Citation2019), three measured relaxation (Anderson et al., Citation2017; Blum et al., Citation2019; Naylor et al., Citation2019), three measured restoration (Chung et al., Citation2018; Karacan et al., Citation2021; Mattila et al., Citation2020), one measured life satisfaction (Cikajlo et al., Citation2017), and one measured creativity (Palanica et al., Citation2019). HMDs used were Oculus Rift (N = 5), HTC Vive (N = 2), Samsung GearVR (N = 2), LG 360 VR glasses (N = 1), VUZIX Wrap 1200VR (N = 1), and Oculus Quest (N = 1). One study did not report the HMD brand but described the HMD as “second-generation VR glasses of the illusion mirror type” (Wang et al., Citation2019).
There were four studies that used other immersive technologies. Two displayed images of an office on a two-dimensional screen while a sample of students (Ma & Shu, Citation2018) or university staff and students (Abdalrahman & Galbrun, Citation2020) listened to audio playback of nature sounds on headphones (Abdalrahman & Galbrun, Citation2020; Ma & Shu, Citation2018). One of these studies included audio of air conditioner sound effects and office conversations with nature sounds (Ma & Shu, Citation2018). A study with medical surgeons as participants used a computer-generated tropical “Dream Island” scene on a cinema screen, with audio facilitation of relaxation techniques, to test the calming effect of the scene before participants were instructed to undertake a stressful VR-based task, such as an emergency surgery simulation (Stetz et al., Citation2011). In another study, frontline healthcare worker participants explored an immersive multi-sensory “Recharge” room with high-definition projections of natural landscapes, voice-activated colour lighting, and ambient music (Putrino et al., Citation2020). Three studies assessed stress, and one measured sound perception and preferences in offices (Abdalrahman & Galbrun, Citation2020) as a primary outcome.
Feasibility, acceptability, and effectiveness
Head-mounted display virtual reality studies
Out of 13 studies, 10 indicated the feasibility of HMD VR as a tool to support wellbeing in the workplace. Seven studies concluded that VR is a practical, intuitive, and convenient tool for those lacking access to outdoor space, such as those working in isolated and confined environments (Anderson et al., Citation2017) or offices (Blum et al., Citation2019; Chung et al., Citation2018; Cikajlo et al., Citation2017; Karacan et al., Citation2021; Mattila et al., Citation2020; Naylor et al., Citation2019; Vaquero-Blasco et al., Citation2021). Seven studies argued that VR is a time- and cost-efficient tool to support wellbeing in the workplace, which is becoming more affordable due to technological developments (Anderson et al., Citation2017; Chung et al., Citation2018; Mattila et al., Citation2020; Naylor et al., Citation2019; Rockstroh et al., Citation2019; Stetz et al., Citation2011; Vaquero-Blasco et al., Citation2021), although pointed out that costs of certain equipment are prohibitive (Gaggioli et al., Citation2014). Four studies reported occasional technical or practical difficulties with hardware, such as equipment overheating (Cikajlo et al., Citation2017), participants struggling to operate technology (Gaggioli et al., Citation2014), physical difficulties wearing HMDs relating to its weight and the brightness of visual stimuli (Naylor et al., Citation2019), and cybersickness (Karacan et al., Citation2021).
Six out of 13 studies indicated the acceptability of HMD VR as a tool to support wellbeing in the workplace. Participants reported that interventions were immersive (Vaquero-Blasco et al., Citation2021), interesting (Maarsingh et al., Citation2019), a positive experience (Anderson et al., Citation2017), improved confidence (Blum et al., Citation2019), and increased motivation (Rockstroh et al., Citation2019). Participants expressed a desire to use VR in the future (Anderson et al., Citation2017; Rockstroh et al., Citation2019), with 80% indicating they would recommend it for workplace wellbeing (Maarsingh et al., Citation2019; Naylor et al., Citation2019). Data privacy was a concern for a minority of participants in one study (Naylor et al., Citation2019).
Three studies reported reduced stress or changed mindset about stress in HMD conditions, although there were no comparison conditions (Maarsingh et al., Citation2019; Vaquero-Blasco et al., Citation2021; Wang et al., Citation2019). Two controlled studies reported reduced stress with HMDs, although there was no significant difference with comparison conditions of a 2D screen (Rockstroh et al., Citation2019) or cognitive behaviour therapy (CBT) (Gaggioli et al., Citation2014). One study reported increased relaxation in HMD conditions, although there was no comparison condition (Anderson et al., Citation2017). Two controlled studies reported increased relaxation with HMDs, although there was no significant difference with 2D screen comparison conditions (Blum et al., Citation2019; Naylor et al., Citation2019). Three studies reported increased restoration with HMDs, although there was no comparison condition (Chung et al., Citation2018; Karacan et al., Citation2021; Mattila et al., Citation2020). An 8-week virtual mindfulness programme slightly decreased self-reported life satisfaction of a small sample of hospital volunteers and employees but patients increased life satisfaction (N = 8) post-intervention (Cikajlo et al., Citation2017). Both 2D and HMD VR nature scenes significantly increased indicators of creativity compared to urban scenes (Palanica et al., Citation2019). One large RCT (N = 121) with follow-up data found a therapist-assisted, 8-week intervention of coping skills in virtual work scenarios and relaxation techniques in virtual nature reduced self-reported stress in nurses and teachers as effectively as traditional CBT, and significantly more than a wait list control (Gaggioli et al., Citation2014). Another large study (N = 101) conducted in a real-world office found ‘immersive calming’ and ‘immersive stimulating’ VR nature scenes increased positive affect and decreased negative affect significantly when compared to 2D calming and stimulating nature scenes (Karacan et al., Citation2021). One large study (N = 100) found an immersive VR nature scene increased attention (Mattila et al., Citation2020), while another (N = 111) found a VR biofeedback game improved employees stress mindset (Maarsingh et al., Citation2019) in addition to their primary variables of restoration and stress. Increases in restoration were found in addition to primary variables of relaxation (Anderson et al., Citation2017) and stress (Wang et al., Citation2019) post-VR nature scenes.
Other immersive technology studies
Three out of four studies evaluated the feasibility of immersive technologies to support wellbeing in the workplace. The multi-sensory “Recharge” room was considered an accessible and scalable wellbeing and stress-reduction tool in healthcare settings (Putrino et al., Citation2020); the “Dream Island” scene was reported to be a time- and cost-efficient relaxation and anxiety-management tool for military personnel (Stetz et al., Citation2011); and the virtual water feature was found to be feasible to improve office environments (Abdalrahman & Galbrun, Citation2020).
Two out of four studies evaluated acceptability, and both reported positive feedback. Ninety-nine percent of healthcare worker participants, from a sample of 219, recommended the “Recharge room” for wider use in healthcare settings, especially during the COVID-19 pandemic (Putrino et al., Citation2020). Participants who experienced the “Dream Island” scene reported that they would like to use the intervention again in the future (Stetz et al., Citation2011).
The large “Recharge Room” study (N = 219) found significantly reduced self-measured stress after 15 minutes (Putrino et al., Citation2020). A 2D image of an attractive open plan office paired with water feature sounds had a significant restorative impact (Ma & Shu, Citation2018). Military medical personnel had significantly less anxiety after a VR guided relaxation scene compared to a waiting list control (Stetz et al., Citation2011). However, a subsequent stressful VR task showed no significant differences between conditions. One study found the addition of a simulated water feature combined with water feature sounds increased positive perception of a 2D image of an open plan office compared to an audio only condition, and masked ‘office conversations’ significantly more (Abdalrahman & Galbrun, Citation2020).
Quality assessment
Global ratings were “strong” (N = 1), “moderate” (N = 13), and “weak” (N = 3). See for quality ratings. Of the HMD VR studies, global ratings were “strong” (N = 1), “moderate” (N = 10), and “weak” (N = 2). Seven studies were RCTs, of which five were classified by the EPHPP tool as CCTs. The remaining studies were single group cohorts (N = 6) and rated “moderate”. All seven RCTs did not report if the assessor was blind to participant conditions or if participants were blind to study research questions. One study was rated “strong”, eight “moderate”, and four “weak” for how likely participants were to represent the target population. Data collection tools of seven studies were “strong” with evidence of validity and reliability. All studies reported an 80–100% study completion rate, giving them a withdrawals and dropouts rating of “strong”, although it is important to note that most studies were using a single session. Of the other immersive technology studies, global ratings were “moderate” (N = 3) and “weak” (N = 1). One study had an RCT study design, classified as a CCT, and rated “strong”. The remaining studies were single group cohorts (N = 3) rated “moderate”. All studies were unclear on important confounder information and rated “weak”. All studies were rated “moderate” for failing to report participant and assessor blinding. All studies demonstrated validity but not reliability in data collection tools giving them a “moderate” rating. Two studies were rated “strong” for reporting an 80–100% participant completion rate, and two rated “weak” because they had low or unreported withdrawals and dropouts.
Table 3. Summary of quality ratings of studies of virtual reality and immersive technologies to promote workplace wellbeing.
Discussion
This systematic review provides a narrative synthesis of evidence for feasibility, acceptability, and effectiveness of VR and immersive technologies to promote workplace wellbeing. Seventeen studies were included in the review, of which 13 used HMD VR and four used other immersive technologies, such as audio-visual environments and multi-sensory rooms. VR and immersive technologies were found to be feasible, acceptable, and effective. Experimental conditions mainly consisted of immersive audio-visual nature-based scenes with half employing relaxation exercises. They were found to improve wellbeing and reduce work-related stress and stress-related variables, such as restoration. Findings are consistent with research that indicates VR is a safe and popular wellbeing tool (Barton et al., Citation2020; Jerdan et al., Citation2018), can be used for stress management interventions (Naylor et al., Citation2020; Riches et al., Citation2021), and is increasingly affordable and available to consumers and organisations (Ahmaniemi et al., Citation2017).
Most studies indicated that nature-based virtual stimuli reduced stress and improved wellbeing in the short-term. This is consistent with reviews that have concluded that virtual nature-based experiences have a positive impact on wellbeing-related variables such as stress and affect (Riches et al., Citation2021). Even after short exposures, virtual nature – much like real-world nature – increases parasympathetic activity, lowers blood pressure, and reduces cerebral blood flow in the cerebral cortex, which improves wellbeing, mood, and stress (Annerstedt et al., Citation2013; Bowler et al., Citation2010; de Kort et al., Citation2006). Stress Reduction Theory postulates that nature, compared to urban environments, is uniquely restorative due to our evolutionary adaption to natural places. Attention Restoration is another prominent theory that explains the positive effect of nature on stress. In a work context, emotional recovery during breaktimes has been shown to increase job satisfaction and have a positive impact on work performance (Nijland et al., Citation2021; Panaccio & Vandenberghe, Citation2012; Sonnentag & Zijlstra, Citation2006), suggesting experiencing nature-based immersive technologies may be an effective way to improve employee wellbeing and productivity, particularly for those who do not have access to real-world nature during the working day.
The studies included in this review used both self-reported and physiological measurements to assess primary outcomes, such as stress, which enabled evaluation of the use of immersive technologies for workplace wellbeing. Most studies had comparison conditions which allowed the effectiveness of VR and immersive technology interventions to be more confidently assessed. Nearly a third of studies included 100 or more participants, which improved the strength of the findings. Limitations of the reviewed studies include a primary focus on short-term effectiveness and limited, brief interventions, which means that it is not possible to draw conclusions about any longer-term impact of these technologies. Only one study had follow-up data and most studies consisted of single-session interventions. In terms of study design, there were limited RCTs and most of these failed to report blinding. Sample limitations included limited information on participant occupations, limited occupations and workplaces tested, and demographically homogenous samples. Several studies discussed the application of immersive technologies in workplaces but only a small minority tested interventions in naturalistic workplace settings. Having longer-term data in real workplace environments is critical to validate the benefits of immersive technologies and assess if they can be maintained over time. Although several studies in this review reported that immersive technologies are now more cost-effective than they used to be (Putrino et al., Citation2020), this was generally not investigated by the studies themselves. Although some HMDs are significantly cheaper than they used to be, many non-HMD immersive technologies remain expensive (Guilbaud et al., Citation2021), which is likely to have contributed to the lack of these studies.
This systematic review is the first to assess the feasibility, acceptability, and effectiveness of VR and immersive technologies to promote workplace wellbeing. The comprehensive search strategy, with multiple databases searched, strengthens the confidence that the review found the most relevant research. Formal searching, screening, and data extraction were completed by two researchers which minimises researcher bias. Screening limitations might include the omission of grey literature, which may mean that interesting research not published in academic journals was excluded; and the research team’s limited capacity to review only English language publications, which means non-English language studies may have been overlooked. The review was deliberately broad in scope to cover a range of interventions and mixed samples. Therefore, further limitations of the review might include a lack of standardisation of sampling, interventions, measurements, and definitions. Sampling limitations reduces generalisability to broader workplace populations or to specific occupations. Stress was defined inconsistently across studies, and no standardised ‘stress’ measure was adopted, with each study implementing different self-report and physiological measures. Interventions varied in duration and number of sessions, which limits comparisons. Although this breadth of interventions and samples may hinder the extent to which studies can be compared, it also enabled a more comprehensive review of interventions for a variety of workers and workplaces in what is an emerging and exciting area of research.
The findings of this review, that VR promotes wellbeing, improves relaxation, and decreases stress in the workplace, indicates it has potential to be implemented as both a stress prevention and management tool in a variety of workplaces. Many VR HMDs and immersive technologies require minimal space, deployment costs, and maintenance, making them particularly viable and convenient (Vaquero-Blasco et al., Citation2021). This review found VR HMD interventions were widely considered easy-to-use and intuitive, making them particularly useful for those working from home, travelling away from home for work, or working in small or confined environments (Kanas et al., Citation2009). Wider research has found VR to be a generally popular intervention technology, suggesting it would be well-received in a variety of workplaces (Pretsch et al., Citation2020). The convenience and immersiveness of VR may lend itself to emotionally challenging working environments in which there is a lack of time to engage in stress management or access natural environments during the working day (Nahar & Gurav, Citation2018). With certain workforces, such as keyworkers, who may be at high risk of stress-related illnesses, VR and other immersive technologies could play an important role in facilitating stress relief in the workplace, both in general or as a designated ‘breaktime’ (Lin et al., Citation2015; Rössler, Citation2012). The findings of this review indicates that VR and immersive technologies that promote wellbeing in the workplace are likely to be important tools to provide early intervention and prevention of mental health problems for employees. This conclusion is supported by VR relaxation and wellbeing studies on people with mental health conditions that indicate benefits for stress and affect (Herrero et al., Citation2014; Liszio et al., Citation2018; Veling et al., Citation2021).
Immersive technologies may be particularly useful for employees impacted by COVID-19 who have seen workplaces and roles affected by changing circumstances. Indeed, government guidelines such as social distancing and working from home, have increased the number of people isolated and without regular contact with colleagues, leading to higher rates of mental illness (Holmes et al., Citation2020). For employees working during the pandemic, such as healthcare professionals and other keyworkers, COVID-19 has created extremely demanding workloads in unfamiliar working environments, severe staff shortages, and concerns for personal safety (Blake et al., Citation2020; Putrino et al., Citation2020). Immersive technologies offer employees, particularly those with less access to real-world nature, a viable respite from increasingly stressful workplaces. Organisations may wish to consider introducing these technologies to support staff wellbeing.
Given the limited number of studies and methodological limitations in this promising area, future research is vital. Research should aim to standardise study protocols, measures, and definitions, and consider differences amongst worker populations. Further research on a broader range of immersive technologies, such as cave systems and multi-sensory rooms, which show promise (Manjrekar et al., Citation2014), should be encouraged, as well as expanding outcome measures to other work-related variables, such as creativity and concentration. Longitudinal data, specialist employee-only samples, and larger RCT studies are crucial to understanding effectiveness, especially in the longer-term, of these immersive technologies. Naturalistic field studies testing specific worker populations in real working environments will help validate the applicability of immersive technologies in real-world workplaces. Studies should also investigate “dose” of the intervention (given that many had only one session), measure effects beyond the immediate change in stress and affect, and investigate mechanisms. Formal cost-effectiveness studies are needed, calculating effect on absenteeism, productivity, and healthcare costs.
In conclusion, this is the first systematic review and narrative synthesis of VR and other immersive technologies that aim to promote workplace wellbeing. Most studies used HMDs to display nature-based VR, with the majority reporting improvements in a range of wellbeing-related outcomes. Although methodological limitations mean caution should be taken when generalising findings to broader worker-populations or technologies, this review provides optimism for the use of immersive technologies, particularly VR, to promote workplace wellbeing. These technologies can be feasible, acceptable, and effective interventions that help mitigate the mental health impacts of isolating and unfamiliar working environments, and for those with highly stressful work demands.
Acknowledgements
All authors contributed to the study conception and design. The literature search and data analysis were performed by SR, LT, and PJ. Quality assessment was performed by LT, PJ, and SR. The first draft of the manuscript was written by SR and LT. All authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Disclosure statement
The authors have conducted virtual reality research that is related to the topic of this article.
Additional information
Funding
References
- Abdalrahman, Z., & Galbrun, L. (2020). Audio-visual preferences, perception, and use of water features in open-plan offices. The Journal of the Acoustical Society of America, 147(3), 1661–1672. https://doi.org/10.1121/10.0000892
- Ahmaniemi, T., Lindholm, H., Muller, K., & Taipalus, T. 2017. Virtual reality experience as a stress recovery solution in workplace [Paper presentation]. Paper presented at the 2017 IEEE Life Sciences Conference (LSC). https://doi.org/10.1109/LSC.2017.8268179
- Anderson, A. P., Mayer, M. D., Fellows, A. M., Cowan, D. R., Hegel, M. T., & Buckey, J. C. (2017). Relaxation with immersive natural scenes presented using virtual reality. Aerospace Medicine and Human Performance, 88(6), 520–526. https://doi.org/10.3357/AMHP.4747.2017
- Annerstedt, M., Jönsson, P., Wallergård, M., Johansson, G., Karlson, B., Grahn, P., Hansen, A. M., & Währborg, P. (2013). Inducing physiological stress recovery with sounds of nature in a virtual reality forest—Results from a pilot study. Physiology & Behavior, 118, 240–250. https://doi.org/10.1016/j.physbeh.2013.05.023
- Balaji, P., Varne, S. R., & Ali, S. S. (2012). Physiological effects of yogic practices and transcendental meditation in health and disease. North American Journal of Medical Sciences, 4(10), 442–448. https://doi.org/10.4103/1947-2714.101980
- Barton, A. C., Sheen, J., & Byrne, L. K. (2020). Immediate Attention Enhancement and Restoration From Interactive and Immersive Technologies: A Scoping Review. Frontiers in Psychology, 11, 2050. https://doi.org/10.3389/fpsyg.2020.02050
- Blake, H., Bermingham, F., Johnson, G., & Tabner, A. (2020). Mitigating the psychological impact of COVID-19 on healthcare workers: a digital learning package. International Journal of Environmental Research and Public Health, 17(9), 2997. https://doi.org/10.3390/ijerph17092997
- Blum, J., Rockstroh, C., & Göritz, A. S. (2019). Heart rate variability biofeedback based on slow-paced breathing with immersive virtual reality nature scenery. Frontiers in Psychology, 10, 2172. https://doi.org/10.3389/fpsyg.2019.02172
- Bowler, D. E., Buyung-Ali, L. M., Knight, T. M., & Pullin, A. S. (2010). A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health, 10(1), 1–10. https://doi.org/10.1186/1471-2458-10-456
- Chung, K., Lee, D., & Park, J. Y. (2018). Involuntary attention restoration during exposure to mobile-based 360 virtual nature in healthy adults with different levels of restorative experience: Event-related potential study. Journal of Medical Internet Research, 20(11), e11152. https://doi.org/10.2196/11152
- Cikajlo, I., Staba, U. C., Vrhovac, S., Larkin, F., & Roddy, M. (2017). A cloud-based virtual reality app for a novel telemindfulness service: rationale, design and feasibility evaluation. JMIR Research Protocols, 6(6), e6849. https://doi.org/10.2196/resprot.6849
- de Kort, Y. A., Meijnders, A. L., Sponselee, A. A., & IJsselsteijn, W. A. (2006). What’s wrong with virtual trees? Restoring from stress in a mediated environment. Journal of Environmental Psychology, 26(4), 309–320. https://doi.org/10.1016/j.jenvp.2006.09.001
- Edwards, D., & Burnard, P. (2003). A systematic review of stress and stress management interventions for mental health nurses. Journal of Advanced Nursing, 42(2), 169–200. https://doi.org/10.1046/j.1365-2648.2003.02600.x
- EPHPP (2010). Quality assessment tool for quantitative studies. The Effective Public Health Practice Project. http://www.ephpp.ca/PDF/Quality%20Assessment
- Gaggioli, A., Pallavicini, F., Morganti, L., Serino, S., Scaratti, C., Briguglio, M., & Bernava, G. (2014). Experiential virtual scenarios with real-time monitoring (interreality) for the management of psychological stress: a block randomized controlled trial. Journal of Medical Internet Research, 16(7), e3235. https://doi.org/10.2196/jmir.3235
- Gorini, A., & Riva, G. (2008). The potential of Virtual Reality as anxiety management tool: a randomized controlled study in a sample of patients affected by Generalized Anxiety Disorder. Trials, 9(1), 1–9. https://doi.org/10.1186/1745-6215-9-25
- Guilbaud, P., Guilbaud, T. C., & Jennings, D. (2021). Extended Reality, Pedagogy, and Career Readiness: A Review of Literature. [Paper presentation]. Paper presented at the International Conference on Human-Computer Interaction.
- Harvey, S. B., Modini, M., Joyce, S., Milligan-Saville, J. S., Tan, L., Mykletun, A., Bryant, R. A., Christensen, H., & Mitchell, P. B. (2017). Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occupational and Environmental Medicine, 74(4), 301–310. https://doi.org/10.1136/oemed-2016-104015
- Herrero, R., García-Palacios, A., Castilla, D., Molinari, G., & Botella, C. (2014). Virtual reality for the induction of positive emotions in the treatment of fibromyalgia: a pilot study over acceptability, satisfaction, and the effect of virtual reality on mood. Cyberpsychology, Behavior and Social Networking, 17(6), 379–384. https://doi.org/10.1089/cyber.2014.0052
- Holmes, E. A., O'Connor, R. C., Perry, V. H., Tracey, I., Wessely, S., Arseneault, L., Ballard, C., Christensen, H., Cohen Silver, R., Everall, I., Ford, T., John, A., Kabir, T., King, K., Madan, I., Michie, S., Przybylski, A. K., Shafran, R., Sweeney, A., … Bullmore, E. (2020). Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. The Lancet. Psychiatry, 7(6), 547–560. https://doi.org/10.1016/S2215-0366(20)30168-1
- Horesh, D., & Brown, A. D. (2020). Traumatic stress in the age of COVID-19: A call to close critical gaps and adapt to new realities. Psychological Trauma : theory, Research, Practice and Policy, 12(4), 331–335. https://doi.org/10.1037/tra0000592
- HSE (2020a). Health and Safety Executive, Costs to Great Britain of workplace injuries and new cases of work-related Ill Health – 2018/19. https://www.hse.gov.uk/statistics/cost.htm
- HSE. (2020b). Health and Safety Executive, Work-related stress, anxiety or depression statistics in Great Britain, 2020. https://www.hse.gov.uk/statistics/causdis/stress.pdf
- Jerdan, S. W., Grindle, M., van Woerden, H. C., & Boulos, M. N. K. (2018). Head-mounted virtual reality and mental health: critical review of current research. JMIR Serious Games, 6(3), e9226. https://doi.org/10.2196/games.9226
- Kanas, N., Sandal, G., Boyd, J., Gushin, V., Manzey, D., North, R., & Fiedler, E. (2009). Psychology and culture during long-duration space missions. Acta Astronautica, 64(7-8), 659–677. https://doi.org/10.1016/j.actaastro.2008.12.005
- Karacan, B., Kombeiz, O., & Steidle, A. (2021). Powered by virtual realities: promoting emotional recovery through technology-based recovery interventions. Ergonomics, ;64(10):1351–1366. https://doi.org/10.1080/00140139.2021.1912399
- Kirkham, H. S., Clark, B. L., Bolas, C. A., Lewis, G. H., Jackson, A. S., Fisher, D., & Duncan, I. (2015). Which modifiable health risks are associated with changes in productivity costs? Population Health Management, 18(1), 30–38. https://doi.org/10.1089/pop.2014.0033
- Klatt, M. D., Buckworth, J., & Malarkey, W. B. (2009). Effects of low-dose mindfulness-based stress reduction (MBSR-ld) on working adults. Health Education & Behavior : The Official Publication of the Society for Public Health Education, 36(3), 601–614. https://doi.org/10.1177/1090198108317627
- Li, M., Wang, L., Jiang, M., Wu, D., Tian, T., & Huang, W. (2020). Relaxation techniques for depressive disorders in adults: a systematic review and meta-analysis of randomised controlled trials. International Journal of Psychiatry in Clinical Practice, 24(3), 219–226. https://doi.org/10.1080/13651501.2020.1764587
- Liberatore, M. J., & Wagner, W. P. (2021). Virtual, mixed, and augmented reality: A systematic review for immersive systems research. Virtual Reality, 25(6), 1–27. https://doi.org/10.1007/s10055-020-00492-0
- Lin, S. L., Huang, C. Y., Shiu, S. P., & Yeh, S. H. (2015). Effects of yoga on stress, stress adaption, and heart rate variability among mental health professionals—A randomized controlled trial. Worldviews on Evidence-Based Nursing, 12(4), 236–245. https://doi.org/10.1111/wvn.12097
- Liszio, S., Graf, L., & Masuch, M. (2018). The relaxing effect of virtual nature: immersive technology provides relief in acute stress situations. Annual Review of Cybertherapy and Telemedicine, 16, 87–93.
- Ma, H., & Shu, S. (2018). An experimental study: The restorative effect of soundscape elements in a simulated open-plan office. Acta Acustica United with Acustica, 104(1), 106–115. https://doi.org/10.3813/AAA.919150
- Maarsingh, B. M., Bos, J., Van Tuijn, C. F., & Renard, S. B. (2019). Changing stress mindset through Stressjam: a virtual reality game using biofeedback. Games for Health Journal, 8(5), 326–331. https://doi.org/10.1089/g4h.2018.0145
- Manjrekar, S., Sandilya, S., Bhosale, D., Kanchi, S., Pitkar, A., & Gondhalekar, M. (2014). CAVE: an emerging immersive technology–a review [Paper presentation]. Paper presented at the 2014 UKSim-AMSS 16th International Conference on Computer Modelling and Simulation.
- Mattila, O., Korhonen, A., Pöyry, E., Hauru, K., Holopainen, J., & Parvinen, P. (2020). Restoration in a virtual reality forest environment. Computers in Human Behavior, 107, 106295. https://doi.org/10.1016/j.chb.2020.106295
- Mezzina, R., Sashidharan, S., Rosen, A., Killaspy, H., & Saraceno, B. (2020). Mental health at the age of coronavirus: time for change. Social Psychiatry and Psychiatric Epidemiology, 55(8), 965–968. https://doi.org/10.1007/s00127-020-01886-w
- Michalos, G., Karvouniari, A., Dimitropoulos, N., Togias, T., & Makris, S. (2018). Workplace analysis and design using virtual reality techniques. CIRP Annals, 67(1), 141–144. https://doi.org/10.1016/j.cirp.2018.04.120
- Michel, A., Bosch, C., & Rexroth, M. (2014). Mindfulness as a cognitive–emotional segmentation strategy: An intervention promoting work–life balance. Journal of Occupational and Organizational Psychology, 87(4), 733–754. https://doi.org/10.1111/joop.12072
- Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & Group, P, PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Medicine, 6(7), e1000097. https://doi.org/10.1371/journal.pmed.1000097
- Nahar, S., & Gurav, R. (2018). Practice of relaxation techniques amongst working women. Practice, 3(1), 226–229.
- Naylor, M., Morrison, B., Ridout, B., & Campbell, A. (2019). Augmented experiences: investigating the feasibility of virtual reality as part of a workplace wellbeing intervention. Interacting with Computers, 31(5), 507–523. https://doi.org/10.1093/iwc/iwz033
- Naylor, M., Ridout, B., & Campbell, A. (2020). A scoping review identifying the need for quality research on the use of virtual reality in workplace settings for stress management. Cyberpsychology, Behavior and Social Networking, 23(8), 506–518. https://doi.org/10.1089/cyber.2019.0287
- Nijland, J., Veling, W., Lestestuiver, B. P., & Van Driel, C. M. (2021). Virtual reality relaxation for reducing perceived stress of intensive care nurses during the COVID-19 pandemic. Frontiers in Psychology, 12, 706527. https://doi.org/10.3389/fpsyg.2021.706527
- Nordgård, R., & Låg, T. (2021). The effects of virtual reality on procedural pain and anxiety in pediatrics: a systematic review and meta-analysis. Frontiers in Virtual Reality, 2, 95. https://doi.org/10.3389/frvir.2021.699383
- Palanica, A., Lyons, A., Cooper, M., Lee, A., & Fossat, Y. (2019). A comparison of nature and urban environments on creative thinking across different levels of reality. Journal of Environmental Psychology, 63, 44–51. https://doi.org/10.1016/j.jenvp.2019.04.006
- Panaccio, A., & Vandenberghe, C. (2012). Five-factor model of personality and organizational commitment: The mediating role of positive and negative affective states. Journal of Vocational Behavior, 80(3), 647–658. https://doi.org/10.1016/j.jvb.2012.03.002
- Pretsch, J., Pretsch, E., Saretzki, J., Kraus, H., & Grossmann, G. (2020). Improving employee well-being by means of virtual reality–REALEX: an empirical case study. European Journal of Economics and Business Studies, 6(1), 95–105. https://doi.org/10.26417/ejes.v6i1.p95-105
- Putrino, D., Ripp, J., Herrera, J. E., Cortes, M., Kellner, C., Rizk, D., & Dams-O’Connor, K. (2020). Multisensory, nature-inspired recharge rooms yield short-term reductions in perceived stress among frontline healthcare workers. Frontiers in Psychology, 11, 3213. https://doi.org/10.3389/fpsyg.2020.560833
- Quick, J. C. E., & Tetrick, L. E. (2011). Handbook of occupational health psychology. American Psychological Association.
- Rajguru, C., Obrist, M., & Memoli, G. (2020). Spatial soundscapes and virtual worlds: challenges and opportunities. Frontiers in Psychology, 11, 2714. https://doi.org/10.3389/fpsyg.2020.569056
- Riches, S., Azevedo, L., Bird, L., Pisani, S., & Valmaggia, L. (2021). Virtual reality relaxation for the general population: a systematic review. Social Psychiatry and Psychiatric Epidemiology, 56(10), 1707–1727. https://doi.org/10.1007/s00127-021-02110-z
- Riches, S., & Smith, H. (2022). Taking a break in the “new normal”: virtual reality relaxation for a stressed workforce. Mental Health Review Journal, 27(2), 133–136. https://doi.org/10.1108/MHRJ-06-2022-095
- Rockstroh, C., Blum, J., & Göritz, A. S. (2019). Virtual reality in the application of heart rate variability biofeedback. International Journal of Human-Computer Studies, 130, 209–220. https://doi.org/10.1016/j.ijhcs.2019.06.011
- Rössler, W. (2012). Stress, burnout, and job dissatisfaction in mental health workers. European Archives of Psychiatry and Clinical Neuroscience, 262(2), 65–69. https://doi.org/10.1007/s00406-012-0353-4
- Seymour, L. (2010). Common mental health problems and work: applying evidence to inform practice. Perspectives in Public Health, 130(2), 59–60. https://doi.org/10.1177/1757913910363221
- Slater, M., Usoh, M., & Steed, A. (1994). Depth of presence in virtual environments. Presence: Teleoperators and Virtual Environments, 3(2), 130–144. https://doi.org/10.1162/pres.1994.3.2.130
- Sonnentag, S., & Zijlstra, F. R. (2006). Job characteristics and off-job activities as predictors of need for recovery, well-being, and fatigue. The Journal of Applied Psychology, 91(2), 330–350. https://doi.org/10.1037/0021-9010.91.2.330
- Stetz, M. C., Kaloi-Chen, J. Y., Turner, D. D., Bouchard, S., Riva, G., & Wiederhold, B. K. (2011). The effectiveness of technology-enhanced relaxation techniques for military medical warriors. Military Medicine, 176(9), 1065–1070. https://doi.org/10.7205/MILMED-D-10-00393
- Tetrick, L. E., & Winslow, C. J. (2015). Workplace stress management interventions and health promotion. Annual Review of Organizational Psychology and Organizational Behaviour, 2(1), 583–603. https://doi.org/10.1146/annurev-orgpsych-032414-111341
- Vaquero-Blasco, M. A., Perez-Valero, E., Morillas, C., & Lopez-Gordo, M. A. (2021). Virtual reality customized 360-degree experiences for stress relief. Sensors, 21(6), 2219. https://doi.org/10.3390/s21062219
- Veling, W., Lestestuiver, B., Jongma, M., Hoenders, H. R., & van Driel, C. (2021). Virtual reality relaxation for patients with a psychiatric disorder: crossover randomized controlled trial. Journal of Medical Internet Research, 23(1), e17233. https://doi.org/10.2196/17233
- Villani, D., Riva, F., & Riva, G. (2007). New technologies for relaxation: The role of presence. International Journal of Stress Management, 14(3), 260. https://doi.org/10.1037/1072-5245.14.3.260
- Wang, X., Shi, Y., Zhang, B., & Chiang, Y. (2019). The influence of forest resting environments on stress using virtual reality. International Journal of Environmental Research and Public Health, 16(18), 3263. https://doi.org/10.3390/ijerph16183263
- WHO. (2017). Mental health in the workplace. https://www.euro.who.int/en/health-topics/noncommunicable-diseases/mental-health/areas-of-work/mental-health-in-the-workplace
- Wiegner, L., Hange, D., Björkelund, C., & Ahlborg, G. (2015). Prevalence of perceived stress and associations to symptoms of exhaustion, depression and anxiety in a working age population seeking primary care-an observational study. BMC Family Practice, 16(1), 1–8. https://doi.org/10.1186/s12875-015-0252-7
- Wolever, R. Q., Bobinet, K. J., McCabe, K., Mackenzie, E. R., Fekete, E., Kusnick, C. A., & Baime, M. (2012). Effective and viable mind-body stress reduction in the workplace: a randomized controlled trial. Journal of Occupational Health Psychology, 17(2), 246–258. https://doi.org/10.1037/a0027278
- Yu, C.-P., Lee, H.-Y., & Luo, X.-Y. (2018). The effect of virtual reality forest and urban environments on physiological and psychological responses. Urban Forestry & Urban Greening, 35, 106–114. https://doi.org/10.1016/j.ufug.2018.08.013