
Abstract
Purpose: To explore ideas experts, working in the field of physical activity for people with a disability, pose on a stimulating movement intervention for physically disabled people longer than one year post rehabilitation or not familiar with rehabilitation.
Methods: Four semi-structured focus groups were conducted with experts (n = 28). Transcripts were analysed following thematic analysis, using the integrated physical activity for people with a disability and intervention mapping model.
Results: Experts expressed no need for a new intervention, but, instead, a need for adapting an existing intervention, and increased collaboration between organisations. Such an adapted intervention should aim to change participants and environmental attitude towards physical activity, and to increase visibility of potential activities. Several methods were mentioned, for instance individual coaching. Potential participants should be personally approached via various intermediates. The intervention owner and government are responsible for stimulating physical activity and should finance an intervention together with health insurances and the user.
Conclusions: According to experts adapting an existing intervention, together with increased collaboration between organisations, will be effective in stimulating physical activity in the target population. This study provides requirements on an intervention to stimulate physical activity, and suggestions for the approach of the target population, finance, and responsibility.
There is no need for designing a new intervention, but need for adaptation of an existing intervention for stimulating physical activity in physically disabled people.
An intervention to stimulate physical activity in physically disabled people should aim to change participants and environmental attitude towards physical activity, and to increase the visibility of potential activities.
Methods for stimulating physical activity in physically disabled people could be the use of individual coaching, feedback, a trial period, and role models.
Potential participants should be personally approached via a network of intermediate organisations and via marketing, and the social environment.
Implications for Rehabilitation
Introduction
In 2011, 15% of the world population was estimated to live with some form of disability [Citation1]. Globally between 110 and 190 million adults have some difficulty in functioning [Citation1]. Due to population aging and increased incidence of chronic health conditions, rates of people with a disability are rising [Citation1]. In the Netherlands, in 2012, 9.6% of the adult population suffered from impaired mobility [Citation2]. Physical activity1 benefits health in healthy people [Citation3], as well as disabled people. In disabled people, physical activity can reduce pain, depressive symptoms, stress, and the risk for secondary health conditions and improve fitness, strength, and quality of life [Citation4–7]. Despite these beneficial effects, participation in physical activity of physically disabled people (41%) in the Netherlands is significantly lower compared to healthy people (64%) [Citation8]. Within physical activity a distinction can be made between daily physical activity and sports2 participation. Sports are a specific part of physical activity [Citation9].
Movement interventions are structured programmes aimed to increase the level of physical activity. In the Netherlands, for physically disabled people a number of stimulating movement interventions already exist [Citation10,Citation11]. Most existing interventions for disabled people are offered within the setting of primary health care, special education or rehabilitation [Citation10,Citation11]. However, only a limited part of the entire physically disabled population can be reached by these intermediate organisations. It has been suggested that this limited reach reduces the effectiveness of existing interventions when evaluating physical activity in the entire physically disabled population [Citation8]. For approaching the entire spectrum of physically disabled people, an intervention in a community setting is required.
The internationally available movement interventions for physically disabled people are described in two systematic reviews [Citation12,Citation13]. However, both described organised exercise groups which were specifically organised and offered as an intervention, instead of interventions that stimulate physically disabled people to participate in existing physical activity groups. One of the reviews focused specifically on interventions in a community setting. Although only structured exercise programmes were found as an intervention, different strategies for approaching the target population, as the use of flyers, patient groups, and newspapers were described [Citation13].
For planning health promoting interventions, intervention mapping (IM), consisting of six steps, is a generally approved method [Citation14]. This study focuses on selecting theory-based intervention strategies and practical strategies (step 2 and 3 of IM) [Citation14]. The physical activity for people with a disability (PAD) model describes physical activity behaviour in people that suffer from a physical disability [Citation15]. In this study, the IM model and the PAD model are integrated to describe both an intervention that stimulates physical activity and the physical activity behaviour itself. Supplementary material S1 describes the integration of the IM (steps 2 and 3) and the PAD model into the final integrated framework.
The need for the development and evaluation of physical activity interventions for disabled adults is emphasised in two recent systematic reviews [Citation12,Citation13]. This study focuses on physically disabled people longer than one year post rehabilitation or not familiar with rehabilitation, since these people are currently not reached by an existing intervention during and after clinical rehabilitation [Citation16]. The aim of this study is to explore ideas that experts working in the field of physical activity for people with a disability pose on an intervention to stimulate all kinds of physical activity in this target population. These ideas can help to compose an effective intervention for stimulating physical activity in this population.
Methods
Study design
In September 2015, three focus groups were held with experts, working in the field of physical activity for people with a disability (for instance consultants in disability sports, or rehabilitation physicians) or being active in institutions that create conditions for physical activity for people with a disability (for instance municipalities). Evaluating these focus groups, experts working in strategic and policy-making positions were found missing. Consequently, a fourth group was organised in January 2016 with the latter experts. In this explorative phase, focus groups were preferred above individual interviews because of the interaction that benefits the discussion [Citation17]. In rehabilitation medicine the use of focus groups is recommended for generating programme ideas that can be subsequently tested [Citation17]. All four groups were organised at a neutral location, allowing participants to speak freely. After being informed that participation was voluntary and data would be processed anonymously, participants gave their written informed consent and agreed with audio recording the focus group interviews. The study protocol was approved by the Medical Ethical Committee of the University Medical Center Groningen, the Netherlands (METc 2015/378).
Participants
Potential participants were sampled purposively from the network of the research group and the national sports federation (NOC*NSF) (LK, RD). Potential participants worked in the sports-, healthcare-, social-, or governmental-sector, either at the execution or policy level, and were experienced with physical activity for people with a disability. Moreover, representatives of patient associations were invited. Thirty-seven potential participants were contacted by phone, after which an e-mail was sent including more detailed information (LK). By responding this e-mail potential participants declared their intention to participate. A total of 28 experts participated in this study (). Nine experts did not participate, mostly because of a lack of time.
Table 1. Descriptive information on the focus group participants.
Data collection
The first three groups were assigned based on maximum variation in expertise and gender within each group. All groups were guided by external experienced moderators, not involved in the research group (ST, FW, and JH), who launched discussion topics, ensured each participant was involved in the discussion, and stimulated discussion if necessary. Furthermore, content experts (LK, RD, and EJ) asked and answered content related questions. Lastly, assistants (DH, NF, and TZ) were responsible for audio-recordings and making notes.
Prior to the focus groups all participants received concise information about three existing interventions for stimulating physical activity in physically disabled people to ensure that all participants had the same basic knowledge. These three were the only Dutch licensed interventions aimed at stimulating sports or physical activity in physically disabled people that were not sport-specific [Citation11]. The first intervention provided recommendations for sports directly after clinical rehabilitation, the second intervention provided an overview of sport facilities, and the third provided individual guidance to organised sports. To define the specific target population, a short presentation was given prior to the focus groups. During the focus groups a semi-structured interview guide was used (supplementary material S2). Questions were based on step 4 of IM [Citation14] and the RE-AIM framework for evaluating the implementation of public health interventions [Citation18]. In the fourth focus group the order of questions 3 and 4 was changed to focus more on responsibility and financing instead of the content of the intervention, because of the more strategic background of the participants. Focus group sessions lasted 120 min.
Data analysis
The audio-recordings were transcribed verbatim (LK, DH, and NF). The transcripts were analysed following the method of thematic analysis since this forms a useful approach for applied research [Citation19,Citation20]. At first, the transcripts were read and summarised in order to get familiarised with the data (LK, DH, and NF). Secondly, LK, DH, and NF together created a preliminary coding tree, based on the summaries of the focus groups. All transcripts were coded (LK, DH, and NF) using the preliminary coding tree. New emerging codes were added to the preliminary coding tree during the coding process. To ensure consistency and quality of the coding process, the authors constantly discussed coding, and final coding was checked by the first author. After coding all focus groups, similar codes were grouped into themes, whereby the final coding tree was developed (LK, DH, and NF). This final coding tree was discussed within the research group. As a last step, data was interpreted by inserting the final codes into the integrated PAD-IM model. The Atlas.ti version 7.5.10 (GmbH, Berlin, Germany) software was used for analyses. The summary of the focus group was sent to all participants for member-checking.
Results
The results of the focus groups are summarised into the integrated PAD-IM model (). Throughout the results and discussion section, major topics, which are also presented in , are printed italic. Most experts stressed no need for a new intervention, but indicated a need for adapting an existing intervention, especially in the way the existing intervention approaches the target population.
Figure 1. Results of the focus group discussions summarised in the theoretical model. The order does not impose any sequence of importance. References refer to earlier studies that found comparable results. *Theme mentioned in the focus groups. PA: physical activity.
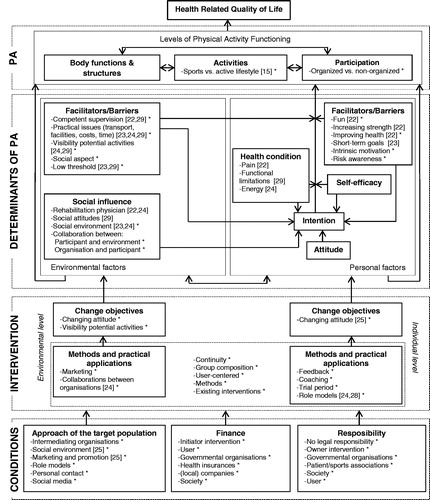
There are a lot of interventions in the Netherlands (…), so I think the whole secret is to pick out the right components, and combine these into one intervention. (Subject 20, adviser research and monitoring)
Physical activity
Experts stressed the importance of the distinction between sports and active lifestyle, since the term sports frightens and discourages some people. According to the experts, the intervention should not only stimulate sports participation, but also the adoption of an active lifestyle. All experts agreed that an intervention should not only stimulate participation in organised sports but should also focus on unorganised physical activity. However, some people are not independently able to participate in physical activity.
I think the focus is on how to activate as much people as possible, and then it does not matter if that is in organised or unorganised settings. (Subject 24, board member municipality)
Determinants of physical activity
The experts mentioned several determinants of physical activity, on which the intervention should focus. At the personal level experts indicated that the intervention should stimulate intrinsic motivation. A trainer in disability sports indicated that intrinsic motivation can be enlarged by gaining health benefits. For this it is essential that people gain insight in the risk of inactivity, and thereby the importance of physical activity. However, some experts mentioned that fun is more important than health effects of physical activity.
It has sort of a rehabilitation context. What benefits health, instead of what do you enjoy? (Subject 11, representative patient organisation)
One of the determinants of physical activity at the environmental level that was mentioned by the experts is the social aspect of physical activity. Especially participating in team activities can induce peer support whereby everyday troubles can be discussed. The most strongly emphasised environmental facilitator by the experts was that the activity should have a low threshold related to practical issues as location, accessibility of the accommodation, costs, and availability of devices. In a sparsely populated area, a carrousel in which different clubs and activities participate was suggested, since the location varies between the lessons. However, others assume a carrousel to be only useful for searching for an appropriate activity. Moreover, according to experts it is essential that the potential and suitability of activities are visible.
You still hear that people state as a barrier ‘I do not know what possibilities there are for me’. And anno 2015 that is something I hear of which I think ‘do we still hear this?’. Yes, we still hear this. (Subject 20, adviser research and monitoring)
Potential activities should be attuned to the population and thereby may differ from non-handicapped activities. One of the mentioned differences is on the competence of the supervisor, who requires knowledge and expertise with respect to the target population. Moreover, experts emphasised that the supervisor should be enthusiastic and should let the participants feel safe.
The experts assumed social influence of family and others in the social environment to increase participation in physical activity, especially in this population that is often dependent on others. Therefore, a collaboration between the participant, social environment, and the supplier is essential. The majority of the experts suggested that if the social environment, in particular the direct family, is enthusiastic, they will be more stimulant. One expert suggested that during organised movement activities for the target population an activity could be organised for the peers as well, in order to share experiences. However, this was not unanimously supported.
Intervention
The experts mentioned three different objectives on which an intervention should focus. The first objective influencing the environmental factors of physical activity is changing the attitude of the environment. There was general consensus that when physical activity for people with a disabilty becomes more accepted, physically disabled people will feel more comfortable and welcome to participate in physical activity.
The first team of a soccer club is still the most important, and disability soccer takes place on field 12 remotely (…). (Subject 16, project employee)
Secondly the visibility of potential activities should be increased. The experts suggested the use of an online search tool that describes the suitability of activities in a certain geographical area for different disabilities, and provides contact information.
Marketing and appropriate collaboration between organisations were mentioned as methods for both changing the attitude of the environment and increasing the visibility of potential activities. Effective marketing and publicity are required to gain attention for physical activity for people with a disabilty. An appropriate marketing strategy is required in which storytelling and an ambassador are suggested to form the basis. Unanimously, all experts expressed the need for an increased collaboration between organisations in the sports-, health care-, and governmental-sector to exchange experiences and to ensure that potential activities are aligned between different sectors and regions.
A third objective of the intervention should be to change the potential participant’s attitude towards physical activity. Especially, the representatives of the target population that were involved in the focus groups stressed that many physically disabled people assume physical activity as something that is for others, and do not feel comfortable in sports clubs. Experts suggested that the attitude towards physical activity can be changed by (media) attention.
With a general campaign on active lifestyle, a major part of this target population thinks this (active lifestyle campaign) is for others. ‘Having my impairment this does not apply’, because it (adopting an active lifestyle) will not succeed. (Subject 4, consultant disability sports)
Moreover using feedback, coaching, a trial period, and role models were suggested to change the potential participant’s attitude. Experts suggested “Motivational Interviewing” for stimulating intrinsic motivation during coaching sessions. Coaching sessions should result in an individual advice considering the demands and the suitable activities for each individual participant. In one of the four groups it was suggested to include feedback in the intervention, for instance an activity tracker, to stimulate intrinsic motivation. Also a trial period can improve the attitude towards physical activity. However, experts indicated a follow-up and a small financial contribution as essential to stimulate participants to actually participate. Lastly, in three of the four focus groups role models were suggested to be applicable for changing the attitude of physically disabled people towards physical activity because the target population can better identify with them.
Stimulating someone as a fellow sufferer, when I say ‘you can ski on one leg’, that sounds different than when you (non-impaired person) say that. (Subject 18, representative target population)
A sustainable behavioural change is needed that requires long-term coaching and after care, for what continuity of the activities is necessary. In order to improve the social aspect of physical activity, sports or physical activity groups should be composed of likeminded people. However, experts indicated that in some cases physical activity for people with a disability can be integrated into physical activity for non-disabled people, in order to increase social commitment. All experts agreed that the intervention should be user-centred, what implies that it should be question based, and adjustable to the participant. For attracting potential participants, fitness tests, free consults, movement gardens, and mobile phone applications were advised by the experts.
Conditions
According to experts the target population should be approached using various intermediate organisations, such as welfare organisations, general practitioners, or physiotherapists. Since primary care has a signalling function, the local organisational structure should be acquainted by the primary care, so that they can address their patients to the appropriate organisation. However, from the experiences of our experts, general practitioners have a lack of time, and physiotherapists do not want to “lose” their patients.
But then they take away my patients’. Because the physiotherapist was not primarily focused on the interest of the patient. (…) So his first focus is I am a business owner and the patient comes second. (Subject 6, adviser disability sports)
Moreover, experts suggest patient associations, organisations for disabled people and organisations that provide indications for medical devices to act as intermediate organisations since they are in contact with the target population. According to the experts, the disadvantage of approaching the participants via intermediate organisations is that it is mostly not possible, for privacy reasons, to obtain contact information of the target population, making the executor of the intervention dependent on the willingness of intermediate organisations.
Furthermore, social environment is suggested as a way to approach the target population. The target population can be found in their own residential area, for instance at the library or supermarket. A board member of a local government emphasised that many Dutch municipalities are developing a structure of social district teams. These social district teams do have personal contact with their fellow residents and can have a signalling and referring function.
That are people that could signal issues (for instance problems with physical activity) close by, and perhaps hear from their neighbours that their neighbour in a wheelchair never participates (in physical activity). (Subject 27, manager)
Experts expressed the importance of a good marketing and promotion strategy from which physical activity appeals. According to the experts this strategy should be varied and not only include flyers. Moreover, the experts expressed a need for nationwide unity so that the programme can be promoted nationwide. Marketing and promotion can be advertisements (in newspapers, at general practitioners and at sports and patient organisations), at meetings and word of mouth advertisement. Experiences of role models can be used for marketing. Unanimously, all experts emphasised that it is essential to personally approach people. However, one manager indicated that this seems unrealistic. As a method for approaching potential participants, social media was also suggested, although there were also negative experiences on the effect of social media.
For maintaining the execution of the intervention, experts considered structural finance and allocation of responsibility to be important. With regard to the financing of the intervention the experts indicated the initiator of the intervention being responsible for both financing the initiation phase as the long-term finance. The initiator is responsible for proving cost-effectiveness of the intervention and for finding long-term finance. According to the experts, physical activity should be financed by the user itself, since non-disabled people also finance their own physical activity, and it increases motivation.
Therefore I think that it is important to be owner and finance your physical activity yourself (impaired person), because if it will be paid for you than you will earlier cease. (Subject 12, researcher, teacher)
Experts indicated that physically disabled people are in a lower financial status more often because of the consequences of their disability. Therefore, some experts stated that the additional costs of physical activity for people with a disability (compared to physical activity for non-disabled people) should be financed. Experts assume the government (Ministry of Health, Welfare, and Sport) as partly responsible for financing since they determine the health policy. However, experts experienced getting interventions aimed at stimulating physical activity financed by the national government to be difficult. When an intervention contributes to the achievement of local governmental goals it may be financed by local government. A board member of a local government indicated that currently in the Netherlands the way local government finances sports is changing. Where sport clubs obtained money from local government nowadays, they have to earn it by acting as a social organisation in the nearby future. By means of this change, sport clubs can maybe play a role in executing interventions for people with a disability in order to earn financial support from local government.
What do we (local government) finance, and what do we get back? And should this be in a traditional way as we always did, or can we also consider if we are (…) a social organisation instead of only a sport club. (Subject 24, board member local government)
It was stated that when an intervention proves to be cost-effective, reducing the costs of health care, health insurances, profit companies, and society are more likely to also financially contribute, since the intervention is commercially attractive and may reduce the premium of the health care insurance.
Regarding the responsibility for stimulating physical activity the experts indicated that the responsibility is not legally determined, because being physically active is not compulsory by law. When the development of an intervention is part of a research project, it is needed to focus on securing the intervention during the early designing phase, in order to designate an organisation in which the intervention can be accommodated structurally. To ensure unity in the stimulation of physical activity this requires nationwide control and an appropriate monitoring system.
Experts stated that governmental organisations are responsible for welfare of their citizens, including stimulating physical activity. For the experts, it was unclear on which governmental level this should be executed in order to have a sufficient population. Some experts experienced that municipal governments are often not aware of the number of physically disabled people in their community what makes them not feeling responsible.
We do not have physically disabled people in our community’, and that remains. Yes they say so, they (municipal government) literally give this as a reason not to participate. (Subject 4, consultant disability sports)
Furthermore, experts assumed rehabilitation centres to be responsible for the execution of interventions since they have knowledge and experience in working with the target population. Moreover, as stated by a rehabilitation physician, in some cases rehabilitation centres are obliged to implement interventions for getting a status (as for instance a centre of excellence for cardiac rehabilitation) awarded. However, project managers experienced that it is hard to secure interventions in rehabilitation centres when project finance ends.
Inactivity leads to health risks. If secondary health problems occur, this costs community money, whereby the experts stated that society is also partly responsible for stimulating physical activity. Since many parties are partly responsible, experts expressed a need for an appropriate structure in which healthcare, welfare, sports, and policymakers collaborate. These collaborations can organise interventions in which each organisation focuses on its own expertise. However, experts indicate primarily the user as responsible for its own physical activity behaviour, since this improves intrinsic motivation what leads to increased enthusiasm. Therefore, the experts recommend to involve the target group in designing the intervention.
According to the experts an intervention should be organised nationwide, and implemented locally. This national collaboration leads to exchange of knowledge and experiences, while the local implementation enables adaptation to the local situation.
Discussion
This study aimed to explore experts’ ideas on the content and implementation of a physical activity stimulating intervention for physically disabled people longer than one year post rehabilitation or not familiar with rehabilitation. Experts stressed no need for a new intervention, but instead, suggested to adapt a number of key aspects () of an existing intervention. An intervention should for instance increase intrinsic motivation, have a low threshold and involve social environment. For this, it is required to change attitude towards physical activity in both the individual and the environment, and to increase the visibility of potential activities. Strongly emphasised concepts that should be included in an intervention were for instance user-centred coaching sessions and role models. Moreover, there was a strong demand towards more collaboration between organisations. For this intervention, the target population should be approached via intermediate organisations and social environment. The development of an intervention should be financed by the initiator, physical activity itself should be mainly financed by the user itself, and possibly partly by health insurances. There is no legal responsibility for stimulating physical activity in the physically disabled population.
The finding that no new intervention should be designed, but that an existing intervention should be adapted is consistent with research of Rimmer et al., which describes a framework for adapting existing evidence-based strategies for people with disabilities [Citation21]. The importance of stimulating both sports and active lifestyle agrees findings of van der Ploeg et al. [Citation15]. Determinants of physical activity were described in several studies, whereby the importance of fun, improving health, competent supervision, visibility of potential activities, and a low threshold regarding practical issues as transport and facilities are supported by earlier research [Citation22–25]. The focus on the social aspect of being physically active has not been found in earlier literature. The importance of involving the social environment corresponds with findings by Murphy et al. [Citation23]. The social influence of an appropriate collaboration between participant and environment and organisation, and participant are added by this study.
Findings of this study contribute to a broader physical activity and disability research agenda, in which science shifts from describing barriers and facilitators to developing strategies to increase physical activity among persons with a disability [Citation24]. For this reason, this study mainly adds intervention methods and required conditions for the implementation of the intervention. Earlier research of Geidl et al. provided a theory-based toolbox for designing exercise interventions, which primarily focused on personal factors of physical activity [Citation26]. Results of this study indicate that the intervention should aim changing the attitude of disabled people to physical activity. This is supported by literature and in accordance with the theory of planned behaviour, in which behavioural attitude is one of the aspects influencing intention [Citation25–27]. Experts advised the use of feedback, which agrees with earlier research describing that establishing short-term goals can increase motivation [Citation23,Citation26]. Moreover, the use of role models was advised, which is supported by earlier research [Citation24,Citation26,Citation28]. Compared to earlier research this study adds the use of individual coaching sessions and a trial period as methods at the individual level. The advice to use individual coaching sessions can be explained by the diverse target population. Hereby, it is possible to individually tailor the intervention to the individual capacity of the participant.
Moreover, the intervention should aim to change societal attitude towards physical activity. This finding agrees with research of Rimmer et al. and with the theory of planned behaviour in which subjective norms are influencing intention [Citation27,Citation29]. The last mentioned objective of the intervention, increasing visibility of potential activities, has not been found in earlier literature. The demand towards increased collaboration between organisations is supported by literature [Citation24]. However, this study adds marketing as a method for reaching the objectives of the intervention. Moreover, several practical applications, as group composition, are added by this study. Only social environment and marketing and promotion as ways to approach the target population were consistent with literature [Citation25]. No earlier studies described a network of intermediate organisations, role models, social media, and the importance of personal contact to approach the target population. To the best of our knowledge, this is the first study assigning the responsibility for financing and executing an intervention to stimulate physical activity in this target population.
A strength of this study is the high number of experts participating in our focus groups, and their very heterogeneous background. By performing the fourth focus group with experts with a more strategic background it was ensured that the view of multiple disciplines was investigated. To increase the validity of this qualitative study, a member check was performed after each focus group. To increase the reliability of the analysis, constant discussion took place during the coding process. Moreover, triangulation was achieved by including experts from various backgrounds.
Despite emphasising that this study focuses on stimulating both daily physical activity and sports participation, it could have been that experts in our focus groups focused more on either daily physical activity or on sports, depending on their background. Despite experts from social background were included, a relatively large number of experts from sports background were also included, since potential participants were recruited from the network of the research group and the national sports federation. This inclusion could have biased the results. Because of organisational reasons, all focus groups were led by three of the researchers, while two is more common. It could have been that experts felt limited to speak freely because of these three researchers, introducing bias in the results.
Moreover, during the discussions probably participants were guided by experience rather than imagination, what resulted in conventional ways of for instance approach of the target population. In this study only experts from the Netherlands were included. It should be taken into account that organisational structures that were mentioned for the approach of the target population, finance, and responsibility would be different in countries in which the health care system and sports policies are different from that in the Netherlands. However, content related components of the intervention, as aims and methods, are suggested to be applicable worldwide.
Future research should focus on adapting an existing intervention to this specific target population, and should investigate the feasibility and effectiveness of this adapted intervention. Based on the results of this study, the target population should be involved in composing the intervention. Since the target population was not fully represented in this study, it is suggested to also investigate the ideas regarding a physical activity stimulating intervention among the target population. Practical organisations should improve collaboration between organisations in multiple disciplines, as strongly recommended by the experts in this focus group.
Conclusions
According to experts working in the field of physical activity for people with a disabilty, there is no need for a new intervention, since adapting a number of key elements of an existing intervention are believed to be effective in stimulating movement in the target population. An adapted intervention should aim to improve attitude towards physical activity in both the individual and the environment, and to increase the visibility of potential activities. This study poses requirements on an intervention, and provides several practical applications for an intervention to stimulate physical activity. Moreover, suggestions are given to create conditions for an intervention, as how to approach the target population, how to finance the intervention, and parties that are responsible for stimulating physical activity in physically disabled people.
Leonie_Krops_et_al_supplemental_content.zip
Download Zip (428.7 KB)Acknowledgements
The authors thank S. van Twillert, F. P. C. Waterschoot, J. M. Hijmans, E. A. Jaarsma and T. Zijlstra for moderating and assisting the focus group discussions. Thanks to the National Sports Federation NOC*NSF for assisting the organisation and hosting the first three focus group discussions. We acknowledge participants on these focus group discussions for sharing their opinions and experiences.
Disclosure statement
The authors report no conflicts of interest.
Notes
Additional information
Funding
Notes
1 In this study, physical activity is defined as any bodily movement produced by skeletal muscles that require energy expenditure [Citation9].
2 Sports is defined as an activity involving physical exertion with or without game or competition elements, with a minimal duration of 30 min for at least two times a week, and where skills and physical endurance are either required or to be improved [Citation30].
Related Research Data
References
- World Health Organisation. World report on disability. Geneva, Switzerland: WHO Press; 2011.
- Van den Brink C, Savelkoul M, Gezondheidsmonitor GGD’en. CBS en RIVM [Health monitor Joint Health Duties, Central Statistical offica and National institute for health and Environment]. Volksgezond Toekomst Verkenning, Nationaal Kompas Volksgezond. 2013. Dutch.
- Haskell WL, Lee IM, Pate RR, et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007;39:1423–1434.
- Heath GW, Fentem PH. Physical activity among persons with disabilities-a public health perspective. Exerc Sport Sci Rev. 1997;25:195–234.
- Mulroy SJ, Thompson L, Kemp B, et al. Strengthening and optimal movements for painful shoulders (STOMPS) in chronic spinal cord injury: a randomized controlled trial. Phys Ther. 2011;91:305–324.
- Hicks AL, Martin KA, Ditor DS, et al. Long-term exercise training in persons with spinal cord injury: effects on strength, arm ergometry performance and psychological well-being. Spinal Cord. 2003;41:34–43.
- Rau B, Bonvin F, de Bie R. Short-term effect of physiotherapy rehabilitation on functional performance of lower limb amputees. Prosthet Orthot Int. 2007;31:258–270.
- von Heijden A, van den Dool R, van Lindert C, et al. (On)beperkt sportief 2013. Monitor sport- en beweegdeelname van mensen met een handicap [(Un)limited exercise 2013. Monitoring sports and physical activity participation of people with a disability]. Utrecht, the Netherlands: Mulier Instituut; 2013. Dutch.
- Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985;100:126–131.
- Rijksinstituut voor Volksgezondheid en Milieu. Centrum Gezond Leven [National institute for health and environment. Center for healthy life]. 2016 [cited 2016 July 7]. Available from: https://www.loketgezondleven.nl/leefstijlinterventies/interventiedatabase-gezond-en-actief-leven.Dutch.
- Kenniscentrum Sport. Netwerk in Beweging [Knowledge center Sport. Network in movement]. [cited 2016 July 7]. Available from: www.netwerkinbeweging.nl/interventies. Dutch.
- Rimmer JH, Chen MD, McCubbin JA, et al. Exercise intervention research on persons with disabilities: what we know and where we need to go. Am J Phys Med Rehabil. 2010;89:249–263.
- Cervantes CM, Taylor WC. Physical activity interventions in adult populations with disabilities: a review. Quest. 2011;63:385–410.
- Bartholomew LK, Parcel GS, Kok G, et al. Planning health promotion programs: an intervention mapping approach. San Fransisco: Jossey-Bass; 2011.
- van der Ploeg HP, van der Beek AJ, van der Woude LH, et al. Physical activity for people with a disability: a conceptual model. Sports Med. 2004;34:639–649.
- Alingh RA, Hoekstra F, van der Schans CP, et al. Protocol of a longitudinal cohort study on physical activity behaviour in physically disabled patients participating in a rehabilitation counselling programme: ReSpAct. BMJ Open. 2015;5:e007591.
- Race KE, Hotch DF, Packer T. Rehabilitation programme evaluation: use of focus groups to empower clients. Eval Rev. 1994;18:730–740.
- Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. 1999;89:1322–1327.
- Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psych. 2006;3:77–101.
- Braun V, Clarke V. What can “thematic analysis” offer health and wellbeing researchers? Int J Qual Stud Health Well-being. 2014;9:26152.
- Rimmer JH, Vanderbom KA, Bandini LG, et al. GRAIDs: a framework for closing the gap in the availability of health promotion programs and interventions for people with disabilities. Implementation Sci. 2014;9:100.
- Jaarsma EA, Dekker R, Geertzen JHB, et al. Sports participation after rehabilitation: barriers and facilitators. J Rehabil Med. 2016;48:72–79.
- Murphy NA, Carbone PS. Promoting the participation of children with disabilities in sports, recreation, and physical activities. Pediatrics. 2008;121:1057–1061.
- Martin Ginis KA, Ma JK, Latimer-Cheung AE, et al. A systematic review of review articles addressing factors related to physical activity participation among children and adults with physical disabilities. Health Psychol Rev. 2016;7199:1–31.
- Baker PR, Francis DP. Cochrane review: community-wide interventions for increasing physical activity. J Evid Based Med. 2015;8:57–58.
- Geidl W, Semrau J, Pfeifer K. Health behaviour change theories: contributions to an ICF-based behavioural exercise therapy for individuals with chronic diseases. Disabil Rehabil. 2014;36:1–10.
- Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50:179–211.
- Payne W, Reynolds M, Brown S, et al. Sports role models and their impact on participation in physical activity: a literature review. Australia: University of Ballarat; 2003.
- Rimmer JH, Riley B, Wang E, et al. Physical activity participation among persons with disabilities: barriers and facilitators. Am J Prev Med. 2004;26:419–425.
- Kemper H, Ooijendijk W, Stiggelbout M. Consensus over de Nederlandse norm voor gezond bewegen [Consensus on Dutch norm for healthy exercise]. Tijdschr Voor Soc Gezondheidszorg. 2000;78:180–183. Dutch.