
Abstract
Purpose: The aim was to identify and explore factors, which facilitate or hinder work participation for people with hearing impairment.
Materials and methods: In-depth interviews with 21 hearing impaired individuals of 32–67 years of age with a present or recent vocational affiliation were conducted. The analysis was conducted using a grounded theory approach.
Results: The analysis resulted in a conceptual framework of working life trajectories evolving through three phases of acknowledgement of hearing loss impact: the pre-acknowledgement, acknowledgement, and post-acknowledgement phase. The phases were influenced by the qualities of three contexts: the personal, the workplace, and the service provider. The qualities of the contexts, together with the amount of time spent in a pre-acknowledgement phase, formed the trajectories towards continuation of work participation or towards a disconnection. Accumulated risk factors constituted increased likelihood of disconnecting trajectories, while accumulated facilitating factors supported sustainable trajectories.
Conclusions: The results revealed a need for extended support at the workplaces, which includes the manager, colleagues, and professionals in the aim of preventing exhaustion and facilitate work participation among employees with hearing impairments. Joint action in facilitating communicative participation would share the responsibility for accommodation measures and broaden the room for manoeuver at the workplace.
Fatigue prevention in employees with hearing loss needs to be addressed in occupational rehabilitation.
Knowledge transfer on hearing loss implications needs to be included in aural rehabilitation.
Occupational rehabilitation professionals and professionals targeting hearing impairments should enter into systematic, multidisciplinary follow-up at the worksite.
Implications for rehabilitation
Introduction
Work participation is crucial to economic independency, professional and social fulfillment, and an important element of the personal identity. However, barriers to work participation might occur in individuals with impairments [Citation1]. Hearing impairments imply reduced access to oral communication which might result in such barriers and cause adverse effects on work participation. For instance, hearing impairment has been associated with a reduced degree of vocational participation, such as unemployment/underemployment [Citation2,Citation3], increased risk of disability pension [Citation4], and increased risk of stress-related sick leave [Citation5]. Moreover, increased levels of anxiety and depression in patients with severe and profound hearing loss compared to the population at large were found in a retrospective study [Citation6]. Participants with hearing impairments who were of working age were less likely to have high education and income, compared to normal hearing peers according to a cross-sectional study from the Netherlands [Citation7]. Additionally, persons with hearing impairments were less likely to have paid work exceeding 12 h and more likely to look for work or to be unfit for work [Citation7]. Higher odds for low-educational attainment and low income among people with hearing impairments were also found in the United States of America [Citation2]. Diverging results have been found for the risk of early retirement. Decreased likelihood was found among subjects with hearing impairment in a Dutch cross-sectional study [Citation7], while an increased risk was found with an increase in low-frequency hearing loss in a cohort study from Norway [Citation8].
Hearing loss is a highly prevalent chronic condition with an estimated 328 million adults worldwide [Citation9]. It is also prevalent in the working age population. The prevalence in the United States of America was estimated to 12.9% in 40– 49-year-olds and 28.5% in the age group 50–59 [Citation10]. In Norway, the estimated prevalence was approximately 11% in 45–64-year-olds [Citation11]. A Swedish study included tinnitus and found that 31% of the working population reported hearing loss, tinnitus or both and 36% did so in the non-working population [Citation12].
Many employees with hearing loss experience a high degree of strain or tiredness related to work. Thus, there is a need to consider hearing loss as a risk factor for fatigue [Citation5]. An increased need for recovery with increased hearing loss was found in a cohort study [Citation13], and a higher prevalence of hearing problems (hearing loss and/or tinnitus) was found among those with higher burnout scores [Citation12]. Moreover, an elevated fatigue score among people with hearing loss of working age was found in a cross-sectional study [Citation14]. The high levels of fatigue/exhaustion have been associated with the concentration and the hypervigilance, which employees with hearing impairments need in work settings [Citation15]. The task of compensating for the hearing loss together with the need to be prepared to initiate such compensation has been described as a double or triple workload [Citation16].
Employees with hearing impairments still face considerable barriers at work, such as restrictions in group interactions and suitable workplace accommodation awareness [Citation15]. However, how employees with hearing impairments perceive barriers and how the barriers contribute to fatigue are less understood. Furthermore, we know little about what employees with hearing impairments perceive as factors that facilitate work participation. Such knowledge is needed to develop appropriate measures to increase the likelihood of sustainable participation. Thus, the aim of this study was to identify and explore factors which facilitate or hinder work participation, as described by employees with hearing impairments. An ecologic perspective, which includes various contextual factors, was adopted since a variety of persons and mechanisms within and outside the workplace influence work participation.
Methods
An inductive approach was necessary to explore experiences with hearing loss at work. Thus, a qualitative approach based on individual interviews with persons with hearing impairment was chosen. An objective in this study was to reflect the variety of working life. Thus, we wanted to recruit participants from a wide spectre of professions, on different managerial levels and with various educational backgrounds.
Participants
Participants were recruited through an article in the journal of the Norwegian Association of the Hearing Impaired (December 2015) where the study was described and readers invited to participate. Inclusion criteria were: (1) having a hearing loss, (2) being of working age (18–67), and (3) having a recent vocational affiliation. We had no exclusion criteria.
Fifty-two individuals responded to the article. Potential participants who matched the inclusion criteria were contacted successively for interview arrangements, four of whom did not respond. Another one did not have a recent vocational affiliation. Purposeful sampling [Citation17] aiming for variation within working life experiences was performed based on the list of the potential participants. Further, sampling towards exploration of specific concepts was sought towards the end of the data collection representing theoretical sampling. Theoretical sampling implies that data collection is pursued until the developed concepts have been sufficiently explored [Citation18].
A total of 21 individuals were interviewed, where the age range was 32–67 and 13 were women (). All the participants had spoken language as their first language, and they had long-term experience of hearing loss. Of the 17 participants who did not have cochlear implants, audiograms were provided by 14 participants.
Table 1. Characteristics of participants.
The severity of hearing loss was assessed by the first author (who is an educational audiologist) based on the available audiograms and grouped according to the WHO classification (no impairment: 25 dB or better, mild impairment: 26–40 dB, moderate impairment 41–60, severe impairment: 61–80, profound impairment: 81 dB or greater (http://www.who.int/deafness/hearing_impairment_grades/en/)). Participants with cochlear implants were assessed as having severe/profound hearing loss, while other participants without audiograms were classified based on self-assessment.
Ethics
The study was approved by The Norwegian Centre for Research Data, NSD (ref. no. 47760). All participants received information about the project in advance of the appointment and signed an informed consent before the interview was conducted.
Data collection and analysis
An interview guide with open-ended questions (attached as supplementary material) was developed based on these professional experiences and previous research. The purpose of the interview guide was to ensure that the interviews included the following subjects: the nature of the hearing loss, working conditions, accommodation matters, leadership and cooperation, social belonging and participation. Questions were only asked if the participants did not launch the subjects themselves, or if elaboration was needed.
All interviews were conducted face to face in a quiet environment of the participants own choice. The participants were asked to tell their story of working life participation as hearing impaired with emphasis on present or most recent position including experiences throughout their total timespan of the hearing loss.
The interviews lasted from 55 min to 2 h, and were recorded and transcribed verbatim.
The first author is trained in the audiological field and has long-term experience in working with people with hearing impairments. The second author has experience with mixed methods studies, while the third author has extensive experience with qualitative research, both interview studies and grounded theory. None of the authors had any pre-existing relationship with any of the participants.
A grounded theory approach was chosen as method of analysis building on the procedure described in Corbin and Strauss [Citation18]. This method is particularly appropriate for areas scarcely described with an aim to develop an explanatory theory. In grounded theory, analysis and data collection are conducted successively until the concepts developed through the data analysis are defined, i.e., theoretical saturation is obtained. Data collection was performed as long as new interviews added to the concepts developed in the on-going analysis. When new interviews no longer added to the variety of the concepts within the frame of the sample available, theoretical saturation was perceived as obtained.
The analysis started directly after the first interview with the first author (EVS) reading through and writing a memo (written records of analysis) [Citation18] on the entire text describing the first impression of the story told. NVivo version 11 (QSR International, Melbourne, Australia) was used as a tool during the process of analysis.
In the next step, the text was decomposed into sections according to the theme in question, and memos on each section were written. The memos were labelled according to the main content. The last author (MBR) read the transcript of the interview and the memos, and the labels were discussed and renamed when necessary. The labels constituted an initial code list. Further exploration of the memos was conducted searching for concepts, and then for properties and dimensions. The next interview was analysed in the same manner with memos and coding at the existing codes. When new codes were added, the previous interview was revisited searching for similar text elements. Some codes needed relabelling during the process, while others needed elaboration into lower-level concepts. For example, a high-level code such as “workplace relations” had lower-level concepts such as “workplace culture,” “management involvement,” and “interactions.” The subsequent interviews were analysed in the same manner with memos and coding. The first (EVS) and last (MBR) authors discussed the further elaborated memos and code lists.
The aim of grounded theory is to build theory from data, where theoretical integration evolves through a central or core category [Citation18]. The central category could be a conceptual idea and should comprise all other categories. In this analysis process, the central category developed was “participation characteristics modifiable by support and knowledge.”
Another important step in grounded theory approach as presented in Corbin and Strauss [Citation18] is searching for process in the data. Throughout the analysis, the importance of time and the contexts in which the participants were engaged appeared fundamental. Amick et al. [Citation19] described a model on working life courses in a social context by the shape of trajectories. Their theoretical framework had constructive concepts, which appeared relevant to the understanding of this data material. Hence, the concepts of contexts and trajectories, as described in their article, were explored as a framework during the further course of analysis. The life course perspective in this study was limited to the hearing loss experiences. The contexts were elaborated and/or narrowed according to the quality of the data, i.e., the social context was limited to service providers, the labour market context was omitted, and a personal context was added. Furthermore, we have concentrated on transitions concerning hearing-related health aspects and work participation and elaborated on the influence of such transitions into trajectory phases.
In the analysis process, the procedure of Corbin and Strauss [Citation18] was followed as far as practically feasible. However, it was necessary to conduct interviews continuously. Consequently, the procedure of alternating between interviews and analysis was followed in the sense that interviews were analysed one at a time and that the continuous analysis brought new aspects to subsequent interviews. The final memo in the analysis constituted an analytic story, which told the main outline of participants’ stories. The theoretical framework of working life trajectories was outlined based on this analytic story.
Results
The participants’ stories of work participation as hearing impaired constituted working life trajectories, either towards sustainable working life participation or towards a disconnection from working life. The trajectories consisted of phases, which the participants underwent over the course of time, and contexts in which their working life experiences evolved. In the following, the contexts and the phases that constitute the trajectories are described and illustrated by citations. The term “key person” pertains to individuals, within or outside the enterprise, significant for the participants’ work performance.
The importance of context
The participants spoke of three main contexts, which played an important role in their work situation: their personal context, their workplace context, and their service provider context. During the working life course, the contexts influenced the resilience of the participants’ participation in working life. The degree of strain within the three contexts and the possible relationship between them are described in .
Figure 1. Factors influencing the degree of strain according to the contexts. Arrows indicating possible relationships between the levels of the contexts.
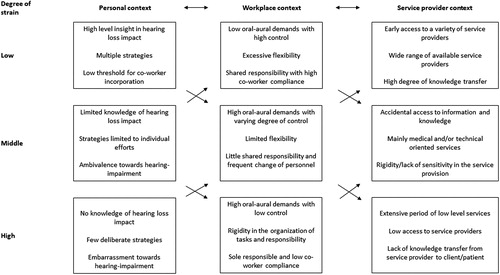
The personal context
The personal context comprised the individual situation of the participants including their individual perception of the hearing loss. Three concepts within the personal context were important to regulate the degree of strain: Knowledge of the impact of hearing loss, strategies used in dealing with the challenges, and the participant’s attitude towards the hearing loss itself.
Knowledge: At the time of onset of the hearing loss or at the time of diagnosis, the participants’ level of knowledge about possible consequences and impact of hearing loss was low. The lack of knowledge led to a low level of workplace accommodation and few adjustments, and the participants did not see the relationship between the signals of strain and the hearing impairment when such signals occurred. However, when knowledge was gained, the needs for accommodation and adjustments became clearer.
[Attending the course] first and foremost made me aware of the hearing loss. Being able to raise my voice to say: ‘I have a problem with this’. That was the primary thing. And meeting others with hearing difficulties, since I hadn’t met anyone else […] It was good to become aware, and gain the courage to talk about it at work– to tell the others what it entailed. [Attending the course] influenced my thoughts about myself, which I hadn’t really thought about before. (No. 1, female, 56–67, moderate hearing loss, two half-time positions education sector and health and care sector)
Strategies: The participants applied strategies to manage the consequences of their hearing condition depending on the perceived severity of the hearing loss and other individual needs. Visual support and strategic physical positioning were frequently used. To cope with speech perception challenges, some had adopted a highly complex analytic process of using fragments of words, sentences, and intonation, together with context, to make a puzzle of meaning. Others mainly used lip-reading, while others had few explicit strategies. The auditory capacity varied with the day-to-day health condition, where a day with less energy gave poorer hearing. Limiting strain was important, and for some, the goal of all adjustments. Severe tinnitus aggravated the circumstances of life, especially regarding the level of energy. Some perceived severe tinnitus as a bigger challenge than their hearing loss. However, tinnitus could function as an “alert lamp,” where the participants used an increase in the tinnitus as an indication of too much stress or workload.
Not only do I organise my day. I organise my time by keeping a weekly plan. I am very dependent on seeing the week as a whole. I plan the distribution of my work – so that I know when to expect the peaks. (No. 3, female, 46–55, moderate to severe hearing loss, full-time employment office and communication work sector)
Attitude: Among the participants, personal attitudes towards hearing loss varied from assertiveness, to ambivalence to embarrassment. Participants who had an assertive attitude towards the impact of the hearing loss were specific about their needs towards key persons during working hours, while ambivalent participants were selective in which occasions they would include others in solving their communication challenges. Ambivalence or a negative attitude towards ones’ own hearing loss evoked uneasiness when the hearing loss became visible, because visibility could imply unwanted attention to ones’ differentness. Assistive listening devices in particular evoked such uneasiness, together with the needs for communication measures which involved partaking of others, e.g., meeting participants having to pick up a microphone or enforcing a tight communication structure. Hence, the participants rarely used assistive listening devices, especially when communication partners had to take an active part to use such devices.
It has taken a lot of practice to dare… and to trust that I have something to offer. That I am as important as others are. That I have something to say as well. I have a right to hear. That entails placing demands upon others… it is not just my responsibility to hear what people say. It is actually the responsibility of others too. To demand from others that measures are taken and that they show consideration. Standing up and speaking up have been quite difficult. Firstly, you want to be kind of invisible, especially with such a hearing loss, and you quickly become invisible. But ironically, with my kind of disability it is very important to make yourself visible. That has been the most difficult part, to stand up for your rights and for who you are. (No. 16, female, 30–45, severe hearing loss, part-time employment education sector)
Knowledge, strategies, and attitudes were closely connected. In-depth knowledge of hearing loss and its impact on one’s life tended to advance an assertive attitude towards hearing impairment, which seemed to facilitate the development of relevant strategies, particularly the inclusion of key persons at work in the execution of accommodation measures.
The workplace context
The workplace context consisted of three main concepts, which influenced the degree of strain: oral-aural demands, flexibility, and accommodation by manager and coworkers.
Oral-aural demands: The participants described workplaces with oral communication demands challenging their speech perception abilities. A high amount of oral communication situations with a low level of structure had a negative impact. This could be a working situation with a large number of meetings with unstructured dialogues and scarce access to minutes. On the other hand, highly structured oral communication and a high degree of information given in writing had a positive impact. Having the opportunity to control the oral communication situations was also beneficial. Acting as the moderator of a meeting, using amplification devices and limiting the number of meetings were types of control that decreased demands.
I am good at writing, and my bad hearing does not restrict it. The difficult parts are projects or work tasks that entail a lot of coordination between departments and locations and video meetings. It does not work well [laughing]. […] What follows is a lot of guessing… I have to do many things off the cuff. You get good at that after a while [laughing]. I have been in all kinds of setting with hearing impairment, and have felt and thought that I do not want to experience them again. (No. 9, male, 30–45, severe hearing loss, full-time employment office and communication work sector)
The acoustic environment, such as the level of noise at the workplace and the acoustic qualities of the premises, influenced the speech perception. Noise reduction options were important to control such aural demands, i.e., being able to withdraw from noisy situations, and join meetings and lunch in adequate acoustic environments.
The oral-aural demands as described above were associated with performance and participation limitations.
Flexibility: Workplaces which facilitated a flexible way of organising the workday and the tasks, contributed to less strain among the participants. Types of flexibility were regulating working hours including taking breaks when needed, variation in the daily agenda related to oral-aural demands, and home office possibilities. Rigidity in workplace organisation gave few possibilities of recuperation during the day, and signalled a lack of recognition of one’s individual needs.
I have a good capacity for work. I really do. But I felt that I received more and more tasks, and that I stretched too far. I asked my manager if I could reduce the amount of tasks a bit. I felt that I could still work but that it was necessary to do some restructuring in the department. The manager was not willing to do that. The consequence was that I became sick-listed due to burnout because I stretched too far. It does not feel good, since I have tried to focus on solutions, and I know my work place for better and worse. I know that many tasks and routines are not taken care of, and I suggested taking on such work, to help where staff was short […]. However, the manager did not want that. It has been difficult. On some occasions, I have been invited to take part in some projects, and it has worked out well. Unfortunately, those projects have been short-term and didn’t offer a permanent solution. I have always wanted a permanent solution. (No. 10, female, 56–67, severe hearing loss, full-time employment office and communication work sector)
Accommodation by manager and coworkers: The participants were frequently alone with the responsibility of making oral communication audible. They frequently saw this responsibility as reasonable, but it became tiresome and lonely over time. Hence, managers and coworkers who engaged in finding and executing adequate measures relieved the participants of strain. Some coworkers made sure microphones were used, took notes on behalf of their coworker with hearing impairment, or in other ways made oral information more accessible. Such initiatives were warmly welcomed by most participants, and took pressure away. A manager with a positive inclination towards accommodating the work situation provided important support and signalled an acceptance of ones qualifications independent of the impairment. However, managers’ lack of knowledge about hearing impairment limited their degree of taking responsibility and initiative in the accommodation process. Most participants thought that their coworkers and manager needed information on hearing impairments. Some workplaces had frequent change of personnel, and keeping colleagues and managers updated and informed at all times was demanding and tiresome. Additionally, normal-hearing coworkers tended to quickly forget the specific needs, and the participants had to repeat this information regularly.
The IT department has really helped me and it still does. They have assistive listening devices and video magnifiers. Every time that there were large lectures the IT-department handled the presentations and microphones and so on. In addition, they always reserved a seat in the front for me, so that I could both hear and see. They did that in such a laid-back way. I never had to ask for it. They still do it, after all these years. That is admirable of them, very gratifying. (No. 7, female, 46–55, moderate hearing loss, tinnitus, full-time employment office and communication work sector)
Consequently, the participation possibilities were formed by the degree of oral-aural demands. However, the degree of demands was reduced with accommodation offered by manager and coworkers and with the degree of flexibility in the work situation. High degree of accommodation by manager and coworkers and flexibility reduced the oral-aural demands and thus, limited the strain.
The service provider context
The service provider context constituted of three main concepts, which played an important role in the participants’ encounter for the services to be perceived as adequate and contribute to reduce strain: access to services, extent of services, and proficiency in the execution. This context included general and specialised health services, as well as welfare services.
Access: Access to service provision was associated with information about the existence of a specific service provider. At the early stage of the adult-onset hearing loss, the participants reported mainly access to medical follow-up and hearing aid fitting. Frequently, a long period of time had elapsed without further service provision. Typically, different needs, in or outside work, would surface during the course of time, but the participants had rarely enough knowledge about existing providers to request support or to see the connection between the needs and the hearing loss. For many, the discovery of service providers was a coincidence, for instance from a peer or a coworker who randomly shared useful information about accommodation possibilities and relevant service providers.
I think it was that nurse [at a rehabilitation course] who told me about it. […]She had hearing difficulties herself and thus paid attention to the issue for her clients. […] Without her, I think I would not have had assistance with a hearing aid in quite a few years. I had come to terms with the fact that tinnitus was something you got and that you just carried on. There is nothing to be done. […] So, I was actually very lucky. (No. 11, female, 56–67, slight hearing loss, tinnitus, full-time employment office and communication work sector)
Extent: Participants talked about the usefulness of having access to a variety of professionals, both audiologically trained and other professionals such as physiotherapists and psychologists, in order to develop a sustainable work situation. Different professional approaches, when the information was both abundant and specific, gave broader perspectives and knowledge that was more thorough. It tended to result in an extensive selection of tools, such as measures for noise and strain protection. The participants used these tools to find efficient and individually suitable measures in coping with their working life challenges as hearing impaired. Especially, participants with severe tinnitus benefitted from extensive training in dealing with the unwanted sound in general. Moreover, the participants found access to peers, in addition to professionals, valuable, were the most important benefits were sharing of experiences and a feeling of fellowship.
[For two years] I put a lot of effort into attending courses […] It included mindfulness and “find your peace”, which I obviously needed. I attended practically oriented [courses] regarding assistive devices. I desperately craved something that could help me have a better everyday life. I joined all kinds of Facebook groups to see how other people were trying to cope. The sum of all of that and that I was granted one treatment day per week, as well as receiving physiotherapy […] all of that is the reason that I can manage. (No. 7, female, 46–55, moderate hearing loss, tinnitus, full-time employment office and communication work sector)
Proficiency: The participants were concerned about the proficiency in the execution of services when meeting with professionals, both in health care and welfare. In proficiency, they included the professional’s ability to detect individual needs and finding a flexible way of reaching the goal of the services. Some participants claimed that encounters with professionals should be characterised by dialogue and transmission of knowledge from the professional (e.g., an audiologist or a case manager) to the participant. Rigid ways of handling the process could increase the strain. The effort would then be used on fulfilment of the demands from the service providers instead of on improving health and work ability. Encounters without dialogue and transmission of knowledge were experienced as particularly exhaustive for participants on long-term sick leave or with fatigue.
The path has taken seven years – to have the Labour and Welfare Administration accept and recognise me as a working member of society. It has been quite hard sometimes, because the system is difficult and slow. It goes slowly, and you have to meet so many people and attend so many meetings and centres, and you must try and fail so much. […] I have been tested in many work situations, been to lectures, career counselling, and work-related rehabilitation. I must have tried everything there is to try. I knew myself and that my goal had to be disability pension. If I could manage to work 50%, then that would be my contribution in life. That is what I can give to society. […] The Labour and Welfare Administration didn’t agree, of course […] And I did what they told me. ‘Try this, try this, try this’, and I tried everything. I attended every meeting, and I attended every consultation. Every time it ended with: ‘No, maybe it wasn’t the right thing for you’. At the end, they actually didn’t have more alternatives. At that time, my general practitioner, a psychologist, and the head physician at the ear-nose-throat department had sent documentation that I should be granted disability pension. It took about a year before the application answer arrived […] that I was granted 50%. A huge burden was taken off my shoulders. I could concentrate on the 50% part, not on everything else. I could finally go all in at work, feel that I was doing my part. It was a very good feeling – to be recognised for who I am. (No. 16, female, 30–45, severe hearing loss, part time employment education sector)
Participants who had a network of supporters, both professionals and nonprofessionals, felt assured in their daily life, knowing that assistance was at hand whenever problems would occur. Participants without a supporter network were, on the other hand, far more vulnerable and at the mercy of one’s own initiative and endurance.
Forming trajectories through phases
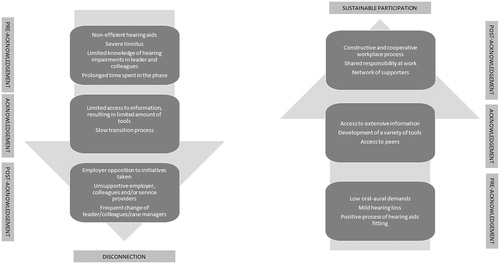
The working life trajectories evolved through three phases of acknowledgement of the impact of the hearing loss: Phase 1: pre-acknowledgment, phase 2: acknowledgement, and phase 3: post-acknowledgement. Different influential factors during the phases affected the direction of the trajectories either towards sustainability of work or towards disconnection. In the following, the three phases are presented chronologically, including influential factors and trajectory outcomes (see ).
Figure 2. Influential factors in working life trajectories.

Phase 1: Pre-acknowledgement
The pre-acknowledgement phase started with the time of onset of the hearing loss. Participants with adult-onset hearing loss were often unaware of the time of onset, but had in retrospect frequently a notion of an extended period before they had their hearing loss diagnosed. Having the hearing loss diagnosed and hearing aids fitted did not lead to acknowledgment in itself, but rather to a period continuing as usual while adapting to the hearing aids. Participants with childhood-onset hearing loss had also experienced the same pre-acknowledgment phase when they had limited interventions during childhood and education, resulting in limited knowledge about the hearing loss. Consequently, they would not have prerequisites to make informed choices on education and work concerning their hearing loss and its impact.
The degree of strain during this phase depended on the degree of hearing loss and the type of work. The level of strain the participant experienced () influenced how much energy and time the participant spent in this phase. Lack of knowledge in both the personal and the workplace context resulted in few prerequisites for initiating change. Hence, neither the participants nor their manager requested support from service providers.
It was not until 2008, when my problems become so grave, when the tinnitus and the hearing had become worse, that I went to see a doctor. At that moment, it was so troubled… I managed my job, but I was so tired when I got home. I had no energy, and I was irritable and short-tempered. […] I was offered a stay at [a rehabilitation centre], a course for mastering tinnitus. [...] I learned a lot there […] I learned what tinnitus is and what it does to you. That was a revelation. […] I understood that the hearing loss and the aggravated tinnitus was a stress factor – I had to be told that – a nurse who said: ‘Are you aware of how much energy you spend on hearing?’ Then I started to think – that it is associated with a tight neck, which I have suffered from for a long time. I had hearing troubles earlier, but hadn’t seen the connection, and that it can result in difficulties with concentrating. Having a job in which you need to keep up – it affects the tinnitus, like a volume button, and it increases. […] It was only after the stay [at the rehabilitation centre] that I started to realise how much the hearing problems affected my everyday life. (No. 12, male, 56–67, moderate hearing loss, severe tinnitus, in disability assessment, office and communication work sector)
Influential factors. Mild hearing loss and low oral-aural demands were important protective factors in this phase, while troublesome tinnitus and poorly fitted hearing aids were important risk factors. Furthermore, spending an extended period of time in the pre-acknowledgement phase constituted a risk of an accumulation of strain, especially with high oral-aural demands. The most important factor in limiting the duration and the negative impact of this phase was the participants’ experience of proficiency in the audiological encounter. A process with little knowledge transfer and limited dialogue in the fitting-process was common and could result in an adverse effect on the self-efficacy, limiting the access to tools to bring into the workplace. In this case, the pre-acknowledgement phase stabilised and lasted for years. The toil during a long-lasting pre-acknowledgement phase lead to exhaustion and/or sick leave in some participants.
Phase 2: Acknowledgement
The acknowledgement of the impact of the hearing loss started as a growing sense of awareness and constituted a life course transition. Prior to the transition a need for change evolved as the level of strain increased. Some experienced a period of long-term sick leave or a sense of fatigue or burnout, which initiated the process. The participants started with a search for knowledge or they accidentally got access to information on relevant hearing loss matters, such as courses with various relevant subjects. Through access to broad information from various professions and meeting peers in the same situation, the connection between their daily life struggles and the hearing loss was established. The knowledge gained was used to create a personal toolbox in order to deal with the challenges.
A life course transition, which reduced the level of strain in the personal context (as described in ), was a good starting point for initiating constructive changes. Through knowledge and contact with peers, negative attitudes were altered and broader strategies were developed. Thus, a favourable situation was created where the hearing loss could be incorporated as an accepted part of the working situation.
It is about learning relaxation techniques, not doing things you don’t have to engage in. I was very enthusiastic earlier, socially minded, my thoughts were always ahead of what I was doing. That is OK, but when you can’t bear it, you can’t bear it. When you get home and you realise ‘Oh s***, now it’s whistling [in your ears]. You understand that your head is stressed. To practise to reduce the stress in your head… we work a lot on that. Use nature a lot. Actually, I have started to kayak. That experience was an eye-opener. I had to sell my motor boat since it made too much noise, and I didn’t think it was possible to have a life without a boat. I have always had a boat. […] Getting out into nature […] and you notice ‘God, now it doesn’t bother me that much’. […] I have never experienced that before. I have always been accompanied by the sounds of the things that I have done, boats and all that… sound, sound, sound, model plane, racing cars, always sound. The quietness, the here-and-now stuff, mindfulness, oh gosh, what good it has done for me. […] Now it is actually possible to live with this. (No. 14, male, 56–67, moderate hearing loss, severe tinnitus, in disability assessment, practical work/support sector)
Influential factors. Extended and highly accessible information was an important protective factor. Through extensive knowledge, a deeper insight into the hearing loss impact developed. If information was not abundant, the knowledge tended to evolve slowly and the process would halt before thorough insight was gained. Adequate measures were taken, but they were less extensive, and the transition could stop and restart at a later point in time prolonging the process and not sufficiently reducing the degree of strain.
Phase 3: Post-acknowledgement
The quality of the post-acknowledgment phase depended on how the accommodation suggestions were met by the manager and the service providers involved. If the manager had a positive inclination towards the initiatives taken, a constructive and cooperative process started to find adequate measures. If the manager took little interest in or was opposed to accommodation measures, the process stopped and change was less likely. This would add to the strain and to the risk of disconnection. Having access to adequate service provision influenced the post-acknowledgement phase positively. To find and to build up the relevant network formed a basis at which the participant could stand firmly during working life.
We [the participant and the manager] had meetings about adjustments of different work tasks and stuff like that. What he always said was ’Teaching is what we do here’. […] He did not really understand what kind of duties a manager has […] I spent a lot of effort showing him… in addition to the fact that I was tired already. I felt that I constantly had to show him that I was entitled to this and that it had to be sorted out. I felt quite alone […] When I finally realized the situation I talked to the employee representative and then the head safety delegate, and they joined me at all meetings. That is the smartest thing that I have ever done. […] I can’t attend meetings alone with a manager who doesn’t know the right time to strike. (No. 8, female, 56–67, moderate hearing loss, part-time position education sector)
Influential factors. Shared responsibility of finding and implementing relevant measures was an important protective factor, which reduced strain and helped sustain the labour market participation. Solitary responsibility, on the other hand, increased the risk of discouragement and disconnection. If either the workplace or service provider context was reluctant or unsupportive, it resulted in added strain and discouragement. The previous exhaustion would be prolonged increasing the risk of disconnection from the labour market.
Additionally, change of colleagues or managers had a potentially adverse effect. New coworkers meant frequent repetition of information, while change of manager meant starting afresh with creating understanding for their specific needs. It also meant an additional uncertainty of whether accommodation measures could be withdrawn, or if a constructive relationship could be established. Changing case officer or having multiple case officers also meant explaining one’s needs repeatedly with a risk of not succeeding. This could have an adverse effect on the adequacy of the services given, such as having suitable welfare benefits withdrawn.
A serious risk factor was long-lasting severe tinnitus. To cope with severe tinnitus a high level of knowledge was necessary, but not sufficient. A high flexibility level at work, allowing for a variety of measures to reduce strain, was equally important. Still, severe tinnitus was a high-risk component for disconnection even in adequately functioning workplaces.
Outcome of working life trajectories
To have a vocational affiliation was described as important to all participants. Disconnection from working life was perceived as a last resort and was associated with grief and a feeling of inadequacy, also for those with a partial disconnection in combination with disability or welfare benefits. Finding ones limit of endurance concerning working hours within an acceptable auditory environment was crucial to sustain participation.
The two possible outcomes of the working life trajectories, sustainable working life participation or a disconnection, are illustrated in . Sustainable vocational participation was associated with balancing the level of strain without making the job less interesting. On the other hand, the risk of disconnection increased when the hearing impairment was not an integrated part of the daily working situation. The situation would then be characterised by insecurity, solitude, and unnecessary toil.
Figure 3. Outcome of working life trajectories through the phases of acknowledgement.
Disconnecting trajectories
An accumulation of risk would constitute a strenuous working situation and increase the likelihood of entering disconnecting trajectories. Remaining ignorant of how hearing loss could have an impact on life hindered a development of suitable and sufficient coping strategies. Such ignorance maintained ambivalence or negative attitudes towards hearing impairments. Service provision encompassing technical assistance only, such as hearing aids, limited the possibility of developing further knowledge and strategies. When a low level of knowledge endured over time the risk of fatigue increased. An unengaged manager reduced the possibility to implement adequate measures and possible adjustments became marginal. Lack of knowledge by managers narrowed the room for manoeuvre, while lack of knowledge in coworkers meant having to repeat hearing loss needs frequently. Change of manager or case-officer created uncertainty about future maintenance of accommodation measures.
I spent so much energy at work to fulfil the goal I had aimed at, to convince myself and others that it was possible, that I was like a worn-out rag when I was at home, and not possible to contact that much. I slept a lot, on the couch. I had dinner, and then I was just gone. And it was not a break of fifteen minutes like I can have now. It could be two hours actually, it could be three hours. […] I am proud because I convinced myself and others, but I am disappointed with myself because I actually put the wrong priority on the values that are the far most important in life. (No. 4, male, 56–67, cochlear-implant user, full-time position office and communication work sector)
Sustainable trajectories
An accumulation of facilitating factors supported sustainable trajectories. An acknowledging attitude towards the hearing situation seemed to constitute a safe platform for handling the work situation. This attitude tended to invite key persons into joint efforts towards a manageable daily life. Acknowledgement was reached through knowledge rather than experience, and a wide range of professionals facilitated the acknowledgment process and served as a security net for future challenges. Access to peers reduced the sense of loneliness through the fellowship and sharing of experiences. A high degree of flexibility in shaping the work schedule and accomplishing the work tasks was important in maintaining a low degree of strain.
If I am to sum it up, I am obviously in a very favourable situation. Suppose that I had had to be at school 100%, then the strain would have felt a lot worse. […] Then I believe I would have ended up with a graded [position] of some kind, and then I think I would have at least been tempted to take partial AFP [contractual early retirement scheme] or something like that. […] Because then I would have had so many daily situations that I would have perceived as challenging and stressing to say the least. And what is difficult with stress you know – how are you going to understand it – is it the hearing capacity, or is it me as a person, or is it my way of thinking at base? And it is entirely impossible to find an exact answer to that, and then maybe you will feel that you have to defend something all of the time. (No. 1, female, 56–67, moderate hearing loss, two half-time positions education sector and health and care sector)
Discussion
The aim of this study was to identify and explore factors that facilitate or hinder work participation, as described by employees with hearing impairments. The analysis resulted in a conceptual framework of working life trajectories evolving through three phases of acknowledgement of the impact of the hearing loss. The phases were influenced by the qualities of three contexts: the personal, the workplace, and the service provider. The qualities of the contexts, together with the amount of time spent in a pre-acknowledgement phase, formed the trajectories towards continuation of work participation or towards a disconnection. Accumulated risk factors increased the likelihood of disconnecting trajectories, while accumulated facilitating factors supported sustainable trajectories.
An important barrier to participation found in this study was spending a long time in the pre-acknowledgement phase. Previous studies have shown that accepting a hearing loss frequently takes time for individuals with acquired hearing loss [Citation20,Citation21]. The time spent has been described as a process from avoidance to acceptance where key persons could facilitate the process [Citation20]. A study among working-age adults with acquired hearing loss found that the participants had mainly been persuaded into hearing assessment by key persons [Citation21]. Two different trajectories were described in early hearing correction, where one was embedded in social pressure and the other as a situational sense of need where the hearing problem was located in the periphery of their lives. Thus, the participants’ perspective of their hearing loss was not restricted to the disease, and could not be solved by a medical solution [Citation21]. This study showed a somewhat similar process from reluctance towards an awakening in the pre-acknowledgement phase. A lack of acceptance and acknowledgement could prevent initiation of accommodation processes and thus be a barrier to fatigue prevention.
We also found that lack of knowledge of the impact of hearing loss was an important barrier in reaching acknowledgement. Such knowledge tended to be a key to self-efficacy, but was frequently accessed coincidentally. A lack of access to knowledge of how to enable efficient work accommodation processes in employees with hearing impairments has been found previously [Citation22]. Thus, to avoid exhaustion it seems pivotal to access knowledge earlier and thus limit the time spent in the pre-acknowledgement phase. Systematic follow-up is needed to secure knowledge transfer. Additionally, the follow-up has to encompass the process of avoidance-acceptance to succeed with knowledge transfer.
In this study, we found that flexibility and accommodation offered by manager and coworkers were important facilitating factors. However, the flexibility and accommodation by manager and coworkers tended to be restricted to task adjustments and occasional communication adaptations normally without the use of assistive listening devices. A cross-sectional study in Norway also found a low use of assistive listening devices (18.9%) additional to hearing aids among persons with hearing impairments in working age [Citation14]. The same study also found that 30.7% reported to be in need of hearing related accommodation without receiving it. Thus, we hypothesise that there is an unexploited room for manoeuvre in reducing strenuous working conditions among employees with hearing impairments. A systematic follow-up using knowledge on the impact of hearing loss would improve the prerequisites for initiation of adequate measures.
We found that the participants were reluctant to cause inconvenience when considering accommodation measures. Measures that implied actions from others were often considered inappropriate or embarrassing. Previous studies have addressed the subject of willingness to request accommodation among employees with hearing impairments [Citation23–26]. Baldridge and Veiga [Citation23] claimed that there are reasons to believe that people with disabilities often withhold requests for useful accommodation despite their right to claim it. They presented a conceptual framework consisting of nine propositions concerning the requester’s beliefs about pros and cons of making the requests, which contributed to a request likelihood. For instance, an accommodation measure or a request for such might make the disability more visible and by such potentially lead to a negative assessment from colleagues and the manager (“anticipated image cost”). Moreover, receiving additional advantages over colleagues would be perceived as unjust. Thus, to increase the request likelihood the requester must perceive the need as a sufficient reason for the fairness (“perceived fairness”). The reluctance and embarrassment found in this study might be interpreted as “anticipated image cost” and “perceived fairness,” and as such functioning as barriers to adequate accommodation processes. Furthermore, anticipated social consequences were important factors when deciding on whether to make a request or not for recurring needs [Citation24]. Particularly difficult was the imposition which the request put on others, because the colleagues and manager were exposed to a repeated burden [Citation24]. Difficulties concerning recurring communication needs were an issue in this study as well. Hearing loss is a permanent condition, and accommodation needs will inevitably be recurrent. Thus, this is a factor which needs to be addressed in a follow-up process. Receiving assistance in the accommodation process when assessing measures could relieve the employee with hearing impairment of responsibility. Furthermore, the assistance needs to encompass how to avoid an actual loss of image and increase the colleagues’ perceived fairness if the measures involve special treatment.
The role of aural rehabilitation in sustainable participation
The lack of access to adequate service providers, particularly, services with audiological knowhow, was a major barrier to sustainable participation, thus confirming previous research [Citation22]. Danermark and Gellerstedt [Citation27] found in a cross-sectional study that employees with hearing impairments reported higher demands and lower control in stressful work than their normal-hearing peers, and the authors claimed a need for more intense aural rehabilitation. In a qualitative study, three narratives revealed gaps in services and supports [Citation28]. Professional assessment of the impact of the hearing loss at the workplace had not been performed in these cases, and the authors requested appropriate tools for such assessment together with educational programmes for stakeholders. In a qualitative study on conceptions of working life among employees with mild-moderate hearing impairment, Hua et al. [Citation29] argued that there is a need for extensive services after hearing aid fitting also for this group due to the impact of the hearing loss on the work situation.
This study showed that few participants had access to a variety of supporters, and that referral to aural rehabilitation measures other than hearing aid fitting was rare. A lack of such rehabilitation measures in Norway has been described in public reports over the years [Citation30]. A systematic review of vocational rehabilitation services for hearing loss found that statistical evidence for the effectiveness of the vocational rehabilitation programmes was scarce [Citation31]. The authors questioned if programmes directed at the employee with hearing loss alone would meet the needs of the employee in the most efficient and appropriate way. Three programmes in the review had an integrated approach where stakeholders in the workplace were included in the process to increase implementation likelihood of suggested accommodations. One of the programmes included in the review was a multidisciplinary vocational enablement protocol in the Netherlands [Citation32]. The protocol was implemented in a Dutch audiological centre, and the majority of the patients reported that it facilitated work participation. The effectiveness of the Dutch vocational enablement protocol was measured in a randomised controlled trial [Citation33]. No differences were found between the groups apart from a minor increase in “self-acceptance” in the intervention group. The authors pointed to the low implementation rate of the advices provided as one explanation for the lack of effect. Further, they suggested that the implementation rate could have increased with a closer contact with relevant stakeholders at the workplace. This argument is in line with Danermark and Gellerstedt [Citation27], who claimed a need for more intense aural rehabilitation and that there ought to be coordination between the clinical audiological rehabilitation and the rehabilitation at the worksite. Kramer [Citation32] as well argued that it is of great importance to perform an extensive evaluation of the workplace, the tasks, and the workplace conditions because hearing status and job title do not provide sufficient information per se. Hence, a more integrated approach involving managers and other stakeholders in vocational rehabilitation are needed.
Hearing loss occurs in a wider social context as it affects both the person with hearing impairment and the communication partner [Citation34]. This study has pointed to a need for having a wider perspective on vocational participation of employees with hearing loss. Stakeholders at work and service providers should play a more prominent part in the accommodation process. A multidisciplinary approach at the worksite could benefit employees with hearing impairment in reducing strain at work.
Strengths and limitations
Recruiting participants through the Norwegian Association of the Hearing Impaired was done with the intention of reaching a wide range of people of working age with hearing loss. In Norway, this is only efficiently done through their own organisation. Members of a special interest organisation might not be representative of the target population by e.g., being more knowledgeable about their situation than nonmembers. However, the Norwegian Association of the Hearing Impaired has a large number of members. This might partly be explained by a compensation arrangement if hearing aids are lost, which they offer their members, and new hearing aid users are routinely informed about this arrangement.
The participants represent different educational areas and managerial levels, but unfortunately, we did not succeed in recruiting self-employed participants, or traditional blue collar workers. Thus, their experiences are not represented, which might have limited the range of experiences. However, one participant had worked in a factory for many years. Due to a noise-induced hearing loss, he had been transferred to perform support tasks in the same company. Among our participants, there was a majority who experienced their manager as somewhat positive towards accommodation matters. We cannot say if this reflects the general attitude in the Norwegian labour market or is due to the recruitment process. Further, health conditions other than hearing loss may influence work performance. Such information has not been available in this study and may be considered a limitation.
The life course perspective as described in Amick et al. [Citation19], was an appropriate gateway to the analysis of this study. Particularly the concepts of trajectories and contexts were adequate within these narratives. However, the complete life course perspective as Amick et al. [Citation19] employed was beyond the scope of this article since our narratives were limited to hearing loss matters in a life course perspective. Furthermore, the contexts could have been elaborated further. For instance, the service provider context could be expanded to a societal context including legislation, political incentives, and other distant factors influencing the working conditions. Similarly, the concepts in the workplace context could be described more thoroughly through sub-concepts. However, we consider that the account given of the contexts here covers the most significant experiences and hence depicts their importance.
The first author is trained as an educational audiologist and has long-term experience in working with people with hearing impairments, implying a position as an informed outsider as an interviewer and throughout the analysis process. Being informed implies insight into the issues in question and thus the possibility to pursue important subjects when arisen, while being an outsider implies a necessary emotional distance to the theme. Nevertheless, previous experiences may intervene and disturb in both the interviewing and the analysis resulting in a search for ones’ own prejudices. In this study, an unprejudiced attitude was pursued through performing as unstructured interviews as possible. Additionally, thorough notes on experiences and prejudices were written down in advance. A wider perspective was also secured by being two individuals throughout parts of the analysis process.
Conclusions
This study confirms previous research showing that hearing impairment is a strenuous condition which may have adverse effects on work participation. Lack of knowledge on the impact of hearing loss tended to be a barrier to satisfactory accommodation processes. Access to service providers who transferred knowledge on hearing loss impact tended to be a prerequisite for gaining acknowledgement of the condition and its impact. The knowledge gained was facilitating an accommodation process including key persons at the workplace. Thus, there is a need for extended support at the workplaces, which includes the manager, colleagues, and professionals in the aim of preventing exhaustion and facilitates work participation among employees with hearing impairments. Joint action in facilitating communicative participation would share the responsibility for accommodation measures and broaden the room for manoeuvre at the workplace.
Supplementary Interview_guide.docx
Download MS Word (13.7 KB)Acknowledgements
The authors would like to thank researcher Jorunn Solheim, Ph.D., Lovisenberg Diakonale Hospital, for her constructive contributions to the research process.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
Related Research Data
References
- WHO. World report on disability. Geneva, Switzerland: World Health Organization; 2011. p. 350.
- Emmett SD, Francis HW. The socioeconomic impact of hearing loss in U.S. adults. Otol Neurotol. 2015;36:545–550.
- Jung D, Bhattacharyya N. Association of hearing loss with decreased employment and income among adults in the United States. Ann Otol Rhinol Laryngol. 2012;121:771–775.
- Helvik AS, Krokstad S, Tambs K. Hearing loss and the risk of disability pension in Norway: the Hunt Study. Scand J Public Health. 2013;41:818–824.
- Kramer SE, Kapteyn TS, Houtgast T. Occupational performance: comparing normally-hearing and hearing-impaired employees using the Amsterdam Checklist for Hearing and Work. Int J Audiol. 2006;45:503–512.
- Carlsson PI, Hjaldahl J, Magnuson A. Severe to profound hearing impairment: quality of life, psychosocial consequences and audiological rehabilitation. Disabil Rehabil. 2015;37:1849–1856.
- Stam M, Kostense PJ, Festen JM, et al. The relationship between hearing status and the participation in different categories of work: demographics. Work. 2013;46:207–219.
- Helvik AS, Krokstad S, Tambs K. Hearing loss and risk of early retirement. The HUNT study. Eur J Public Health. 2013;23:617–622.
- WHO. Deafness and hearing loss World Health Organization. 2017 [updated 2017 Feb; cited 2017 Sep 19]. Available from: http://www.who.int/mediacentre/factsheets/fs300/en/
- Lin FR, Niparko JK, Ferrucci L. Hearing loss prevalence in the United States. Arch Intern Med. 2011;171:1851–1853.
- Engdahl BL. Fakta om hørselstap/døvhet/hørselshemming [Facts on hearing loss/deafness/hearing impairment]. Norwegian Institute of Public Health. 2015 [cited 2017 Sep 19]. Available from: https://fhi.no/hn/eldre/horselstap—faktaark/
- Hasson D, Theorell T, Westerlund H, et al. Prevalence and characteristics of hearing problems in a working and non-working Swedish population. J Epidemiol Community Health. 2010;64:453–460.
- Nachtegaal J, Kuik DJ, Anema JR, et al. Hearing status, need for recovery after work, and psychosocial work characteristics: results from an internet-based national survey on hearing. Int J Audiol. 2009;48:684–691.
- Svinndal EV, Solheim J, Rise MB, et al. Hearing loss and work participation: a cross-sectional study in Norway. Int J Audiol. 2018. DOI:10.1080/14992027.2018.1464216
- Punch R. Employment and adults who are deaf or hard of hearing: current status and experiences of barriers, accommodations, and stress in the workplace. Am Ann Deaf. 2016;161:384–397.
- Coniavitis Gellerstedt L, Danermark B. Hearing impairment, working life conditions, and gender. Scand J Disabil Res. 2004;6:225–245.
- Patton MQ. Qualitative research & evaluation methods. 3rd ed. Thousand Oaks (CA): Sage Publications; 2002.
- Corbin J, Strauss A. Basics of qualitative research. Techniques and procedures for developing grounded theory. 3rd ed. Thousand Oaks (CA): Sage Publications; 2008.
- Amick BC, McLeod CB, Bultmann U. Labor markets and health: an integrated life course perspective. Scand J Work Environ Health. 2016;42:346–353.
- Wänström G, Öberg M, Rydberg E, et al. The psychological process from avoidance to acceptance in adults with acquired hearing impairment. Hearing Balance Commun. 2014;12:27–35.
- Hindhede A. Everyday trajectories of hearing correction. Health Sociol Rev. 2010;19:382–394.
- Shaw L, Tetlaff B, Jennings MB, et al. The standpoint of persons with hearing loss on work disparities and workplace accommodations. Work. 2013;46:193–204.
- Baldridge DC, Veiga JF. Toward a greater understanding of the willingness to request an accommodation: can requesters’ beliefs disable the Americans with Disabilities Act? Acad Manag Rev. 2001;26:85–99.
- Baldridge DC, Veiga JF. The impact of anticipated social consequences on recurring disability accommodation requestst. J Manage. 2006;32:158–179.
- Baldridge DC, Swift ML. Withholding requests for disability accommodation: the role of individual differences and disability attributes. J Manage. 2013;39:743–762.
- Baldridge DC, Swift ML. Age and assessments of disability accommodation request normative appropriateness. Hum Resour Manage. 2016;55:385–400.
- Danermark B, Gellerstedt LC. Psychosocial work environment, hearing impairment and health. Int J Audiol. 2004;43:383–389.
- Jennings MB, Shaw L. Impact of hearing loss in the workplace: raising questions about partnerships with professionals. Work. 2008;30:289–295.
- Hua H, Anderzen-Carlsson A, Widen S, et al. Conceptions of working life among employees with mild-moderate aided hearing impairment: a phenomenographic study. Int J Audiol. 2015;54:873–880.
- Helsedepartementet, Sosialdepartementet. Et helhetlig rehabiliteringstilbud til hørselshemmede. Plan for utvikling og organisering av tjenestetilbudet [A comprehensive rehabilitation service for hearing-impaired. Plan for development and organization of services]. 2002.
- Gussenhoven AH, Jansma EP, Goverts ST, et al. Vocational rehabilitation services for people with hearing difficulties: a systematic review of the literature. Work. 2013;46:151–164.
- Kramer SE. Hearing impairment, work, and vocational enablement. Int J Audiol. 2008;47:S124–S130.
- Gussenhoven AHM, Anema JR, Witte BI, et al. The effectiveness of a vocational enablement protocol for employees with hearing difficulties: results of a randomized controlled trial. Trends Hear. 2017;21:233121651769230.
- Barker AB, Leighton P, Ferguson MA. Coping together with hearing loss: a qualitative meta-synthesis of the psychosocial experiences of people with hearing loss and their communication partners. Int J Audiol. 2017;56:297–305.