
Abstract
Purpose: Evidence for efficacy of early intervention in infants at high risk of cerebral palsy (CP) is limited. We compared outcome of infants at very high risk of CP after receiving the family centered program COPing with and CAring for infants with special needs (COPCA) or typical infant physiotherapy.
Materials and methods: Forty-three infants were randomly assigned before the corrected age of 9 months to 1 year of COPCA (n = 23) or typical infant physiotherapy (n = 20). Neuromotor development, cognition, and behavior was assessed until 21 months corrected age. Video-recorded physiotherapy sessions were quantitatively analyzed for further process analyses. Outcome was evaluated with nonparametric tests and linear mixed effect models.
Results: During and after the interventions, infant outcome in both intervention groups was similar [primary outcome Infant Motor Profile: COPCA 82 (69–94), typical infant physiotherapy 81 (69–89); Hodges Lehman estimate of the difference 0 (confidence interval −5;4)]. Outcome was not associated with contents of intervention.
Conclusions: One year of COPCA and 1 year of typical infant physiotherapy in infants at high risk of CP resulted in similar neurodevelopmental outcomes. It is conceivable that combinations of active ingredients from different approaches are needed for effective early intervention.
For infants at very high risk of cerebral palsy, 1 year of intervention with the family-centred programme Coping with and Caring for infants with special needs resulted in similar infant outcome as 1 year of typical infant physiotherapy.
Infant’s neuromotor, cognitive, and behavioural outcome was not associated with specific interventional elements, implying that the various elements may have a similar effect on developmental outcome.
We suggest that a specific mix of ingredients of different approaches may work best, resulting in comprehensive care including both infant and family needs.
IMPLICATIONS FOR REHABILITATION
Introduction
In general, infants at risk for neurodevelopmental disorders such as cerebral palsy (CP) receive early intervention in middle and upper income countries. Many different intervention programs exist. Gradually our knowledge on the effect of early intervention increased. Post-discharge early intervention programs for premature infants showed positive effects on cognition at preschool age, but effects on motor development are limited [Citation1]. Prematurity is one of the risk factors for developing CP, but—fortunately—only a minority of premature infants develop CP. Additional risk factors for developing CP are serious brain lesions, such as periventricular leukomalacia or a cerebral infarction [Citation2]. Currently, little is known about the effects of early intervention in such infants at very high risk of CP.
Recently, two systematic reviews [Citation3,Citation4] addressed the effect of early intervention in infants at high risk of CP. They concluded that limited evidence for the effect of early intervention in high-risk infants is available, as only a few studies have been performed that applied various interventions and usually suffered from a lack of power and other methodological shortcomings. Both reviews suggested that a combination of interventional ingredients might be most promising for a beneficial effect, but opinions on the nature of the ingredients varied. This means that additional information on the effect of early intervention in high risk infants is needed.
In the first decade of the 21st century, a new intervention program has been developed in The Netherlands: COPCA, COPing with and CAring for Infants with special needs—a family centered program [Citation5]. COPCA has two main components: (1) a family and educational component and (2) a neurodevelopmental component. The first component stresses family autonomy and coaches families to cope with their situation and make their own decisions [Citation6]. The second component addressing neurodevelopment is based on the Neuronal Group Selection Theory [Citation5,Citation7]. This component aims to increase the size of the motor repertoire (variation) and to enhance adaptability in an active learning process with trial and error experiences.
Previously we performed an RCT on the effectiveness of a 3-month period of COPCA intervention in comparison to typical infant physiotherapy, the Vroegtijdig Interventie Project (VIP) project [Citation8,Citation9]. Typical infant physiotherapy in the Netherlands is an eclectic mix of different approaches and theories, traditionally based on NeuroDevelopmental Treatment principles. However, over time, a more functional approach with more family involvement, has been integrated resulting in a heterogeneous mix of physiotherapy ingredients [Citation5]. The standard RCT design was combined with a detailed process analysis of the interventions. At RCT level, both intervention groups developed similarly. Process analysis revealed that contents of intervention was associated with outcome, especially in the subgroup of infants diagnosed with CP. Challenging the infant to explore and try out its own motor actions, and coaching the family were positively associated with motor outcome, whereas sensory experience was negatively associated with motor outcome. However, only about a quarter of the children were diagnosed with CP. Therefore, we embarked on another intervention study in infants at higher risk of CP, the LEARN2MOVE 0–2 years (L2M0–2) study [Citation10], using a similar double approach of RCT design and process analysis of the COPCA and typical infant physiotherapy interventions. COPCA and typical infant physiotherapy were now applied for a longer period: one year. Outcome was evaluated in a broad way, including child (neuromotor, cognition, and behavior), functional (daily life, activities and participation), and family outcome (e.g., family empowerment, coping) [Citation10]. In this article, we report the infant’s neuromotor, cognitive, and behavioral outcome. In our accompanying article [Citation11], we address family outcome and the child’s activities and participation.
Our research questions for this study are: (1) do infants at high risk of CP receiving COPCA or typical infant physiotherapy differ in neuromotor, cognitive, or behavioral outcome; (2) are specific physiotherapy actions related to child’s neuromotor, cognitive, or behavioral outcome; and (3) does the nature of the brain lesion, and especially the most severe brain lesion cystic periventricular leukomalacia [Citation12], affect the effect of intervention? We hypothesized that no or minor differences between COPCA and typical infant physiotherapy are present at RCT level on infant outcome measures, due to heterogeneity in interventions and knowledge from other intervention trials. We hypothesized on the basis of our previous trial [Citation5,Citation8] that specific physiotherapy actions—such as coaching and challenging—will be positively related to the infant’s outcome. Finally, we expected that early intervention has least effect in infants with more severe brain lesions, as we assumed that a more affected brain will have less capability to reorganize or compensate.
Materials and methods
Participants
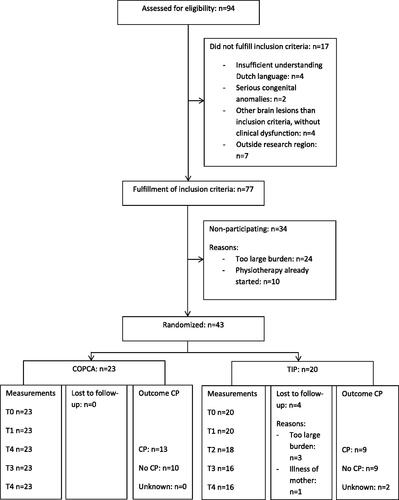
Infants were eligible for the study when they presented between 0 and 9 months corrected age at very high risk of CP. The latter meant the fulfillment of one of the following criteria: (1) cystic periventricular leukomalacia; (2) parenchymal lesions as result of infarction or hemorrhage; (3) severe asphyxia with brain lesions on magnetic resonance imaging; or (4) clinical dysfunction suspect for development of CP. Exclusion criteria were (1) insufficient understanding of the Dutch language; or (2) severe congenital anomalies. Infants were recruited between November 2008 and November 2013 by pediatricians, child neurologists, and physiotherapists from 12 hospitals in the northern half of the Netherlands. Seventy-seven infants fulfilled the inclusion criteria and caregivers of 43 infants gave informed written consent to participate (). The 43 infants in the study were randomly assigned to receive 1 year COPCA (n = 23) or typical infant physiotherapy (n = 20). Infants were included based on one of the four above-mentioned inclusion criteria, from the 12 different hospitals. Randomization was stratified according to the inclusion criteria, with random sequence generating and concealment of groups by one of the authors who assigned participants to one of the interventions. After inclusion, imaging data from the various hospitals were reclassified in order to obtain a uniform classification of brain lesions, to specify brain pathology, and to preclude interobserver differences in classification. Reclassification was performed by an experienced child neurologist into the following categories: (a) periventricular leukomalacia, divided into noncystic and cystic; (b) cortical infarction; (c) posthaemorrhagic porencephaly; (d) basal ganglia or thalamic lesions; (e) no or nonspecific brain lesions. The study was approved by the Medical Ethical Committee of the University Medical Center of Groningen and registered in the Dutch trial register (NTR1428).
Figure 1. Flow diagram participants. COPCA: COPing with and CAring for Infants with special needs—a family-centered program; TIP: typical infant physical therapy; CP: cerebral palsy; T0: baseline; T1: after 3 months; T2: after 6 months; T3: after 12 months; T4: at 21 months corrected age.
Interventions
The randomized parallel intervention of COPCA and typical infant physiotherapy started after inclusion and lasted 1 year. All interventions were face-to-face for individual family’s with an infant at very high risk of CP. COPCA was provided at home; typical infant physiotherapy was in generally also provided at home, but occasionally it was delivered in an outpatient setting (n = 3). Frequency of both COPCA and typical infant physiotherapy was intended to be once a week (), 30–60 min per session. All physiotherapists had a background of pediatric physical therapy education. Physiotherapists in the COPCA group followed an additional COPCA-course. They were asked not to share information about COPCA with physiotherapist colleagues who did not follow a COPCA course, to prevent contamination between the groups.
Table 1. Baseline characteristics and classification of cerebral palsy.
Measurements
In the time period between November 2008 and September 2015, in each infant tests were performed at baseline (T0; i.e. immediately after inclusion, before start of the intervention), after 3 months (T1), after 6 months (T2), and after 12 months (T3) of intervention (i.e. at the end of the study’s intervention period) and at 21 months CA (T4; only if the infant had an age below 8 months corrected age at inclusion, as in the other infants T3 and T4 coincided). Assessments were performed at the infant’s home. shows which neuromotor, cognitive, and behavioral measurements were used at the various measurement moments. At the last measurement (21 months CA), infants were assessed with the Touwen Infant Neurological Examination [Citation13], to provide information about the neurological condition and on the absence or presence of CP. In case of CP, severity was classified according to the Gross Motor Function Classification System [Citation14]. All measurements, described in the table and below, have shown to be sufficiently valid and reliable [Citation10]. However, it should be noted that some measures have been developed mainly for general populations and some measures specifically for children with CP. In our study population, we did not know beforehand the developmental trajectories of the infants and therefore, we used both general and specific measures. Assessors were blinded for type of intervention, caregivers were asked not to inform them.
Table 2. Neuromotor, cognitive, and behavioral outcome measures at the different measurements during and after the intervention period.
Our primary outcome was the Infant Motor Profile [Citation15], a video-based measurement to assess motor behavior. The Infant Motor Profile does not only assess motor performance, but also the quality of motor behavior in the domains of variation (i.e. the size of the motor repertoire), adaptability (i.e. the ability to select adaptive motor strategies), symmetry, and fluency. Infant Motor Profile scores are expressed in percentages of the maximum score and are based only on the abilities of the infant at the time of the assessment.
Secondary neuromotor outcome measures consisted of the Albert Infant Motor Scale [Citation16], the Gross Motor Function Measure [Citation17,Citation18] and the Bayley Scales of Infants Development—Psychomotor Developmental Index, second edition [Citation19]. Realizing that our primary outcome measure was relatively new and that evaluation of motor development of infants at very high risk of CP is difficult, we also documented motor development with other instruments. The Alberta Infant Motor Scale and Gross Motor Function Measure were used to document gross motor function, the Bayley Scales of Infant Development-II Psychomotor Developmental Index to assess gross, and fine motor capacity. We used the original Gross Motor Function Measure (GMFM-88) [Citation17], the shortened version (GMFM-66) [Citation17] and our own adapted version for infants (GMFM-adapted) [Citation18]. The GMFM is developed for children with CP, but infrequently used below age 2, because infants are usually not yet diagnosed with CP at that age. We used total scores of the original GMFM-88 and the shortened version GMFM-66. In addition, we applied the infant adaptation of the GMFM, which we called “GMFM-adapted”. Of the Alberta Infant Motor Scale and Bayley Scale of Infant Development-II Psychomotor Developmental Index we used raw scores, as percentiles and developmental indices of many infants were below the 5th percentile and therefore lacked discriminatory sensitivity in our groups. Cognitive development was assessed with Bayley Scales of Infant Development-II Mental Developmental Index [Citation19]; again total raw scores were used in the analyses. Behavioral outcome was measured with the Child Behavior Checklist, Dutch Version, for children aged 1.5 to 5 years [Citation20] at the last measurement at 21 months CA. The Child Behavior Checklist is a questionnaire regarding infant’s emotions and behavior. The questionnaire was filled out by caregivers, resulting in a raw score. Raw scores were computed into T scores. The higher the T score, the more problematic behavior.
Quantification of intervention sessions
We aimed to video-record physical therapy sessions three times: at 1, 6, and 12 months after the onset of intervention. As video recording after 12 months was only moderately successful (31 videos (72% of participants) obtained), we only used video recordings obtained after 1 month (n = 41) and after 6 months (n = 37). Comparable with the VIP study [Citation5], contents of the 1 and 6 months videos was largely similar. Therefore, we decided to use the mean scores of these two intervention sessions for further analyses. This implies that in infants in whom only one of these intervention videos was available, single video information was used (filmed after 1 or 6 months of intervention).
Video-recordings were analyzed with the Groningen Observer Protocol 2.0 [Citation21] with the computer program The Observer (version 11.5, Noldus, Wageningen). Total percentage of time spent on specific physiotherapy actions was scored within five main categories: neuromotor actions, educational actions, communication, position, and situation. Within each category, specific behaviors could be specified in subcategories (so-called modifiers). Two persons from the L2M0–2 research group scored 10 videos independently and had overall good to excellent interobserver reliability, measured by intraclass correlation coefficients ().
Table 3. Percentages of time spent on physiotherapy actions for COPCA and typical infant physiotherapy.
Data analyses
Power calculation was based on the Infant Motor Profile, our primary outcome measure. A sample size of 19 infants in both intervention groups, resulted in a power of 80% (α = 0.05) to detect a clinically relevant change of 7.5 points in the total Infant Motor Profile score (SD = 8.2).
In the RCT, the infant outcomes were compared at the various measurement times. We used univariate statistics to compare baseline characteristics and outcome at 21 months CA. For this purpose, we used Statistical Package for Social Sciences (SPSS) version 21 [Citation22]. As the data were not normally distributed, we used non-parametric statistics. Differences in baseline characteristics and outcome between the two intervention groups were tested with Mann–Whitney U and Chi-square tests. Estimates of differences of the median outcome values at 21 months corrected age were expressed by Hodges Lehmann.
To achieve data reduction in the process analysis on the role of specific physiotherapy actions, we used factor analysis by applying principal axis factoring with an Oblimin rotation (as we dealt with interrelated physiotherapy actions; SPSS version 21) [Citation22]. Factor loadings above 0.45 were regarded as contributing sufficiently to the factor. The factor analysis resulted in three components: (1) NeuroDevelopmental Treatment versus COPCA factor, a dimension reflecting the diametrically opposed core elements of Neurodevelopmental Treatment (hands-on techniques and training) and COPCA (coaching and challenging self-generated motor activities), with a high score reflecting NeuroDevelopmental Treatment-like actions and a low score COPCA-like actions; (2) non-directive communication and self-produced motor behavior, i.e. physiotherapy actions incorporated in the COPCA approach; and (3) directive communication and training, i.e. physiotherapy actions that are discouraged in COPCA (). Total variance explained with these three factors was 45% (factor 1: 21%; factor 2: 15%; factor 3: 9%), with a Kaiser–Mayer–Olkin Measure of 0.681. Factor loadings per infant were used as indicators of contents of intervention and we considered a minimal factor loading’s value of 0.45 as significantly contributing to the factor.
Table 4. Factor analysis physiotherapy actions.
Multilevel analyses were performed with linear and non-linear mixed effect models (nlme) library in R version 3.3.1 [Citation23] to study longitudinal potential differential effects of COPCA and typical infant physiotherapy on the main motor (Infant Motor Profile) and cognitive (Bayley Scales of Infant Development II Mental Developmental Index) outcome parameters, taking into account the age in corrected months and possibly confounding factors. We used linear mixed effects models to describe the subject-specific time profiles per infant, as this type of analysis takes into account correlation between observations from the same infant. We first tested possible effects over time of intervention (COPCA versus typical infant physiotherapy), taking into account possible interaction effects of intervention with age. In these analyses, we did not use measurement moment as indicator of time but corrected age in months (and its square), to get the best model fit and avoid introducing error by neglecting the unstructured nature of the data. In the analyses, we adjusted a priori for the following background variables: gestational age, level of parental education, and presence of cystic periventricular leukomalacia (a major predictor of CP) [Citation12], as these factors are known to influence motor and cognitive outcome [Citation1,Citation2,Citation24]. We repeated these analyses for both outcome variables in a similar way for the three factors describing physiotherapy (1 = NeuroDevelopmental Treatment versus COPCA; 2 = non-directive communication; 3 = directive communication), using similar models for each outcome and again, a priori adjusted for the selected covariates. We considered p values below 0.01 as statistically significant. We chose a lower p values than the usually used 0.05, to reduce the risk of type 1 error in a study with multiple measures.
Results
Participants
Of the 43 included infants (n = 23 COPCA, n = 20 typical infant physiotherapy), four infants were lost to follow-up, all from the group of typical infant physiotherapy (). Reasons for withdrawal from the study were maternal illness (n = 1), and study burden (n = 3). Of two “lost” infants, we did obtain information on outcome in terms of CP and level of the Gross Motor Function Classification System around 21 months corrected age, based on information from medical records, obtained with caregivers’ permission. In the COPCA group, two infants were included at the corrected age of 9 months. At the end of the 1-year intervention period, they reached the age of 21 months CA. Therefore, the T3 (1 year after inclusion, at the end of the intervention period) and T4 (21 months corrected age) measurement coincided. In the linear mixed effect models, the overlapping data of these two infants were only included once.
Baseline characteristics of caregivers and infants, of both intervention groups were comparable (). In both groups, frequency of intervention was somewhat lower than the intended once a week, amongst others due to holidays, illness, or logistical reasons. The median number of intervention sessions per month was 3.0 (range 1.8–4.0) in the COPCA group and 2.5 (range 1.3–4.3) in the typical infant physiotherapy group ().
At 21 months corrected age, 22 out of 41 infants (54%) were diagnosed with CP, without significant differences between COPCA and typical infant physiotherapy. Also, no significant differences in severity of CP were present, according to the levels of the Gross Motor Function Classification System ().
Neuromotor, cognitive, and behavioral outcome
Neuromotor, cognitive, and behavioral outcome of the two intervention groups at the various measurement moments was similar ().
Table 5. Outcome in both intervention groups at the various measurement moments.
Also the multilevel analyses showed that the effect of the interventions COPCA and typical infant physiotherapy on the various outcome measures was similar (). shows the results of the linear mixed effects models with random intercept and random slope (random linear time effect, IMP model only). Outcome was especially associated with covariate age at assessment (Infant Motor Profile and Bayley Scales of Infant Development II Mental Developmental Index) and the covariate presence of cystic periventricular leukomalacia (Bayley Scales of Infant Development-II Mental Developmental Index). No interaction effects of intervention with age and cystic periventricular leukomalacia were found.
Table 6. Longitudinal analyses, using linear mixed effect models with interventions COPCA and typical infant physiotherapy.
We repeated the multilevel analyses with the three factors describing interventional elements with physiotherapy actions (). None of the three factors were significantly associated with infant outcome, although the association between factor 2 and Infant Motor Profile approached significance; it suggested that more time spent with nondirective communication might have been associated with worse Infant Motor Profile scores. Also in these analyses, infant outcomes were mainly associated with covariates age at assessment and cystic periventricular leukomalacia.
Table 7. Longitudinal analyses, using linear mixed effect models with factors (1) NDT versus COPCA; (2) nondirective communication; (3) directive communication.
No significant effects of caregivers’ educational level or infant’s gestational age were found (data not shown in the tables).
Discussion
In our study, infant neuromotor, cognitive and behavioral outcome was comparable after both types of intervention and not associated with interventional elements. The type of brain lesion, in the form of cystic periventricular leukomalacia, and the age at assessment were most strongly associated with the infant’s developmental outcome; they did not interact with type of intervention.
Being aware of the overlap between the two interventions and having knowledge of previous studies, the similar outcome in the randomized intervention groups was not unexpected. Moreover, due to selective attrition, the RCT part of our study was underpowered. Therefore, lack of differences between interventions does not mean that no differences may exist between the groups. It raises the question whether the RCT should be the gold standard for measuring effectiveness of early intervention, knowing that the ideal study (controls no intervention) cannot be performed, that interventions are heterogeneous and that trials may suffer from small sample sizes [Citation1,Citation5,Citation24]. Knowing about RCTs pitfalls, we did a detailed process analysis of physiotherapy contents, independent from group randomization, to retrieve distinguishing interventional elements. After analyzing the contents of the interventions, a clear contrast was found between NeuroDevelopmental treatment-related actions (hands-on techniques, caregiver training) and COPCA-related actions (challenging the infants to self-produced motor behavior, caregiver coaching). Despite the clearly discriminating interventional elements, we did not find any significant association between the elements and infant outcome. This finding differs from our previous study [Citation5,Citation8], in which multiple associations between contents of intervention and infant outcome were present. The current absence of associations may be related to differences in study design. First, in the L2M0–2 study, most infants had severe brain lesions; in the VIP study, most infants had no or nonsignificant brain lesions. It could be hypothesized that the presence of serious brain lesions alters the effect of early physiotherapy. Recent reviews and intervention studies suggest that multifaceted interventions may be most effective for infants at very high risk of CP [Citation3,Citation4]. Where we did find comparable infant outcomes in our study groups, the Goals-Activity-Motor-Enrichment (GAME) study of Morgan et al. [Citation25] reported a significant advantage for the GAME intervention on infant’s motor and cognitive outcome, but the study suffered from a selective drop-out of children in the GAME group. The difference in outcome may be related to differences in neuromotor approach: COPCA uses a “hands-off” strategy to stimulate infants to develop own strategies, whereas the GAME study uses combined principles of motor learning and dynamic systems theory, in which manual guidance is provided when needed and withdrawn when the infant shows the ability to begin to demonstrate the motor action. Possibly, the lack of associations between contents of therapy and outcome may be due to the design of our study. We especially evaluated the contrast between the NeuroDevelopmental Treatment techniques, including hands-on manual guidance, and coaching with challenge of self-produced motor behavior (as revealed by factor 1 of the physical therapy actions) and not the effect of the combination of challenging self-produced motor behavior and hands-on manual guidance, as confirmed by our factor-analysis. The differences in outcome for infants with severe brain lesions (L2M0–2 and GAME study) compared with infants with no or nonsignificant brain lesions (VIP project), may suggest that severely affected infants may benefit from some hands-on assistance in addition to the stimulation of the infant’s trial and error activity to develop its own motor strategies, whereas infants with less severely affected neuromotor development may profit from the latter without additional hands-on assistance [Citation4].
Also, the intervention’s duration and dosage may have affected outcome. The VIP-project provided a three months intervention twice a week, the L2M0–2 study a 1-year intervention once a week. Literature suggests positive effects of short and intensive interventions [Citation26]. Unfortunately, we did not succeed in gathering sufficient data about implementation of the intervention, i.e. dosage of interventional elements in daily life activities, which we had aimed to gather with videos of bathing sessions. This is certainly a limitation of our study. Our findings emphasize the need for good measurement tools for implementation of interventions into daily life.
In line with our expectations and the literature [Citation12], infants with the most severe brain lesions (cystic periventricular leukomalacia) were at highest risk for impaired motor and cognitive outcome. Behavioral outcome did not differ between infants with or without cystic periventricular leukomalacia. Possibly, the lack of difference may be attributed to the fact that most behavioral problems first emerge later in childhood [Citation27]. We did not find that infants with the most severe brain lesions profited less from early intervention than the other infants at very high risk of CP. Amongst others, the following two explanations may be offered. First, it is conceivable that the optimal mix of intervention ingredients was insufficiently present in our study, and therefore its differential effect on infants with different types of brain lesions could not be demonstrated. Second, it is possible that a differential effect does not exist.
Strengths of our study are the longitudinal evaluation of infants at very high risk of CP from early age onwards, knowledge about infants’ brain lesions, the detailed process analysis of intervention contents and the broad evaluation of child outcome. The longitudinal design allowed for a mixed-effect model analysis, allowing for the adjustment for potential confounders, taking into account the correlation structure in the data. Our study is one of the few early intervention studies that had brain imaging data for all infants [Citation1], and therefore, we were able to study relations between severe brain lesions, outcome and possible interaction effects. The detailed process analysis made it possible to study real contents of the intervention programs, and allowed to uncover potential working elements within the intervention programs. It is a strategy to cope with the large heterogeneity within interventions. Knowledge about contents of intervention is needed, because information of active ingredients is the basis for establishing evidence-based interventions.
A certain limitation of our study is the small sample size, which resulted in underpowering after drop outs. All results should be interpreted with caution. Another limitation is the selective attrition in the group receiving typical infant physiotherapy. Being assigned to the typical infant physiotherapy group, meant receiving physiotherapy comparable with infants who did not participate in the study, but with additional research appointments. In families that are already overloaded, this may have been the reason to drop out of the study. Caregivers in the COPCA group were aware that they received a novel intervention and this may have contributed to the absence of drop outs in the COPCA group. The inclusion of a few infants who presented with clinical signs suggestive of CP but without a severe lesion of the brain is another limitation, as none of the infants without severe brain lesions in our study were diagnosed with CP. Looking back, it would have been better to include only infants with severe brain lesions. An additional limitation of our study is the long recruitment period, which increased risk of contamination between the intervention groups. To minimize risk of contamination, all therapists who followed the COPCA courses, were asked not to communicate about contents of COPCA. But it is possible that information has been shared. However, our process evaluation showed clear differences between COPCA and TIP, which suggests that contamination was limited.
In conclusion, our study shows that COPCA and typical infant physiotherapy as performed in the Netherlands did not result in differences in child outcome. Interventional elements in our studies were not associated with infant’s outcome. We should be careful in drawing conclusions, because the RCT part of our study was underpowered. Unfortunately, we do not know the infants’ outcome without intervention, and probably we will not know in future trials because it is unethical to withhold infants at very high risk of CP from intervention. Therefore, based on our study we do not know whether both interventions are equally effective or ineffective in modifying infant outcome. More research is needed to disentangle the complex multifactorial interplay between the elements of physical therapy intervention, the infants at risk, their families and environments, to be able to discover effective working mechanisms which could influence infants and families at risk in a positive way.
Acknowledgements
We are grateful to the infants and their families for participation in the LEARN2MOVE 0–2 years study. The L2M0-2 study is part of the Dutch national LEARN2MOVE research program. Funders were not involved in study design, data collection, data analysis, manuscript preparation and/or publication decisions.
The following members of the L2M0-2 study group contributed to this study, in the form of including infants for the study or collecting data:
University of Groningen, Department of Special Needs Education and Child Care, Groningen: C. Vlaskamp; University Medical Center Groningen, Department of Pediatrics, division neonatology: M. Boeve, A.F. Bos, H.J. ter Horst, C.V. Hulzebos, E.W.M. Kooi, E.F. Stremmelaar; University Medical Center Groningen, Department of Neurology, division of Child Neurology: M. Boon, O.F. Brouwer, J.M. Fock, R.J. Lunsing, D. Sival; Martini Ziekenhuis Groningen: H.A. van Dijk, W.B. Geven, H.J. Waalkens, M.J. Wiersma-Zweens; Ziekenhuis Nij Smellinghe Drachten/Revalidatie Friesland: W.A. van Asselt, C. Peer, M. Wilsterman; Gelre Ziekenhuis Zutphen: F.P.J. Dikken; Vrije Universiteit Medisch Centrum Amsterdam: J.G. Becher, S.R.D. van der Schoor, R.J. Vermeulen (MUMC + Maastricht), I.A. Zonnenberg; Isala Zwolle: J. Bekhof, C. Bunkers, J. Cornelissen, L.J.M. Groot-Jebbink, E. d’Haens, M.A.C. Hemels, R. van der Lee, R.A. van Lingen, S.M. Mulder-de Tollenaer, O.F. Norbruis, J.M.E. Quack, M. de Rooij, H.L.M. van Straaten, D.C. Vijlbrief; Medisch Spectrum Twente Enschede: A.G. Kaspers; Ziekenhuisgroep Twente Almelo/Hengelo: D.S.J. van Bommel-Slee, R.S. Rijlaarsdam, G. Shabo, M.L.J. Torringa; Isala Diaconessenhuis Meppel: E. Maza; Spaarne Ziekenhuis Hoofddorp: A. Baauw, J. Christenhuis, H. Kiezenbrink, P. de Winter; Medisch Centrum Leeuwarden: R. Boontje, N.S.K. de Vries, T. de Vries; De Tjongerschans Heerenveen: S.M. van Dorth, W.F. Heikens, A.I. Kistemaker, T. Wiersma; physical therapists: I.K. de Boer, J. Geltink, M. Hijlkema; researchers, students and interns: L.C. van Balen, M.J. Coenraads, L.J. Dijkstra, I. Ebbers-Dekkers, S.J. Hooijsma, K.S.J. Post, R.F. Toonen. The Netherlands.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Spittle A, Orton J, Anderson PJ, et al. Early developmental intervention programmes provided post hospital discharge to prevent motor and cognitive impairment in preterm infants. Cochrane Database Syst Rev. 2015;(24):CD005495.
- Himpens E, Oostra A, Franki I, et al. Predictability of cerebral palsy in a high-risk NICU population. Early Hum Dev. 2010;86:413–417.
- Morgan C, Darrah J, Gordon AM, et al. Effectiveness of motor interventions in infants with cerebral palsy: a systematic review. Dev Med Child Neurol. 2016;58:900–909.
- Hadders-Algra M, Boxum AG, Hielkema T, et al. Effect of early intervention in infants at very high risk of cerebral palsy: a systematic review. Dev Med Child Neurol. 2017;59:246–258.
- Dirks T, Blauw-Hospers CH, Hulshof LJ, et al. Differences between the family-centered "COPCA" program and traditional infant physical therapy based on neurodevelopmental treatment principles. Phys Ther. 2011;91:1303–1322.
- Akhbari Ziegler S, Dirks T, Hadders-Algra M. Coaching in early physical therapy intervention: the COPCA program as an example of translation of theory into practice. Disabil Rehabil. 2018;16:1–9.
- Hadders-Algra M. Early human motor development: from variation to the ability to vary and adapt. Neurosci Biobehav Rev. 2018;90:411–427.
- Blauw-Hospers CH, Dirks T, Hulshof LJ, et al. Pediatric physical therapy in infancy: from nightmare to dream? A two-arm randomized trial. Phys Ther. 2011;91:1323–1338.
- Hielkema T, Blauw-Hospers CH, Dirks T, et al. Does physiotherapeutic intervention affect motor outcome in high-risk infants? An approach combining a randomized controlled trial and process evaluation. Dev Med Child Neurol. 2011;53:e8–15.
- Hielkema T, Hamer EG, Reinders-Messelink HA, et al. LEARN 2 MOVE 0-2 years: effects of a new intervention program in infants at very high risk for cerebral palsy; a randomized controlled trial. BMC Pediatr. 2010;10:76.
- Hielkema T, Boxum AG, Hamer EG, et al. LEARN2MOVE 0-2 years, an early intervention trial for infants at very high risk of cerebral palsy: family outcome and the infant’s activities and participation. Disabil Rehab.
- Hielkema T, Hadders-Algra M. Motor and cognitive outcome after specific early lesions of the brain – a systematic review. Dev Med Child Neurol. 2016;58:46–52.
- Hadders-Algra M, Heineman KR, Bos AF, et al. The assessment of minor neurological dysfunction in infancy using the Touwen infant neurological examination: strengths and limitations. Dev Med Child Neurol. 2010;52:87–92.
- Palisano RJ, Rosenbaum P, Bartlett D, et al. Content validity of the expanded and revised gross motor function classification system. Dev Med Child Neurol. 2008;50:744–750.
- Heineman KR, Bos AF, Hadders-Algra M. The infant motor profile: a standardized and qualitative method to assess motor behaviour in infancy. Dev Med Child Neurol. 2008;50:275–282.
- Piper MC, Darrah J. Motor assessment of the developing infant. Philadelphia (PA): Saunders; 1994.
- Russell D, Rosenbaum P, Avery L, et al. Gross motor function measure (GMFM-66 and GMFM-88) User's manual. London: Mac Keith Press; 2002.
- Hielkema T, Hamer EG, Ebbers-Dekkers I, et al. GMFM in infancy: age-specific limitations and adaptations. Pediatr Phys Ther. 2013;25:168–176.
- Van der Meulen BF, Ruiter SAJ, Spelberg HCL, et al. Bayley Scales of Infant Development – II. Dutch version. Lisse: Swets Test Publishers; 2002.
- Achenbach TM, Rescorla LA. Manual for ASEBA Preschool Forms and Profiles. Burlington (VT): University of Vermont, Research Center for Children, Youth, & Families; 2000.
- Sonderer P, Akhbari Ziegler S, Gressbach Oertle B, et al. Psychometric properties of a standardized observation to quantify pediatric physical therapy actions. Ped Phys Ther. 2017;29:244–250.
- IBM Corp. 2012. IBM SPSS Statistics for Windows, Version 21.0. Armonk (NY): IBM Corp.
- R Development Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2008. ISBN 3-900051-07-0, URL http://www.R-project.org
- West SG, Duan N, Pequegnat W, et al. Alternatives to the randomized controlled trial. Am J Public Health. 2008;98:1359–1366.
- Morgan C, Novak I, Dale RC, et al. Single blind randomised controlled trial of GAME (Goals – Activity – Motor Enrichment) in infants at high risk of cerebral palsy. Res Dev Disabil. 2016;55:256–267.
- Trahan J, Malouin F. Intermittent intensive physiotherapy in children with cerebral palsy: a pilot study. Dev Med Child Neurol. 2002;44:233–239.
- Van Zeijl J, Mesman J, Stolk MN, et al. Terrible ones? Assessment of externalizing behaviors in infancy with the child behavior checklist. J Child Psychol Psychiatry. 2006;47:801–810.