
Abstract
Purpose
To cross-cultural translate the Cumberland Ankle Instability Tool (CAIT) to Taiwan-Chinese version (CAIT-TW), and to evaluate the validity, reliability and cutoff score of CAIT-TW for Taiwan-Chinese athletic population.
Materials and methods
The English version of CAIT was translated to CAIT-TW based on a guideline of cross-cultural adaptation. 77 and 58 Taiwanese collegial athletes with and without chronic ankle instability filled out CAIT-TW, Taiwan-Chinese version of Lower Extremity Functional Score (LEFS-TW) and Numeric Rating Scale (NRS). The construct validity, test-retest reliability, internal consistency and cutoff score of CAIT-TW were evaluated.
Results
In construct validity, the Spearman’s correlation coefficients were moderate (CAIT-TW vs LEFS-TW: Rho = 0.39, p < 0.001) and strong (CAIT-TW vs NRS: Rho= 0.76, p < 0.001). The test retest reliability was excellent (ICC2.1 = 0.91, 95% confidential interval = 0.87–0.94, p < 0.001) with a good internal consistency (Cronbach’s α: 0.87). Receiver operating characteristic curve showed a cutoff score of 21.5 (Youden index: 0.73, sensitivity: 0.87, specificity 0.85).
Conclusions
The CAIT-TW is a valid and reliable tool to differentiate between stable and instable ankles in athletes and may further apply for research or daily practice in Taiwan.
For athletes, chronic ankle instability is prevalent and causes negative sequela, such as lowered quality of daily life, affected functional performance, and may cause post traumatic osteoarthritis.
The psychometric properties of the Taiwan-Chinese version of the Cumberland Ankle Instability Tool showed moderate to strong construct validity, excellent test retest reliability, a good internal consistency and a cutoff score of 21.5.
The validity and reliability of the Taiwan-Chinese version of the Cumberland Ankle Instability Tool are to enable clinicians to evaluate and manage ankle instability in Taiwanese who speaks Mandarin Chinese.
Implications for rehabilitation
Introduction
Ankle sprain is the most common injury in the athletic population accounting for 6.9–14.5% of all reported injuries in sports, such as American football, soccer, volleyball, gymnastics, lacrosse, basketball, and cross country [Citation1]. Sports that demand running, cutting, jumping, landing accelerating and decelerating cause a high rate of ankle sprain [Citation2]. After an acute ankle sprain 35% of individuals suffer from residual symptoms, pain, swelling, recurrent ankle sprain, loss of ankle function, giving way, and strength decreasing [Citation3]. Different descriptions of this phenomenon had been suggested, chronic lateral ankle instability, recurrent lateral ankle instability, ankle instability, residual ankle instability, chronic instability, and chronic ankle sprain [Citation3,Citation4]. However, in 2014 the International Ankle Consortium termed that as Chronic Ankle Instability (CAI) and characterized CAI as an individual that had endured a significant ankle sprain, and experienced episodes of giving way and/or recurrent ankle sprain and/or subjective ankle instability [Citation5]. 40% of first-time acute ankle sprain developed into CAI, which caused a high rate of recurrent ankle sprain (12–80%), lowered the quality of daily life, affected functional performance, and may cause post-traumatic osteoarthritis [Citation5–9].
To qualify for subjective ankle instability, the International Ankle Consortium recommended three valid and reliable self-report questionnaires with cutoff scores: the Ankle Instability Instrument (AII), the Cumberland Ankle Instability Tool (CAIT) and the Identification Functional Ankle Instability (IdFAI) [Citation5]. The CAIT has been translated into different languages: Brazilian-Portuguese, Spanish, Korean, Japanese, Persian, Dutch, French, and Greek which is then applied towards research and clinical practice [Citation10–19]. A valid and reliable self-report questionnaire is low cost and able researchers and clinicians to evaluate the ankle instability and to access improvements to the rehabilitation [Citation12].
The prevalence of CAI has been investigated in different countries and different populations [Citation20–23]. A systematic review indicated that 61% of soccer athletes, 60% of basketball athletes and 46% of volleyball athletes suffered from recurrent ankle sprain; and 28% of basketball athletes experienced perceived ankle instability while 30% experienced other residual symptoms [Citation21]. Attenborough et al. applied CAIT to investigate the prevalence of CAI in Australian netballs athletes, and they found that 88.4% of them had CAI [Citation20]. Simon et al. found 75.9% (41/54) of professional dancer had CAI using IdFAI [Citation22]. Tanen and colleagues applied CAIT to survey the prevalence of CAI in US high schools and colleges, and the result showed that 23.4% of athletes had CAI [Citation23]. The prevalence of CAI is varying in different sport populations and areas. In terms of sports injury prevention and management, it is important to recognize the prevalence of CAI in the athletic population in different areas and provide an efficient and specific intervention protocol or strategy to improve the quality of sports performance.
Chinese is a widely used language, and it is the official language in Taiwan. However, there is no Taiwan-Chinese version of CAIT that has been evaluated for validity and reliability. A valid and reliable self-reporting questionnaire in Taiwan-Chinese would be helpful for monitoring and injury prevention in athletes who speak Mandarin Chinese in Taiwan. Therefore, the objective of this study was to develop a valid and reliable cross-cultural adapted Taiwan-Chinese version of CAIT (CAIT-TW).
Methods
The current study was a cross-sectional study of cross-cultural adaption and validation of a self-report questionnaire. This study was conducted from June to October 2018 for a total of 5 months.
Cross-cultural translation
We informed the developer of CAIT about this study and also obtained the license of using CAIT in the current study from Elsevier (license number: 4758770436837) [Citation24]. The English version of the CAIT was translated to a Taiwan-Chinese version referring to the guidelines for the process of cross-cultural adaptation [Citation25]. There are six steps:
Initial translation (step I): Two bilingual translators, a certified athletic trainer and a non-medical background translator, translated the English CAIT into CAIT-TW individually.
Synthesis of the translations (step II): The differences of translations between the two translators were synthesized in a consensus meeting.
Back translation (step III): The primary CAIT-TW was translated back to English by two English native speakers without any medical background. The translators were unaware of the existence of the original English CAIT.
Expert committee (step IV): The expert committee consisted of a methodologist, a health professional, a language professional, and the translators (forward and back translators). Then, they discussed the discrepancies of all versions of translations and reach an agreement based on semantic, idiomatic, experiential, and conceptual equivalence to consolidate the prefinal version of CAIT-TW.
Test of the prefinal version (step V): To examine the meaning and subjects’ understanding of each item, 33 athletes filled out the prefinal version of CAIT-TW (172.1 ± 9.6 cm, 64 ± 12.2 kg, 14.1 ± 10.1 hours of training per week, and 7.3 ± 3.0 years of training experience, the score of CAIT-TW was 22.6 ± 6.0). Identified problems in the questionnaire were reported and revised in preparing the final CAIT-TW-version.
Submission of documentation to coordinating committee for appraisal of the adaptation process (step VI): The questionnaire developer reviewed the final version of CAIT-TW, all reports about the step I to V, and appraised the process of adaption.
Participants
For sample size determination Terwee et al. suggested that to evaluate internal consistency at least 100 subjects are required, and to assess the Intraclass Correlation Coefficient a minimum of 50 participants are required [Citation26]. We applied convenience by contacting coaches and athletic trainers on the campus to recruit participants in sports teams. In total, 135 native Mandarin speakers (98 males and 37 females), who were over the age of 18 were regularly attending to trained athletes (≥ 10 hours per week), whom were recruited from sports teams from two universities in Taiwan. Athletes with CAI were allocated in the CAI group and athletes without any ankle issues were assigned to a control group (CON). Subjects in the CAI group met the following criteria: a history of at least one significant ankle sprain; and/or a history of the previously injured ankle joint “giving way,” and/or recurrent sprain and/or “feelings of instability” in their daily or sports activity [Citation5]. Subjects with bilateral CAI were included in this study too. The subjects were excluded if they (1) had a history of previous surgeries or a fracture to the musculoskeletal structures in either lower extremity requiring realignment; or (2) had acute musculoskeletal injuries of the lower extremity in the previous 3 months, which affect joint integrity and function (i.e., sprains or fractures) disturbing their desired physical activity in at least 1 day (3) were attending regular balance training; or (4) were not able to complete the questionnaire [Citation5]. All participants read and signed the informed consent document. This study procedure was approved by the Ethics Committee of the University of Potsdam in Germany (Number: 25/2018).
Instruments
Cumberland Ankle Instability Tool questionnaire: The CAIT questionnaire contains nine questions to evaluate both ankles concerning pain in each ankle for daily activities, ankle instability in different types of physical activities, ankle control when recurrent sprain occurring and recovery period after recurrent ankle sprains [Citation24]. The maximum score is 30, and the cutoff point to identify the subject with or without CAI is 24 in the original English version [Citation5,Citation27].
Lower Extremity Functional Scale (LEFS): LEFS contained 20 items to evaluate the function of lower extremity in patients with orthopedic problems [Citation28]. LEFS has been translated to a Taiwan-Chinese version of LEFS (LEFS-TW) with satisfactory validity and reliability (internal consistency: Cronbach α was 0.98 and test-retest reliability: ICC 2,1 was 0.97) [Citation29].
Numeric Rating Scale (NRS): The maximum score of NRS is 10, meaning extremely instable in the ankles, and the minimum score is 0, indicating very stable ankles. NRS has been applied to evaluate the degree of each ankle’s instability and perception of effort in isometric exercise [Citation16,Citation30].
Analysis of psychometric properties
For psychometric properties examination, the construct validity, test-retest reliability, and internal consistency reliability of CAIT-TW were analyzed. The cutoff score between participating athletes with or without CAI was built up by testing discriminating ability.
Construct validity: Due to the lack of a gold standard, construct validity is to evaluate if ankle function is truly measured by CAIT-TW. To confirm it, the correlations between similar tools were evaluated [Citation26]. To examine the construct validity of CAIT-TW, Spearman’s correlation coefficient were used to examine the correlation between CAIT-TW and LEFS-TW [Citation29] and between CAIT-TW and NRS [Citation16,Citation30]. The Spearman’s correlation coefficient is ≤ 0.30 considered as poor, 0.30–0.60 as moderate, > 0.60 as strong [Citation11,Citation16,Citation19,Citation26].
Test-retest reliability: Participants filled out this questionnaire twice, with a week period in between testing. The test-retest reliability was examined by the intraclass correlation coefficient (ICC1,2). The test-retest reliability of the questionnaire was considered excellent when the ICC value is > 0.90, good as 0.75–0.90, moderate as 0.50–0.75 and <0.50 as poor [Citation31].
Internal consistency: For internal consistency reliability examination, Cronbach’s α coefficient was applied to the testing of the internal consistency of CAIT-TW. Cronbach’s alpha of a good questionnaire should be between 0.70 and 0.95 [Citation26].
Discriminating ability: The position statement of the International Ankle Consortium suggested that the 24 points of CAIT is the cutoff point to distinguish the subject with or without CAI. To determine the cutoff score of CAIT-TW in an athletic population, a receiver operating characteristic (ROC) curve was utilized to find the highest Youden index [Citation32].
Statistical analysis
All data analysis was performed using IBM SPSS 22.0 (Chicago, IL, USA). Construct validity tested the correlation between CAIT-TW and LEFS-TW and between CAIT-TW and NRS using Spearman’s correlation. Test-retest reliability was conducted by the intraclass correlation coefficient (ICC1.2), and internal consistency reliability was performed by Cronbach’s α coefficient. Discriminating ability was determined using ROC to find the highest Youden index.
Results
The English version of CAIT was adapted to a Taiwan-Chinese version based on the guidelines [Citation25]. No specific problem of semantic, idiomatic, experiential, and conceptual equivalence was relevant during the translation process. The most frequently asked question when testing the prefinal version was about item 9: after a TYPICAL incident of my ankle rolling over, my ankle returns to “normal.” According to the athletes’ experience, there were different degrees of rolling over, which affects the duration of recovery. Without a specific definition of that, it was difficult for some athletes to answer this question. For this item, we decided to follow the original CAIT guidelines without any changes due to being a translated version. In total 292 athletes filled out the questionnaires (). After excluding invalid questionnaires and participants who did not meet the inclusion criteria, 135 questionnaires were included to assess psychometric properties (). In total, 77 were athletes with CAI and 58 were athletes without CAI. 116 of 135 questionnaires were used to evaluate construct validity () and 87 of 135 questionnaires were applied to examine test-retest reliability, internal consistency, and discriminating ability (). There was no difference in demographics between two groups, but the score of CAIT-TW, LEFS-TW and NRS showed a statistical difference between the CAI and the CON groups (see and Citation3).
Figure 1. The flow chart of data collection. CAIT-TW: Taiwan-Chinese version of Cumberland Ankle Instability Tool; LEFS-TW: Taiwan-Chinese version of Lower Extremity Function Scale; NRS: Numeric Rating Scale; CAI: chronic ankle instability.
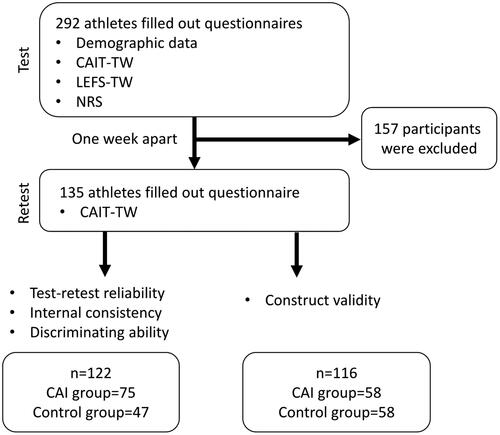
Table 1. Taiwan-Chinese version of Cumberland Ankle Instability Tool.
康柏蘭腳踝穩定性評估量表 在以下問題中, 請選擇最能描述您腳踝狀況的選項:
Table 2. Participants’ characteristics for testing construct validity.
Table 3. Participants’ characteristics in evaluating test-retest reliability, internal consistency, and discriminating ability.
Construct validity: The correlation between CAIT-TW and LEFS-TW was moderate (Rho = 0.39, p < 0.001) and the correlation between CAIT-TW and NRS was strong (Rho = 0.76, p < 0.001).
Test-retest reliability: CAIT-TW had excellent test-retest reliability (ICC2.1 = 0.91, 95% confidence interval: 0.87–0.94, p < 0.001) overall. The test and retest scores of CAIT-TW were 20.3 ± 6.3 and 20.8 ± 6.6. For each item test-retest reliability were moderate to good (ICC2.1 = 0.60–0.85) (see ). The drop-out rate was 9.6% (13/135) (see ). The reasons for this drop-out rate were the absence of practice or incomplete questionnaires.
Table 4. Test-retest of Taiwan-Chinese version of Cumberland Ankle Instability Tool.
Internal consistency: CAIT-TW had good internal consistency. Cronbach’s α coefficient of CAIT-TW was 0.87. There was no improvement if any item of CAIT-TW was deleted ().
Table 5. Internal consistency of Taiwan-Chinese version of Cumberland Ankle Instability Tool.
Discriminating ability: The mean score of CAIT-TW in the CAI group was 16.6 ± 4.3 and in the CON group was 26.1 ± 4.0. ROC showed that the cutoff score of CAIT-TW was 21.5 according to the maximum Youden index (0.73) ( and ). The sensitivity and specificity were 0.87 and 0.85 respectively.
Figure 2. The receiver operating characteristic (ROC) curve of Taiwan-Chinese version of Cumberland Ankle Instability Tool. The area under the curve was 0.94.
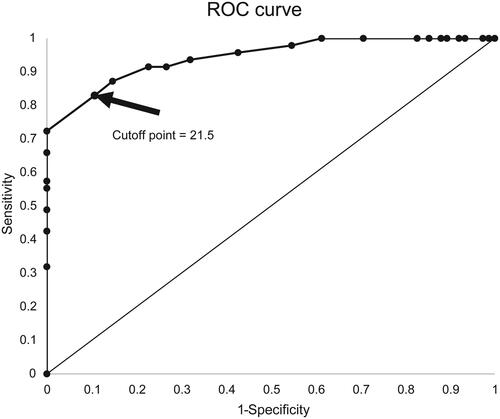
Table 6. Sensitivity, specificity and Youden index of Taiwan-Chinese version of Cumberland Ankle Instability Tool.
Discussion
The current study translated and cross-culturally adapted CAIT from English to Taiwan-Chinese version. The CAIT-TW assessed the validity, reliability and cutoff score using an athletic population. In construct validity CAIT-TW showed a strong correlation with NRS and moderate correlation with LEFS-TW. CAIT-TW had overall excellent test-retest reliability, good internal consistency and was with a 21.5 cutoff score to discriminate between a stable ankle and an unstable ankle.
In construct validity, the Spearman’s correlation coefficient between CAIT-TW and LEFS-TW was not optimal but acceptable. This may be caused by the testing population and property of the questionnaires. The correlation between the English version of CAIT and LEFS was moderate (0.50, p < 0.01), and the correlation between the Greek version of CAIT and LEFS was strong (0.71, p < 0.001), and their participants were from the general community, dancers in an art school, and students from a physiotherapy’s school [Citation19,Citation24]. The participants in this current study were all competitive athletes, attending 18–20 h of high-intensity training every week. The athletes with CAI did not drop out of their daily training because of their ankle condition, and they performed their sports-specific tasks every day. Most of the questions in Lower Extremity Functional Scale (LEFS) is based on activities in daily life (15 items out of 20), which may not be sensitive enough to detect ankle instability for highly competitive athletes. In addition, LEFS focus on general functional in lower extremities instead of specialization in ankle condition. This may cause the correlation between LEFS-TW and CAIT-TW resulting in not optimal in competitive athletes. On the other hand, the Spearman’s correlation coefficient between CAIT-TW and NRS showed strong correlation (Rho= 0.76, p < 0.001). This result is comparable with previous studies [Citation15,Citation16,Citation24]. The correlation between English, Iranian and Dutch version of CAIT and Visual Analogue Scale or NRS were 0.64–0.80 [Citation15,Citation16,Citation24].
For test-retest reliability, although the test-retest of CAIT-TW on each item was moderate to good, the overall test-retest reliability was excellent, which is consistent with previous studies (ICC2,1 were from 0.83–0.98) [Citation10–16,Citation19,Citation24]. The current study applied a one-week interval to examine the overall test-retest reliability, which was similar with the Brazilian-Portuguese version (ICC2,1 = 0.98), two Spanish versions (ICC2,1 = 0.98 and 0.95), the French version (ICC2,1 = 0.96), the Persian version (ICC2,1 = 0.91–0.95) and the Korean version (ICC2,1 = 0.95) of CAIT [Citation10–13,Citation15,Citation18]. The Greek version showed 0.95 to 0.97 of ICC2,1 with seven to ten days in between testing [Citation19]. In the English version and the Japanese versions of CAIT, the test-retest intervals were between two and three weeks respectively and the ICC2,1 were 0.96 and 0.83 [Citation14,Citation24]. The current result should be interpreted carefully, because the test-retest reliabilities in five out of nine items were moderate (ICC2.1 = 0.60–0.73), which is not perfect but acceptable. Compared to the French and the Greek version of CAIT, the test-retest reliabilities of each item were excellent (ICC2.1 = 0.95–0.99 and 0.84–0.91). The differences may cause by the athletes’ dynamic status. Athletes may have a different level of fatigue between test and retest, which may affect posture stability and then affect the score of each item [Citation33].
In CAIT-TW the Cronbach’s α coefficient was 0.87 indicating good internal consistency. The Cronbach’s α coefficient would not improve if any item was omitted. This result is comparable with the French version of CAIT, which is with the Cronbach’s α coefficient of 0.89 and there is no improvement if any item was deleted [Citation18]. The result was comparable with previous studies. In the original English version Cronbach’s α coefficient was 0.83. The Cronbach’s α coefficient of Brazilin-Portuguese, Korean, Japanese, Persian, Dutch and Greek versions ranged from 0.73–0.97 [Citation10,Citation13–16,Citation19]. In the Spanish version, published by Cruz-Duaz et al., the Cronbach’s α coefficient was 0.77, and if items 5 or 6 were deleted, the Cronbach’s α coefficient would be 0.79 and 0.78 respectively [Citation11]. In the other Spanish version of CAIT, the Cronbach’s α coefficient was 0.84 of the right ankle and 0.80 of the left ankle, and if item 9 was deleted the Cronbach’s α coefficient would increase [Citation12].
The current study showed that the cutoff score of CAIT-TW was 21.5 based on 0.73 of the Youden index. It is lower than the English, Japanese, French and Greek versions of CAIT [Citation14,Citation18,Citation19,Citation24,Citation27]. The original English CAIT suggested the cutoff score was 27.5 (Youden index: 0.68, sensitivity: 0.83 and Specificity: 0.75) [Citation24]. Later Wright et al. recalibrated the cutoff score of the English CAIT, and suggested that the cutoff score is 25.5 (Youden index: 0.89, sensitivity: 0.97 and Specificity: 0.87) [Citation27]. The cutoff score of the Japanese CAIT is also 25.5 (Youden index: 0.69, sensitivity: 0.71 and Specificity: 0.98) [Citation14]. The cutoff score of the French and Greek versions of CAIT are 23.5 and 24.5 [Citation18,Citation19]. The differences in cutoff scores may be caused by different characteristics of the participants. In the English CAIT, the subjects were selected from students in universities and dancers from art schools [Citation24,Citation27]. In the French version of CAIT the participants were not specifically described and in the Greek version, the participants were students from a physiotherapy’s school [Citation18,Citation19]. In the current study, the participants were highly competitive athletes. Although in the Japanese CAIT, the participants were from a soccer club in a university, the study did not provide information of the participants’ competitive level [Citation14]. The study of the Korean version of CAIT applied similar subjects as the current study, but they did not evaluate the cutoff score [Citation13]. In addition, the cutoff score of the Dutch version, whose participants were patients in an orthopedic outpatient clinic, was 11.5 (Youden index: 0.72, sensitivity: 0.76 and Specificity: 0.91), which is even lower than the current study [Citation16]. The study population in the French version of CAIT is unknown [Citation18]. This indicates that different populations may need different cutoff points of CAIT to differentiate between a stable and an unstable ankle.
There were some limitations in the current study. First of all, the current study did not categorize the mechanical instability of the CAI group. Mechanical instability also affects the feeling of instability [Citation3,Citation14]. Secondly, the cutoff point of CAIT-TW was calculated based on an athletic population. Therefore, this cutoff point may not be fit to evaluate the general population. Thirdly, some of the athletes had difficulties in answering item number 9: after a TYPICAL incident of my ankle rolling over, my ankle returns to “normal,” because they have different degrees of rolling over during their daily training, which affects the recovery period. This may affect the precision of scoring. Finally, the sensitivity to change, which is defined as an ability to detect the meaningful clinical change, was not assessed in the current study owing to the limited resources [Citation34].
Conclusion
The Taiwan-Chinese version of the Cumberland Ankle Instability Tool showed satisfactory construct validity, excellent test-retest reliability and good internal consistency. In an athletic population, it can differentiate between a stable ankle and an unstable ankle with a 21.5 cutoff score. This tool can assist experts in sports medicine in Taiwan to conduct research or to apply it to daily practice.
Acknowledgements
We acknowledge Professor Chi-Huang Huang, Associate Professor Li-Lan Fu, and Associate Professor I-Hsin Kai from National Taiwan Sport University and translators, Yo-Rong Chen, Chia- Hung Lin, Michael Toy and Chen Lin, assisted to the translation process. We are also grateful to the coaches and athletes from National Taiwan Sport University and athletic trainer- Su Po-Wen from Chinese Culture University who kindly agreed to assist and participate in this study. We are thankful to Henry Robert Mumm to help with proofreading.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Doherty C, Delahunt E, Caulfield B, et al. The incidence and prevalence of ankle sprain injury: a systematic review and meta-analysis of prospective epidemiological studies. Sports Med. 2014;44(1):123–140.
- Gribble PA, Bleakley CM, Caulfield BM, et al. Evidence review for the 2016 International Ankle Consortium consensus statement on the prevalence, impact and long-term consequences of lateral ankle sprains. Br J Sports Med. 2016;50(24):1496–1505.
- Hertel J, Corbett RO. An updated model of chronic ankle instability. J Athl Train. 2019;54(6):572–588.
- Hubbard TJ, Kramer LC, Denegar CR, et al. Contributing factors to chronic ankle instability. Foot Ankle Int. 2007;28(3):343–354.
- Gribble PA, Delahunt E, Bleakley C, et al. Selection criteria for patients with chronic ankle instability in controlled research: a position statement of the International Ankle Consortium. Br J Sport Med. 2014;48(13):1014–1018.
- Doherty C, Bleakley C, Hertel J, et al. Recovery from a first-time lateral ankle sprain and the predictors of chronic ankle instability: a prospective cohort analysis. Am J Sports Med. 2016;44(4):995–1003.
- Arnold BL, Wright CJ, Ross SE. Functional ankle instability and health-related quality of life. J Athl Train. 2011;46(6):634–641.
- Witchalls JB, Newman P, Waddington G, et al. Functional performance deficits associated with ligamentous instability at the ankle. J Sci Med Sport. 2013;16(2):89–93.
- Valderrabano V, Hintermann B, Horisberger M, et al. Ligamentous posttraumatic ankle osteoarthritis. Am J Sports Med. 2006;34(4):612–620.
- De Noronha M, Refshauge KM, Kilbreath SL, et al. Cross-cultural adaptation of the Brazilian-Portuguese version of the Cumberland Ankle Instability Tool (CAIT). Disabil Rehabil. 2008;30(26):1959–1965.
- Cruz-Diaz D, Hita-Contreras F, Lomas-Vega R, et al. Cross-cultural adaptation and validation of the Spanish version of the Cumberland Ankle Instability Tool (CAIT): an instrument to assess unilateral chronic ankle instability. Clin Rheumatol. 2013;32(1):91–98.
- Rodriguez-Fernandez AL, Rebollo-Roldan J, Jimenez-Rejano JJ, et al. Psychometric properties of the Spanish version of the Cumberland Ankle Instability Tool. Disabil Rehabil. 2015;37(20):1888–1894.
- Ko J, Rosen AB, Brown CN. Cross-cultural adaptation and validation of the Korean version of the Cumberland Ankle Instability Tool. Int J Sports Phys Ther. 2015;10(7):1007–1014.
- Kunugi S, Masunari A, Noh B, et al. Cross-cultural adaptation, reliability, and validity of the Japanese version of the Cumberland ankle instability tool. Disabil Rehabil. 2017;39(1):50–58.
- Hadadi M, Ebrahimi Takamjani I, Ebrahim Mosavi M, et al. Cross-cultural adaptation, reliability, and validity of the Persian version of the Cumberland Ankle Instability Tool. Disabil Rehabil. 2017;39(16):1644–1649.
- Vuurberg G, Kluit L, van Dijk CN. The Cumberland Ankle Instability Tool (CAIT) in the Dutch population with and without complaints of ankle instability. Knee Surg Sports Traumatol Arthrosc. 2018;26(3):882–891.
- Cruz-Diaz D, Lomas-Vega R, Osuna-Perez MC, et al. Effects of 6 weeks of balance training on chronic ankle instability in athletes: a randomized controlled trial. Int J Sports Med. 2015;36(09):754–760.
- Geerinck A, Beaudart C, Salvan Q, et al. French translation and validation of the Cumberland Ankle Instability Tool, an instrument for measuring functional ankle instability. Foot and Ankle Surgery. 2019;S1268-7731(19)30065-7.
- Tsekoura M, Billis E, Fousekis K, et al. Cross cultural adaptation, reliability, and validity of the Greek version of the Cumberland Ankle Instability Tool. Physiother Theory Pract. 2019;7:1–9.
- Attenborough AS, Sinclair PJ, Sharp T, et al. A snapshot of chronic ankle instability in a cohort of netball players. J Sci Med Sport. 2016;19(5):379–383.
- Attenborough AS, Hiller CE, Smith RM, et al. Chronic ankle instability in sporting populations. Sports Med. 2014;44(11):1545–1556.
- Simon J, Hall E, Docherty C. Prevalence of chronic ankle instability and associated symptoms in university dance majors: an exploratory study. J Dance Med Sci. 2014;18(4):178–184.
- Tanen L, Docherty CL, Van Der Pol B, et al. Prevalence of chronic ankle instability in high school and division I athletes. Foot Ankle Spec. 2014;7(1):37–44.
- Hiller CE, Refshauge KM, Bundy AC, et al. The Cumberland ankle instability tool: a report of validity and reliability testing. Arch Phys Med Rehabil. 2006;87(9):1235–1241.
- Beaton DE, Bombardier C, Guillemin F, et al. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. 2000;25(24):3186–3191.
- Terwee CB, Bot SDM, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42.
- Wright CJ, Arnold BL, Ross SE, et al. Recalibration and validation of the Cumberland Ankle Instability Tool cutoff score for individuals with chronic ankle instability. Arch Phys Med Rehabil. 2014;95(10):1853–1859.
- Binkley JM, Stratford PW, Lott SA, et al. The Lower Extremity Functional Scale (LEFS): scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys Ther. 1999;79(4):371–383.
- Hou WH, Yeh TS, Liang HW. Reliability and validity of the Taiwan Chinese version of the Lower Extremity Functional Scale. J Formos Med Assoc. 2014;113(5):313–320.
- Lampropoulou S, Nowicky AV. Evaluation of the Numeric Rating Scale for perception of effort during isometric elbow flexion exercise. Eur J Appl Physiol. 2012;112(3):1167–1175.
- Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163.
- Deyo RA, Centor RM. Assessing the responsiveness of functional scales to clinical change: an analogy to diagnostic test performance. J Chronic Dis. 1986;39(11):897–906.
- Steib S, Zech A, Hentschke C, et al. Fatigue-induced alterations of static and dynamic postural control in athletes with a history of ankle sprain. J Athl Train. 2013;48(2):203–208.
- Liang MH, Lew RA, Stucki G, et al. Measuring clinically important changes with patient-oriented questionnaires. Med Care. 2002;40(4 Suppl):II45–51.