
Abstract
Purpose
We explored the experiences of working-age and older adults with acquired vision impairment who pursued braille rehabilitation training, and the facilitators and barriers they encountered throughout this process.
Methods
Semi-structured interviews of up to 90 min in length were conducted with 14 participants from across Canada who learned braille between the ages of 33 and 67 (Mdn = 46). Transcripts were analyzed by two researchers using interpretive phenomenological analysis.
Results
A variety of personal, social and institutional factors characterize the adult braille learning experience. Among these, participants highlight the role of prior identity and experience, the impact of access to resources and the cost of materials and devices needed to maintain braille skills. Findings also emphasize invisible barriers, including the role of societal perceptions towards braille, the level of support provided by family and friends, and the influence of unconscious biases towards braille and aging held by both adult learners and those around them.
Conclusions
These findings provide important context to improve policies and practice in adult braille rehabilitation. As the prevalence of age-related vision impairment continues to increase, it will become imperative to understand the unique needs of working-age and older adults with acquired vision impairment who pursue braille.
This study is one of the first to explore the experiences of working-age and older adults with acquired visual impairment who pursue braille rehabilitation training.
Rehabilitation professionals must take into account prior learning and reading experiences which may shape the braille learning process.
Family members require greater access to resources and support during the training process.
There is a significant need for public education to address societal misconceptions about braille and blindness that can lead to a reluctance to use braille.
Interactions with other braille users foster more empowering definitions of braille that align with the social model understanding of disability.
Implications for REHABILITATION
Introduction
Considering that the training of new or compensatory skills is often at the heart of vision rehabilitation [Citation1], it is curious that so little attention has been devoted to directly engaging with the knowledge gained from other domains on the adult learning process [Citation2], or the implications of adult learning theory and practice within the rehabilitation context. Questions on how to best serve adults with acquired vision impairment, whose experiences differ intrinsically from those born with congenital vision impairment, become more imperative to address as the prevalence of age-related vision impairment continues to increase. It is estimated that the population of people with vision impairment (that is, those who are blind or who have low vision) will triple worldwide over the next 30 years due to both population growth and aging. This continues to place new burdens on existing healthcare and rehabilitation systems [Citation3]. In the United States alone, the prevalence of age-related vision impairment is expected to double by 2050 [Citation4]. This raises the need for innovative evidence-based approaches and policies that can respond to these evolving priorities.
Braille is among the skills taught to adults with vision impairments who pursue rehabilitation training, as it provides a tactile alternative to visual print [Citation1]. Although reports indicate that fewer than 10% of individuals who are blind are braille readers [Citation5], these rates remain greatly contested (for example, see [Citation6]). Practitioners within the field of blindness as well as braille readers themselves accentuate that these figures do not reflect the individual benefits of braille as a literacy medium [Citation7]. Braille carries benefits for adults who are functionally blind or who have fluctuating vision, and can be vital for the growing number of older adults with dual sensory (combined vision and hearing) impairment [Citation8]. Best practices and prior research on braille learning centers heavily on blind children who acquire braille as a literacy medium through the educational system, given the historically high prevalence of congenital vision impairment [Citation9]. Comparatively less is known about the unique experience of learning braille in adulthood after acquired vision impairment or about the facilitators and barriers encountered by older clients who pursue braille rehabilitation training. The present study therefore explores the experience of learning braille in adulthood and the enablers and obstacles encountered, as a catalyst for future policy and practice recommendations to address existing service gaps.
There is ample evidence demonstrating the ways in which adults can and do learn differently from children. Within the braille context, blind children typically learn braille through the process of acquiring literacy, and an emphasis is placed on the development of spelling, phonetics and underlying concept development [Citation10]. In these instances, braille is merely the means through which literacy is attained, just as print is the vehicle through which literacy is acquired for children with sight. Adults and seniors, on the other hand, are already literate as print readers prior to age-related vision loss and do not seek rehabilitation training to acquire fundamental literacy skills. Rehabilitation training for these older clients therefore places emphasis on the development of tactile perception and fine-motor skills needed to effectively use braille later in life [Citation11].
Studies directed explicitly at exploring the experiences of working-age and older adults who learn braille are rare, but typically centre on the physiological and cognitive implications of acquiring new skills after childhood. For example, a wide body of research explores the degree of learning plasticity that can be expected as individuals age. These investigations reveal that those who learn braille early in life recruit the visual cortex during braille reading and exhibit cortical magnification in the regions associated with the braille-reading fingers [Citation12,Citation13]. Some isolated studies also suggest that, with ample exposure and practice, this cortical plasticity might also be observable in adult learners of braille [Citation14]. Others have explored tactile sensitivity declines as individuals age and the potential relationship between tactile acuity and braille reading performance, resulting in mostly inconsistent findings [Citation15–20]. These findings are essential because they consider the effect of the aging process on the skills needed to use braille; however, they fail to account for the subjective implications of learning something new as an adult after the onset of a diagnosis, or the factors which influence this experience.
Other studies explore the impact of braille among adults who learned it early in life. Schroeder [Citation21] interviewed eight legally blind adult braille users and observed that self-esteem, self-identity and the meanings ascribed to being a person with a disability were closely intertwined with expressed feelings towards braille. In comparing outcomes among congenitally legally blind adults who learned braille versus print as their primary medium in childhood, Ryles [Citation22] found that those who learned braille had higher levels of education and income and engaged in more extensive reading as adults. In a study of 443 legally blind adults, Silverman and Bell [Citation23] observed that adults who had learned braille as either a primary or secondary medium expressed more positively perceived well-being and life satisfaction as compared to legally blind adults who had not learned braille at all. These investigations are valuable in that they reveal the ways in which braille may impact quality of life for legally blind adults who already know it, but they do not explicitly focus on the experience of learning braille beyond childhood.
Though not centered on braille in particular, prior literature is replete with examples of how adjustment to vision loss later in life can affect both the decision to initially pursue rehabilitation and overall training outcomes [Citation24,Citation25]. Barriers to seeking rehabilitation have been shown to include practical factors such as lack of transportation and the cost of traditional assistive devices [Citation24], but also the denial to accept a visual diagnosis and the stigma often associated with blindness [Citation26]. Adults with acquired vision impairment may carry a lifetime of misconceptions about blindness that must be untangled and confronted throughout the rehabilitation process and beyond. These psychosocial considerations may further impede adjustment to vision loss [Citation24]. Such stigma is evidenced by the many inaccurate and problematic depictions of blindness in both literary and visual culture which habitually portray the blind as symbols of pity and charity [Citation27–29].
Recognizing the role of stigma as an impediment, some service organizations have removed the term “blind” from their name to instead highlight that the majority of those who seek rehabilitation today do not have total blindness [Citation30,Citation31]. It is worth noting, however, that the reluctance to use the term “blind” may work to further deepen the stigmatization of blindness and the symbols closely associated with it. Traditional assistive devices which disclose an otherwise invisible visual impairment, for instance, are often abandoned or under-used despite their potential utility [Citation32]. The white cane, arguably the most recognizable symbol of blindness, identifies the user as someone who is blind and can be attached to unwanted attention for those still adjusting to vision loss [Citation33,Citation34]. Adults with remaining functional vision may postpone the adoption of such tools until it is deemed to be necessary, due to fears of being judged or misunderstood. Though the role of braille within this discussion has not been directly examined, it is possible that braille could conjure similar feelings of reluctance for those still adjusting to vision loss, given its role as a prominent symbol of blindness.
It is, however, from the field of adult learning rather than rehabilitation that the greatest insight on the uniqueness of the adult learning process can be gained. Coined by Malcolm Knowles in the 1970s, andragogy as a field of inquiry accentuates the factors which uniquely influence the learning experiences of adults, and which proponents argue should be taken into consideration in any adult training context [Citation2]. Based on empirical research and observations, the andragogical framework is structured around six core assumptions of adult learners [Citation35]. An emphasis is placed on self-directed learning and the notion that the motivation to learn in adulthood is greatly driven by a perceived need to know in order to fill a gap or improve quality of life [Citation2]. In a series of related investigations, Tough [Citation36] observed that adults who undertake to learn something on their own are especially cognizant of the potential benefits as well as the negative consequences that might arise if that learning is abandoned. The model further accentuates the role of prior life experiences which adults bring with them into any learning situation, as a consequence of having lived longer than children. It implies that the richest resources for learning in adulthood reside in the adult learners themselves and in harnessing their previous experiences [Citation2].
Above and beyond these considerations, a variety of other factors may influence the experiences of adult learners generally. These factors may include anxiety about returning to school (or adopting the often long-shed role of learner), resistance to change, poor past academic success which may effect self-confidence and locus of control, rigid schedules and limited time due to family, finances and other adult responsibilities [Citation37]. Such insights have led to the development of paradigms that better respond to the needs of adult learners, such as Universal Design for Learning (premised on the importance of flexibility) [Citation38], transformational learning theory (which acknowledges the relevance of world views) [Citation39], and constructivism (which harnesses the value of prior experience) [Citation40], but such frameworks have gained little attention in the field of braille rehabilitation.
To date, a lack of ample evidence has contributed to ongoing inconsistencies in the ways in which adult and senior braille clients are assessed, trained and supported among rehabilitation centres generally [Citation11]. This is especially true in countries like Canada, where rehabilitation services may vary drastically due to geography and the resulting discrepancies among provincial or regional healthcare and rehabilitation systems [Citation41]. Moreover, questions on improving service delivery have garnered renewed attention in recent years due to legislative efforts at the macro level. The United Nations Convention on the Rights of Persons with Disabilities (UNCRPD), ratified by 181 countries, calls upon states to provide adequate educational and rehabilitation services, including the provision of braille and other alternative format training where required [Citation42]. As rehabilitation agencies encounter a growing number of adults and seniors who may pursue braille training, it will become imperative to understand how the experience of learning braille in adulthood might align or veer from childhood learning, and whether specific enablers or barriers influence this process.
This study aims to explore the experience of learning braille as an adult or senior with acquired vision impairment, and to identify the facilitators and barriers that manifest in different ways throughout this process. A phenomenological approach to analysis was therefore deemed to be most appropriate, given the desire to understand the essence of a shared or common experience that is not yet well understood [Citation43]. Recognizing the importance of foregrounding the first-hand experiences of participants, it is believed that such a qualitative approach will raise aspects of the adult and senior braille rehabilitation experience that might otherwise be overlooked through other methods of inquiry. It is also hoped that the insights gained from this study will serve as the impetus for future tangible recommendations that begin to tackle the obstacles that emerge.
Methods
Eligibility and recruitment
The data for this study are drawn from the transcripts of semi-structured interviews conducted between July 2018 and January 2019. Ethics approval was obtained through the Centre for Interdisciplinary Research in Rehabilitation of Greater-Montreal (CRIR# 1311-0218), a prerequisite to recruiting participants from Montreal-based rehabilitation centres. Additional approval was granted by Vision Loss Rehabilitation Canada (formerly the Canadian National Institute for the Blind) in order to recruit participants outside of Quebec. To take part in the study, participants had to reside anywhere in Canada, had to have learned braille anytime after the age of 21 (the age at which braille would no longer fall under the purview of the educational system), and had to have completed their formal braille training at least one year before participation. Additionally, all participants self-reported meeting the legal definition of blindness (a measure of distance and peripheral vision used to determine access to services in most western countries), defined as a visual acuity of 20/200 or less or a visual field of 20 degrees or less in the better eye with best correction [Citation44] (see Supplementary Appendix A for the interview guide).
The invitation to participate (which also described the eligibility criteria) was circulated internally to rehabilitation agencies and organizations for the blind within Canada and also posted publicly onto social media platforms geared towards blind and low vision Canadians, with moderator approval. Snowball sampling, whereby participants were invited to share the invitation with others in their circles who may be interested, provided additional reach beyond these means [Citation45].
Study design
The creation of the semi-structured interview guide applies the process described by Smith [Citation46] and other qualitative researchers engaged in interpretive phenomenological analysis (IPA) [Citation43, Citation47]. The first and second authors developed an outline through discussion to delineate the general parameters of the interview. It was agreed that the questions guiding the interviews should explore the experience of learning braille in adulthood from three successive time-points (before, during and after formal braille training), in order to acknowledge the circumstances both before and after braille training that may also play a role [Citation48]. Recognition of the continuing nature of the learning process helps to contextualize the decisions which lead participants to pursue braille training and the ways in which braille is applied and understood once formal training has ended. This is especially pertinent given the emphasis in rehabilitation research on understanding the factors which lead some to abandon or under-use seemingly effective assistive devices and techniques as an important component of the overall rehabilitation experience [Citation49–51].
In designing this study, the authors also recognize that self-perception as a construct is dynamic in nature [Citation48]. Adequate distance from the time when a health or rehabilitation intervention occurs is sometimes warranted to more effectively reflect and look back upon its impact, as the overcharge of emotions or fatigue experienced immediately afterwards may bias the lens through which the experience is contextualized [Citation48]. It is for these reasons that eligibility to participate required that participants had completed their formal braille training at least one year before.
Questions were developed based broadly on the categories of the International Classification of Functioning, Disability and Health (ICF) model [Citation52]. The interview questions generated with this framework in mind therefore consider both the person at the centre of the learning process and the environments in which they are situated.
Data collection and sample size
Prior to the start of the interview, participants were provided with a copy of the Information and Consent form in their preferred format (large print, braille, electronic, or read aloud to them on the phone). Informed consent was either provided verbally and audio-recorded or obtained in written form, in accordance with The Declaration of Helsinki and Public Health [Citation53]. The option to provide recorded verbal consent offered an accessible alternative for blind and low vision participants who could not or who preferred not to indicate their consent through written signature or trust in a third party [Citation54], an option which all participants selected. The merits of ensuring flexibility during the data collection phase have been discussed in other research with diverse populations [Citation55], and is especially important for people with disabilities and older adults who may not easily be able to travel to a research site or directly respond to invitations to participate [Citation56]. The individual interviews (which were recorded with participant consent) required roughly 90 min of the participants’ time, and in all cases, both the first and second author were present. The interviews could be completed either by phone or by visiting one of the approved research sites, though all participants chose to take part by phone.
The methodological approach of interpretive phenomenological analysis, as with other qualitative paradigms, is concerned with understanding and foregrounding participant perspectives, and values above all else the richness of data stemming from participant stories [Citation43,Citation46,Citation57]. It is this in-depth exploration of the essence of an experience that phenomenology as an epistemological tradition seeks to unearth [Citation43]. Rigor in phenomenology is therefore cultivated not through achieving statistical power but through the quality and richness of data provided by each participant [Citation58]. The valuing of such first-hand voices gives rise to vital testimony which informs research and practice and gives prominence to what can be overlooked when these first-hand perspectives remain absent from the conversation. This is especially noteworthy given the enduring criticism that the voices of people with disabilities are generally ignored or silenced in the scientific and healthcare research that directly impacts them [Citation59,Citation60]. It was decided that data collection would conclude not when an a priori sample size was achieved, but with theoretical saturation, when no new themes emerged [Citation58]. The resulting sample size (n = 14) is consistent with many prior examples of phenomenological inquiry, where sample sizes of between 10 and 15 are common [Citation43,Citation61].
Data analysis
A bottom-up inductive approach to thematic content analysis (following the steps put forth by Braun and Clarke [Citation62]) was applied in order to ensure that emerging themes were driven by the data:
The recorded interviews were transcribed verbatim by a research assistant. InqScribe [Citation63] software was employed for transcription purposes, as it inserts time stamps at the start of each statement to facilitate later analysis. All participant names and identifying details (such as geographic location and the rehabilitation centre where braille training was pursued) were omitted from the transcripts to ensure anonymity for storage purposes and in the quotes used within the manuscript.
The transcripts were read and reread several times by the first and second authors to gain a general sense of the participants’ observations.
These initial transcripts were reread and both authors began to generate initial codes separately based on significant statements of relevance to the research questions. These codes were then reviewed and discussed. Emerging themes which cluster common threads across transcripts were identified, recognizing that these themes would continue to evolve through an iterative process [Citation64].
Each transcript was reviewed by both authors respectively and the codes (blocks of text) as well as the names and boundaries of themes were discussed and revised through reflection and consensus after the coding of each interview.
The resulting themes and codes provide a description of the essence of the shared experience of learning braille in adulthood, as well as the meanings and contexts which shape the experience [Citation43].
Validity, rigor and trustworthiness
In recognizing that researchers bring with them their own unconscious biases and preconceptions which colour the interpretation of any data [Citation65], the authors made deliberate efforts to engage in a bracketing process through ongoing dialogue with each other; However, it is acknowledged that no act of interpretation is completely free of unconscious bias [Citation43]. Data collection and analysis were conducted jointly by the first and second author. Their distinct yet complimentary backgrounds as a blind braille user and rehabilitation specialist (author 1) and sighted low vision rehabilitation specialist (author 2) ensured that the interpretation of data was not merely a reflection of one specific viewpoint. The third author (doctoral supervisor of author one, internship supervisor for author two) provided additional feedback throughout the project. All transcripts were coded separately by both the first and second author. Where disagreements in codes emerged, these were discussed and consensus was reached collaboratively, leading to an inter-coder agreement coefficient of >98%: Gwet’s agreement coefficient = .988 (range .959 − 1.0).
In discussing the impact of insider epistemology, Asselin posits that it is crucial for the insider researcher to proceed carefully during data collection and analysis, because though the researcher may be intimately connected to an aspect of the topic under study, “she might not understand the subculture, which points to the need for bracketing assumptions” [Citation66]. Here, the first author was innately aware of her role as insider, specifically as a person who is both blind (like the participants being interviewed) and a braille user who has navigated the rehabilitation system available to Canadians with visual impairments, both as a rehabilitation specialist and past service recipient. It emerged that the role as insider led to a perceived sense of unspoken connection felt by participants that contributed to a heightened degree of trustworthiness during information-sharing, in a way that may not have transpired had both researchers been perceived as “outsiders” to the community. Here the first author observed inklings of what Mingus calls “access intimacy,” “that elusive, hard to describe feeling when someone else “gets” your access needs” [Citation67]. Though consciously aware of the insider label attributed to her by participants, and the need to self-check any unconscious biases that arose because of this, the first author equally considered her role as “outsider” – as someone who learned braille early in life and can therefore not ever fully comprehend the experience of learning braille in adulthood after acquired vision impairment. It is this tension that exists when navigating between the insider and outsider role that required the researchers to engage in a process of regularly “reining in and reflexively interrogating their own understandings” [Citation64].
Results
Fourteen participants from Canada took part in this study (7 male, 7 female; 3 from Quebec, 5 from Ontario, 6 from British Columbia). Participants ranged between the ages of 40 and 72 at the time of the interviews (M = 54.6, SD = 9.5) and began learning braille between the ages of 33 and 67 (M = 46.3, SD = 9.5). outlines the age of onset and cause of visual impairment, the age when braille was learned, frequency of braille instruction and the braille codes learned for each participant. First name pseudonyms have been used to protect confidentiality. Note that while some report a childhood visual diagnosis, these are progressive conditions that deteriorate over time though all participants reported being legally blind at the time when braille training was pursued. Three of the participants had additional disabilities above and beyond vision impairment: one self-reported a learning disability, 1 had a severe hearing impairment, and one had fused fingers which prevented him from using a regular keyboard for typing. In total, 9 of the participants had a Bachelor’s degree, 2 had a Master’s, 1 obtained a Ph.D. and 2 completed a High School diploma. Only two participants reported being unemployed, with 6 retired, 3 working full-time, and 3 working in part-time positions. All participants had used print or large print and audio at some point prior to their learning of braille.
Table 1. Participant descriptors.
Twelve of the participants learned braille through a rehabilitation centre, and 2 pursued correspondence courses through adult blindness agencies. Of the 12 who attended a rehabilitation centre, 3 attended a residential program that required them to live in residence throughout the duration of training. Braille training ranged from 5 months to 2.5 years depending on the availability of services and the level of instruction required (whether the participant went on to learn contracted braille or additional braille codes). Training for most participants followed a similar progression, beginning with the alphabet. Activities typically began with short words comprised of the letters learned, and progressed to phrases and passages. Some participants were introduced to braille writing at the start of training, while others began using writing tools once half of the alphabet had been learned. Most used a structured textbook designed for adult braille learners during training sessions. Following their braille training, 5 participants report now using braille on a daily basis; 4 use it several times per week; 3 use it once per week, and 2 participants report using braille a few times per month. summarizes the tasks where braille is currently being used for each participant. Of interest is that only 2 participants report using braille for longer reading tasks such as reading novels, but all expressed that they value braille as an essential skill and do not regret having learned it.
Table 2. Tasks for which participants utilize braille.
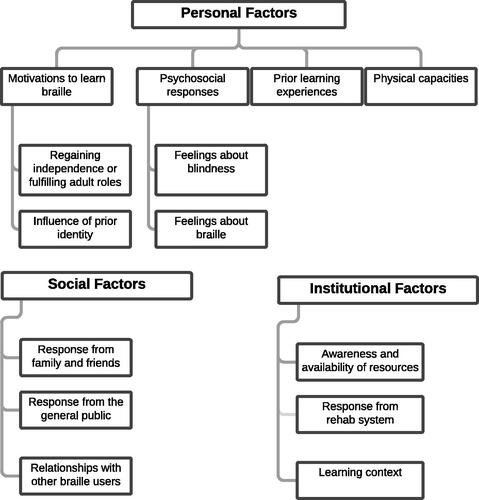
Analysis of the transcripts reveal that the braille learning process for adults and seniors with acquired vision impairment is characterized by personal, social and institutional factors (see for an overview). In the present section, we define and provide examples of each of these three broad themes.
Figure 1. Diagram depicting the hierarchy of personal, social, and institutional themes that characterize the adult braille learning experience.
Theme 1: personal factors
The first broad theme highlighted by participants related to the personal factors attributed to their personality, emotions or intrinsic characteristics that influenced their braille learning journey in different ways. Four categories of interest fall under the theme of personal factors: the personal motivations to learn and use braille; psychosocial responses to blindness and braille; the role of prior learning experiences; and the physical capacities needed to use braille.
Motivations to learn braille
Although others may have influenced the decision to learn braille (as will be discussed in later themes), this decision was ultimately one that was personally motivated and that participants made on their own in order to maintain personally meaningful adult labels. This motivation was described as either a practical necessity to regain independence or as a means of reconnecting with a core part of identity, and was sometimes prompted by a moment characterized as a turning point.
Regaining independence or fulfilling adult roles. For a majority of participants, the personal motivation to learn braille stemmed from an inability to engage in a meaningful home or work activity. The learning of braille was described as being necessary to regain or maintain a label closely tied to adulthood identity (such as employee or parent) and in re-establishing confidence after vision loss:
Margaret: I felt helpless because I couldn’t do things on my own. I was dependent on always asking others. I couldn’t make little notes to myself. Making voice memos didn't work out so well for me. So when I could start writing telephone numbers, shopping lists and notes to myself… Oh my God! I felt absolutely fantastic… It felt a little bit like Lazarus rising.
One participant explained that it was only in her adult years that she made the personal choice to learn braille, in order to fulfill her role as a parent.
Barbara: by the time I started braille, I had three kids… around the time my boy started kindergarten, that's when I started realising I had problems. Spelling lists, homework. I couldn't remember how to spell. I wanted to help my kids more and make it so they had a good education.
Another participant described the personal decision to learn braille as simply a practical necessity in order to maintain his job title, regardless of any feelings he may have had about braille at the time:
Jacob: I guess I might have been my own biggest obstacle in starting to learn it but once I realized that I was going to need a set of tools if I wanted to go back to work, that obstacle went away pretty quickly.
Participants with low vision expressed this same notion; However, their decision was attached to the personal realization that, although certain tasks could still be done with functional vision, learning braille would eliminate perceived inconveniences:
Stephanie: I was just really struggling with magnification, and it was taking me a very long time to look at things. I just eventually thought that, for around the home and things, it would be easier if I could learn braille as opposed to running around my house looking for a magnifying glass and then dealing with the struggle and the strain of trying to focus.
For some participants, the motivation was prompted by the need to take on an entirely new adult role, due to the loss of an integral support system or other drastic life change.
Toby: If there was some materials that I needed to read, I would ask my wife but my wife died at the same time that I retired, so I had to learn braille to fill in those gaps.
Some shared a pivotal or memorable moment that represented a turning point that finally instigated their decision to learn braille. For example, one participant described learning braille (and the broader acceptance of her blindness) as a means of regaining control:
Kelly: Every single week, and sometimes every single day, there was something I could no longer do… that was very, very traumatic. So for me, the process of losing my sight in that way slowly over time was much more traumatic than just being blind. It got to a point where I hurt myself… I felt so stupid. I just walked into a closed door, with a very hot coffee, and I lost it. So I cried and I said… enough! I just want to be blind. If it's going to happen, then I want to be blind now . And when I did become blind it felt like being in a pool, hitting the bottom, and from then on, everything I did would be a positive, a recovery. (…) Blindness is not fun but you know what? Now that I'm blind and so many doors are closed, I'm going to reopen all the doors. As many of them as I can… because I was not going to be a sorry blind person … stuck in her apartment, never coming out again… I couldn't just give up on my life.
Influence of prior identity. Prior identity emerged as a second important personal factor that either helped or hindered the decision to learn braille. Here, participants who perceived themselves as “readers” as a core part of their identity prior to vision loss viewed the learning of braille as a means of regaining a fundamental part of themselves they felt they had lost. In this way, an interesting juxtaposition was drawn by some between identity before and after vision loss, and the disconcerting period “in between,” before braille was learned.
Margaret: Well when I read print I had an internal voice that read along with me. And when I read braille, I get my internal voice back. It’s just … My existential self is kind of reaffirmed. I feel like I am not losing anything (…) It’s that crisis that happens when you have yourself taken away, the things you identify with strongly. Like in my case, reading… and then all of a sudden that’s gone. People say “well do something else”. But remember I’m an adult and you don’t become “something else” readily.
For these participants, the learning of braille afforded them something that could not be gained through other formats alone (such as audio), because they spoke of braille as a form of literacy that is equivalent to the print they remember as sighted readers. This perception served as a motivator for learning braille.
Kelly: I love paper, I love the feel of paper, I love touching paper, I love writing on paper… and I loved the smell of paper, like the smell of a new book…
Margaret: And I placed very high value on things like spelling form, the functions of grammar, and it was hard for me to live in a world that was only audio, and not have contact with commas and paragraphs.
One participant used the analogy of a land-line to explain the need for braille, even when audio is available.
Jacob: My daughter and son-in-law do not have a landline in their house. I have a cell phone and a landline… What happens if something goes wrong with the cell? I could still use my phone, I have a landline. So for me it's knowing that I have something to fall back on.
On the other hand, participants who did not view themselves as “readers” as a core component of their identity prior to vision loss expressed feeling initially uncertain about the need for braille.
Stephanie: I wasn't sure if I'd really use it, because I am not a reader. I don't really sit down and read books. So for me at that time, I was like, well I don't really see how it would be helpful to me, because I'm not interested in sitting down and reading a braille book.
Psychosocial responses
A second category of personal factors that either served as a facilitator or barrier before, during and after braille training related to internalized feelings that participants held about braille and blindness.
Feelings about blindness. Participants either described vision loss as something they accepted as a part of who they are, or as a barrier that prevented them from initially seeking braille and other rehabilitation training. For some participants, vision loss was tied to feelings of denial which prevented them from wanting to adopt tools or behaviours that would disclose their vision impairment to others. In these cases, the reluctance to use a white cane was often used as a comparison.
Stephanie: I didn’t really accept it (vision loss) up until a few years ago (…) I just didn't let on that I was really struggling. (…) I felt at the time it (white cane) was already drawing attention to myself and then everybody was going to know why I can’t see.
On the other hand, a few participants described accepting their vision impairment early on as one part of who they are. Participants in this situation typically had low vision for a longer period of time before it deteriorated further, and may have known others with vision impairment over the years. For these participants, a direct connection was made between their blind identity and their understanding of braille as a logical next step.
Ellen: I've always been extremely positive about my blindness. I was lucky to have a wonderful mother and a supportive family. I just always thought of it [being blind] as another way of being and it’s part of who I am. Braille is just a part of my life.
Some participants explained how their feelings about vision loss changed as a consequence of their braille learning experiences.
Brian: I kind of see the struggles that I've had, and I want to make them better for other people, so that was my motivation to pursue my degree and career. I just want to kind of share that with other people so that I can help them get through the struggles that they have and lead an independent and as full of a life as they can. So my feelings [about vision loss] certainly have … actually become more positive in that I feel like I want to take my strengths and help others.
Others emphasized that adjustment to vision loss is an ongoing process, especially if that vision loss occurred later in life. This acknowledgment is different from an altogether denial of vision loss that may postpone the use of tools such as braille.
Jacob: Well [sighs] I'm going from somebody who could see, and I drove, and I played sports and I did a lot of stuff. I went in one minute from seeing to not seeing… You know, that was 15 years ago, and I'm still not over it. I’m not happy that I’m blind, unlike some of my [congenitally] blind friends (…) I know what I miss (…) I know what it was like to drive… I know what it is not to see my grand daughter's face. and those are things that I miss. So, yeah I'm not happy that I'm blind, but am I going to sit in the corner and cry about it? No. I'm going to live my life to the fullest, to the best that I can.
Feelings about braille. Feelings about braille prior to training functioned as an enabler or obstacle, depending on whether those feelings were attached to certain misconceptions. In particular, beliefs about braille being only for those who are totally blind, that it would be too hard to learn, or that it is only for those who engage in extensive reading emerged as important and reoccurring considerations.
While some participants understood that braille could be used by both people who are blind and those who have low vision, some expressed that they initially held the misconception that braille was only for those who were fully blind. This stereotype served to delay the start of training, especially if the person in question felt a sense of stigma towards blindness as a whole.
Seth: I knew where to go. I had good contacts [to learn braille]. There was a group at the time and I went to a couple of meetings, but I was kind of turned off because they were all blind… and I didn’t think that I was that bad yet.
The notion that braille would be too hard to learn or that one has to be exceptionally smart to learn it also played an influential role. For some, this misperception ironically served as a motivator – a challenge to overcome – particularly if they viewed intelligence as a positive attribute.
Margaret: Most of the people were fairly educated people who liked to read (…) So I’d say that what these two ladies have in common is that they're really smart [laughing] so I don't know if that plays in anything but they're really intellectually bright…
On the other hand, others described that they feared braille would be hard to learn initially, but that this misconception dissipated once the logic of the braille system was revealed to them through training. Understanding the rationale behind the code served as a helpful motivator.
Thomas: I actually came to enjoy it. At first I thought it was going to be really hard. Then I started learning the logic [behind the symbols]… I realized that made it easier.
Finally, some participants described that the delay in initially learning braille or even fully engaging with the learning process stemmed from the misconception that braille was primarily for extensive reading. In these cases, there was a lack of awareness of the different ways in which braille could be applicable to their lives.
Stephanie: I didn't go into it with a great understanding but it has helped me tons now that I know (…) I didn't realize all of the uses there were for braille. Especially labeling. That's something that I hadn't really thought about. I really just thought it was for reading books.
The role of prior learning experiences
Prior learning experiences served as invisible enablers or barriers to learning, depending on whether they were associated with positive or negative memories. For participants who held positive memories of learning and who looked back upon their previous learning experiences with fondness, these other learning contexts served as examples to motivate learning. For example, some participants used the analogy of first learning the alphabet or first learning to tie shoelaces as reference points to motivate their braille learning.
Margaret: Remember when you were a kid learning print. when you start in kindergarten, you start slow and then the next thing you know, after a number of years, you won't even notice the task and you'll be reading easily… It’s like when you’re a kid with your shoelace, the first time you tie your shoelace, you're a little kid and you don't think about it you're just, “oh my god, my laces are done!” that was a giant leap forward, then you know all kinds of things are possible, you're heading down the right road.
Some used the analogy of learning other skills even as adults as positive reference points
Jacob: I’m just old enough that I remember getting one of the first computers… All of a sudden… this contraption called a computer landed on my desk with a keyboard and they said "You're going to learn how to use this" and I went “what is that?" [laughs]… so I had to learn how to type… So after losing my eyesight…. I thought well I’m going to have to communicate. So how will I do that? Well, braille.
These positive learning reference points influenced not only feelings towards learning a new skill in adulthood, but also the specific learning strategies applied. For example, one participant described herself as a visual learner in the past, and drew on visual memory strategies to facilitate braille learning.
Rachel: Because I had eyesight, there was a visual connection I saw. I would say “Okay, the letter “a” is like a circle… and the letter “d” in braille faces the correct way [like the letter d in print] (…) I knew that helped me.
Another participant described the lack of self-checking study tools as an impediment to learning braille, based on his past study habits.
Toby: I wished we had… the answers at the back of the book… So when you’re doing your [braille] exercises you could… look ahead, test yourself. I used to always work ahead in school [because of my low vision] so that when the class reached a lesson, I had some idea what the lesson was about, even if I couldn’t see the blackboard.
On the other hand, some participants shared negative previous learning experiences and the fact that they did not view themselves as strong learners. For example, when asked whether her fear of braille or her confidence as a learner held her back initially, one participant said:
Stephanie: Me as a learner. I really thought that would hold me back a little bit. I would think "I don't know if I can do this!"
Physical capacities
Though physical capacities such as the role of tactile perception were mentioned by some, it is worth noting that these were by no means the most frequently highlighted personal factors. Here, some participants expressed the frustration they felt at the start of training when developing the tactile skills needed to recognize braille symbols, or the hand movements needed to maintain position on a braille page. For some participants, this frustration served as a discouragement at the start of training.
Stephanie: For me, it was quite frustrating at first. I had a really hard time staying on the lines. I still struggle with it a little bit. Because I end up with bad posture and I rub a little bit where I shouldn't be rubbing, I should be gliding. So I found it a bit challenging.
Some participants highlighted that difficulties with tactile perception were greatest at the start of training, but also returned when learning more advanced symbols that were not being encountered outside of training sessions.
Barbara: Learning the alphabet, numbers and punctuation was easy. The basic things you use every day. But stuff I don’t use, like some of the contractions, I wouldn’t put in my long-term braille memory. It made it harder for me. My mental capacity to hold it was harder, because I was older.
Finally, all participants highlighted that the frustration related to tactile perception diminished over time as proper techniques developed.
Jacob: Trying to memorize it at first was difficult… I won't say it was easy, it was not. I got frustrated with it… because I was a visual learner… before I lost my eyesight I would learn stuff by watching it get done… Eventually I figured out how to do it and it started going well. Once I got it, then it became pretty easy.
Theme 2: social factors
The second broad theme related to the social factors which influenced the braille learning process. Here, participants emphasized the role of sighted family and friends, the response from the general public, and the influence of knowing other more experienced braille users.
Response from family and friends
Participants highlighted the influence of biases or misconceptions held by family and friends about braille, and the role of family support during the braille learning process.
Margaret: There was a presumption that I would learn Braille… And I have to say it's really funny, people think "Oh, so you lose your vision, you know how to read Braille!" like it comes with the vision loss… I was a little frustrated because, at that point… I was having difficulty finding someone to teach braille to me! I would say that people expecting that you will learn braille is not the same thing as encouraging you.
Other participants shared comments from family members who felt that braille would be too difficult to learn, and this may have deepened the level of discouragement felt.
Brian: Some of the people maybe saw that I was getting a little frustrated with how I wasn't able to apply it as quickly as I thought, or read as much as I wanted to, and at that point they maybe got a little discouraging, and would say, "Well you don't really need it, if it's that difficult". I think they were trying to be helpful to me, but I don't think that was really helpful.
On the other hand, for some, comments from family and friends who felt impressed because they held the belief that braille would be too difficult to learn served as a source of motivation or pride.
Kelly: there are many things that I needed help with, or that I couldn't do as quickly… but this I can do and they can't!
Some participants with low vision made the point that family members may not have been aware of the need for braille once training began, especially if the learner still outwardly appeared to be coping visually.
Stephanie: I think a lot of my family and friends didn't realize how much I really needed it - because I did things well - I'm very bubbly and just didn't let on that I was really struggling.
Other participants highlighted that, though well-meaning, responses from family members were influenced by the feelings towards braille that those family members carried with them based on their own past experiences.
Barbara: I asked them [at the time] why they wanted me to learn print. Later on I learned from my mom that she didn’t want me getting headaches. She told me that she could sit in a dark room and read braille, but as soon as there was light, it would give her headaches. She didn’t want me to have those same problems. She didn’t discourage me from learning it, but didn’t want me to learn it too soon.
Many participants described the impact of family and friends who provided tangible positive support throughout the learning process and beyond. This support may have included driving them to training interventions, learning some braille to facilitate household communication, or simply showing a level of awareness.
Toby: well, for instance, I needed somebody to tell me what my CDs were [so that I could label them in braille]. I had a neighbour who would come and go through my CDs with me at the time.
Jacob: my wife was supportive and said "you take the time you need to do what it takes to get back to work"… She made sure that if I had to go to the rehab centre, she was there to take me… Our lives to some extent were put on hold.
Margaret: I think that when people are familiar then they are much more likely to be respectful with the [braille] material itself. Not to leave it out or put it in an obscure place… I find even now having friends who come over and if they bring me something and take the time to label it in braille, that’s fantastic! Very small things make it really easy… I do think it's helpful if they know some braille… just Grade One braille.
Above all else, participants highlighted the need to provide resources to family members during the braille learning process. For example, one participant describes how the lack of informational resources for family members influenced his learning experience:
Brian: I think a supportive environment really helps encourage someone to stick with it and to learn. had my family members been exposed to any kind of information about why it was important to learn braille, maybe they would have encouraged it more. I mean, they didn't discourage it, but they didn't encourage it either. Education for family members might help and so the advice I would give is to have that available to them, or point the blind individual to resources they can share with their family to help.
Response from the general public
Participants overwhelmingly described reactions from the general public. Some participants drew a distinction between the white cane or guide dog and braille as symbols that put the user on display, and connected this to their broader acceptance of blindness.
Thomas: The cane is more obvious, but if you’re reading braille in public it is the same thing. I’m not concerned about that anymore. In the beginning you kind of have to decide to accept that [attention] or not.
Others highlighted that the usual social contract is broken in some interactions, where members of the public behave in ways that would normally seem inappropriate.
Kelly: Sometimes people will comment. One time a man (this was when I was beginning to learn braille) he said "if you're going to be that slow I don't even know why you bother!"
This same participant described an interaction with a stranger who physically removed a braille book from her hands, an experience which she described as distressing as a new braille user.
Kelly: I said, "what's happening? what's happening?" and this woman said "oh, I wanted to show my grandson!" and I said "you can't do that! Do you do that to sighted people, come to them and remove their book from out of their hands?" (…) She gave it back to me and said "read to him?" and I said "please don't do that."
Participants overwhelmingly highlighted that the misconceptions held by the general public remain a pervasive problem. For some, these social interactions translated into a source of empowerment and raised their own awareness of their visible platform.
Ellen: You know how people take sign language just for fun? So I thought, why don’t people learn braille like that? I like to bring braille to people… Try to get rid of all those misconceptions.
Influence of other braille users
Most participants revealed the ways in which knowing (or not knowing) other braille users influenced their braille learning experiences. For example, one participant highlighted the influence of seeing first-hand examples of braille being used before she began learning braille:
Rachel: This one lady, she completed a degree and (…) she read all her books in braille. I think that was very important for me, to understand that if you have that background in braille, it allows you to have a lot more opportunity.
Others highlighted the value of knowing other braille users during the learning process, as a useful resource or point of reference for the ways in which braille could be used in daily life.
Brian: I think if you can bounce ideas off other people of what they're using braille to do, there is value in that for sure. I don't think it's the be all and end all but I think just having a connection with other people who are using braille is important if you want to make that a part of your life.
On the other hand, some participants expressed that the lack of these social connections functioned as an early barrier, especially if a lack of information or stigma delayed the learning of braille.
Stephanie: I hadn't really met a lot of blind people myself so you know I didn't really have any interaction, which is something personally I think is a lacking feature in Canada.
Above and beyond the influence of having these practical reference points, an interesting thread emerged related to the experience of identifying with a larger braille or blindness community and the influence this had on identity formation during the braille learning process. Here, some participants described the notion that remaining a non-braille reader in a sighted world was more disabling than being a braille reader in a blind world.
Ellen: I knew totally blind people who knew braille and read it extraordinarily well. You know, it was the weirdest experience. I went to a restaurant with a totally blind friend… and they read the menu to me. I couldn’t read the menu. So I’m stuck in this nowhere land, because I’m in the middle. I can’t read print, but I can’t read braille. It was like when I had blind friends that would play [braille] Scrabble, but… I couldn’t do it. Then finally when I learned braille… I could do these things. It felt so empowering.
Linked to this, some participants touched on the influence of coming to identify with a braille or blindness community during the braille learning process and the broader impact this had on them as adult braille learners.
Kelly: In a funny way it felt good to be part of a very select club… For me, it was proof positive that there is a need for expression, that there is a need for literacy… that blind people could persevere… I was so proud to be part of that group.
For participants who acknowledged feeling this sense of community, the learning and use of braille often came to be viewed through an identity-based perspective.
Ellen: It was so liberating… I know I sound a bit over the top, but it was almost like being given my heritage, finally. Being given what I felt I should have been given because I was born blind. Braille is the reading mode of the blind, but I was deprived of that, and it made me really upset and sad.
Theme 3: institutional factors
The final theme emphasized by participants underscored the institutional factors which considerably shaped the adult braille learning journey. Overwhelmingly, participants highlighted that they encountered institutional barriers at different points of the learning trajectory. Specifically, participants emphasized the role of awareness and availability of resources, the response from the rehabilitation system, and the influence of learning context.
Awareness and availability of resources
Several participants described that once they decided to pursue braille training, they encountered difficulties in securing that training, due to a lack of resources, long wait lists or a lack of awareness of where to go. One participant described having to turn to a correspondence course because he could not find training where he lived.
Brian: Looking back now, I probably would have preferred to have either group or one-on-one instruction which would have been much more effective but due to the lack of services that was not an option.
Another participant described that even now that she has learned braille, she is unaware of training resources in her region to further her skills:
Margaret: I had difficulty finding someone who would teach me braille! Even now… I don’t know right now how to learn, if I wanted to learn today. For somebody with my enthusiasm, you think I’d be able to easily find out about braille continuing education but no.
On the other hand, participants who lived in regions where rehabilitation fell under provincial healthcare jurisdiction did not encounter difficulties when seeking training. However, long wait lists often postponed the start of training where these services were more readily available.
Most participants expressed that they could not find reading materials to maintain their braille skills during and after training, either due to a lack of resources for adults or a lack of awareness about where to search.
Brian: One of the biggest obstacles is that I wanted to order some braille books to practice when I first started learning. I remember it took almost a year for me to even get anything mailed to me (…) So that first year of taking courses, I didn't really have any material to practice with beyond the textbook and I think that discouraged me.
A final reoccurring thread related to lack of access to braille devices, due to cost and the lack of funding programs specifically for adults. For example, one participant describes having seen electronic braille displays during training and how having access to one of his own would have facilitated learning.
Thomas: We did see a braille display and it was really neat, but it was so expensive. I probably would have used braille more if I actually would have had my own braille display.
Another participant highlighted that having access to such a tool would have been a beneficial supplement to her as an adult learner with decreased tactile sensitivity.
Stephanie: I have a friend here now that has been letting me play with his braille display and I, for one, struggle feeling the dots, and found the braille display so much easier. It is a cost issue.
Response from rehabilitation system
In telling their stories, several participants often returned to what they viewed as a perceived reluctance to provide braille training among some rehabilitation specialists, due to their beliefs about braille and aging.
For example, a participant highlighted the strong emotional response she experienced when she was told that she should wait for further vision loss before pursuing braille:
Kelly: I could not see the dots themselves, but I could see the shadow of the dots. And because I could see the shadow of the dots, he said “No, you’re not ready” and I almost cried. I thought ‘is this it?’ I could learn. I could learn to read a new code. Write a new code. I could touch paper again… And you’re saying no? I was devastated.
Some participants felt that their advanced age led rehabilitation specialists to believe that they would be unable to succeed to the same degree as younger clients:
Toby: He was quite doubtful [about me taking the braille test]. He said “I don’t know… some younger people can't do it”
Learning context
Participants described how learning context (the inclusion or exclusion of different learning approaches) influenced their training experiences. Specifically, participants emphasized the role of relevant and motivating materials for adults, and the impact of learning alone or with others.
There was a consensus among participants that it is difficult to remain motivated as an adult learner when materials used in training are either deemed to be irrelevant or too far below the age level of adult learners. For example, one participant described the positive impact of selecting her own reading material during training sessions. In her case, this book also provided her with valuable information as a newly blinded adult:
Kelly: This book had a dual purpose. Allowing me to practice braille in an unstructured way and of course there was a lot of information in there for somebody who was very recently blind.
Another participant expressed that the lack of relevant materials prevented him from reading braille between sessions. Here, he felt that access to a braille display would have permitted him to read personally meaningful material, such as emails and websites:
Brian: I think it would have made a huge difference because if I had the braille display I probably would have made myself use it more with the computer and practiced a lot more. It would have opened a lot of doors to me but of course we don't have any source of funding in Canada for that.
On the other hand, other participants highlighted that the need for relevant materials for adults must be balanced with those that are at an appropriate level. For example, one participant described that it was helpful for her to read books that were familiar to her from her childhood. This allowed her to encounter new braille symbols but within the context of familiar content:
Rachel: I chose a book that I was particularly interested in… Black Beauty, Because I knew the story. It helped to rote learn the new contractions.
Another participant noted that the inclusion of personally meaningful projects during sessions helped her develop an appreciation for braille and the role it could play in her own life.
Ellen: In our braille class, they wanted us to do a project. I ended up making a braille menu for a restaurant that didn’t have one. I had them email me the text and my project was to put it all together… learn the braille contractions and I printed it out and I had to bind it. And that made it more relevant, more personal.
Finally, participants highlighted the impact of either learning braille alone or with other adult clients. For many participants, learning in a group context provided a level of support and a sense of unified community that they felt they had been lacking.
Margaret: The atmosphere was really informal and I would say that we were all unified by a common cause (…) It also really helped with motivation to punctuate our progress with little celebrations of achievement.
Another participant highlighted that learning in a group context provided her with mentors, but also allowed her to develop her own confidence through the process of helping less advanced learners.
Stephanie: Having other peers in the class who were a bit further ahead helped me. And I was helping the new person, and that was kind of a little bit of an encouragement for me too because I was so new to braille yet at the same time I was able to help someone.
On the other hand, some participants emphasized the value of maintaining different options for adult learners, who may have other responsibilities or impairments that require them to learn at home or on a one-on-one basis:
Jacob: I’m glad that I learned it privately. As a kid it’s not so bad, but as an adult I needed to learn in a quiet space and I needed to be with somebody who was very patient. Not judgmental about it and who would let me learn at my own pace.
Discussion
The purpose of this study was to explore the experiences of working-age and older adults who pursue braille rehabilitation training, and to identify the enablers and barriers which may influence this process. Participants describe that the adult braille learning journey is shaped by a variety of personal, social and institutional factors. Their insights provide important context for future research and practice, and help to work towards the development of evidence-based recommendations to address existing gaps.
Personal factors
Among the personal factors that emerged, it can be seen that the motivation to learn braille is typically instigated by a perceived “need to know” in order to maintain a life activity or meaningful adult label. It is true that this echoes the andragogical assertion that learning is most effective when the decision to learn is made deliberately in order to tangibly improve some aspect of life [Citation35]. However, a barrier appears to arise when the prospective learner is operating upon misconceptions about what braille is and who it can serve. This is evidenced by participants who expressed initial misconceptions that may have delayed their training, such as the belief that braille is only for those who are fully blind or for those who engage in extensive reading. The onus therefore remains with the rehabilitation specialist to be cognizant of unspoken misconceptions that prospective braille clients might hold, and to foreground the practical usage of braille in daily life during any learning situation.
Prior identity also emerged as an important personal factor that either motivated or impeded the decision to pursue braille, regardless of its potential utility. Here, a subtle but seemingly important distinction is drawn between those who attached the “reader” label to their identity prior to vision loss, and those who did not. For individuals who viewed themselves as readers and who felt a personal connection to the physicality of reading, braille enables them to reconnect with a part of themselves they feel they had lost. This concept is echoed in comments from participants who speak of braille literacy as “the self reaffirmed” or “like Lazarus rising” (Margaret).
The concept of the perceived loss of self-identity that accompanies acquired impairment has been explored in other studies in the field of rehabilitation, though not specifically in relation to braille. Levack et al. [Citation68], for instance, describes how some participants with acquired traumatic brain injury (TBI) feel that their self-identity becomes fragmented or disrupted following diagnosis, leading them to speak of the “self” before and after TBI as two separate identities. In a similar way, braille for some participants appears to bridge the gap between their identity before and after the onset of vision loss. The implication of this is that while other alternative formats (such as audio) may equally enable the completion of tasks, they will not address the identity gap felt by some clients. Rehabilitation specialists must therefore consider not only what tools may be best to complete a specific task, but also the holistic experiences attached to literacy that adults carry with them as important sources of motivation.
Previous learning experiences, whether positive or negative, appear to also influence both the motivation to learn braille and the views adults have of themselves as learners, echoing the notion that experience is the adult learners living textbook [Citation35]. Participants describe the use of past learning tactics which served them well, such as drawing on visual imagery (Rachel) or the use of self-checking study methods (Toby). Others turn to examples of previous learning experiences as positive reference points to motivate learning (as with Margaret who uses the analogy of learning to tie her shoelaces or Jacob who remembers the initial learning curve when computers were introduced to the workplace). On the other hand, we can see that prior learning experiences can also serve as invisible impediments to learning if they are associated with failure.
Though little attention has been devoted to previous learning within the adult braille rehabilitation context, a wide body of research from other domains explores the role of past learning memories on adult motivation and self-efficacy. According to expectancy-value theory, for instance, learning motivation is a function of both the expectancy of success (“Can I do this?”) and the subjective value ascribed to a learning task (“Do I want to do this?”), and it is influenced by a variety of preceding variables including affective learning memories [Citation69]. In a sample of 300 adults, for example, Gorges illustrates how previous education and the memories associated with it function as important predictors of adult learning engagement [Citation69]. Research also suggests that adults whose metacognitive skills are well developed are more able and motivated to learn [Citation70]. In this way, adult learners gain a sense of self-agency when they are included in the assessment process (by asking them what works and what could be done differently) and by directly incorporating learning tactics that have worked effectively for them in the past. Our findings demonstrate that prior experiences should be considered as part of the often invisible baggage that adults carry with them, and that positive learning experiences (including accumulated interests and expertise) should be harnessed to enhance training outcomes.
Social factors
At the level of social factors, it is evident that reactions from family and friends play an influential role during the braille learning process, even though they are not physically in the room when learning takes place. Participants highlight the value of tangible support that family members provide, but also the negative impact of misconceptions held by family and friends. The stories shared illustrate the ways in which family and friends may also be adjusting to vision loss in the background. They may either not be aware of the need for braille if the client is “passing” as sighted or may themselves discouraged the use of braille based on their unconscious biases. Participants accentuated the need for greater information geared towards family and friends, such as basic awareness to dispel myths about braille and (in some cases) exposure to the braille alphabet to facilitate communication. In fact, rehabilitation research is replete with examples of how support from those in a client’s inner circle can influence training outcomes or contribute to the abandonment or under-use of compensatory tools [Citation71]. While the role of family members (and in particular, parents) is an integral consideration during childhood braille learning [Citation72], it is clear that a greater emphasis should be placed on providing adult clients with resources to share with family and friends, and that these social networks can function as positive supports when considered.
Moving to the macro level, these findings also point to the potential influence of societal perceptions of braille and blindness during the adult braille learning process. Through the anecdotes of participant interactions with members of the public, a subtle yet clinically significant distinction begins to emerge. When blindness is viewed through a medical model lens [Citation73] (as a stigma or impediment), braille is by extension also viewed as an outward symbol of deficit: “I didn’t think I was that bad yet” (Seth); “I felt at the time it (white cane) was already drawing attention to myself” (Stephanie). On the other hand, when blindness comes to be viewed through a social model lens [Citation73] or as “simply a part of who [you are]” (Ellen), then braille by extension is perceived as a symbol of independence that empowers the user: “it [learning braille] felt so liberating…almost like being given my heritage finally” (Ellen). What participants illustrate through their comments is that braille can become entangled and inseparable from the self-identity that adult braille learners with acquired vision impairment must negotiate.
Though theoretical on the surface, these insights carry important implications for adult braille learning. Ellen, for example, described that what disabled her prior to learning braille was not her blindness, but her inability to access information. She shared the feeling of being “disabled” in the presence of her braille-using friends who could read the restaurant menu. Coming to this understanding reinforces that braille is not an impediment but instead an empowering tool that enabled her to achieve her goals (because her braille-using blind friends were not disabled in this moment, though she was). Though adjustment to vision loss is an ongoing process, these stories raise the importance of fostering the understanding of braille as a tool that ultimately minimizes the disabling impact of blindness. Several participants describe that this social definition of blindness is often forged through the connections made with other experienced braille users during the learning process, or in coming to feel as though they are part of a larger blindness community. Although participants highlight the need to ensure flexible learning options, they also stress that access to other braille users as mentors and sources of peer-support helps to address many of the emotions attached to braille as a symbol of blindness. It therefore becomes imperative to consider the value of group training paradigms for those who would benefit from it [Citation74], and the inclusion of peer-support initiatives to bridge learning both during and once training concludes.
The influence of societal responses to braille during the learning process raises another important fact. Misconceptions about blindness and braille can occasionally lead to uncomfortable or unwanted social interactions for adult braille learners (as described by Kelly who had a book physically removed from her hands). The tendency to view people who use braille in public as exceptional simply because they are reading resonates with what disability scholars have come to call “inspiration porn” [Citation75], and underscores the level of public education that is still required. Previous studies, for instance, illustrate how challenges in the physical environment including attitudinal barriers lead some older adults with acquired low vision to retreat to the private sphere [Citation76]. In this way, clients can be equipped with the tools that they need to manage vision loss (such as braille), but may still encounter barriers outside the training room when using the tools that increase their hypervisibility [Citation77]. These interactions, which may be distressing to adult braille learners who are new to vision impairment, raise the need to not merely “rehabilitate” clients, but also to consider ways to rehabilitate a society that continues to influence the outcomes of the adults who are served.
Institutional factors
The institutional factors discussed by participants point to the benefit of having access to materials and tools geared towards adults, both to bridge learning between sessions and to maintain braille skills once formal training has concluded. However, a recurring obstacle reiterated by almost all participants was that these practice resources were not consistently available to adult braille learners in Canada, and that the cost of electronic braille devices (upwards of $3 000), which would increase access to braille, remains prohibitive. Currently, governmental funding programs to purchase assistive devices (including braille devices) are not available in all provinces, and typically only support clients who are either studying or working, even when they are available [Citation78]. The problem that arises is that adults with newly acquired vision loss are often temporarily neither working nor studying, but can only return to such forms of social participation once their blindness skills (such as braille) are at an adequate level [Citation79]. Similarly, eligibility criteria based upon these requirements will impede access for older adults with acquired vision impairment who are retired but who nonetheless might benefit from braille for home, recreation and personal communication needs. The consequence is that the inability for older adults to develop adequate braille skills during training or the abandonment of braille in the post-training period may wrongly be viewed as a problem with braille as an appropriate tool, rather than due to the insufficient supports provided to adults who genuinely wish to use braille but cannot: “I probably would have used braille more if I actually would have had my own braille display” (Thomas). This points to the need to develop practice materials and tools geared towards the age level and interests of adult learners, and to advocate for the expansion of funding regimes that account for the needs of older adults with acquired vision loss. Though the introduction of lower cost electronic braille devices have gained prominence in recent years [Citation80], these findings also further the need to reduce the cost of production attributed to these tools.
Finally, several participants described a perceived reluctance on the part of rehabilitation specialists to provide braille training, and the considerable distress that this caused for them during the time when they attempted to access these services. While this certainly does not reflect the response of all professionals, these comments do suggest that unconscious biases about both braille and aging can impact professional judgments and decision-making. Implicit in some comments is that misconceptions about the abilities of older adults in particular may be influencing decisions about whether braille should be considered as a viable option. Prior research has explored the influence of ageism in health care and rehabilitation, illustrating the ways in which implicit views about the elderly may unconsciously determine the amount and quality of care delivered to older adults [Citation81]. Similarly, Wittenstein and Pardee [Citation82] found a direct relationship between the training that blindness professionals receive and their attitudes towards braille, with those who receive more training in braille holding more positive attitudes. These findings bolster the need for rehabilitation specialists to remain self-reflexive and aware of the impact of their unconscious biases, and to ensure that adequate training addresses the misconceptions that rehabilitation specialists may carry with them into the field. Future research should further explore how the often unconscious lens through which both braille and aging are perceived might be informing views on clinical decision-making.
Limitations and future research priorities
While these results provide vital context about existing barriers, they do not directly probe the experiences of working-age and older adults who tried but ultimately did not prevail with their braille learning goals. This raises a methodological challenge of how to best reach out to clients who abandoned their training or chose not to pursue it in the first place. Often, clients may feel uneasy about sharing these experiences, especially if they view them as personal failures. However, it is this perspective that will provide a more comprehensive picture of why some are able to persist and others encounter obstacles that are ultimately insurmountable. Mixed-method longitudinal studies that follow adult braille clients from referral to the completion (or abandonment) of training could help to address this gap.
A second related limitation stems from the fact that the participants in the present study (save for two) lived in larger Canadian cities during the time of braille training. Despite the differences in residence, participants highlighted reoccurring themes which suggest that similar facilitators and barriers are experienced by adults who pursue braille rehabilitation training regardless of location. However, those living outside large cities or in smaller provinces encounter additional barriers that must be addressed. Though no research on braille services in rural Canada currently exists, a cursory look at healthcare research generally points to the lack of available services in rural areas, a lack of awareness among prospective clients, and healthcare and rehabilitation models which do not adequately acknowledge cultural context, such as the deep-rooted history between indigenous and non-indigenous peoples [Citation83]. Though invitations to participate were advertised widely and telephone-based interviews were provided as available options for those who could not travel to central locations, no prospective participants from these other geographic areas contacted the research team. Future studies should strive to consider alternative methods of recruitment that better facilitate and encourage participation from adults who live in these regions. The lack of communication from those residing in rural areas or smaller provinces may also suggest that braille training has not routinely been as available to adults in these regions. This raises important concerns that warrant future attention.
Finally, although the current investigation is one of the very few braille studies that incorporates the perspective of older adults, most participants learned braille in middle-age. This may reflect the reality that few older adults above the age of 60 are referred to braille training. This is alluded to in the current findings which point to a possible stigma towards aging and a hesitancy among some (but not all) rehabilitation specialists to view braille as a viable option for older adults. Future research should focus more exclusively on any older adults who have learned braille, to add to the knowledge that this current study provides.
Conclusion
This study is among the first to explore the experiences of working-age and older adults who pursue braille rehabilitation training. In following the braille learning journey that participants describe, it becomes clear that a variety of personal, social and institutional factors can either facilitate or impede adult braille learning before, during and after training concludes. Findings bring to the forefront barriers that can be addressed through policy and practice changes. Results also complicate the notion that physical factors (such as declines in tactile perception) are solely or primarily responsible for shaping the training outcomes of older braille clients. It can also be seen that many of the variables highlighted by participants reflect existing andragogical learning models. Future research can expand upon these insights to work towards an adult braille learning theory, in order to contemplate how adult braille learning may veer from other forms of adult learning, and the practice implications of these distinctions. Undoubtedly, understanding the enablers and barriers encountered by older adults who pursue braille training will become increasingly important in decades to come.
Ethics approval
Ethics approval was obtained through the Centre for Interdisciplinary Research in Rehabilitation of Greater-Montreal (CRIR# 1311-0218), a prerequisite for recruiting participants through the Montreal-based network of vision rehabilitation centres. Additional approval was granted by Vision Loss Rehabilitation Canada (formerly the Canadian National Institute for the Blind, the largest Canadian provider of blindness and low vision rehabilitation services outside of Quebec) in order to facilitate the recruitment of participants residing in other provinces.
Supplementary_Appendix_A.docx
Download MS Word (24.5 KB)Acknowledgments
The authors would like to thank research assistants Camille Demers and Fatima Tangkhpanya who produced the verbatim transcripts of participant interviews.
Disclosure statement
The authors report no conflicts of interest.
Additional information
Funding
References
- Ponchillia PE, Ponchillia SV. Foundations of rehabilitation teaching with persons who are blind or visually impaired. New York (NY): American Foundation for the Blind; 1996.
- Knowles MS, Holton EF, Swanson RA. The adult learner: the definitive classic in adult education and human resource development. London & New York: Routledge; 2015.
- Bourne RRA, Flaxman SR, Braithwaite T, et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(9):e888–e897.
- Varma R, Vajaranant T, Burkemper B. Visual impairment and blindness in adults in the United States: demographic and geographic variations from 2015 to 2050. J Am Med Assoc Opthalmol. 2016;134(7):802–809.
- Kleege G. Visible braille/invisible blindness. J Vis Cult. 2006;5(2):209–218.
- Graves A. Braille literacy statistics research study: history and politics of the "braille reader statistic": a summary of AFB leadership conference session on education. J Vis Impair Blind. 2018;112(3):328–331.
- Dixon J, editor. Braille into the next milennium. Washington (DC): National Library Service for the Blind and Physically Handicapped; 2000.
- Mick P, Hämäläinen A, Kolisang L, et al. The prevalence of hearing and vision loss in older Canadians: an analysis of Data from the Canadian Longitudinal Study on Aging; 2019. https://doi.org/https://doi.org/10.31234/osf.io/v7kr5
- Holbrook MC, McCarthy T, Kamei-Hannan C. Foundations of education: volume i: history and theory of teaching children and youths with visual impairments. 3rd ed. New York: AFB Press; 2017.
- Wormsley DP, D'Andrea FM. Instructional strategies for braille literacy. New York (NY): American Foundation for the Blind; 1997.
- Ponchillia PE, Durant PA. Teaching behaviors and attitudes of braille instructors in adult rehabilitation centers. J Vis Impair Blind. 1995;89(5):432–439.
- Hannan CK. Review of research: neuroscience and the impact of brain plasticity on braille reading. J Vis Impair Blind. 2006;100(7):397–413.
- Sadato N, Okada T, Honda M, et al. Critical period for cross-modal plasticity in blind humans: a functional MRI study. Neuroimage. 2002;16(2):389–400.
- Sterr A, Muller M, Elbert T, et al. Development of cortical reorganization in the somatosensory cortex of adult Braille students. Electroencephalogr Clin Neurophysiol Suppl. 1999;49:292–298.
- Stevens JC. Aging and spatial acuity of touch. J Gerontol. 1992;47(1):P35–P40.
- Stevens JC, Foulke E, Patterson MQ. Tactile acuity, aging, and braille reading in long-term blindness. J Exp Psychol Appl. 1996;2(2):91–106.
- Goldreich D, Kanics IM. Tactile acuity is enhanced in blindness. J Neurosci. 2003;23(8):3439–3445.
- Goldreich D, Kanics IM. Performance of blind and sighted humans on a tactile grating detection task. Percept Psychophys. 2006;68(8):1363–1371.
- Legge GE, Madison CM, Vaughn BN, et al. Retention of high tactile acuity throughout the life span in blindness. Percept Psychophys. 2008;70(8):1471–1488.
- Legge GE, Madison CM, Mansfield JS. Measuring braille reading speed with the MNREAD test. Vis Impair Res. 1999;1(3):131–145.
- Schroeder FK. Perceptions of braille usage by legally blind adults. J Vis Impair Blind. 1996;90(3):210–218.
- Ryles R. The impact of braille reading skills on employment, income, education, and reading habits. J Vis Impair Blind. 1996;90(3):219–226.
- Silverman AM, Bell EC. The association between braille reading history and well-being for blind adults. JBIR. 2018;8(1):1–1. https://www.nfb.org/images/nfb/publications/jbir/jbir18/jbir080103.html
- Southall K, Wittich W. Barriers to low vision rehabilitation: a qualitative approach. J Vis Impair Blind. 2012;106(5):261–274.
- Pollard TL, Simpson JA, Lamoureux EL, et al. Barriers to accessing low vision services. Oph Phys Optics. 2003;23(4):321–327.
- Spafford MM, Laliberte Rudman D, Leipert BD, et al. When self-presentation Trumps access: why older adults with low vision go without low-vision services. J Appl Gerontol. 2010;29(5):579–602.
- Fraser SA, Kenyon V, Lagacé M, et al. Stereotypes associated with age-related conditions and assistive device use in Canadian media. Gerontologist. 2016;56(6):1023–1032.
- Bolt D. Caught in the chasm: literary representation and suicide among people with impaired vision. Br J Vis Impair. 2005;23(3):117–121.
- Jernigan K. Blindness: is literature against us? Chicago (IL): National Federation of the Blind; 1974.
- Rudgard O. Calling people 'blind' is shocking and misleading says charity as it looks to change name. The Telegraph; 2018. Available from: https://www.telegraph.co.uk/news/2018/04/25/calling-blind-people-blind-off-putting-misleading-charity-says/
- Greenland C. Vision Canada: the unmet needs of blind Canadians. Toronto: Canadian National Institute for the Blind; 1976.
- Martiniello N, Eisenbarth W, Lehane C, et al. Exploring the use of smartphones and tablets among people with visual impairments: are mainstream devices replacing the use of traditional visual aids? Assist Technol. 2019. DOI:https://doi.org/10.1080/10400435.2019.1682084
- Hersh M. Cane use and late onset visual impairment. TAD. 2015;27(3):103–116.
- Hogan CL. Stigma, embarrassment and the use of mobility aids. Int J Orientation Mobility. 2012;5(1):49–52.
- Knowles MS. Andragogy: adult learning theory in perspective. Community Coll Rev. 1978;5(3):9–20.
- Tough A. Choosing to Learn. In: Healy GM, Ziegler WL, editors. The learning stance: essays in celebration of human learning. Toronto: Ontario Institute for Studies in Education; 1979.
- Zhang C, Zheng G. Supporting adult learning: enablers, barriers, and services. Proceedings of the 14th annual ACM SIGITE conference on Information technology education (SIGITE '13); 2013 Oct; Orlando, Florida, USA. New York (NY, USA): Association for Computing Machinery; 2013. p. 151–152.
- Meyer A, Rose DH, Gordon D. Universal design for learning: theory and Practice. Wakefield, MA: CAST Professional Publishing; 2014.
- Baumgartner LM. An update on transformational learning. New Dir Adult Cont Educ. 2001;2001(89):15–24.
- Michael J. Where's the evidence that active learning works? Adv Physiol Educ. 2006;30(4):159–167.
- Leat SJ. A proposed model for integrated low-vision rehabilitation services in Canada. Optom Vis Sci. 2016;93(1):77–84.
- Convention on the Rights of Persons with Disabilities (CRPD). United Nations Division for Social Policy and Development - Disability; 2016. https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities.html
- Creswell JW. Qualitative inquiry and research design: choosing among five approaches. London: Sage Publications; 2007.
- Corn AL, Lusk KE. Perspectives on low vision (Chapter 1). In: Foundations of low vision: clinical and functional perspectives. New York (NY): American Foundation for the Blind; 2010. p. 3–34.
- Goodman LA. Snowball sampling. Ann Math Statist. 1961;32(1):148–170.
- Smith JA. Semi-structured interviewing and qualitative analysis. In: Smith JA, Harré R, van Langenhove L, editors. Rethinking methods in psychology. London: Sage; 1995.
- Horrigan-Kelly M, Millar M, Dowling M. Understanding the key tenets of Heidegger’s philosophy for interpretive phenomenological research. Int J Qual Methods. 2016;15(1):160940691668063.
- Ninot G, Moullec G, Desplan J, et al. Daily functioning of dyspnea, self-esteem and physical self in patients with moderate COPD before, during and after a first inpatient rehabilitation program. Disabil Rehabil. 2007;29(22):1671–1678.
- Fuhrer MJ. Assistive technology outcomes research: challenges met and yet unmet. Am J Phys Med Rehabil. 2001;80(7):528–535.
- Phillips M, Proulx MJ. Social interaction without vision: an assessment of assistive technology for the visually impaired. Technol Innov. 2018;20(1):85–93.
- Sugawara AT, Ramos VD, Alfieri FM, et al. Abandonment of assistive products: assessing abandonment levels and factors that impact on it. Disabil Rehabil Assist Technol. 2018;13(7):716–723.
- International Classification of Functioning, Disability and Health (ICF). World Health Organization; 2001. https://www.who.int/classifications/icf/en/
- World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194.
- Saleh GM, Patel JI, Sivaprasad S, et al. Digital Voice Signature: the future of consent? Clin Exp Ophthalmol. 2007;35(3):297.
- Knobf M, Juarez G, Lee S-YK, et al., editors. Challenges and strategies in recruitment of ethnically diverse populations for cancer nursing research. Oncol Nurs Forum. 2007;34(6):1187–1194.
- Becker H, Roberts G, Morrison J, et al. Recruiting people with disabilities as research participants: challenges and strategies to address them. Intellect Dev Disabil. 2004;42(6):471–475.
- Matua GA, Van Der Wal DM. Differentiating between descriptive and interpretive phenomenological research approaches. Nurse Res. 2015;22(6):22–27.
- Hennink MM, Kaiser BN, Marconi VC. Code saturation versus meaning saturation: how many interviews are enough? Qual Health Res. 2017;27(4):591–608.
- Ferguson PM, Nusbaum E. Disability studies: what is it and what difference does it make? Res Pract Persons Severe Disabil. 2012;37(2):70–80.
- Mankoff J, Hayes GR, Kasnitz D. Disability studies as a source of critical inquiry for the field of assistive technology. Proceedings of the 12th international ACM SIGACCESS conference on Computers and accessibility; Orlando, Florida, USA: Association for Computing Machinery; 2010. p. 3–10.
- Reynolds F, Prior S. 'A lifestyle coat-hanger': a phenomenological study of the meanings of artwork for women coping with chronic illness and disability. Disabil Rehabil. 2003;25(14):785–794.
- Braun V, Clarke V. Thematic analysis. APA handbook of research methods in psychology., Vol 2: Research designs: Quantitative, qualitative, neuropsychological, and biological. APA handbooks in psychology®. Washington (DC): American Psychological Association; 2012. p. 57–71.
- InqScribe. 2.2.4. Inquirium; 2018. https://www.inqscribe.com/
- Finlay L. Unfolding the phenomenological research process:iterative stages of “seeing afresh. J Humanist Psychol. 2013;53(2):172–201.
- Smith JA, Flowers P, Larkin M. Interpretative phenomenological analysis: theory, method and research. London: Sage Publishing; 2009.
- Asselin ME. Insider research: issues to consider when doing qualitative research in your own setting. J Nurses Staff Dev. 2003;19(2):99–103.
- Mingus M. Leaving Evidence [Internet]; 2011 [cited 2020]. Available from: https://leavingevidence.wordpress.com/2011/05/05/access-intimacy-the-missing-link/
- Levack WMM, Boland P, Taylor WJ, et al. Establishing a person-centred framework of self-identity after traumatic brain injury: a grounded theory study to inform measure development. BMJ Open. 2014;4(5):e004630.
- Gorges J, Kandler C. Adults' learning motivation: expectancy of success, value, and the role of affective memories. Learn Individ Differ. 2012;22(5):610–617.
- Rivers WP. Autonomy at all costs: an ethnography of metacognitive self‐assessment and self‐management among experienced language learners. Mod Lang J. 2001;85(2):279–290.
- Gitlin LN. Why older people accept or reject assistive technology. Generations. 1995;19:41–46.
- Rogers S. Learning braille and print together — the mainstream issues. Br J Vis Impair. 2007;25(2):120–132.
- Bogart KR, Logan SW, Hospodar C, et al. Disability models and attitudes among college students with and without disabilities. Stigma Health. 2019;4(3):260–263.
- Farrow KR. Using a group approach to motivate adults to learn braille. J Vis Impair Blind. 2015;109(4):318–321.
- Grue J. The problem with inspiration porn: a tentative definition and a provisional critique. Disabil Soc. 2016;31(6):838–849.
- Fraser S, Beeman I, Southall K, et al. Stereotyping as a barrier to the social participation of older adults with low vision: a qualitative focus group study. BMJ Open. 2019;9(9):e029940.
- Hammer G. If they‘re going to stare, at least i‘ll give them a good reason to”: blind women’s visibility, invisibility, and encounters with the gaze. Signs. 2016;41(2):409–432.
- Gordon P, Kerzner L, Sheldon T, et al. Assistive devices in Canada: ensuring inclusion and independence. Toronto: ARCH Disability Law Centre; 2007.
- Burmedi D, Becker S, Heyl V, et al. Emotional and social consequences of age-related low vision. Vis Impair Res. 2002;4(1):47–71.
- Walker AS, Sangelkar S, editors. Design exploration of affordable refreshable braille display technology for low-income visually impaired users. Proceedings of the ASME 2017 International Design Engineering Technical Conferences and Computers and Information in Engineering Conference; 2017: American Society of Mechanical Engineers Digital Collection.
- São José JMS, Amado CAF, Ilinca S, et al. Ageism in health care: a systematic review of operational definitions and inductive conceptualizations. Gerontologist. 2019;59(2):e98–e108.
- Wittenstein SH, Pardee ML. Teachers' voices: comments on braille and literacy from the field. J Vis Impair Blind. 1996;90(3):201–209.
- Rush KL, Chiasson M, Butterfield M, et al. Recognition: key to the entrepreneurial strategies of rural coalitions in advancing access to health care. Int J Equity Health. 2019;18(1):119.