
Abstract
Purpose
As the prevalence of age-related visual impairment increases, a greater understanding of the physiological and cognitive capacities that are recruited during braille reading and the potential implications of age-related declines is required.
Methods
This scoping review aimed to identify and describe primary studies exploring the relationship between tactile, motor and cognitive capacities and braille reading performance, the instruments used to measure these capacities, and the extent to which age is considered within these investigations. English peer-reviewed articles exploring the relationship between these capacities and braille reading performance were included. Articles were screened by two researchers, and 91% agreement was achieved (kappa = 0.84 [0.81, 0.87], p < 0.01).
Results
2405 articles were considered of which 36 met the inclusion criteria. Fifteen investigated the relationship between tactile capacities and braille reading performance, 25 explored motor capacities, and 5 considered cognitive capacities. Nineteen instruments were used to measure tactile capacity, 4 for motor dexterity, and 7 for cognitive capacity. These studies focus on younger participants and on those who learned braille early in life.
Conclusions
Although this overview underscores the importance of tactile perception and bimanual reading, future research is needed to explore the unique needs of older adults who learn braille later in life.
The studies in this review underscore the importance of developing both haptic tactile perception and efficient hand reading patterns early in the braille learning process.
Practitioners should consider whether specific pre-braille readiness activities can be used to address the unique needs of older adults who may experience tactile, motor or cognitive declines.
Most of the studies in this review require replication before they should serve as reliable clinical guidelines; however, braille reading (like print) is a complex process that draws on multiple capacities that should be developed in unison.
The studies in this review focus heavily on younger participants and on those who learned braille early in life, and highlight the need for future research on braille and aging.
IMPLICATIONS FOR REHABILITATION
Introduction
Tactile sensitivity, manual dexterity and cognitive capacities are vital components of efficient braille reading [Citation1,Citation2]. Many of these physiological and cognitive capacities are known to decline as part of the typical aging process [Citation3]. While there is a broad scope of literature centered on braille literacy and childhood [Citation2,Citation4–6], there is insufficient evidence on the extent to which age-related declines in these capacities will effect braille reading outcomes. In recent decades, a variety of instruments have been developed to measure tactile, motor and cognitive capacities in blind individuals and to explore the relationship between these measures and braille reading outcomes (for example, see [Citation7–10]). However, these studies are sparce and have given rise to inconsistent findings depending on the instruments that are used, even when those instruments purportedly measure the same underlying capacity. For example, both Bola [Citation11] and Veispak [Citation12,Citation13] explored the association between passive tactile acuity (using the Grating Orientation Test [Citation14]) and braille reading speed, though Veispak observed a relationship while Bola did not. Thus far, there is no research which describes and summarizes these findings within a single comprehensive review. As the prevalence of age-related visual impairment continues to increase [Citation15,Citation16], there are growing calls for research on braille and aging and for the development of evidence-based practices that best support the needs of older adults who pursue braille [Citation17]. It is possible that older adults with impaired tactile, motor or cognitive capacities may benefit from specific pre-braille readiness activities designed to target their unique needs [Citation17]. Similarly, research is needed to ensure that clinical decisions are not based upon conjecture and overarching generalizations about aging, such as the prevailing belief among some prospective clients and rehabilitation practitioners that older adults are unable to pursue braille due to reduced tactile sensitivity [Citation17,Citation18]. The objectives of this review are to provide an overview of primary studies that explore the relationship between tactile, motor and cognitive capacities and braille reading performance in order to consolidate available research as a precursor to future studies that will build upon this evidence.
The ability to read is necessary for the completion of common daily tasks, from identifying household products to reading prescriptions, documents and instructions, and is closely tied to feelings of self-competence and independence for individuals who acquire a visual impairment [Citation19,Citation20]. In fact, reading-related difficulties are among the most common reasons for referral to low vision rehabilitation services [Citation21,Citation22]. Braille, a tactile system of reading and writing, provides a non-visual alternative to print for those with significant or fluctuating visual impairments or for those who have a degenerative visual condition [Citation19]. As a literacy medium, it provides access to spelling, punctuation and other grammatical nuances that are often difficult to access through auditory-based methods alone [Citation23]. Moreover, for the growing population of individuals with acquired dual sensory impairment (concurrent vision and hearing loss), braille may be the only vehicle through which communication becomes possible [Citation24].
The reading of braille draws on the somatosensory cortex responsible for processing tactile perception, the motor cortex for fine movements of the fingers and hands, and much like visual reading, the cognitive functions of memory, sustained attention, information processing and comprehension [Citation25]. Tactile information is perceived by a variety of peripheral touch receptors that transmit information from the distal pads of the fingertips to the central nervous system. The combined information when a reader lightly slides their fingers across a page of braille leads to the ability to discriminate braille characters [Citation3]. Unlike print reading, braille reading can only occur haptically, through the smooth and constant movements of the reading hands, and disruption to movement will necessarily impede perception [Citation1,Citation26]. Impairments in one or both hands or instability stemming from degenerative disease may consequently impede tactual perception and reading speed [Citation27]. Braille reading differs from print in that characters are read sequentially as the fingers move across a line rather than being perceived simultaneously during a single saccadic gaze. New or less proficient braille readers must retain each successive symbol in working memory to build a representation of the word in question [Citation23,Citation28–31], initially placing a greater emphasis on working-memory [Citation17,Citation32]. Conversely, more profficient or experienced braille readers with greater reading fluency are able to draw on lexical, perceptual and contextual cues to facilitate faster reading and comprehension [Citation33–35].
Normal aging is associated with steady declines in tactile acuity, fine motor dexterity, and cognitive functions, including working-memory and sustained attention [Citation3]. Tactile acuity of the fingertips has been shown to decrease with age [Citation7,Citation36], particularly among the sighted who lack a lifetime of tactile experience [Citation37], and this can be further impaired by neuropathic comorbidities such as diabetes [Citation25]. Declines in fine and gross motor dexterity are also observable with advancing age. In particular, fine-motor dexterity appears to be most affected by the aging process, gradually impacting the use of fingers and hands during tasks that require pinching, grasping or the manipulation of objects, finger strength, or the coordinated use of the fingers and hands [Citation38]. Similarly, gray and white matter deterioration is observable after the fifth decade of life [Citation39,Citation40]. Among sighted print readers, a correlation exists between degree of hippocampal shrinkage, performance on memory-based tasks (such as word retention) and overall memory decline [Citation40]. Though the relationship between working-memory and braille reading performance has not been directly explored, it has been shown that age-related declines in short-term working memory are significantly correlated with reading comprehension difficulties among the sighted [Citation41].
Although increased age is generally correlated with declines in tactile, motor and cognitive capacities, these characteristics have been measured using a wide range of instruments [Citation42,Citation43]. Moreover, tactile perception, motor dexterity and cognitive functioning are broad descriptors of capacities that may refer to different underlying components that are not directly comparable [Citation44]. These considerations may therefore give rise to inconsistencies among results, depending on the specific capacity that is being assessed and the measurement instrument that is used. For example, tactile sensation can be passively perceived (without any movement between the stimulus and the skin) or actively perceived (where there is movement or friction between the stimulus and the skin), each of which activate different receptors [Citation43,Citation44]. The passive 2-point discrimination test, originally pioneered by E.H. Weber in the mid-nineteenth century [Citation45], is routinely employed within medical and research domains but has been called into question due to its purportedly poor test-retest reliability. Alternative measurements of passive tactile acuity (such as the Grading Orientation Test) which emphasize the ability to discern groove orientation rather than the ability to perceive two individual points have therefore also been devised [Citation43]. Quite apart from the specific instrument used to measure different facets of tactile acuity, the question of whether methods used to measure passive and active touch acuity are interchangeable remains the subject of debate [Citation25,Citation43,Citation46]. Reliance on the findings of a single study or the use of a specific instrument may therefore lead to uninformed clinical decisions, such as wrongly assuming that performance on a specific measure will predict braille reading capacity.
While congenital visual impairments were historically prevalent [Citation4,Citation47], there has been a steady increase of working-age and older adults with acquired visual impairment over recent decades. It is projected that the prevalence of age-related visual impairment will double in Canada and triple worldwide over the next two decades, due to both population growth and aging [Citation15]. This raises critical new questions for rehabilitation practitioners, including the need to understand how older populations and those who learn braille later in life differ from children in underlying mechanisms that influence their braille training outcomes, and whether specific remedial activities or supports would enhance their braille reading performance. For example, a report on braille and aging compiled by Cryer [Citation17] synthesized several existing methods used to test and train tactile ability among adult braille clients. Though vital in that it answered some initial questions, this report did not include a systematic overview of all existing primary literature and did not consider the contribution of motor and cognitive capacities within the braille reading context. Recognizing this, the authors concluded by explicitly emphasizing the need to explore these themes in greater depth as a first step towards developing methods to better support older adults who learn braille [Citation17].
The aims of this review are to (1) identify and describe existing literature on the relationship between tactile, motor and cognitive capacities and braille reading performance; (2) summarize the range of instruments that have been used to measure these capacities, and (3) describe the extent to which the relationship between age and braille reading performance is considered within these investigations. This overview will clarify the current state of knowledge on braille and aging within a field that has traditionally focused almost exclusively on braille learning in childhood [Citation5,Citation48], and will set future research agendas on braille and aging by highlighting where current knowledge gaps exist.
Methods
A scoping review [Citation49] that summarizes all relevant primary studies was deemed to be optimal, rather than alternative review methodologies that exclude articles on the basis of sample or effect size. Following the scoping review methodology outlined by Arskey and O’Malley [Citation49] and Levac, Colquhoun and O’Brien [Citation50], this study consisted of five separate stages, each of which is described below. This review also complies with the methodological recommendations outlined within the Joanna Briggs Institute manual for conducting systematic scoping reviews [Citation51].
Stage 1: identifying the research questions
This scoping review is based on the following research questions:
What is known about the relationship between tactile, motor and cognitive capacities and braille reading performance?
What are the instruments that have been used to measure these capacities?
To what extent is the relationship between age and braille reading performance considered within these investigations?
The search strategy for this study was guided by the following parameters:
Population
This review focuses on the study of participants who read braille tactually with their fingers. Studies with braille readers who are described as blind, low vision or visually impaired are included, even if specific acuities and fields are not reported. Braille readers of any age and any braille level are included, as long as the study in question explores the relationship with at least one of the identified capacities (tactile, motor or cognitive) and at least one of the braille reading measures (reading speed, accuracy or comprehension).
Concept
Tactile capacity: may includes studies of passive acuity, where a stimulus is applied to the fingertip without any movement between the finger and the stimulus, or active (haptic) acuity, where such movement is permitted or required (as with the reading of braille) [Citation42].
Motor capacity: may include measures of fine or gross motor dexterity [Citation52], as well as studies that examine the use of fingers and hands and the relationship of these patterns to braille reading outcomes [Citation53].
Cognitive capacity: refers to domain-specific cognitive mechanisms that are known to decline with age, such as working-memory, sustained attention and information processing [Citation54]. Notably, this does not include level of education, phonological awareness, orthography or other literacy-based competencies. We recognize the importance of prior education and literacy experiences, but narrowed the focus of the present investigation to the physiological and cognitive capacities that are known to decline with age.
Braille reading performance is divided into the following subcomponents, in line with measures usually considered when assessing braille reading skills [Citation2]: speed (characters or words per minute), accuracy (number of misread characters or words) and comprehension (understanding of the text, typically assessed through the use of comprehension questions or methods such as the closed procedure) [Citation2]. Studies which examine at least one of these reading outcomes in relation to tactile, motor or cognitive capacities were included. Both oral and silent reading measures were deemed eligible as is the reading of uncontracted (alphabetic) or contracted (abbreviated) braille.
Age: To address the final research question on the extent to which the relationship between age and braille reading performance is explored within the eligible studies, three age-related variables are considered: chronological age, age of onset, and age when braille was learned.
Context
No limitations were placed on geographic location or date of publication. Only peer-reviewed articles published in English were considered.
Stage 2: identifying relevant articles
A comprehensive search of four peer-reviewed academic databases (PsycInfo, ERIC, Cochrane and PubMed) was conducted in August 2019 and updated in July 2020, in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist: see Supplementary Material (PRISMA-ScR Checklist) for details. Given the limited size of the research base relating to braille, the decision was made to simply search for the word “braille” and to rely on the inclusion criteria to narrow the analysis (see for inclusion/exclusion criteria). Second, a manual search in the JVIB online database was conducted in July 2020, due to the relevance of this publication to the field of braille and blindness. Given the focus on braille and blindness within JVIB, specific key words were used to narrow the search: (keyword: “braille AND (speed OR accuracy OR comprehension).” Finally, the reference lists of all included articles were reviewed to ensure that no relevant articles were omitted. All relevant citations and abstracts were downloaded and imported into a Microsoft Excel worksheet. Duplicates were flagged (based on their title and author list) with a custom macro and then manually reviewed prior to being removed.
Table 1. Inclusion and exclusion criteria.
Stage 3: article selection
Articles were screened by two reviewers (the first author and an additional research assistant). Screening consisted of a two-stage process, beginning with the screening of titles and abstracts and finally with the review of the full texts of those articles which had not been excluded at the first stage. Inclusion/exclusion decisions were marked in separate files by each reviewer and then compared and discussed.
shows the flow of article selection and number of excluded articles at each stage of the process (including results from both the initial search and the July 2020 update).
Figure 1. PRISMA-ScR diagram showing flow of included studies.
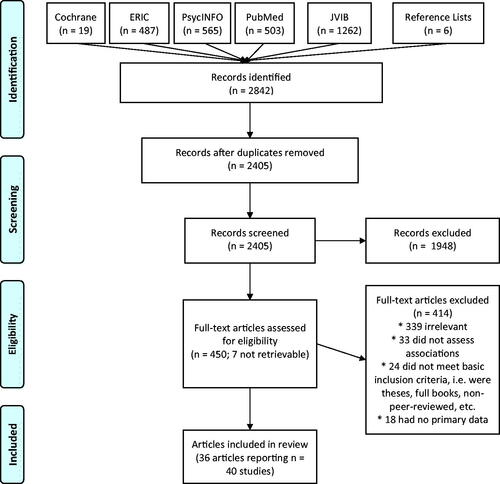
The search identified 2405 articles after duplicates were removed (including 6 additional articles identified through manual review of the reference lists of included articles). Some articles reported on multiple studies and, where that occurred, this will be indicated.
Titles and abstracts of an initial 250 articles were reviewed by the two reviewers, with 83% agreement as to inclusion (Cohen’s kappa = 0.76 [0.71, 0.81], p < 0.01). Differences were resolved between the reviewers through discussion, and after screening all 2405 titles and abstracts, 91% agreement was achieved (kappa = 0.84 [0.81, 0.87], p < 0.01). Where doubt remained about inclusion, articles were kept.
Screening of the titles and abstracts left 457 which met the criteria for a full-text review. The full text of 450 of these papers was then acquired (7 could not be obtained) and assessed against the inclusion criteria by the two reviewers, with 83.1% agreement achieved (kappa = 0.57 [0.46, 0.68], p < 0.01). It became evident that the most common disagreement related to articles that reported on relevant tactile, motor or cognitive capacities, but did not actually consider any of those characteristics in the analysis. With those articles removed, 93.2% agreement was achieved (kappa = 0.81, [0.76, 0.86], p < 0.01), and the remaining disagreements were resolved through discussion between the two reviewers, resulting in 36 articles selected for inclusion. All analyses for interrater reliability were conducted using the irr [Citation55] and psych [Citation56] packages from the computer program R (The R Foundation for Statistical Computing, Vienna, Austria, version 3.4.4).
Stage 4: charting the data
The 36 articles that met the inclusion criteria [Citation8–12,Citation27,Citation57–86] were then subject to data extraction following the guidelines outlined by Peters et al. [Citation51]. The extracted data for each study are summarized in Appendix.
Stage 5: collating, summarizing, and reporting the results
Descriptive numerical analysis: Numerical analysis (percentage, range, central tendency, variation) was computed to describe the nature and distribution of all included studies.
Qualitative thematic analysis: Following the procedure for qualitative thematic analysis outlined by Braun et al [Citation87], the 36 included studies were coded by the two reviewers into one of three categories according to whether they examined tactile, motor or cognitive capacities in relation to braille reading performance. The studies were further categorized into subthemes to describe the underlying tactile, motor and cognitive capacities investigated in the studies. Each reviewer coded the articles separately and this was then compared through discussion, where no disagreements were observed.
Results
The 36 articles (representing 40 unique studies) that met the inclusion criteria were published between the years of 1934 and 2019. depicts the number of articles published in each decade. It can be seen that between 1954 and 1994, the number of publications steadily increased, resulting in more than half (58%) of the included studies published during this time frame. Of interest, n = 9 articles were published between 1984 and 1994, making this the most prolific decade. As shown in , the top three represented journals were the Journal of Visual Impairment & Blindness (n = 9), Research in Developmental Disabilities (n = 4), and Neuropsychologia (n = 3). summarizes the characteristics of the 36 articles (40 studies), and the detailed data extracted is provided in Appendix.
Figure 2. Histogram depicting the number of published articles appearing in each decade since 1934.
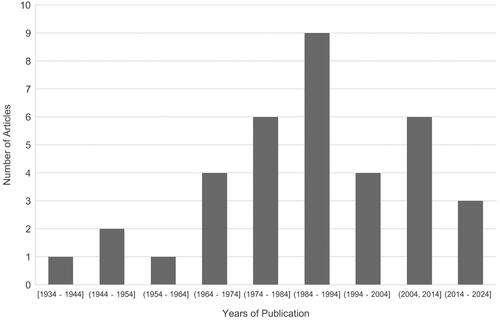
Figure 3. Graph depicting the number of articles published by journal of publication.
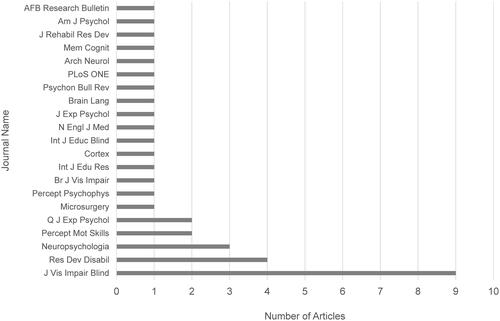
Table 2. Summary of characteristics of included studies.
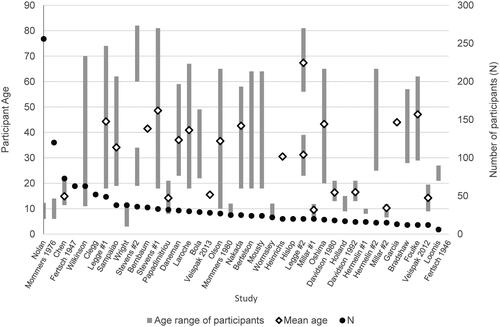
As will be discussed, two notable characteristics of the included studies were their sample size and the range of included participant ages (depicted in ). The sample size for the 40 studies ranges between 6 and 73 participants (with two outliers having n = 120 and n = 256 respectively, both focused on young children). The mean sample size among the 40 studies is 37.1 (SD = 46.8) (removing the two outliers: mean = 26.4, SD = 14.1) and only four have n > = 50. Collectively the studies included participants between the age of 3 and 82 (mean = 30.1, SD = 14.2); however, the average lower and upper bounds of the age groups represented (where this information was available) were 14.3 and 40.1 respectively. Among the 32 studies that reported sufficient information to determine the age range of participants, 32.5% (n = 13) studies included participants over the age of 60, and 25% (n = 10) included only participants below the age of 21. Importantly, 20% (n = 8) did not provide enough information to determine the age range of participants, and a full 47.5% (n = 19) did not report the mean or median age of participants.
Figure 4. Graph summarizing the age range of participants (depicted by a bar plotted against the left-hand side axis) and sample size (depicted by a dot against the right-hand side axis) in each of the included studies. Diamonds indicate the mean age of participants within the sample.
Relationship between capacities, braille reading and instruments used
Tactile capacities
Among the 40 studies (36 articles), 15 studies (13 articles) explored the relationship between tactile capacity measures and braille reading performance (). Of these, 8 studies (7 articles) examined passive (or static) acuity and 7 studies (6 articles) explored active (or haptic) acuity. In total, 19 different instruments were used to measure tactile capacity (11 for passive and 8 for active). Only 6 of the instruments were used in more than one study (Grating Orientation Test, Static Two-point Discrimination Test, Two-point Gap Discrimination Test, Nylon Filament Test, Roughness Discrimination Test, and Legge Dot Chart). Overall, 12 studies (10 articles) explored the relationship between tactile capacity and reading speed, 4 studies (4 articles) for reading accuracy, and 3 of the studies (3 articles) explored the relationship between tactile capacity and a more general can read/cannot read measure. None of the articles explored the relationship between tactile capacity and reading comprehension.
Table 3. Tactile capacities and relationship to braille reading performance.
Motor capacities
Twenty-five of the studies (23 articles) examined motor capacities in relation to braille reading performance, with 22 studies (20 articles) investigating reading speed, 9 studies (8 articles) examining accuracy, and 5 studies (5 articles) exploring reading comprehension (see ). The measurement of motor capacities in these studies relied upon the observation of fingers and hand usage during braille reading. Among the 25 studies, 2 examine the relationship between contact force (the amount of pressure applied by the reading fingers) and braille reading performance; 5 focused on the use of specific fingers during braille reading; 9 focused on hand usage (left vs. right hand); and 13 focused on the use of specific hand reading patterns (whether the hands move together across the line or whether they employ the more advanced scissors technique, where one hand reads the remainder of the current line while the other begins reading the next line).
Table 4. Motor capacities and relationship to braille reading performance.
Cognitive capacities
In total, 5 of the studies (reported in 5 articles) explored the correlation between cognitive capacities and braille reading performance, with 5 investigating speed, 3 investigating accuracy, and 1 exploring comprehension (see Table 5). Overall, 7 instruments were used, which fall into one of three broad categories: intelligence or IQ tests; tests of processing speed (the speed at which a participant is able to process information being perceived); and tests relating to short-term working memory (the ability to retain and recall information that is just perceived).
Table 5. Cognitive capacities and relationship to braille reading performance.
The relationship between age and reading performance
provides an overview of the extent to which age-related variables were considered across the 40 studies. The 11 studies (in 10 articles) which directly explored the relationship between age-related variables (chronological age, age of onset or braille learning age) and braille reading performance included between 13 and 73 participants (mean 31.9, SD 16.8) ranging in age from 11 to 74 (mean 36.9, SD 9.5).
Table 6. Relationship between various measures of age and measures of braille reading performance (speed, accuracy, comprehension).
Overall, 5 of the studies (in 5 articles) explored the relationship between chronological age and braille reading performance, with 4 examining reading speed; 0 exploring reading accuracy; 2 for reading comprehension, and 1 exploring general braille reading capacity.
In total, 5 of the studies (in 5 articles) explored the relationship between age of onset and braille reading performance. All 5 explored the relationship between age of onset and reading speed; 1 also explored reading accuracy; and 2 also explored reading comprehension. It is impossible to provide a lower and upper age of onset range for these studies collectively, as sufficient information is not provided and different definitions of “age of onset” are used across these studies. While some articles provided continuous age of onset values, others simply categorized participants into dichotomous groups (e.g., congenital vs. adventitious). The specific definitions used for age of onset for these studies are indicated in the legend found at the end of .
In total, 3 of the studies explored the relationship between the age at which braille was learned and braille reading performance. Of these, 2 examined braille learning age and reading speed; 1 examined reading accuracy; 2 explored the relationship with reading comprehension, and 1 explored the relationship between braille learning age and general “braille reading capacity.” Note that the definition of braille learning age varied across these 3 studies. Garcia [Citation67] did not specifically identify the age at which participants learned braille (except to note that participants had between 1 and 55 years reading experience); Laroche [Citation72] divided participants into two groups (learned before age 10 and learned after age 10); and in Nakada [Citation78], participants had completed two years of braille rehabilitation training yielding braille learning ages of between 18 and 58 (mean 42.6, SD 10.2).
Discussion
The aim of this scoping review was to summarize the breadth and nature of research exploring the relationship between tactile, motor and cognitive capacities and braille reading performance, the instruments used to measure these capacities, and the extent to which age has been considered within these investigations. Spanning 4 databases and 85 years of published literature, this review is noteworthy not merely for the insights it affords, but also for heightening the discrepancies that remain. Though no restrictions were placed on year of publication, only 36 articles (representing 40 studies) published between 1934 and 2019 were deemed eligible. Of note, although braille reading draws on multiple capacities [Citation1], none of the included studies explore the relationship between tactile, motor and cognitive capacities and braille reading measures within a single sample. This may lead to an over-simplification of the braille reading process, and the misinterpretation of findings which obscure the potential influence of other confounding age-related variables. Similarly, though a wide range of instruments has been used to measure these capacities, most of these tools have only been employed within a single study, highlighting the need for replication. As the prevalence of age-related visual impairment continues to increase, there is an evident need for research focusing on older adults and on those who learn braille beyond childhood.
Relationship between capacities and braille reading and the range of instruments used
Tactile capacities
It can be seen that among the 15 studies (13 articles) in , there is a clear focus on whether passive acuity measures could be used to predict current or future braille reading capacity. This trend persists across the decades, with the earliest passive tactile acuity study published in 1969 and the most recent in 2016.
The interest in passive acuity originates from the medical domain where such tools are routinely employed to assess neurological damage, including diabetic neuropathy of the fingertips [Citation43]. From a clinical perspective, several authors have also highlighted that passive acuity instruments are often portable and simple to administer [Citation17]. In the static two-point discrimination test, for example, the points of the calipers are applied to the pad of the stationary finger at different distances from each other, in order to determine the minimal distance at which the participant is able to distinguish the presence of one or two points [Citation10]. Given that the center-to-center distance between dots in the standard braille cell is approximately 2.28 mm [Citation9], it is unsurprising that researchers would contemplate whether 2-point threshold measures could be used to predict braille reading ability or whether individuals with a 2-point threshold above 2.28 mm would find it difficult to read standard braille [Citation27,Citation68,Citation78].
Despite these considerations, the studies in this review differ drastically in the extent to which a relationship between passive acuity and braille reading performance is reported. Among the two most commonly used passive acuity tests within this review (two-point and Grating Orientation), two-point is only related to braille reading performance in 1 of 3 studies, and Grating Orientation in 2 of the 3 studies. These inconsistent findings partially stem from the fact that although the Grating Orientation Test has been found to be a reliable measure of passive tactile perception [Citation42], the two-point discrimination test depends heavily on the examiner’s ability to maintain consistent force with both points across all trials, and is associated with poor test-retest reliability [Citation42,Citation89]. Importantly, it is also difficult to draw specific comparisons across these passive acuity studies, as sufficient demographic information (such as previous braille experience) is not always available, and 3 of the passive acuity studies simply evaluate braille reading performance using a subjective, qualitative scale (cannot read/can read with difficulty/can read well) without specific information about reading rate, accuracy or comprehension [Citation27,Citation68,Citation78].
Several authors have also highlighted that passive acuity measures reveal little about activities that draw on active tactile perception [Citation17], leading to an interest in active acuity measures. Indeed, the focus on passive acuity seems counterintuitive given that braille reading is impaired when the fingers remain static or when ineffective movements (such as vertical scrubbing) are employed [Citation2,Citation53,Citation90]. Braille reading activates the nerve endings of sensory receptors, but also the muscles, joints and tendons of the fingers, hands, wrists, arms and shoulders [Citation2,Citation44,Citation53]. Moreover, active tactile perception provides greater control to the participant over the stimulus being perceived and enables the use of strategies to move across symbols more effectively [Citation9,Citation17].
While there is no doubt that proficient braille reading requires the ability to actively perceive tactile symbols, there are 8 different active acuity instruments used across the studies in this review and only two (Roughness Discrimination Test and Legge Dot Chart) are used in more than one study. Of interest, the Legge Dot Chart is a tactile analogue to the Snellen chart used to measure the threshold of visual perception among the sighted, but is not related to braille reading speed in either of the two studies where it is used [Citation9,Citation80]. This tactile chart consists of nine lines of four randomly presented braille-like symbols (corresponding to the letters d, f, h, and j) where the distance between the dots in each symbol decreases logarithmically from one line to the next. Though it can be seen that blind subjects outperformed sighted age-matched subjects in Legge’s study [Citation9], no relationship between active acuity threshold and braille reading speed (using a braille version of the MN Read) is reported. Of relevance is that the blind participants in this study were all experienced braille readers with early blindness and with active acuity thresholds well below the 2.28 mm distance required for braille reading [Citation9]. As with visual reading, it may be that further increases in acuity do not accord any additional advantage to reading speed when the acuity is already below the threshold required for successful reading [Citation9]. It is possible that a more significant relationship between speed and acuity measures might be observed among late blind participants and among those whose tactile acuities are closer to the 2.28 mm braille threshold.
Motor capacities
A majority of the studies in this review are devoted to the motor capacities recruited during braille reading, with 25 studies (22 articles) falling within this domain (see ). Of interest, this research focuses heavily on observations of finger and hand usage during braille reading, rather than on underlying measures of fine or gross motor capacities that may decline with age.
Several of the earliest studies examined whether the use of specific fingers correlate with better braille reading outcomes, and confirm the superiority of the index fingers for tactile perception [Citation43]. Foulke [Citation66] tested braille reading speed on 8 separate fingers for each participant (all but the two thumbs) and found that performance was best on the index fingers of both hands. This is unsurprising given that the index fingers contain the greatest density of sensory receptors (much like the fovea of the eye) and the number of these receptors gradually declines with each digit [Citation44]. While the superiority of the index fingers for tactile perception is undisputed, it is now also recognized that multiple fingers are often recruited during the braille reading process [Citation2]. Even if the index fingers are the most dominant, students are often encouraged to perceive the braille reading line with multiple fingers as this can facilitate reading by confirming what is being processed [Citation2,Citation76]. From an aging perspective, it is possible that readers with damage or disease in the index fingers may develop a preference for relying more heavily on alternative fingers during braille reading and especially benefit from the use of multiple fingers where tactile perception is impaired, contributing to cortical magnification in the preferred reading fingers [Citation27,Citation44]. As such, studies that test braille reading without taking into account preferred reading fingers and habits may not provide a realistic measure of reading performance in such cases.
Much of the motor literature focuses heavily on hand dominance and hand reading patterns, and the question of whether the left or right hand is best for braille reading. Several studies from the 1970s and 1980s are premised on evidence suggesting that sighted participants who are unfamiliar with braille recruit the right hemisphere during braille reading (believed to be responsible for spatial processing) and will therefore perform best when using the left hand. Alternatively, it was believed that experienced braille readers show a right hand dominance because they recognize braille symbols for their linguistic properties and in turn reveal a left hemispheric superiority [Citation58,Citation69,Citation82]. Despite the appeal of arguments based on cortical asymmetry, these studies result in inconsistent findings and confirmed that there is no universally best hand for braille reading. Instead, multiple parts of the cortex (including the occipital cortex) are recruited during the braille reading process, and two-handed reading is associated with faster reading rates [Citation53].
A total of 13 studies in this review explore the influence of specific hand reading patterns. These patterns are typically categorized as one-handed reading, where either the left or right hand is used alone; two-handed reading where both hands move together with the index fingers spaced slightly apart from each other; and disjointed reading whereby the two hands read together until the midpoint, after which the right hand reads the remainder of the line while the left hand moves diagonally to locate the start of the following line [Citation1]. The latter pattern is virtually always associated with the fastest reading rates, owing in part to the time saved in transitioning from one line to the next [Citation57]. There is considerable evidence that when two hands are used collaboratively, each hand is independently contributing to the reading process. Mommers, for example, observed that when both hands are used, the left hand is used to confirm what has just been read with the right, and in some cases even regresses to re-read passages for confirmation while the right hand continues reading ahead [Citation76]. It has likewise been observed that where large disparities exist between the performance of the left and right hand individually for a particular subject, this disparity limits the potential two-handed reading performance [Citation77].
While two-handed reading is associated with faster reading rates, Wormsley [Citation53] underscores that even where readers use advanced two-handed reading techniques, reading rates do not necessarily improve where tactile recognition skills are deficient [Citation53]. Indeed, poor tactile perception may adversely affect hand reading strategies [Citation71]. These considerations raise the limitations of studies that examine motor capacities in isolation from other factors (such as tactile perception) that may influence overall braille reading rates. Of interest is that, in this review, only the study by Mommers [Citation75] included both measures of tactile perception and motor capacities within the same sample.
Finally, it is well established that motor dexterity, and particularly fine motor skills, declines as a result of the normal aging process and may carry additional consequences that should be considered within the training context [Citation26,Citation38,Citation90]. Though manual dexterity training has led to performance gains among older sighted adults, the degree to which such gains are possible appears to depend on the complexity of the task [Citation38]. Importantly, none of the studies in this review measure fine motor dexterity or whether age-related changes may influence the hand movements which support braille reading.
Cognitive capacities
In total, 5 of the articles (representing 5 studies) in this review directly explore the relationship between cognitive capacities and braille reading performance (see ). Most of these studies explore the influence of short-term working memory on braille reading outcomes, with a total of 4 studies falling within this domain. Despite an evident relationship between working memory and aspects of braille reading performance, the studies in this review employ a wide range of working memory instruments including those which require the completion of auditory or braille reading span tasks, but none specifically evaluated tactile short-term working memory. While this is not inconsistent with research on sighted readers (where measures of listening comprehension have been shown to be associated with reading comprehension ability, for example [Citation61]), care must be taken when using such measures to ensure that other impairments (such as undiagnosed hearing loss) are not confounding results. Furthermore, assessing braille reading performance against a task which itself requires the reading of braille (in the case of “braille span” measures [Citation61], for example) will potentially disadvantage those with poor braille skills who may read slower and who experience greater cognitive load during reading. Instruments such as the one described in Papagno et al. [Citation91] may be worth further exploration as a method for better isolating tactile short-term working memory performance from the potential influence of reading ability.
Prior research also highlights the need to assess comprehension independently of short-term working memory. Of interest, these cognitive aspects are not considered within the studies of this review, save for Daneman [Citation61] where a comprehension monitoring exercise was proposed to permit assessment of comprehension even in the presence of degraded short-term working memory. These factors are important to control in future research particularly given that cognitive processing errors common among older adults may be masked by apparent poor performance on other measures (such as tactile acuity assessments) [Citation92].
Consideration of age
It is apparent that, although the studies in this review examine different aspects of braille reading performance, this research focuses heavily on younger readers and on those who learn braille early in childhood. Of the 40 studies, only 13 include participants who are above the age of 60, most of whom learned braille early in life. Moreover, where braille learning age is directly explored in relation to reading performance measures, insufficient information is often available. For example, Laroche [Citation72] merely divides participants between those who learn before and after the age of 10. This limits the degree to which results can be meaningfully interpreted, given that the abilities of adults differ drastically from those in older adulthood who experience greater age-related declines [Citation3]. Though it is understood that the typical aging process contributes to declines in tactile, motor and cognitive capacities [Citation3], evidence also indicates that individuals with extensive tactile exposure and practice maintain tactile perception abilities as they age [Citation9]. For these reasons, the chronological age of participants should not be examined in isolation from their braille learning age or frequency of braille usage. Despite these considerations, none of the studies in this review consider these age-related variables in unison.
Limitation and weaknesses of this study
This is the first study to synthesize primary research on the relationship between physiological and cognitive capacities and braille reading performance. It is possible that some relevant articles have been omitted if the titles and abstracts did not clearly map onto the inclusion criteria. We limited our search to four academic databases, and on peer-reviewed articles published in English. Nonetheless, we conducted a manual search through the Journal of Visual Impairment and Blindness and through the reference lists of all included articles, and placed no restrictions on date of publication.
Second, as with other scoping reviews, this overview does not aggregate research findings nor eliminate studies on the basis of quality, sample size and effect size. Given the low prevalence of blindness which often contributes to smaller sample sizes, it was believed that a meta-analysis would significantly restrict the scope of research considered. Future studies are needed to build upon this knowledge base and to assess the reliability of specific measurement instruments.
Third, we restricted this review to the physiological and cognitive capacities known to decline with age. Importantly, we did not consider external factors which may further influence the braille learning experience. Research points to a persistent shortage of specialized teachers who serve blind children, and access to rehabilitation services for adults may be constrained by geographic location, funding programs and restrictive eligibility criteria [Citation18]. Future research is needed to explore the facilitators and barriers encountered by adults and seniors who pursue braille training, in order to understand the influence of external factors on the adult braille learning process.
Conclusion
Collectively, the studies in this review underscore the importance of developing tactile perception and efficient hand reading strategies throughout the learning process. However, they do not directly explore the potential influence of age-related declines in fine-motor and short-term working memory. Moreover, this research focuses heavily on younger participants and on individuals who learned braille early in life. As rehabilitation practitioners encounter a growing number of older adults with acquired visual impairments, it will be vital to understand how the aging process may uniquely shape their braille learning experiences. This context would highlight where areas of difficulties may exist, and what specific remedial activities will help to support the success of older clients who are served.
Supplementary Material
Download MS Word (83.7 KB)Acknowledgments
The authors would like to thank Research Assistants Camille Demers, Meaghan Barlow and Fatima Tangkhpanya who assisted with locating and retrieving articles, formatting, and referencing in the manuscript. We thank Atul Jaiswal for his guidance on conducting scoping reviews.
Disclosure statement
The authors report no conflicts of interest.
Data availability statement
The authors confirm that the data supporting the findings of this study are available within the article. Readers interested in accessing our selected articles for specific purposes related to their respective research are invited to do so by contacting the corresponding author through the provided email address.
Additional information
Funding
References
- Kusajima T. Visual reading and braille reading: an experimental investigation of the physiology and psychology of visual and tactual reading. New York (NY): American Foundation of the Blind; 1974.
- Wormsley DP, D'Andrea FM. Instructional strategies for braille literacy. New York (NY): American Foundation for the Blind; 1997.
- Kandel ER, Schwartz JH, Jessell TM, et al. Principles of neural science. New York (NY): McGraw Hill; 2013.
- Holbrook MC, McCarthy T, Kamei-Hannan C. Foundations of education: volume I: history and theory of teaching children and youths with visual impairments. 3rd ed. New York (NY): AFB Press; 2017.
- Ferrell KA, Mason L, Young J, et al. Forty years of literacy research in blindness and visual impairment. Greeley (CO): University of Northern Colorado; 2006.
- Steinman BA, LeJeune B, Kimbrough B. Developmental stages of reading processes in children who are blind and sighted. J Vis Impair Blind. 2006;100:36–46.
- Goldreich D, Kanics IM. Performance of blind and sighted humans on a tactile grating detection task. Percept Psychophys. 2006;68:1363–1371.
- Nolan CY, Morris JE. Development and validation of the Roughness Discrimination Test. Int J Educ Blind. 1965;15:1–6.
- Legge GE, Madison CM, Vaughn BN, et al. Retention of high tactile acuity throughout the life span in blindness. Percept Psychophys. 2008;70:1471–1488.
- Stevens JC, Foulke E, Patterson MQ. Tactile acuity, aging, and braille reading in long-term blindness. J Exp Psychol Appl. 1996;2:91–106.
- Bola L, Siuda-Krzywicka K, Paplinska M, et al. Braille in the sighted: teaching tactile reading to sighted adults. PLoS One. 2016;11:e0153394.
- Veispak A, Boets B, Ghesquière P. Differential cognitive and perceptual correlates of print reading versus braille reading. Res Dev Disabil. 2013;34:372–385.
- Veispak A, Boets B, Ghesquière P. Parallel versus sequential processing in print and braille reading. Res Dev Disabil. 2012;33:2153–2163.
- Van Boven RW, Johnson KO. The limit of tactile spatial resolution in humans: grating orientation discrimination at the lip, tongue, and finger. Neurology. 1994;44:2361–2361.
- Varma R, Vajaranant T, Burkemper B. Visual impairment and blindness in adults in the United States: Demographic and geographic variations from 2015 to 2050. J Am Med Assoc Opthalmol. 2016;134:802–809.
- Cruess AF, Gordon KD, Bellan L, et al. The cost of vision loss in Canada. 2. Results. Can J Ophthalmol. 2011;46:315–318.
- Cryer H, Home S. Final report: feasibility of developing a diagnostic touch test to determine braille reading potential. Birmingham (UK): RNIB Centre for Accessible Information; 2011.
- Ponchillia PE, Durant PA. Teaching behaviors and attitudes of braille instructors in adult rehabilitation centers. J Vis Impair Blind. 1995;89:432–439.
- Ponchillia PE, Ponchillia SV. Foundations of rehabilitation teaching with persons who are blind or visually impaired. New York (NY): American Foundation for the Blind; 1996.
- Schroeder FK. Perceptions of braille usage by legally blind adults. J Vis Impair Blind. 1996;90:210–218.
- Rubin GS. Measuring reading performance. Vision Res. 2013;90:43–51.
- Brown JC, Goldstein JE, Chan TL, et al. Characterizing functional complaints in patients seeking outpatient low-vision services in the United States. Ophthalmology. 2014;121:1655–1662.
- Rex E, Koenig A, Wormsley D, et al. Foundations of braille literacy. New York (NY): American Foundation for the Blind; 1995.
- Ozioko O, Hersh MA, editors. Development of a portable two-way communication and information device for deafblind people. Proceedings of the 13th AAATE Conference; 2015 Sep 9–12; Budapest, Hungary; 2015.
- Heller KW, D'Andrea FM, Forney PE. Determining reading and writing media for individuals with visual and physical impairments. J Vis Impair Blind. 1998;92:162–175.
- Hughes B. Movement kinematics of the braille-reading finger. J Vis Impair Blind. 2011;105:370–381.
- Bernbaum M, Albert SG, McGarry JD. Diabetic neuropathy and braille ability. Arch Neurol. 1989;46:1179–1181.
- Hall AD, Newman SE. Braille learning: relative importance of seven variables. Appl Cognit Psychol. 1987;1:133–141.
- Hannan CK. Review of research: neuroscience and the impact of brain plasticity on braille reading. J Vis Impair Blind. 2006;100:397–413.
- Knowlton M, Wetzel R. Braille reading rates as a function of reading tasks. J Vis Impair Blind. 1996;90:227–236.
- Nolan CY, Kederis JC. Perceptual factors in braille word recognition (research series no. 20). New York (NY): American Foundation for the Blind; 1969.
- Bopp KL, Verhaeghen P. Aging and verbal memory span: a meta-analysis. J Gerontol B Psychol Sci Soc Sci. 2005;60:P223–P233.
- Millar S. Perceptual and task factors in fluent braille. Perception. 1987;16:521–536.
- Argyropoulos V, Papadimitriou V. Braille reading accuracy of students who are visually impaired: the effects of gender, age at vision loss, and level of education. J Vis Impair Blind. 2015;109:107–118.
- Simón C, Huertas JC. How blind readers perceive and gather information written in braille. J Vis Impair Blind. 1998;92:322–330.
- Stevens JC. Aging and spatial acuity of touch. J Gerontol. 1992;47:P35– 40.
- Goldreich D, Kanics IM. Tactile acuity is enhanced in blindness. J Neurosci. 2003;Apr 1523:3439–3445.
- Voelcker-Rehage C. Motor-skill learning in older adults – a review of studies on age-related differences. Eur Rev Aging Phys Act. 2008;5:5–16.
- Gunning-Dixon F, Brickman AM, Cheng JC, et al. Aging of cerebral white matter: a review of MRI findings. Int J Geriatr Psychiatry. 2009;24:109–117.
- Persson J, Pudas S, Lind J, et al. Longitudinal structure-function correlates in elderly reveal MTL dysfunction with cognitive decline. Cereb Cortex. 2012;22:2297–2304.
- Siegel L. Working memory and reading: a life-span perspective. Int J Behav Dev. 1994;17:109–124.
- Bruns P, Camargo CJ, Campanella H, et al. Tactile acuity charts: a reliable measure of spatial acuity. PLoS One. 2014;9:e87384.
- Foulke E. Reading braille. In: Schiff W, Foulke E, editors. Tactual perception: a sourcebook. New York (NY): Cambridge University Press; 1982. p. 168–208.
- Heller MA, Gentaz E. Psychology of touch and blindness. New York (NY): Psychology Press; 2013.
- Weber EH. Weber on the tactile senses. 2nd ed. Erlbaum (UK): Taylor & Francis, Publ; 1996. (Ross HE, Murray DJ, editors).
- Schwartz AS, Perey AJ, Azulay A. Further analysis of active and passive touch in pattern discrimination. Bull Psychon Soc. 1975;6:7–9.
- Corn AL, Lusk KE. Perspectives on Low Vision (Chapter 1). In: Corn AL, Erin JN, editors. Foundations of low vision: clinical and functional perspectives. New York (NY): American Foundation for the Blind; 2010. p. 3–34.
- Dixon J, editor. Braille into the next milennium. Washington (DC): National Library Service for the Blind and Physically Handicapped; 2000.
- Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res. 2005;8:19–32.
- Levac D, Colquhoun H, O'Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5:69.
- Peters MD, Godfrey CM, Khalil H, et al. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. 2015;13:141–146.
- Tiffin J, Asher EJ. The Purdue pegboard; norms and studies of reliability and validity. J Appl Psychol. 1948;32:234–247.
- Wormsley DP. Hand movement training in braille reading. J Vis Impair Blind. 1981;75:327–331.
- Murman DL. The impact of age on cognition. Semin Hear. 2015;36:111–121.
- Gamer M, Lemon J, Fellows I, et al. Package 'irr': various coefficients of interrater reliability and agreement (version 0.84). 2012.
- Revelle W. Package 'psych': procedures for psychological, psychometric, and personality research (version 1.7.8). 2017.
- Bertelson P, Mousty P, D'Alimonte G. A study of braille reading: 2. Patterns of hand activity in one-handed and two-handed reading. Q J Exp Psychol A. 1985;37:235–256.
- Bradshaw JL, Nettleton NC, Spehr K. Braille reading and left and right hemispace. Neuropsychologia. 1982;20:493–500.
- Chen X, Liang L, Lu M, et al. The effects of reading mode and braille reading patterns on braille reading speed and comprehension: A study of students with visual impairments in China. Res Dev Disabil. 2019;91:103424.
- Clegg GD. A study of the Tactual Discrimination Test for measuring tactual ability of the visually handicapped. Research Bulletin No. 25 – January 1973. New York (NY): The American Foundation for the Blind; 1973. p. 259–260.
- Daneman M. How reading braille is both like and unlike reading print. Mem Cognit. 1988;16:497–504.
- Davidson PW, Wiles-Kettenmann M, Haber RN, et al. Relationship between hand movements, reading competence and passage difficulty in braille reading. Neuropsychologia. 1980;18:629–635.
- Davidson PW, Appelle S, Haber RN. Haptic scanning of braille cells by low- and high-proficiency blind readers. Res Dev Disabil. 1992;13:99–111.
- Fertsch P. An analysis of braille reading. Outlook Blind Teach Forum. 1946;40:128–131.
- Fertsch P. Hand dominance in reading braille. Am J Psychol. 1947;60:335–349.
- Foulke E. Transfer of a complex perceptual skill. Percept Mot Skills. 1964;18:733–740.
- Garcia LG. Assessment of text reading comprehension by Spanish-speaking blind persons. Br J Vis Impair. 2004;22:4–12.
- Heinrichs R, Moorhouse J. Touch-perception thresholds in blind diabetic subjects in relation to the reading of Braille type. N Engl J Med. 1969;280:72–75.
- Hermelin B, O'Connor N. Functional asymmetry in the reading of Braille. Neuropsychologia. 1971;9:431–435.
- Hislop DW, Zuber BL, Trimble JL. Text-scanning patterns of blind readers using Optacon and braille. J Rehabil Res Dev. 1985;22:54–65.
- Holland BF. Speed and pressure factors in braille reading. J Vis Impair Blind. 1934;28:13–17.
- Laroche L, Boulé J, Wittich W. Reading speed of contracted French braille. J Vis Impair Blind. 2012;106:37–42.
- Loomis JM. Tactile recognition of raised characters: a parametric study. Bull Psychon Soc. 1985;23:18–20.
- Millar S. Is there a “best hand” for braille? Cortex. 1984;20:75–87.
- Mommers MJC. Braille reading: factors affecting achievement of Dutch elementary school children. J Vis Impair Blind. 1976;70:332–340.
- Mommers MJC. Braille reading: effects of different hand and finger usage. J Vis Impair Blind. 1980;74:338–343.
- Mousty P, Bertelson P. A study of braille reading: 1. Reading speed as a function of hand usage and context. Q J Exp Psychol A. 1985;37:217–233.
- Nakada M, Dellon L. Relationship between sensibility and ability to read braille in diabetics. Microsurgery. 1989;10:138–141.
- Olson M, Harlow SD, Williams J. Rapid reading in braille and large print: an examination of McBride’s procedures. J Vis Impair Blind. 1975;69:392–395.
- Oshima K, Arai T, Ichihara S, et al. Tactile sensitivity and braille reading in people with early blindness and late blindness. J Vis Impair Blind. 2014;108:122–131.
- Papadimitriou V, Argyropoulos V. The effect of hand movements on braille reading accuracy. Int J Educ Res. 2017;85:43–50.
- Sampaio E, Philip J. Influences of age at onset of blindness on braille reading performances with left and right hands. Percept Mot Skills. 1995;81:131–141.
- Veispak A, Boets B, Männamaa M, et al. Probing the perceptual and cognitive underpinnings of braille reading. An Estonian population study. Res Dev Disabil. 2012;33:1366–1379.
- Wilkinson JM, Carr TH. Strategic hand use preferences and hemispheric specialization in tactual reading: impact of the demands of perceptual encoding. Brain Lang. 1987;32:97–123.
- Wormsley DP. Reading rates of young braille-reading children. J Vis Impair Blind. 1996;90:278–282.
- Wright T, Wormsley DP, Kamei-Hannan C. Hand movements and braille reading efficiency: data from the Alphabetic Braille and Contracted Braille Study. J Vis Impair Blind. 2009;103:649–661.
- Braun V, Clarke V. Thematic analysis. In: Cooper H, Camic PM, Long DL, et al., editors. APA handbook of research methods in psychology. Volume 2. Research designs: quantitative, qualitative, neuropsychological, and biological. APA handbooks in psychology®. Washington (DC): American Psychological Association; 2012. p. 57–71.
- Bertelson P. Language by touch: the case of braille reading. In: de Gelder B, Morais J, editors. Speech and reading: a comparative approach. Erlbaum (UK): Taylor & Francis; 1995. p. 91–108.
- Golub DB. A model of successful work experience for employees who are visually impaired: the results of a study. J Vis Impair Blind. 2006;100:715–725.
- Lorimer P. Hand techniques in reading braille; synthesis of spatial and verbal elements of reading. Br J Vis Impair. 2002;20:76–79.
- Papagno C, Minniti G, Mattavelli GC, et al. Tactile short-term memory in sensory-deprived individuals. Exp Brain Res. 2017;235:471–480.
- Daneman M, Carpenter PA. Individual differences in working memory and reading. J Verbal Learning Verbal Behav. 1980;19:450–466.