
Abstract
Purpose
To study differences between men and women in physical activity (PA) and health-related quality of life (HRQoL) before and after participating in a supported osteoarthritis (OA) self-management programme.
Materials and methods
A prospective observational study using data from a Swedish National Quality Register. Patients recorded between 2008 and 2013 with hip and/or knee OA with data at baseline, at 3 and 12 months follow-up (n = 7628) were included. Outcome measures were patient-reported PA and HRQoL (EQ-5D-3L).
Results
A greater proportion of men (p = 0.002) changed to being physically active ≥150 min/week at 3 months follow-up. The proportion of women being physically active ≥150 min/week was larger than for men at baseline (p = 0.003) and at follow-up at 12 months (p = 0.035). Women reported lower HRQoL than men at baseline (p < 0.001), at follow-up at 3 (p < 0.001) and 12 months (p = 0.010). There were no differences between men and women in change in HRQoL at 3 (p = 0.629) and 12 months (p = 0.577) follow-up.
Conclusions
This study showed differences between men and women in PA and HRQoL before and after participating in a supported OA self-management programme. These differences should be considered when supporting PA and HRQoL.
Men with hip and/or knee osteoarthritis (OA) might need more support during rehabilitation in order to maintain or even increase physical activity (PA) in the long run.
Women with hip and/or knee OA might need more support during rehabilitation in order to maintain or even increase health-related quality of life (HRQoL) in the long run.
Booster sessions might be suggested in order to enable both men and women with hip and/or knee OA to sustain improvements in PA and HRQoL after participating in a supported OA self-management programme.
Implications for rehabilitation
Introduction
Osteoarthritis (OA) is considered to be a serious condition [Citation1], which causes difficulties in managing activities of daily life, leads to lower health-related quality of life (HRQoL) [Citation2], and increased risk of premature mortality [Citation1,Citation3]. Symptomatic hip and knee OA affect approximately 10% of men and 18% of women over the age of 60 years [Citation4,Citation5] and the prevalence increases with age [Citation4,Citation6]. Currently, there is no cure or signs of spontaneous remission for OA [Citation1,Citation7], and treatment is focused on relieving the symptoms [Citation7]. First line treatment is information, physical exercise and weight reduction that, according to the evidence, is the best treatment for patients with hip and knee OA [Citation8–10]. In Sweden, first line treatment is often offered through a supported OA self-management programme (SOASP) given within a physiotherapy context [Citation11,Citation12]. The SOASP combines information with exercise in clinical practice and usually offers 6–8 weeks of supervised exercise [Citation11]. The programme has been described elsewhere [Citation11].
Since 2008, there is a register in Sweden called “Better management of patients with OsteoArthritis” (BOA) [Citation12,Citation13]. The register evaluates patient-reported outcome measures (PROMs) collected by a physiotherapist (PT) or an occupational therapist at baseline, at 3 and 12 months after participating in a SOASP [Citation11,Citation12]. The BOA became a National Quality Register in 2010 [Citation12,Citation13].
The World Health Organization (WHO) recommends adults (18–64 years old) to be physically active for at least 150 min a week at a moderate-intensity level, i.e., 3.0–5.9 times the intensity of rest. Episodes of at least 10 min can be added together to achieve the recommended level [Citation14]. Research has shown that physical activity (PA) has a positive effect on OA-related pain and physical function at least in the short run [Citation15,Citation16], and patients who are physically active on a regular basis report less intense pain [Citation17]. A meta-analysis has shown that only a small to moderate proportion of people with hip or knee OA met PA guidelines and recommended steps per day [Citation18] and in a study by Dunlop et al., a large majority of both men and women with knee OA did not reach the recommended level of PA [Citation19].
Health-related quality of life is often impaired for patients with OA [Citation20,Citation21]. HRQoL can be positively affected by PA and the positive effect may last from two to six months [Citation16,Citation22], up to 18 months [Citation23]. However, if patients do not maintain the exercise programme, the positive effects may be lost [Citation24,Citation25]. Women with OA report lower HRQoL than men [Citation21,Citation26], and also report more pain [Citation27,Citation28] and disability than men [Citation29]. The reasons for these differences in severity of OA between men and women are not well known but may be due to factors such as disparities in anatomy, hormonal influences, and previous joint injury [Citation28].
According to the annual BOA report, men tend to be more afraid than women that PA will harm the joints [Citation12]. However, whether men and women have different patient reported outcomes from the SOASP according to BOA has not yet been fully studied. The aim was to study differences between men and women with hip and/or knee OA in PA and HRQoL before and after participating in a SOASP.
Materials and methods
Design
We performed a prospective observational study, using patient-reported data from the BOA register between the years 2008 and 2013. The study was approved by the Regional Ethical Review Board in Gothenburg (782-14).
Data collection
In Sweden, patients who seek health care consultation due to symptoms from hip and/or knee OA and who are diagnosed with symptomatic and/or radiographic OA meet the inclusion criteria to participate in both the SOASP and to be included in the BOA register. Patients who meet the inclusion criteria and who approve to enter the BOA register fill in a questionnaire prior to participating in the SOASP (baseline), and at follow-up at 3 and 12 months. At the time when data were retrieved and during the studied period, patients that had inflammatory joint disease, other serious injuries or illnesses, sequelae hip fractures, and patients who did not understand the Swedish language were not included in the BOA register. Data from the questionnaires are recorded in the BOA register, either by the PT responsible for the self-management programme, or by administrative personnel. As from 2018, patients are also able to answer the questionnaires digitally. The questionnaires contain questions on age, sex, height, weight and which joint is affected by OA [Citation12]. Instruments that measure pain (Visual Analogue Scale, VAS), HRQoL (EQ-5D), self-efficacy (Arthritis Self-Efficacy Scale, ASES-S), and questions about PA [Citation12] are also included in the questionnaires. The coverage ratio for the BOA register, estimated on the proportion of patients attending the SOASP that are also recorded in the register, was 77% for the studied period [Citation30].
During the study period (2008–2013), 25 862 patients were recorded in the BOA register (29.9% men and 70.1% women). Information about age, sex, body mass index (BMI), most affected joint, PA, and HRQoL at baseline and at follow-up at 3 and 12 months, was collected from the BOA register.
Study cohort
We included data from patients that had three registrations (baseline and at follow-up at 3 and 12 months) on PA and/or HRQoL (n = 7628) (). If data for PA and HRQoL were missing at any point, the patients were excluded. Reasons for missing data at 3 and/or 12 months follow-up were that patients had dropped out for surgery or other causes (n = 6531), but also that patients had not reached the time for the follow-ups yet and thus there were no registrations available at follow-up at both 3 and 12 months (n = 11 703) in the register.
Figure 1. Flowchart for the selection of data for analysis in the study.
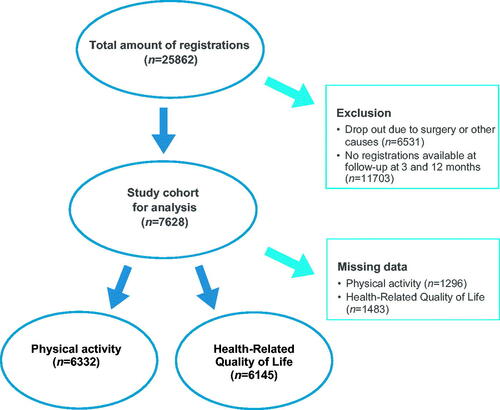
In the study cohort (n = 7628), there were paired data for 6332 recorded patients regarding the questions concerning PA and exercise available at baseline, and at follow-up at 3 and 12 months, respectively. For data regarding HRQoL, there were paired data for 6145 recorded patients available.
The study cohort consisted of 27.3% men (n = 2079) and 72.7% women (n = 5549). Mean age was 65.3 (SD 9.2) (men 65.7 (SD 9.3), women 65.2 (SD 9.2)). The majority (72.2%) reported problems in the knee (men 71.6%, women 72.4%) and 27.0% (men 27.6%, women 26.8%) reported problems in the hip. There were some missing data on most affected joint (n = 61, 0.8%). Mean BMI was 28.0 (SD 4.8) (men 27.9 (SD 4.0), women 28.0 (SD 5.1)).
The study cohort (n = 7628) did not differ from the original cohort of registered patients (n = 25 862) in the BOA register at the time.
Demographic data for the population with paired data on PA (n = 6332) and HRQoL (n = 6145) did not differ from the study cohort (n = 7628), nor did demographic data for the population of missing data regarding PA (n = 1296) and HRQoL (n = 1483).
Outcome measures
Physical activity and exercise
The questions about PA and exercise follow the recommendation from the National Board of Health and Welfare in Sweden and have been changed in the BOA questionnaires over the years. Between 2008 and 31 August 2012, there was one question about PA (“In an ordinary week, on how many days are you physically active for at least 30 min a day?”. The eight possible answers were none to seven days) and two questions about exercise (“In general, how often do you exercise so you are breathless or sweat?”. The seven possible answers were: never, less than once a month, once or twice a month, once a week, twice or three times a week, four to six times a week, and every day. “If you exercise, for how long do you exercise each time, in general?”. The four possible answers were less than 15 min, 15–30 min, 31–60 min, more than an hour) [Citation31]. Since 1 September 2012 the following questions, developed by the Swedish National Board of Health and Welfare and validated against accelerometer [Citation32], are included in the BOA questionnaires: (1) How much time do you devote to PA that makes you short of breath, for example running, keep-fit exercises, or ball games? The six possible answers are no time, less than 30 min, 30–60 min, 60–90 min, 90–120 min, and >120 min. (2) How much time do you devote to everyday PA such as walking, bicycling, or gardening? Include all activities lasting 10 min at a time. The seven possible answers are no time, less than 30 min, 30–60 min, 60–90 min, 90–150 min, 150–300 min, and >300 min. The questions refer to an ordinary week, where the first question relates to exercise and the second to PA [Citation12,Citation31].
Health-related quality of life – EQ-5D index
In the BOA register, HRQoL is measured by EQ-5D [Citation12], which is a generic non-disease specific outcome score where patients score their self-perceived function and health [Citation33,Citation34]. The instrument can be used in evaluation of clinical and economical outcomes [Citation35]. EQ-5D is frequently used in research on OA [Citation36,Citation37]. The instrument consists of two parts. In the descriptive part there are five questions concerning mobility, self-care, activities of daily life, pain/discomfort, and anxiety/depression [Citation34]. During the study period, the EQ-5D-3L was used in the BOA register [Citation12]. For each question, there are three possible answers (no problems, moderate problems, and severe problems) that correspond to a number (1, 2, and 3, respectively) [Citation34]. Each number can be combined into a five-digit number [Citation34,Citation38]. There are 243 possible combinations [Citation34]. A weighted total value with a minimum of −0.594, i.e., dead, and a maximum of 1.0, i.e., full health, provides the result of EQ-5D as a global health index [Citation38]. In our study, the British tariff was used by the BOA register, since there was no Swedish tariff available at the time [Citation39,Citation40]. Studies support validity and reliability for the EQ-5D for several diseases [Citation37,Citation41,Citation42]. EQ-5D has shown sufficient reliability for use in relation to OA [Citation36].
Statistical analysis
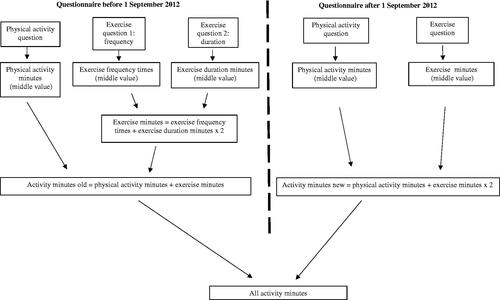
Data from the questions about PA and exercise before and after the 1 September 2012 were analysed. In order to obtain comparable data on PA and exercise for the whole study period, data from all questions were first coded into minutes. For each possible answer, the middle value was chosen, i.e., 15 for the interval less than 30 min, 45 for the interval 30–60 min, 75 min for the interval 60–90 min, 105 min for the interval 90–120 min and so on. Zero was chosen for the answer no time. Then, data were added together according to the definition of minutes of activity, i.e., minutes of PA plus minutes of exercise [Citation43]. According to the definition, one minute of PA at vigorous-intensity equates to two minutes of PA at moderate-intensity [Citation43]. Regarding the questions before 1 September 2012, the two questions about exercise were first added together and then added to the question about PA according to the formula for minutes of activity [Citation43]. Finally, the minutes of activity for all questions about PA and exercise, both before and after 1 September 2012, were added together (). The same procedure was performed with the data from baseline and at follow-up at 3 and 12 months, respectively.
Figure 2. Model for calculation of activity minutes.
Data on PA was also dichotomised to being sufficiently physically active (≥150 activity minutes a week) or insufficiently physically active (<150 activity minutes a week) based on the recommendations of WHO [Citation14]. We calculated the proportion of patients being sufficiently or insufficiently physically active at baseline, and at 3 and 12 months follow-up. This was also done for men and women separately.
Mean values (SD) for HRQoL were calculated for the total study cohort and for men and women.
Any change in the patients’ self-reporting of PA minutes and HRQoL over time was divided into three categories in terms of change, i.e., increased, decreased and no change. Regarding the PA minutes, the category called increased includes data from patients that at baseline reported to be physically active 30–60 min a week (middle value 45 min used) and at follow-up at 3 months reported to be physically active 60–90 min a week (middle value 75 min used), and likewise was done for the rest of the possible answers. The category called decreased includes data from patients that at baseline reported to be physically active 60–90 min a week (middle value 75 min used) and at follow-up at 3 months reported to be physically active 30–60 min a week (middle value 45 min used), and so on for the rest of the possible answers. The category called no change includes data from patients reporting to be equally physically active, for example, 30–60 min a week (middle value 45 min used), both at baseline and at follow-up at 3 months. Regarding HRQoL, patients reporting a higher value (≥0.1) on the EQ-5D-3L-index score at follow-up at 3 months compared to baseline were categorised as increased, patients reporting a lower value (<0.1) on the EQ-5D-3L-index score at follow-up at 3 months were categorised as decreased and patients reporting the same value on the EQ-5D-3L-index score at follow-ups compares to baseline were categorised as no change.
Change in being sufficiently physically active or insufficiently physically active at follow-ups compared to baseline was also analysed and categorised in four groups: from insufficient to sufficient PA, still sufficient PA, still insufficient PA, and from sufficient to insufficient PA. This means that data from patients reporting to be physically active <150 activity minutes a week at baseline and ≥150 activity minutes a week at follow-ups were categorised in the group called insufficient to sufficient PA. Data from patients reporting to be physically active ≥150 activity minutes a week at baseline and <150 activity minutes a week at follow-ups were categorised in the group called sufficient to insufficient PA. Data from patients reporting to be equally physically active at follow-ups compared to baseline were categorised either in the group called still sufficient PA or still insufficient PA depending on if they reported to be physically active ≥150 activity minutes a week or <150 activity minutes a week.
The Chi-square test was used in the data analysis of differences in proportions of men and women regarding sufficient PA, and in analysis of differences in proportions of men and women in change of PA minutes and HRQoL. The z-test (Bonferroni’s adjusted) was used to test the significance of differences in proportions of men and women in change of PA categorised in the four groups (insufficient to sufficient PA, still sufficient PA, still insufficient PA, and from sufficient to insufficient PA). The t-test (two-tailed) was used for analysing differences between men and women regarding HRQoL. A p value < 0.05 was considered to be statistically significant. Statistical analysis was performed using the SPSS version 21 (SPSS Inc., Chicago, IL).
Results
Physical activity
A majority of both men and women reported to be sufficiently physically active (≥150 activity minutes a week) at baseline and at follow-up at 3 and 12 months, respectively. The proportion of women that were physically active ≥150 min a week was larger than for men at baseline (p = 0.003) and at follow-up at 12 months (p = 0.035). At 3 months follow-up, the proportion of physically active men and women was almost the same (p = 0.605) ().
Table 1. Differences in physical activity for men (n = 1721) and women (n = 4611), and in health-related quality of life (HRQoL)a for men (n = 1654) and women (n = 4491) at baseline and at follow-up at 3 and 12 months.
There were no statistically significant differences in proportion of men and women in reporting any change, i.e., increased, decreased, or no change, in PA minutes between baseline and follow-up at 3 months (p = 0.085) or between baseline and follow-up at 12 months (p = 0.530) ().
Table 2. Difference in proportion (%) of men and women in increase, decrease or no change in physical activity, and health-related quality of life (HRQoL)a between baseline and follow-up at 3 and at 12 months.
The analysis of change in PA, categorised in four groups (from insufficient to sufficient PA, still sufficient PA, still insufficient PA, and from sufficient to insufficient PA) showed that there were differences between men and women both between baseline and follow-up at 3 (p = 0.013) and 12 months (p = 0.009) ().
Table 3. Differences in proportion (%) of men and women in change of physical activity group (insufficient to sufficient PA, still sufficient PA, still insufficient PA, and sufficient to insufficient PA), between baseline and follow-up at 3 and at 12 months.
Therefore, a further analysis was performed, showing that a greater proportion of men changed from insufficient to sufficient PA (men 13%, women 10.2%, p = 0.002) between baseline and 3 months follow-up. A larger proportion of women were still sufficiently physically active both at 3 (men 75.6%, women 78.8%, p = 0.006) and 12 (men 67.9%, women 71.0%, p = 0.015) months follow-up. A larger proportion of men (men 10.3%, women 7.8%, p = 0.002) were still insufficiently physically active at 12 months follow-up.
Health-related quality of life
There were differences in how men and women reported HRQoL, both at baseline (p < 0.001) and at 3 (p < 0.001) and 12 (p = 0.010) months follow-up ().
There were no statistically significant differences in proportion of men and women in reporting any change, i.e., increased, decreased, or no change, in HRQoL between baseline and follow-up at 3 months (p = 0.629) or between baseline and follow-up at 12 months (p = 0.577) ().
Discussion
In this study, a majority of both men and women were already sufficiently physically active before the SOASP, and a greater proportion of women were sufficiently physically active compared to men, both at baseline and at follow-up at 12 months. At follow-up at 3 months, there was no difference in proportion of men and women being sufficiently physically active. Women reported lower HRQoL than men, both at baseline and at follow-up at 3 and 12 months.
Our results on men and women self-reporting to be sufficiently physically active are in line with another study based on data from the BOA register, where PA was analysed in a slightly different way [Citation44]. When self-reporting data, there is both a risk for recall bias and a risk that people overrate their level of PA and exercise [Citation45]. This is something that can affect the result in our study since PA data are self-reported in the BOA register.
Overall, men and women in this study seem to follow the same pattern when reporting any change (increase, no change, decrease) in PA at the follow-ups. The increase at 3 months follow-up is not surprising since the intervention lasts for 3 months, and the patients are likely to have had continuous and regular contact with their PT during that time, which has proven to be beneficial for maintaining PA [Citation46]. At 12 months follow-up, the proportion of both men and women being sufficiently physically active had decreased compared to the follow-up at 3 months. Other studies have shown similar results, with a decrease in PA over time [Citation24,Citation25,Citation46], and when patients no longer have contact with the PT [Citation46]. Studies have also shown that having social support [Citation47,Citation48] and opportunities for organised exercise led by professionals [Citation48] are motivational factors for maintaining exercise [Citation47,Citation48]. Booster sessions and follow-ups are recommended to support exercise adherence [Citation49] and important to take in consideration when planning SOASP in the future.
A larger proportion of women than men self-reported to be sufficiently physically active at baseline and at follow-up at 12 months, which is not in line with another study [Citation19] analysing data from the USA where a larger proportion of men with knee OA met PA guidelines, monitored by accelerometer. Studies have shown that in the general population, women are less physically active than men in many countries [Citation50,Citation51], but in Sweden men and women are more equally physically active [Citation52]. Moreover, a European study, comparing PA patterns in older adults with and without knee OA, showed that in Sweden people with knee OA were as physically active as people in general [Citation53]. In 2018, 67% of men and women in the general population in Sweden, at the age of 16–84, self-reported to be sufficiently physically active [Citation52]. This means that the proportion of both men and women in our study reporting to be sufficiently physically active is larger than the proportion of people in the general Swedish population that report themselves to be so. This raises the question of whether there might be a selection bias, i.e., whether how representative the patients included in the BOA-register are in comparison to the total population with hip and/or knee OA in Sweden.
It is notable that when analysing change in PA categorised in four groups (insufficient to sufficient PA, still sufficient PA, still insufficient PA, and sufficient to insufficient PA), a larger proportion of men changed from insufficient PA to sufficient PA between baseline and 3 months follow-up. This might be explained by the fact that more men were insufficiently physically active at baseline, and therefore were able to increase their PA level. Since men seem to be more afraid than women that exercise will harm the joints [Citation12], men might benefit more from the support given by a PT during the intervention.
About a fifth of the total study cohort, more men (23.2%) than women (20.8%), did not reach the recommended level of PA at the 12-months follow-up. Physical inactivity can lead to a number of health-related problems [Citation14]. Further research is needed to investigate what effect being more physically active would have for this population [Citation18]. For the individual, increasing the PA-level on the whole and being as physically active as possible even if it means not reaching ≥150 activity minutes a week may have a significant impact on general health [Citation19,Citation54]. More research is needed to enable health care providers to identify physically inactive individuals with OA early in the disease process, since they are at an increased risk of developing comorbidities and premature mortality. Physically inactive men and women might need more attention, support and closer follow-ups.
Studies have shown similar results as in our study regarding HRQoL after participating in a SOAPS but the evidence seems to be inconclusive [Citation23,Citation55,Citation56]. In our study, both men and women reported higher HRQoL at follow-up at 3 months compared to baseline. The majority of the patients may still have some contact with their PT at follow-up at 3 months. This might explain why they improve their self-reported HRQoL during that time-span. Even though both men and women reported lower HRQoL at 12 months compared to 3 months, HRQoL was still higher at 12 months compared to baseline. This means that the increase in HRQoL is somewhat maintained after a year, which is encouraging both since the aim of the SOASP is increasing quality of life, and since OA is a progressive disease.
In our study, both men and women self-reported ≥0.6 on HRQoL at all measuring points. A score ≥0.6 on EQ-5D has been proposed as a minimum for having sufficient ability to work [Citation57,Citation58]. This means that the study cohort reports quite high HRQoL, and again the question of selection bias is raised. A recently published study, analysing data from the BOA register between 2008 and 2016, indicates that the SOASP does not reach out to people with OA that have a heavier socioeconomic burden, a group who often have a higher disease burden [Citation59].
Women usually report lower HRQoL than men [Citation21,Citation60], which agrees with the results in this study where women reported lower scores than men at both baseline and follow-up at 3 and 12 months. HRQoL, measured by the EQ-5D, is known to be affected by sociodemographic factors such as age and gender [Citation21,Citation60]. Studies show that women with the same radiographic knee findings as men report more pain [Citation27], more severe symptoms [Citation61], and have polyarticular OA more often than men [Citation62]. This is important to have in mind when interpreting the results, since both pain and OA are factors that have a major negative impact on HRQoL [Citation21].
It is noteworthy that although a larger proportion of women in this study reported lower HRQoL than men, more women also reported to be more physically active than men at all measuring points. A study by Tonelli et al., showed that although women reported more pain before a total knee replacement than men, they also reported to be as physically active as men were [Citation63]. Since both referral to orthopaedist and surgery are offered less frequently to women with OA [Citation29,Citation64], women may have to rely on coping and self-management strategies to a greater extent than men, and this would be interesting and important to investigate further.
This study is based on patient reported data from a national register that includes data from patients representing all parts of Sweden. The strength of this study was that only data with complete registrations, i.e., from baseline and follow-up at 3 and 12 months, respectively, were included. Another strength was the large study population included in the analysis.
There are some limitations in this study. First, the questions about PA and exercise have been changed in the questionnaires over the years. The original questions were more general than the revised ones, which make them difficult to compare. In general, measurements of PA vary in different studies [Citation18], which make it difficult to compare results from different studies.
Second, there may be other factors like for example sick-leave or occupation that might influence the outcome but such information was not available for us in this study. However, since men and women in the study cohort did not differ regarding age, BMI, or most affected joint, we have no reason to believe that those factors might affect the outcome.
Finally, it is unclear both how many people with hip and/or knee OA with serious symptoms that do not seek health care, and how many people with OA that seek health care but are not included in the BOA register. Therefore, it is uncertain how representative the studied cohort based on data from the register is to the total population with OA in Sweden.
A challenge for future studies is to develop strategies to identify people with hip and/or knee OA who are insufficiently physically active and/or report lower HRQoL, preferably early in the disease development, and to find efficient strategies to support and enable them to maintain or even increase their level of PA and HRQoL in the long run. More research is also needed to study what factors affect differences between men and women in outcome of SOASP.
Clinical implications
This study indicates that men might benefit more than women from participating in a SOASP when it comes to PA, at least in the short run (3 months follow-up). The differences between men and women found in this study imply a need to individualise the SOASP, and that booster sessions might be required.
Conclusions
This study showed differences between men and women before and after participating in a SOASP. More men increased their PA during the SOASP. More women were physically active ≥150 min a week at baseline and at 12 months follow-up, even though more women also reported lower HRQoL at all measuring points. These differences should be considered when planning for how to support men and women with hip and/or knee OA to maintain or even increase PA and HRQoL in the long run.
Acknowledgements
The authors would like to acknowledge all participating patients and all physiotherapists reporting data to the BOA register, and others involved in BOA. KÅ would like to acknowledge Antonio Marañon, who provided valuable professional statistical advice, and Carina Thorstensson, for valuable input throughout the research process.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- OsteoArthritis Research Society International. Osteoarthritis: a serious disease [Internet]. OsteoArthritis Research Society International; 2016 [updated 2019 Aug 20; cited 2019 Sep 9]. Available from: https://www.oarsi.org/education/oarsi-resources/oarsi-white-paper-oa-serious-disease
- Dieppe PA, Lohmander LS. Pathogenesis and management of pain in osteoarthritis. Lancet (London, England). 2005;365(9463):965–973.
- Hawker GA, Croxford R, Bierman AS, et al. All-cause mortality and serious cardiovascular events in people with hip and knee osteoarthritis: a population based cohort study. PLoS One. 2014;9(3):e91286.
- Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81(9):646–656.
- Murray CJL, Lopez AD. The global burden of disease: a comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. Cambridge (MA): The Harvard School of Public Health on behalf of the World Health Organization and the World Bank, distributed by Harvard Univ. Press; 1996.
- Turkiewicz A, Petersson IF, Bjork J, et al. Current and future impact of osteoarthritis on health care: a population-based study with projections to year 2032. Osteoarthritis Cartilage. 2014;22(11):1826–1832.
- Wittenauer RS, Aden K. Background paper 6.12 osteoarthritis [Internet]. World Health Organization; 2013 [cited 2019 Sep 9]. Available from: https://www.who.int/medicines/areas/priority_medicines/BP6_12Osteo.pdf?ua=1
- Hochberg MC, Altman RD, April KT, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care Res (Hoboken). 2012;64(4):465–474.
- McAlindon TE, Bannuru RR, Sullivan MC, et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis Cartilage. 2014;22(3):363–388.
- Fernandes L, Hagen KB, Bijlsma JW, et al. EULAR recommendations for the non-pharmacological core management of hip and knee osteoarthritis. Ann Rheum Dis. 2013;72(7):1125–1135.
- Thorstensson CA, Garellick G, Rystedt H, et al. Better management of patients with osteoarthritis: development and nationwide implementation of an evidence-based supported osteoarthritis self-management programme. Musculoskeletal Care. 2015;13(2):67–75.
- Thorstensson C, Dahlberg L, Garellick G. Better management of patients with osteoarthritis (BOA) annual report 2013. Gothenburg: Better Management of Patients with OsteoArthritis (BOA) register; 2014.
- Socialstyrelsen. Nationella riktlinjer – utvärdering: underlagsrapport: vård vid rörelseorganens sjukdomar: indikatorer och underlag för bedömningar. Stockholm: Socialstyrelsen; 2014.
- World Health Organization. Global recommendations on physical activity for health. Geneva: World Health Organization; 2010.
- Fransen M, McConnell S, Hernandez-Molina G, et al. Exercise for osteoarthritis of the hip. Cochrane Database Syst Rev. 2014;(4):CD007912.
- Fransen M, McConnell S, Harmer AR, et al. Exercise for osteoarthritis of the knee: a Cochrane systematic review. Br J Sports Med. 2015;49(24):1554–1557.
- Perrot S, Poiraudeau S, Kabir-Ahmadi M, et al. Correlates of pain intensity in men and women with hip and knee osteoarthritis. Results of a national survey: the French ARTHRIX study. Clin J Pain. 2009;25(9):767–772.
- Wallis JA, Webster KE, Levinger P, et al. What proportion of people with hip and knee osteoarthritis meet physical activity guidelines? A systematic review and meta-analysis. Osteoarthritis Cartilage. 2013;21(11):1648–1659.
- Dunlop DD, Song J, Semanik PA, et al. Objective physical activity measurement in the osteoarthritis initiative: are guidelines being met? Arthritis Rheum. 2011;63(11):3372–3382.
- Ackerman IN, Ademi Z, Osborne RH, et al. Comparison of health-related quality of life, work status, and health care utilization and costs according to hip and knee joint disease severity: a national Australian study. Phys Ther. 2013;93(7):889–899.
- Saarni SI, Harkanen T, Sintonen H, et al. The impact of 29 chronic conditions on health-related quality of life: a general population survey in Finland using 15D and EQ-5D. Qual Life Res. 2006;15(8):1403–1414.
- Hansson EE, Jonsson-Lundgren M, Ronnheden AM, et al. Effect of an education programme for patients with osteoarthritis in primary care – a randomized controlled trial. BMC Musculoskelet Disord. 2010;11(1):244.
- Brosseau L, Wells GA, Kenny GP, et al. The implementation of a community-based aerobic walking program for mild to moderate knee osteoarthritis: a knowledge translation randomized controlled trial: part II: clinical outcomes. BMC Public Health. 2012;12:1073.
- van Baar ME, Dekker J, Oostendorp RA, et al. Effectiveness of exercise in patients with osteoarthritis of hip or knee: nine months' follow up. Ann Rheum Dis. 2001;60(12):1123–1130.
- Pisters MF, Veenhof C, van Meeteren NL, et al. Long-term effectiveness of exercise therapy in patients with osteoarthritis of the hip or knee: a systematic review. Arthritis Rheum. 2007;57(7):1245–1253.
- Burstrom K, Johannesson M, Diderichsen F. Health-related quality of life by disease and socio-economic group in the general population in Sweden. Health Policy (Amsterdam, Netherlands). 2001;55(1):51–69.
- Glass N, Segal NA, Sluka KA, et al. Examining sex differences in knee pain: the multicenter osteoarthritis study. Osteoarthritis Cartilage. 2014;22(8):1100–1106.
- Hame SL, Alexander RA. Knee osteoarthritis in women. Curr Rev Musculoskelet Med. 2013;6(2):182–187.
- Hawker GA, Wright JG, Coyte PC, et al. Differences between men and women in the rate of use of hip and knee arthroplasty. N Engl J Med. 2000;342(14):1016–1022.
- Vårdanalys. Nationella kvalitetsregisters täckningsgrad: beskrivning, beräkning och bedömning. Report no.: 9789187213359. Stockholm: Myndigheten för vårdanalys; 2014.
- Socialstyrelsen. Nationella riktlinjer för rörelseorganens sjukdomar 2012: osteoporos, artros, inflammatorisk ryggsjukdom och ankyloserande spondylit, psoriasisartrit och reumatoid artrit: stöd för styrning och ledning. Stockholm: Socialstyrelsen; 2012.
- Olsson SJ, Ekblom O, Andersson E, et al. Categorical answer modes provide superior validity to open answers when asking for level of physical activity: a cross-sectional study. Scand J Public Health. 2016;44(1):70–76.
- EuroQol G. EuroQol – a new facility for the measurement of health-related quality of life. Health Policy (Amsterdam, Netherlands). 1990;16(3):199–208.
- Brooks R. EuroQol: the current state of play. Health Policy (Amsterdam, Netherlands). 1996;37(1):53–72.
- The EuroQol Group. EQ-5D-Y user guide. Basic information on how to use the EQ-5D-Y instrument. Version 1.0 ed. Rotterdam: The EuroQol Group; 2014.
- Fransen M, Edmonds J. Reliability and validity of the EuroQol in patients with osteoarthritis of the knee. Rheumatology (Oxford, England). 1999;38(9):807–813.
- Rolfson O, Bohm E, Franklin P, et al. Patient-reported outcome measures in arthroplasty registries. Report of the Patient-Reported Outcome Measures Working Group of the International Society of Arthroplasty Registries Part II. Recommendations for selection, administration, and analysis. Acta Orthop. 2016;87(Suppl. 1):9–23.
- Dolan P. Modeling valuations for EuroQol health states. Med Care. 1997;35(11):1095–1108.
- Burstrom K, Sun S, Gerdtham UG, et al. Swedish experience-based value sets for EQ-5D health states. Qual Life Res. 2014;23(2):431–442.
- Nemes S, Garellick G, Salomonsson R, et al. Crosswalk algorithms for the conversion of mean EQ-5D indices calculated with different value sets. Scand J Public Health. 2016;44(5):455–461.
- Dyer MT, Goldsmith KA, Sharples LS, et al. A review of health utilities using the EQ-5D in studies of cardiovascular disease. Health Qual Life Outcomes. 2010;8:13.
- Janssen MF, Lubetkin EI, Sekhobo JP, et al. The use of the EQ-5D preference-based health status measure in adults with type 2 diabetes mellitus. Diabetes Med. 2011;28(4):395–413.
- U.S. Department of Health and Human Services. 2008 physical activity guidelines for Americans: be active, healthy, and happy! Washington (DC): U.S. Department of Health and Human Services; 2008.
- Ernstgard A, PirouziFard M, Thorstensson CA. Health enhancing physical activity in patients with hip or knee osteoarthritis – an observational intervention study. BMC Musculoskelet Disord. 2017;18(1):42.
- Troiano RP, Berrigan D, Dodd KW, et al. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40(1):181–188.
- Campbell R, Evans M, Tucker M, et al. Why don't patients do their exercises? Understanding non-compliance with physiotherapy in patients with osteoarthritis of the knee. J Epidemiol Community Health. 2001;55(2):132–138.
- Petursdottir U, Arnadottir SA, Halldorsdottir S. Facilitators and barriers to exercising among people with osteoarthritis: a phenomenological study. Phys Ther. 2010;90(7):1014–1025.
- Loew L, Brosseau L, Kenny GP, et al. Factors influencing adherence among older people with osteoarthritis. Clin Rheumatol. 2016;35(9):2283–2291.
- Marks R. Knee osteoarthritis and exercise adherence: a review. Curr Aging Sci. 2012;5(1):72–83.
- Guthold R, Stevens GA, Riley LM, et al. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1.9 million participants. Lancet Glob Health. 2018;6(10):e1077–e1086.
- Althoff T, Sosič R, Hicks JL, et al. Large-scale physical activity data reveal worldwide activity inequality. Nature. 2017;547(7663):336–339.
- World Health Organisation. Sweden physical activity factsheet 2018. World Health Organisation; 2018 [cited 2020 Jan 2020]. Available from: http://www.euro.who.int/__data/assets/pdf_file/0010/382582/sweden-eng.pdf?ua=1
- Herbolsheimer F, Schaap LA, Edwards MH, et al. Physical activity patterns among older adults with and without knee osteoarthritis in six European countries. Arthritis Care Res (Hoboken). 2016;68(2):228–236.
- Dunlop DD, Song J, Lee J, et al. Physical activity minimum threshold predicting improved function in adults with lower-extremity symptoms. Arthritis Care Res (Hoboken). 2017;69(4):475–483.
- Coleman S, Briffa K, Conroy H, et al. Short and medium-term effects of an education self-management program for individuals with osteoarthritis of the knee, designed and delivered by health professionals: a quality assurance study. BMC Musculoskelet Disord. 2008;9:117.
- Wallis JA, Webster KE, Levinger P, et al. A pre-operative group rehabilitation programme provided limited benefit for people with severe hip and knee osteoarthritis. Disabil Rehabil. 2014;36(24):2085–2090.
- Hansson E, Hansson T, Jonsson R. Predictors for work ability and disability in men and women with low-back or neck problems. Eur Spine J. 2006;15(6):780–793.
- Forsbrand MH, Grahn B, Hill JC, et al. Can the STarT Back Tool predict health-related quality of life and work ability after an acute/subacute episode with back or neck pain? A psychometric validation study in primary care. BMJ Open. 2018;8(12):e021748.
- Gustafsson K, Kvist J, Eriksson M, et al. Socioeconomic status of patients in a Swedish national self-management program for osteoarthritis compared with the general population—a descriptive observational study. BMC Musculoskelet Disord. 2020;21(1):10.
- Burstrom K, Johannesson M, Diderichsen F. Swedish population health-related quality of life results using the EQ-5D. Qual Life Res. 2001;10(7):621–635.
- Cho HJ, Chang CB, Yoo JH, et al. Gender differences in the correlation between symptom and radiographic severity in patients with knee osteoarthritis. Clin Orthop Relat Res. 2010;468(7):1749–1758.
- Nelson AE, Smith MW, Golightly YM, et al. "Generalized osteoarthritis": a systematic review. Semin Arthritis Rheum. 2014;43(6):713–720.
- Tonelli SM, Rakel BA, Cooper NA, et al. Women with knee osteoarthritis have more pain and poorer function than men, but similar physical activity prior to total knee replacement. Biol Sex Differ. 2011;2:12.
- Katz JN, Wright EA, Guadagnoli E, et al. Differences between men and women undergoing major orthopedic surgery for degenerative arthritis. Arthritis Rheum. 1994;37(5):687–694.