
Abstract
Purpose
Disabilities are increasing globally, which is attributed to the overall ageing of populations in affluent countries. This trend may differ in low and middle-income countries. This paper assesses the change over time in Years Lived with Disability (YLD) for South Africa and how this compares to regional and global trends.
Materials and methods
This secondary analysis of the Global Burden of Disease Study 2017 dataset describes the observed contribution of YLD to Disability-Adjusted Life Years (DALYs) per 100 000 people over the period 1990–2016, and forecast to 2030 using simple linear prediction. South African trends are compared to global and sub-Saharan African (SSA) trends to highlight the effect of HIV and policy implications.
Results
Globally, the contribution of YLD to DALYs has increased from ±21.7% in 1990 to ±34% by 2016, with high socio-demographic index countries having a higher contribution (49%). HIV, mental health, musculoskeletal, neurological, and sense organ disorders are the five main contributors to YLD in South Africa (54%). Removing the effects of HIV/AIDS and sexually transmitted infections on YLD, South Africa’s trend appears similar to the global trend, yet opposite to the SSA trend.
Conclusion
Our analysis shows there is a growing burden of disability in South Africa. Differences in trends with the regional and global patterns can be attributed to the high burden of HIV and non-communicable diseases in South Africa. Therefore, strategies are urgently needed to increase integration of disability and rehabilitation services into chronic HIV and non-communicable disease management. This calls for disability screening to identify functional limitations in routine data collection and case management.
South Africa has experienced an increase in disability prevalence over time.
This requires strengthening of services such as mental health interventions, physiotherapy, optometry, and audiology, and linking major disease clusters, such as HIV and the NCDs, to rehabilitation services.
The greatest contributors towards disability adjusted life years in South Africa are currently mental disorders (13.8%), HIV and sexually transmitted infections (11.8%), musculoskeletal disorders (10.4%), neurological disorders (8.2%), and sense organ diseases (7.5%).
Routine data collection and case management needs to include disability screening to identify developing functional limitations.
IMPLICATIONS FOR REHABILITATION
Background
Global trends show that the impact of successful treatments for several previously life-threatening infectious diseases like HIV has increased survival into older ages [Citation1–6]. At the same time, the prevalence of Non-Communicable Diseases (NCDs) has increased, particularly in high socio-demographic index (SDI) countries [Citation2,Citation7]. While some people recover fully, others live long lives with conditions that limit their functioning in some way. As a result, there is an overall global increase in the prevalence of functional limitations and disability [Citation5,Citation7].
Previous research attributes the overall global trend of increasing disability predominately to the overall ageing of populations [Citation7,Citation8]. While this may be true for affluent countries (with high SDI), this may not be the case in countries with lower SDIs like South Africa, which still grapple with major epidemics such as HIV and TB. In fact, the impact of HIV is so profound in South Africa that the triple burden of disease seen in other countries has been expanded into a “quadruple burden of disease,” adding HIV as a specific burden of disease for the South African context [Citation9–12]. Currently, approximately 7.2 million of the 56.7 million people in South Africa are thought to be living with HIV, of which 61% access life-long ART [Citation13,Citation14]. The antiretroviral treatment (ART) program in South Africa has been hailed as a “treatment success,” given the large numbers of people who have access to treatment (over four million) and the subsequent improvement in the life expectancy of people living with HIV [Citation14,Citation15].
The introduction of ART in 2004 has transformed HIV from a deadly disease to a chronic disease in South Africa. Small pockets of emerging literature suggest that long-term, chronic HIV comes with a range of new health-related challenges [Citation16] that include functional limitations and disability, which may be experienced on an episodic, temporary, or permanent basis [Citation17–19]. Furthermore, HIV is not an illness related to ageing as it tends to affect predominantly younger populations (15–49 years). Thus, lifelong management of complex health conditions and functional limitations is a concern for individuals as well as health services. The increase in functional limitations/disability has been highlighted in the WHO “Rehabilitation 2030 Call for Action” [Citation20,Citation21], which calls to address the “unmet rehabilitation needs around the world especially in low- and middle-income countries” [Citation20]. However, low- and middle-income countries often lack data to inform the development of rehabilitation services. Therefore, the WHO “Guide for Action” identifies the need to conduct a country-specific situation analysis as a first step [Citation21]. The Global Burden of Disease (GBD) studies can be utilised to support such a country-specific situation analysis [Citation5].
Overview of the GBD studies
The GBD studies provide annual estimates, disaggregated by age and sex, of the global disease burden capturing data on premature deaths and disability for more than 300 diseases and injuries in 195 countries [Citation8]. The GBD studies cluster diseases into different “levels.” The top level is divided into three “broad causes” including: (A) Communicable, maternal, neonatal, and nutritional diseases; (B) Non-communicable diseases; and (C) Injuries. These broad causes are then further broken up into a second level of “22 disease clusters” (e.g., cardiovascular diseases, diabetes and kidney diseases), a third level of “169 diseases” (e.g., stroke, diabetes mellitus, etc.), and fourth level causes of 293 diseases and disease subtypes (e.g., ischemic stroke, diabetes mellitus type 1, etc.).
The data from the GBD studies can also be used to compute indicators such as Years of Life Lost (YLL) and Years Lived with Disability (YLD) for a diverse set of diseases. YLLs and YLDs are then used to determine Disability-Adjusted Life Years (DALYs), an indicator that can be thought of as one lost year of “healthy life without functional limitations” [Citation8]. In order to calculate YLD, the GBD study uses specific disability weights per health condition (as different health conditions cause different severities of disablement). The disability weights have been developed by the GBD study team who allocated numerical weights estimating the non-fatal consequences of health conditions (from 0, perfect health, to 1, equivalent to dead) [Citation5,Citation22,Citation23]. The full methodology and weighting procedure has been discussed in other published articles [Citation22,Citation23]. The general methods used in the GBD studies are described in detail elsewhere [Citation3,Citation5,Citation7].
Previous research utilising the GBD studies
Public health research and interventions focusing on disease prevention and treatment, measure success through a decrease in the incidence of YLL due to premature death and an increase in healthy life expectancy (HALE). The impact of YLD is seldom considered. GBD papers that focus on YLD often fail to discuss what the increase in the rate of YLD means for health systems [Citation3,Citation7]. Hence, globally less attention is paid to the experience of disability that accompanies longer life expectancy. The shift from YLL to YLD is also different across socioeconomic settings. The Lancet GBD series reports that the gap between healthy life expectancy and overall life expectancy is proportionately smaller in countries with high socio-demographic index (SDI) than in countries with lower SDI [Citation1,Citation7,Citation8]. This means that while functional limitations and disability are increasing worldwide, people from countries with lower SDI spend a greater proportion of their life living with disability than those in countries with high SDIs. With regard to South Africa, the country-specific situation analysis of the national cause of death report does not discuss trends of YLD at all [Citation10]. The report followed the Global Burden of Disease Study 2015 approach to identify specific causes of death and identified HIV/AIDS as the single largest contributor (35.7%) to premature mortality measured using the YLL indicator, with cerebrovascular diseases a distant second at 4.8% [Citation10]. To our knowledge there is no nationally robust trend analysis of data on years lived with disability in South Africa, and what this means for the country’s health and social systems [Citation7].
Therefore, it is necessary to investigate how YLD have changed in the last 20 years alongside large-scale public health interventions such as the ART rollout in South Africa. In countries like South Africa, an impactful epidemic like HIV occurring alongside a predictable wave of non-communicable diseases may not only shift the general burden of disease, but also the portion of that burden that is attributable to years lived with disability (functional limitation). Therefore, this paper uses the GBD 2017 dataset, to examine the trend in YLL [Citation24] and extrapolates YLD to the year 2030 to show the potential future trends and discuss the policy implications of a growing burden of disability in the not-too-distant future. We further explore how YLD have changed in South Africa over the period 1990–2016 alongside the large-scale treatment of major diseases such as HIV. We are particularly interested in the South African case, as this is a country at the epicentre of the global HIV epidemic and also has a rapidly ageing population unlike most low- and middle-income countries in the region [Citation25].
Methods
Study design
For the purpose of this paper we conducted a secondary analysis of the GBD 2017 study dataset, exploring the change over time of YLD during the period of the “HIV treatment success” for major diseases (e.g., HIV, TB, measles, malaria, maternal health), in South Africa and globally. We used the global, regional, and South African data to conduct a retrospective analysis to assess change in YLD over time and extended into the future. In order to do so, we accessed the GBD 2017 study data via the Global Health Data Exchange portal (http://ghdx.healthdata.org/gbd-results-tool). The paper makes use of the annual data from 1990 to 2016 for DALYs, YLL, and YLD in South Africa, Sub-Saharan Africa, high SDI countries, and the world. We used existing forecasts for YLL [Citation24] and a simple prediction model for YLD to examine the GBD trends for the period 2017 − 2030. We included all available data with no restriction on gender or age.
Statistical analysis
Our analysis makes use of the GBD’s first two levels of causes (broad causes and disease clusters) to examine trends in health over time and the contribution of YLD towards the global burden of disease, focusing on the global, regional, and South African rates of DALYs, YLL, and YLD per 100 000 people. This paper is primarily a descriptive analysis looking at the trends over time revealed by the GBD Study. The analysis presented in the figures made use of the full range of the GBD data, while the analysis covered in the tables only covered the latest data from 2016.
While the tables and most of the figures are purely descriptive, and required additional analyses. makes use of existing GBD study forecasts for YLL up to 2030. As recent forecasts could not be found for YLD and the fact that they increase linearly over time, a simple linear prediction (YLDYear = β×(Year − 1990) + intercept; where, β = 28.76, intercept = 10 316.31, derived from regression of YLD on time) was used to generate similar values for YLD using only past values of YLD to forecast it. To provide further insight into , a detrended regression analysis was used to calculate the explained variance in total YLD due to HIV. A detrended regression was used to avoid the spurious regression problem and artificially high R-squareds, as both YLD and YLD due to HIV have an increasing trend. Thus, we first regressed YLD on time and then regressed the residuals of this model on YLD due to HIV and time.
Figure 1. Composition of Global DALYs.
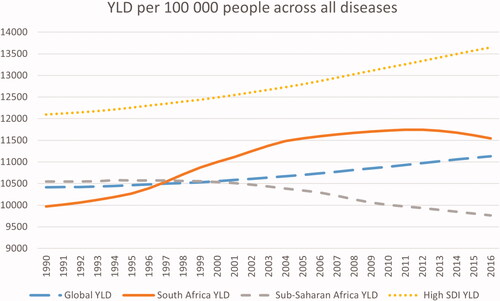
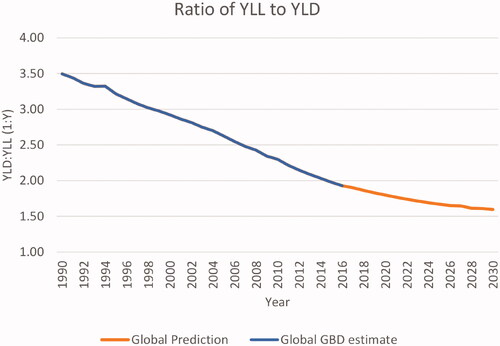
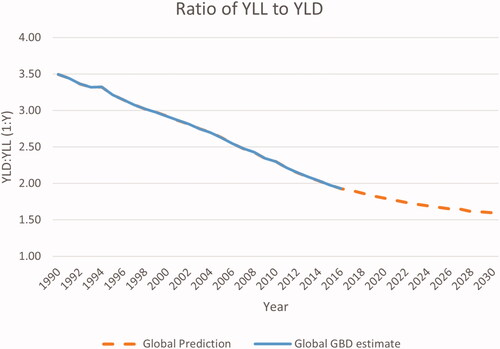
Figure 2. Ratio of YLL to YLD.
Results
There has been a sustained increase in the contribution of YLD to the composition of DALYs from around 22% in 1990 to just under 34% in 2016 (). Between 1990 and 2016, the contribution of YLD to DALYs increased by approximately twelve percent globally (). If the current trends continue, then the proportion of YLD per DALY will continue to rise ().
Figure 3. YLD per 100 000 people for all diseases over time and in different regions.
The data from the GBD study also allows us to further look at the trends in YLD in relation to different diseases, geographical locations, and socioeconomic settings. The trends in the three GBD study broad causes of diseases are shown in , disaggregated by region and includes a comparison to countries scoring high on the SDI.
Table 1. Broad causes of disease across regions (GBD 2016).
The distribution of disease burden across these broad causes differs between each region (). While South Africa and sub-Saharan African (SSA) are most heavily affected by the cluster of communicable, maternal, neonatal, and nutritional diseases (cause A), high SDI countries and the world as a whole are more heavily affected by the cluster of non-communicable diseases (cause B). Looking at the proportion of the DALY’s attributable to YLD, we see that the cluster of cause B for high SDI countries (50%) has a reasonably similar proportion of YLD to YLL as in South Africa (48%) and to a lesser extent globally (44%) and in the SSA region (42%).
In contrast, there is a distinct difference in the composition of broad causes A and C across regions. In SSA, which includes lower and some middle SDI countries, the burden of disease within causes A and C is primarily composed of YLL, 91% and 84% respectively; compared to approximately 54% and 56% in the high SDI countries (with YLD taking a much more significant portion). South Africa has an overall higher portion of YLD per DALY (25%) when compared to other SSA countries (19%), but is still far below high SDI countries (49%). To better understand the causes and scope of YLD in South Africa and predict future development, we have taken a closer look at the leading health concerns in the country today.
Each of the “broad causes” can be further subdivided into level 2 groups to better understand the underlying diseases driving these causes. illustrates the distribution of DALYs, YLD, and YLL in the level 2 sub-groups of clusters A and B for South Africa in 2016.
Table 2. Level 2 causes of disease from cluster A and B for South Africa (GBD 2016).
HIV and other sexually transmitted infections (STIs) are the highest contributors to South Africa’s DALYS (16 480 DALYs [UI 14 562–18 763], ). Overall, HIV/STIs, respiratory infections, cardiovascular diseases, neoplasms, and maternal and neonatal disorders are the five highest contributors to YLL in South Africa (). Of these five, only HIV/STIs is amongst the top five highest contributors to YLD. The remaining contributors to YLD include mental health, musculoskeletal, neurological, and sense organ disorders (5959 out of 10 950 YLD or 54%).
Furthermore, the GBD study can be used to analyse how regions and countries experience different burdens and changes over time, both in terms of diseases causing premature death and disabling conditions. Such an analysis shows that while in 1990 YLD were a smaller part of the global health burden, ±21.7% (: ±10 000 YLD vs ±37 000 YLL), YLDs contributed to a much higher portion of the burden in 2016, 33.6% (±11 000 YLD vs ±22 000 YLL).
The GBD study data also allows us to illustrate longitudinal regional differences of YLD (). The data reveals that the rates of YLD per 100 000 people globally and in High SDI countries has been increasing over time. Conversely, SSA has been gradually decreasing over time since around 1997. In South Africa, the YLDs have been on an upward trajectory since the 1990s, increasing more rapidly between 1997 and 2005, then levelling off with a slight decline in years lived with disability from 2012 onwards. In addition, the rates of YLDs in South Africa are higher than the rate in SSA and globally since 1997 but are still lower than in the high SDI countries ().
Figure 4. YLD per 100 000 people excluding HIV.
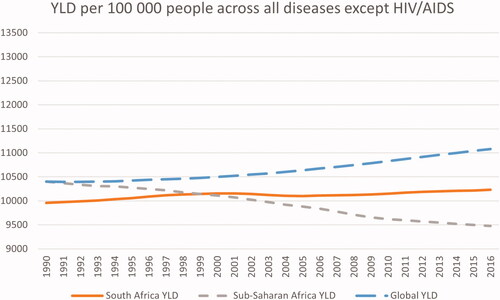
A detrended regression of YLD due to HIV on total YLD accounts for 97.7% of the variance in total YLD over this period. shows the trend in YLD in South Africa without the effects of HIV and AIDS. It reveals that after removing the direct effects of HIV and AIDS on YLD in South Africa, we see a trend over time that is quite similar to that of the global rates of YLD, with YLD changing only marginally in an upward trend in the later 90 s and again between 2005 and 2016.
Discussion
Our article provides a broad country-level analysis of the GBD data that helps to illumine the growing burden of disability in South Africa. It adds further insight to the GBD 2017 report [Citation5] that showed an increase globally in the total YLD despite a 3.9% decline in the age-standardised YLD rate. Our study shows that, globally, YLDs increased in their percentage contribution towards the burden of disease and that the rate of YLD accelerated in South Africa from around 1997 onwards. The analysis also revealed that the rapid increase in South Africa’s YLDs is different from the general regional trend in SSA. The analysis suggested that this can be attributed to a high burden of chronic HIV as well as an increase of non-communicable diseases, that affect the mental, sensory, neurological and musculoskeletal functioning of people.
South Africa is currently managing the highest number of people living with HIV in the world [Citation26], and HIV itself is a key contributor to the accelerated increase of YLDs over the last 20 years. The disabling weights for HIV are not as strong as for NCDs. Hence, they may be more subtle impairments and less noticeable, and therefore need careful monitoring and identification in the continuum of HIV care. Mental health, sensory, musculoskeletal, and neurological disorders have much greater disability weighting. However, these NCDs have received little attention over the last few decades, presumably because they are not significant contributors to YLL. The combination of chronic HIV, together with the increasing prevalence of disability through NCDs, an ageing population and long-term effects of new health emergencies such as COVID-19, create the need to increase screening and treatment for functional limitations/disability in South Africa.
Furthermore, the analysis shows that disability is a cross-cutting issue. Considering the rising proportion of YLD, disability should be a priority area in health research globally. This is especially true in high SDI countries where the proportion of DALY’s due to YLD is almost 50%. However, this issue is no less pressing in lower SDI countries such as South Africa, where YLDs already account for 26% of the total DALYs. We can see from that, due to the rapid rise in rates of YLDs since 1997, South Africa now has a higher burden of YLDs than the global average. Furthermore, we can see from the results here that South Africa’s burden of disease is already significantly shaped by the impact of YLDs, as shown in . Overall, YLDs contribute to 26% of South Africa’s DALYs, which is more than triple the health burden of any level 2 cause other than HIV and STIs. Hence, interventions focusing on reducing or mitigating functional limitations in South Africa through better identification of functional limitation, linkage to care, and provision of rehabilitation and wellness programmes have great potential for improving the population’s health and wellbeing.
Furthermore, from , we see that the global contribution of YLD to DALYs is increasing rapidly and may one day equal that of YLL. Our findings on YLD show that initially in the early 1990s YLD was lower in South Africa than the rest of SSA and globally, but then rapidly increased before levelling off from around 2012. Hence, the upward trend in YLD has been accelerated in South Africa in the last two decades. Globally as well as in South Africa, we live in a period where the need for and potential impact of efficient rehabilitation, disability, and wellness programmes is increasing dramatically.
Unlocking the potential reach of rehabilitation and disability services is thus equally as crucial as more conventional health priorities focusing on disease treatment and prevention [Citation27–32]. This is especially important when one considers the relative paucity of research, both in understanding the causes and prevalence of disability and in developing social and rehabilitation interventions, that enable high quality of life with disability in countries like South Africa [Citation33]. Therefore, integrating disability and functional limitation data collection into public health research needs to become routine practice, both through integration into mainstream health programmes and research and through the provision of specialised programmes. Mainstreaming of disability data collection does not only apply to the GBD study but also key health programmes, such as the South African ART or tuberculosis program; the provision of primary healthcare services; and national data collection through mechanisms such as the Demographic Health Survey. Disability data collection and monitoring will also be important for management of new diseases such as COVID-19, a health emergency which emerged as a pandemic after this paper was drafted. Disability inclusion in health emergencies is important in order to understand whether people with disabilities are more at risk of infection with new emerging diseases such as COVID-19 but also if these new diseases cause any long-term health effect that need rehabilitation [Citation34–36].
Research on disability, mental health, and rehabilitation programmes and services in South Africa and the SSA region is scarce [Citation33]. Emerging evidence in key priority areas such as HIV provides some data on the increased prevalence of functional limitations in populations living with HIV [Citation17,Citation18,Citation37–39]. The available evidence suggests that functional limitations due to the top contributors towards YLD in South Africa can be addressed through utilising technological innovations, disability networks, and feasible service delivery models [Citation39–43]. Some of the approaches have been piloted and evaluated, such as: App-based tools for better identification and diagnosis [Citation38,Citation42,Citation43], personalised exercise programmes [Citation40], community-based or home-based rehabilitation [Citation39], and task shifting in mental health interventions [Citation42]. Some of these innovations make use of new technology (e.g., screening applications) and can be implemented by lay healthcare workers [Citation39,Citation43,Citation44]. These innovations need to be further evaluated and implemented with a strategic approach that enhances linkage to care. Chetty’s work, for instance, describes how rehabilitation innovations can be integrated into long-term care for diseases such as HIV [Citation45]. Hence, the emerging literature already provides us with evidence on innovations that can be further explored with regards to their effectiveness and scalability to address the growing functional limitations and disability.
In South Africa, the need to address disability and integrate mental health and rehabilitation services into disease management of chronic HIV and NCD care has been recognised to some extent. For instance, both the South African National Strategic Plan on HIV, TB, and STIs 2017–2022 and the 2015 Framework and Strategy on Disability and Rehabilitation Services identify the need to integrate these services. However, within the broader response to key health priority areas such as HIV, which is often driven by donor funding and medicalised health priority setting, the need for strengthening, integrating, and funding mental health and rehabilitation research and interventions is often forgotten. A similar trend has been described by rehabilitation researchers for the COVID epidemic [Citation36]. These researchers criticise the current response which focuses on emergency medical help and development of vaccines, while not paying sufficient attention to the rising mental health and rehabilitation needs of the survivors of COVID and the population at large, who experienced social isolation, uncertainty, and unrest [Citation36].
Limitations
The GBD study produces estimates for YLL and YLD, and the accuracy of these estimates has been questioned. However, it is currently the best dataset available to understand and compare the burden of diseases across countries and regions. Our study can only access the existing estimates and cannot access the original population-based data that informed the calculation of these estimates.
The process of analysing the GBD study using a disability focus also highlights some fundamental limitations relating to the GBD datasets. One such limitation pertains to the years lived with disability which is dependent on disability weights applied to disease and mortality data that is usually obtained from population-based and online surveys with the majority of the respondents from high SDI countries [Citation5,Citation7,Citation46]. It is therefore not surprising that in the GBD data’s disability weights tend to be higher for conditions such as back pain, headaches, and depressive disorders [Citation5]. As shown by results from a study conducted on a small community in South Africa, there is usually a low correlation between the global burden of disease and local disease burden disability weights [Citation47]. However, studies such as that by Neethling et al. are not large enough to significantly influence and alter the GBD disability weights, and more work is needed to adjust weights appropriately to local contexts [Citation47]. Therefore, there remains a dearth of national empirical population-level data on disease and injury sequelae for South Africa to inform an accurate weighting for and duration of disability when calculating YLD. Hence, when analysing the South African data, GBD estimates are primarily based on disease and sequelae estimates taken from regional data. There is an urgent need for investment in the generation of local disease and injury data to improve the localisation of GBD estimates.
Conclusion
The GBD study data can be used to illustrate the increasing need to address YLD in the management of the global and South African disease burden. The available evidence indicates that the functional limitations experienced by people living with chronic conditions, including HIV and NCDs, are already accelerating in South Africa. Pilot projects provide some innovative ideas on how to identify functional limitations better and provide access to rehabilitation interventions in South Africa. However, in order to understand how best to provide and integrate rehabilitation services in a manner that is feasible and easy to scale up is a matter that needs more research. Such research needs to provide better data on causes of disability, the severity of disability per disease, and potential rehabilitation interventions including early diagnosis, treatment, and support.
Contribution
JHH and BC conceptualised the study together. JHH has written the first and final draft of the paper. BC has conducted the statistical analysis and written parts of the first and final draft. MN has contributed to the analysis and written parts of the paper.
Acknowledgements
We would like to thank the GBD team for making this data publicly available.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- GBD 2016. DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 333 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2016: a systematic analysis for the global burden of disease study 2016. The Lancet. 2017;390(10100):1260–1344.
- GBD 2016. Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the global burden of disease study 2016. The Lancet. 2017;390(10100):1151–1210.
- GBD 2017. Mortality Collaborators. Global, regional, and national age-sex-specific mortality and life expectancy, 1950–2017: a systematic analysis for the global burden of disease study 2017. The Lancet. 2018;392(10159):1684–1735.
- GBD 2017. Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the global burden of disease study 2017. The Lancet. 2018;392(10159):1736–1788.
- GBD 2017. Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. The Lancet. 2018;392(10159):1789–1858.
- Deeks SG, Lewin SR, Havlir DV. The end of AIDS: HIV infection as a chronic disease. The Lancet. 2013;382(9903):1525–1533.
- GBD 2017. DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. The Lancet. 2018;392(10159):1859–1922.
- The L. Life, death, and disability in 2016. Lancet. 2017;390(10100):1083.
- Econex. South Africa’s burden of disease. Pretoria: Econex; 2009.
- Pillay-van Wyk V, Msemburi W, Laubscher R, et al. Mortality trends and differentials in South Africa from 1997 to 2012: second national burden of disease study. Lancet Glob Health. 2016;4(9):e642-53–e653.
- Nojilana B, Bradshaw D, Pillay-van Wyk V, et al. Emerging trends in non-communicable disease mortality in South Africa, 1997–2010 [non-communicable diseases; mortality rates; South Africa; national burden of disease study. S Afr Med J. 2016;106(5):58.
- Mayosi BM, Flisher AJ, Lalloo UG, et al. The burden of non-communicable diseases in South Africa. Lancet. 2009;374(9693):934–947.
- World Bank. "Antiretroviral therapy coverage (% of people living with HIV)" World development indicators. The World Bank Group; 2017.
- UNAIDS. UNAIDS data 2018. Genva: UNAIDS; 2018.
- Bor J, Herbst AJ, Newell ML, et al. Increases in adult life expectancy in rural South Africa: valuing the scale-up of HIV treatment. Science. 2013;339(6122):961–965.
- Mayosi BM, Benatar SR. Health and health care in South Africa-20 years after Mandela. N Engl J Med. 2014;371(14):1344–1353.
- Hanass-Hancock J, Myezwa H, Carpenter B. Disability and living with HIV: baseline from a cohort of people on long term ART in South Africa. PLoS One. 2015;10(12):e0143936.
- Banks LM, Zuurmond M, Ferrand R, et al. The relationship between HIV and prevalence of disabilities in sub-Saharan Africa: systematic review (FA). Trop Med Int Health. 2015;20(4):411–429.
- Nixon SA, Hanass-Hancock J, Whiteside A, et al. The increasing chronicity of HIV in Sub-Saharan africa: Re-thinking “HIV as a long-wave event” in the era of widespread access to ART. Global Health. 2011;7:41.
- World Health Organization. Rehabilitation 2030: a call for action. Meeting report. Geneva: WHO; 2017.
- World Health Organization. Rehabilitation in health systems: guide for action. Geneva: WHO; 2019.
- Haagsma JA, Maertens de Noordhout C, Polinder S, et al. Assessing disability weights based on the responses of 30 660 people from four European countries. Popul Health Metr. 2015;13:10.
- Salomon JA, Haagsma JA, Davis A, et al. Disability weights for the global burden of disease 2013 study. Lancet Glob Health. 2015;3(11):e712–e723.
- Institute for Health Metrics and Evaluation. GBD foresight visualization. Seattle (WA): IHME, University of Washington; 2018.
- Shetty P. Grey matter: ageing in developing countries. Lancet. 2012;379(9823):1285–1287.
- Henry J Kaiser Family Foundation. The Global HIV/AIDS Epidemic. San Francisco (USA): Henry J Kaiser Family Foundation; 2019.
- University of Toronto Department of Physiotherapy. E-Module on HIV for Rehabiliation Providers in Sub-Saharan Africa Toronto: UoT; 2015 [cited 2021 Oct 29]. Available from: http://www.physicaltherapy.utoronto.ca/research/icdr-lab/e-module-on-hiv-for-rehabilitation-providers-in-sub-saharan-africa/
- World Health Organization. Disability and rehabilitation action plan 2006–2011. Geneva: WHO; 2006.
- World Health Organization. Community-based rehabilitation: CBR guidelines. Towards community-based inclusive development. Malta: WHO; 2010.
- World Health Organization. Draft WHO global disability action plan 2014–2021: Better health for all people with disability. Geneva: World Health Organization; 2014.
- World Health Organization. Disability and health. Key facts. Geneva: WHO; 2018 [cited 2021 Aug 31]. Available from: https://www.who.int/news-room/fact-sheets/detail/disability-and-health
- World Health Organization, World Bank. World disability report. Malta: WHO; 2011.
- Nixon S, Forman L, Hanass-Hancock J, et al. Rehabilitation: a crucial component in the future of HIV care and support. South Afr J Hiv Med. 2011;12(2):12–16.
- COVID-19 Disability Rights Monitor, Siobhan Brennan C. Disability rights during the pandemic. A global report on findings of the COVID-19 disability rights monitor. unknown: Validity, ENIL, IDA, DRI, CfHR, IDDC, DRF; 2020.
- Policy brief. Taking a disability-inclusive approach to pandemic responses. [Internet]. Brighton: IDS; 2021.
- Brown DA, O’Brien KK, Josh J, et al. Six lessons for COVID-19 rehabilitation from HIV rehabilitation. Phys Ther. 2020;100(11):1906–1909.
- Myezwa H, Buchalla CM, Jelsma J, et al. HIV/AIDS: use of the ICF in Brazil and South Africa-comparative data from four cross-sectional studies. Physiotherapy. 2011;97(1):17–25.
- Devendra A, Makawa A, Kazembe PN, et al. HIV and childhood disability: a case-controlled study at a paediatric antiretroviral therapy Centre in Lilongwe, Malawi. PLoS One. 2013;8(12):e84024.
- Cobbing S, Hanass-Hancock J, Myezwa H. A home-based rehabilitation intervention for adults living with HIV: a randomized controlled trial. J Assoc Nurses AIDS Care. 2017;28(1):105–117.
- Roos R, Myezwa H, van Aswegen H, et al. Effects of an education and home-based pedometer walking program on ischemic heart disease risk factors in people infected with HIV: a randomized trial. J Acquir Immune Defic Syndr. 2014;67(3):268–276.
- Chetty V, Hanass-Hancock J, Myezwa M. A model of care for the rehabilitation of people living with HIV in a semi-rural South African setting. South African Health Review. 2015;2014/2015:183–194.
- Petersen I, Hanass Hancock J, Bhana A, et al. A group-based counselling intervention for depression comorbid with HIV/AIDS using a task shifting approach in South Africa: a randomized controlled pilot study. J Affect Disord. 2014;158:78–84.
- Louw C, Swanepoel W, Eikelboom RH, et al. Smartphone-based hearing screening at primary health care clinics. Ear Hear. 2017;38(2):e93–e100.
- Alli F, Hanass-Hancock J, Cobbing S, et al. Closing the gap: building capacity to address the relationship between disability and HIV. Durban: HEARD; 2012.
- Chetty V, Hanass-Hancock J. The need for a rehabilitation model to address the disparities of public healthcare for people living with HIV in South Africa. Afr J Disabil. 2015;4(1):137.
- Murray CJ, Vos T, Lozano R, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2197–2223.
- Neethling I, Jelsma J, Ramma L, et al. Disability weights from a household survey in a low socio-economic setting: how does it compare to the global burden of disease 2010 study? Glob Health Action. 2016;9(1):31754.