
Abstract
Purpose
To assess the measurement properties of EQ-5D-3L and EQ-5D-5L in patients with a major lower limb amputation (LLA).
Methods
This was a retrospective register-based study using data from the Swedish Amputation and Prosthetics Registry (SwedeAmp). Patients with a six-months follow-up (including either EQ-5D-3L or EQ-5D-5L) after a major unilateral LLA were included. The measurement properties of EQ-5D-3L and EQ-5D-5L were compared in terms of feasibility, response patterns, informativity, and convergent and known-group validity.
Results
The sample included 700 patients with below-knee amputation (76%), above-knee amputation (18%), or knee disarticulation (7%). Responses to EQ-5D-3L and −5L were similar regarding feasibility (98% completion rate) and the proportion reporting no problems (7% and 6%). Compared to EQ-5D-3L, EQ-5D-5L showed higher absolute and relative informativity in all dimensions, with the largest improvement in the mobility dimension. In the analyses of convergent validity, the EQ-5D-5L generally showed stronger correlations with disease-specific measures. Only EQ-5D-5L was able to discriminate between subgroups with different amputation levels.
Conclusion
The findings support the use of EQ-5D-5L over EQ-5D-3L in patients with an LLA, mainly due to improved informativity and improved convergent and known-group validity.
The measurement properties of two EQ-5D versions, EQ-5D-3L and EQ-5D-5L, has so far not been evaluated in patients with a lower limb amputation (LLA)
The results support the use of EQ-5D-5L over the use of EQ-5D-3L, mainly due to improved informativity and stronger correlations with disease-specific patient-reported outcome measures
The five-level version of EQ-5D is recommended for future applications of EQ-5D in clinical outcome studies, health economic evaluations, and in the routine follow-up of patients with a major LLA
In the early rehabilitation process six months after an LLA, the majority of patients reported problems with mobility, pain/discomfort, and usual activities
Implications for rehabilitation
Introduction
A lower limb amputation (LLA) is most commonly conducted due to peripheral vascular diseases including diabetes and atherosclerosis [Citation1,Citation2]. Other underlying diagnoses include e.g., trauma, tumor, or infection [Citation3]. The incidence of major LLA (i.e., amputation above the ankle) varies globally, with estimates ranging from 3.6 to 68.4 per 100 000 individuals in the general population [Citation4]. Rehabilitation is focused on restoring mobility with a prosthesis, which has been identified as the primary factor influencing the quality of life after LLA [Citation1,Citation2,Citation5]. A higher amputation level has been associated with worse outcomes, both in terms of post-operative mortality [Citation6] and mobility [Citation7,Citation8]. Furthermore, health outcomes after an LLA have also been observed to vary by sex, age, underlying diagnosis, and comorbidity [Citation1,Citation9,Citation10].
Patient-reported outcome measures (PROMs) are used to measure outcomes such as self-reported health status, symptoms, or health-related quality of life (HRQoL), from the patient perspective [Citation11]. An example of a commonly used PROM is EQ-5D [Citation12,Citation13]. The EQ-5D can be used to assess HRQoL in different populations, to evaluate interventions in terms of health effects and cost-effectiveness, and, more recently, to compare health care performance [Citation14,Citation15]. Previous literature reviews found that a variety of PROMs have been used to assess HRQoL in patients with LLAs, but only a limited number of studies included EQ-5D [Citation1,Citation2]. Although studies presenting the distribution of responses by EQ-5D health dimensions are rare, results from two studies indicate that problems after LLA mainly concern mobility, pain/discomfort, and usual activities [Citation10,Citation16]. Other studies exploring the relationship between different clinical events and the EQ-5D index have included patients with amputations only as a subgroup of 14–80 patients and provided limited information about the characteristics of the population [Citation17–22].
Currently, there are two EQ-5D versions for adults. With an extended number of severity levels on each dimension (five instead of three), the EQ-5D-5L was developed to increase the sensitivity of the health classification system [Citation13,Citation15]. In addition to the increased number of severity levels, minor changes were made to the descriptive system. For example, the level describing extreme problems with mobility was changed from “confined to bed” in EQ-5D-3L to “unable to walk about” in EQ-5D-5L [Citation13].
The original EQ-5D-3L is still commonly used in research and in clinical registries with continuous data collection [Citation15,Citation23], and it could be argued that a change from EQ-5D-3L to EQ-5D-5L could impede comparability of results over time. Further, even though the extended number of severity levels in EQ-5D-5L was expected to contribute to improved sensitivity, the added response levels could also, at least in theory, be left unused by the respondents or lead to misclassifications if not interpreted as intended. Therefore, any recommendation for using either version should be motivated by studies showing its benefits in terms of better measurement properties in a specified patient population.
Comparative studies of the measurement properties have generally presented favorable results for the 5-level version [Citation24,Citation25]. For example, studies have shown improved results for EQ-5D-5L in terms of distributional characteristics, such as reduced ceilings (i.e., the proportion reporting no problems in all dimensions) [Citation26–33], and the informativity captured by the descriptive system [Citation30–34]. However, to our knowledge, no study has yet evaluated the measurement properties of the two EQ-5D versions in patients with an LLA. The mobility dimension in EQ-5D is of particular interest, both due to the fact that mobility is an important outcome after LLA and due to the changes made to the EQ-5D descriptive system.
The objective of the current study was to assess the measurement properties of EQ-5D-3L and EQ-5D-5L in patients with a major LLA by comparatively examining the instruments in terms of feasibility, distributional characteristics, and validity.
Methods
Study design and data
This study was a retrospective register-based study. Data were extracted from the Amputation and Prosthetics Registry (SwedeAmp), a Swedish national registry for amputation of the lower extremities [Citation3]. In SwedeAmp, individual-level data is collected to enable objective assessment of LLAs and the consequences in the complete health care pathway up to 24 months after surgery. As of the end of 2018, the registry contained 5762 patients and approximately 2000 follow-up registrations (at 6, 12, or 24 months) [Citation3]. Data are voluntarily collected in routine health care settings, including surgical units, prosthetic workshops, and rehabilitation units. The PROMs included in the registry are primarily administered and registered at the rehabilitation units, implying that patients involved in prosthetic rehabilitation are the predominant population for whom self-reported health outcome data are available. The EQ-5D-3L (descriptive system) was administered from 2011 to 2016. In 2017, the registry changed the EQ-5D version and started collecting data on the EQ-5D-5L (descriptive system and EQ VAS). As data on EQ-5D-3L and EQ-5D-5L were collected during two separate time periods, the study population consisted of two subsamples, i.e., subsample EQ-5D-3L and subsample EQ-5D-5L.
Study population
The criteria for being included in the study sample were to have had: a unilateral major amputation including transtibial amputation (TTA), transfemoral amputation (TFA), or knee disarticulation (KD); primary amputation or re-amputation as surgical procedure; a follow-up assessment at six months after surgery including an EQ-5D-3L or EQ-5D-5L registration. The exclusion criteria were to have had a bilateral major amputation, or amputation at the hip or pelvic level. Patients who met the eligibility criteria but had missing information regarding sex and/or age (n = 15) were excluded as this information was used to compare the two subsamples.
PROMs
EQ-5D
EQ-5D consists of a descriptive system and a visual analogue scale (EQ VAS) [Citation12,Citation13]. The descriptive system contains five items that each represent a health dimension, including mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. In each dimension, the EQ-5D-3L has three severity levels (no, some, extreme problems/unable), and the EQ-5D-5L has five severity levels (no, slight, moderate, severe, extreme problems/unable). The EQ VAS ranges from 0 (worst health you can imagine) to 100 (best health you can imagine). In this study, Swedish versions of the EQ-5D questionnaires were used. The Swedish version of EQ-5D-3L was constructed during the multilingual development of the original questionnaire, and more recent language versions (e.g., for EQ-5D-5L) have been developed through a formal translation process [Citation15].
Responses to EQ-5D can be presented in several ways. The EQ-5D health profile is a 5-digit number that describes the severity levels on each item (e.g., 11 111 represents no problem in all five dimensions). The EQ-5D level sum score is the unweighted sum of the five digits in each profile and has a possible range of 5–15 for EQ-5D-3L and 5–25 for EQ-5D-5L. Each health profile can be converted into an EQ-5D index value with the use of a country-specific value set. In the development of value sets, stated preferences regarding different dimensions and severity levels are elicited through different health-state valuation methods and are typically obtained from a general population sample [Citation35]. The EQ-5D-3L index values were derived from a value set from the UK [Citation36] and the EQ-5D-5L index values from a cross-walk value set for the UK [Citation37]. The EQ-5D index values range from −0.594 to 1 (“full health”) in both value sets.
Other patient-reported outcomes
The Locomotor Capabilities Index (LCI-5) measures the self-reported capability to perform locomotor activities when wearing a prosthesis [Citation38] and is widely used in patients with LLA. The LCI-5 consists of 14 items that are graded on a 5-point ordinal scale from 0 (not able to) to 4 (yes, alone, without ambulation aids). The two subscales represent basic capabilities (7 items) and advanced capabilities (7 items), and both range from 0 (worst) to 28 (best). Thus, the total score ranges from 0 (worst) to 56 (best). Examples of basic abilities include getting up from a chair and walking indoors. Examples of advanced abilities include going up a few steps (stairs) without a handrail and walking while carrying an object.
The Prosthetic Use Score assesses the extent of normal prosthetic wear per week [Citation39] and is calculated by multiplying the number of days/week (0–7) by the number of hours/day the prosthesis is worn (categorized into six response options). The score takes a value between 0 (no use) and 100 (each day more than 15 hours).
Other patient-reported outcomes included a single question addressing the patient’s overall situation as an amputee (very good; good; neither good nor bad; bad; very bad) and two questions addressing the occurrence of phantom limb pain and residual limb pain during the last three months.
Data analysis
Statistical comparison between subsamples
The comparability of the subsamples was assessed by comparing the respondent characteristics in terms of sex, age at amputation, underlying diagnosis leading to the amputation, and amputation level. Potential statistically significant differences were tested using the chi-square test (nominal categorical variables), Mann-Whitney U test (ordinal categorical variables), and independent t-test (continuous variables), at a significance level of 0.05. In a second step, the other health outcomes were presented for the two subsamples separately, and any differences between the subsamples were analyzed using the Mann-Whitney U test.
Feasibility
The feasibility of EQ-5D-3L and EQ-5D-5L was assessed by comparing the proportions of missing data overall (using a registry variable for those who were asked, but did not respond, to EQ-5D) and internal missing by dimension. We hypothesized to observe a smaller proportion of missing data in the EQ-5D-5L responses compared to EQ-5D-3L.
Distributional characteristics
All patients with complete responses on the EQ-5D descriptive system were included in the description of HRQoL. Responses to the EQ-5D descriptive system were presented using frequencies (n) and percentages (%). EQ-5D index values and EQ VAS scores were presented using mean and standard deviation (SD) or median and interquartile range (IQR).
Analysis of the distributional characteristics included assessments of response patterns and informativity. Response patterns were compared by examining responses on each health dimension, the proportion of patients reporting no problems, and the number of unique health profiles on EQ-5D-3L and EQ-5D-5L. We hypothesized that a relatively smaller proportion would report no problems on EQ-5D-5L. Additionally, the distribution of index values was compared between EQ-5D-3L and EQ-5D-5L responses, where a distribution with no or few clusters was preferred.
Informativity was assessed by calculating Shannon’s indices (using log base 2) for each EQ-5D dimension [Citation40]. The informativity of an instrument assesses its ability to capture all possible health profiles and to discriminate between persons with different health statuses [Citation40]. Shannon’s index (H΄) describes the extent to which information is evenly distributed across all possible response options, and Shannon’s Evenness Index (J΄) corrects for the number of possible response options [Citation24]. A higher index indicates that more information is captured by an instrument, with the underlying assumption that an item is most efficiently used when responses are evenly distributed. Absolute informativity (H΄) ranges between 0 and 1.58 for EQ-5D-3L, and between 0 and 2.32 for EQ-5D-5L. Relative informativity (J΄) takes a number between 0 and 1. We hypothesized that higher absolute informativity (H΄) and equal or higher relative informativity (J΄) would be observed for EQ-5D-5L compared to EQ-5D-3L.
Construct validity
The assessment of construct validity included convergent and known-group validity. Convergent validity is an assessment of whether responses to one instrument are associated with responses to other instruments that, in theory, measure the same or a similar construct [Citation11]. Convergent validity was assessed by separately examining the strength of association of each of the two EQ-5D versions with other measures using Spearman’s rank-order correlation. The correlation coefficients (rho) were interpreted using the following thresholds: absent (rho < 0.2), weak (0.2≤ rho <0.35), moderate (0.35≤ rho <0.5), and strong (rho ≥ 0.5) [Citation41]. We hypothesized that correlations would be observed between: EQ-5D mobility and LCI-5, EQ-5D self-care and LCI-5, EQ-5D usual activities and LCI-5, EQ-5D mobility and the prosthetic use score, EQ-5D pain/discomfort and phantom limb pain, EQ-5D pain/discomfort and residual limb pain, EQ-5D sum score and overall situation as an amputee, and (for EQ-5D-5L) the EQ VAS and overall situation as an amputee. For all correlation analyses concerning the EQ-5D, we hypothesized that there would be equal or stronger correlations between EQ-5D-5L and other measures compared to the correlations between EQ-5D-3L and other measures.
Known-group validity reflects what extent an instrument is able to discriminate between groups with anticipated differences in the construct covered by the instrument [Citation11]. We hypothesized that those with a higher amputation level (TFA/KD) and those with amputation due to diabetes and/or vascular disease would have worse HRQoL. Relative efficiency (RE) was calculated to determine which version was most sensitive in detecting differences between known groups [Citation11]. For each subsample, independent t-tests were conducted to compare mean index values between groups defined by amputation level (TTA; TFA/KD) and by underlying diagnosis (diabetes and/or vascular disease; other). The RE ratio between EQ-5D-3L and EQ-5D-5L was calculated based on the squared t-statistics, using the largest t-statistic as the denominator. The RE was expressed as a ratio between 0 and 1 (strongest). Data analyses were conducted in IBM SPSS Statistics 25.
Ethical considerations
The study was approved by the regional ethical review board in Stockholm, Sweden (Reg. no. 2018/1137-31/2). Before obtaining data from the SwedeAmp registry, an application concerning data extraction for research purposes was approved and the data pseudonymized.
Results
Study population
The total sample included 700 patients with a major unilateral LLA, including subsamples of EQ-5D-3L respondents (n = 435) and EQ-5D-5L respondents (n = 265). After excluding patients with incomplete responses on the EQ-5D descriptive system (n = 15), 425 EQ-5D-3L respondents and 260 EQ-5D-5L respondents were included (). The amputations were performed between 2010 and 2018 and the six-month follow-ups between 2011 and February 2019. More than two-thirds (68%) of the respondents were men, and the mean age at amputation was 72 years (range 20–100). In the total sample, 76% had a TTA, 18% had a TFA, and 7% had a KD. More than 80% had diabetes and/or vascular disease as the underlying diagnosis.
Table 1. Background characteristics for patients with complete responses on the EQ-5D descriptive system at the six-month follow-up after unilateral lower limb amputation, by subsample.
At the six-month follow-up, approximately 60% reported their overall situation as an amputee as “good” or “very good” (61% subsample EQ-5D-3L; 59% subsample EQ-5D-5L), and about 14% reported their overall situation as “bad” or “very bad” (). Fifty percent experienced some degree of residual limb pain, and 67% experienced some degree of phantom limb pain. The median LCI-5 total score was 28 (range 0–56), and the median prosthetic use score was 32 (range 0–100).
Table 2. Self-reported health outcomes at six-month follow-up after unilateral lower limb amputation, by subsample.
Comparison of subsamples
There were no statistically significant differences between the two subsamples regarding sex, age, amputation procedure, amputation level, or underlying diagnosis (p > 0.05) (). In addition, no statistically significant differences were found regarding the overall situation as an amputee, the LCI-5 scores, or the prosthetic use score (p > 0.05) at the six-month follow-up (). However, the subsamples differed regarding phantom limb pain (p < 0.001) and residual limb pain (p < 0.05), with a larger proportion reporting any level of pain in the EQ-5D-5L subsample.
Feasibility
Of all patients with a registered six-month follow-up assessment including EQ-5D, fifteen patients had incomplete EQ-5D responses (73% male, mean age 73.9 years). The number of patients who did not respond to any of the dimensions was eight in the EQ-5D-3L sample and four in the EQ-5D-5L sample. Missing response on the mobility dimension only was observed for two patients in the EQ-5D-3L sample and one patient in the EQ-5D-5L sample. Thus, the feasibility of EQ-5D-3L and EQ-5D-5L was comparable (97.7% versus 98.1% complete responses).
Distributional characteristics
The EQ-5D-3L and EQ-5D-5L dimensions with the most frequent reporting of problems were mobility (78% and 75%), pain/discomfort (70% and 75%), and usual activities (61% and 74%) (). The mean level sum score was 8.30 (SD 1.87) for EQ-5D-3L and 11.46 (SD 4.16) for EQ-5D-5L. The median EQ VAS (available only for the EQ-5D-5L subsample, n = 229) was 70 (supplementary material 1). The EQ-5D index ranged between −0.35 and 1 (mean 0.55, SD 0.31) for EQ-5D-3L respondents, and between −0.40 and 1 (mean 0.53, SD 0.31) for EQ-5D-5L respondents.
Figure 1. Distribution of responses on the EQ-5D dimensions at six-month follow-up after a unilateral amputation, among EQ-5D-3L (3L) respondents (n = 425) and EQ-5D-5L (5L) respondents (n = 260).
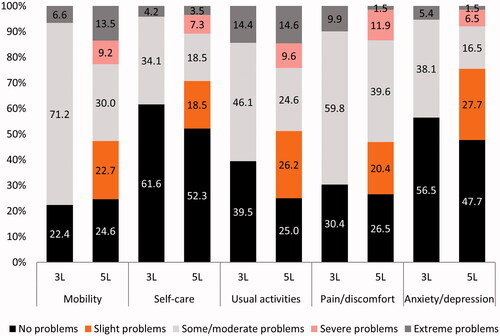
The proportion reporting no problems in all five dimensions (i.e., 11111) was 6.6% among EQ-5D-3L respondents and 5.8% among EQ-5D-5L respondents. None of the respondents reported extreme problems in all dimensions (i.e., 33333 or 55555). The number of observed health profiles in the EQ-5D-3L and EQ-5D-5L samples were 94 and 184, respectively. In the mobility dimension, more than 20% of the EQ-5D-5L respondents reported severe or extreme problems, while less than 7% of the EQ-5D-3L respondents reported extreme problems (). The distributions of EQ-5D-5L index values were slightly less clustered than those of EQ-5D-3L index values (supplementary material 2).
EQ-5D-5L had higher absolute informativity (H΄) and relative informativity (J΄) compared to EQ-5D-3L across all dimensions (). For both versions, the highest informativity was observed in the usual activities dimension. The largest difference in relative informativity (J΄) was observed in the mobility dimension. The lowest absolute (H΄) and relative informativity (J΄) for EQ-5D-3L were observed in the mobility dimension in which the majority (71%) indicated having moderate problems (level 2) ().
Table 3. Informativity, as assessed by Shannon’s indices, by EQ-5D version.
Construct validity
Overall, correlations between EQ-5D dimensions and other measures were in line with the hypotheses, and weak to strong correlations were observed (). As hypothesized, LCI-5 correlated with the EQ-5D dimensions for usual activities, self-care, and mobility in both versions (p < 0.01). Both versions also showed a moderate correlation between the mobility dimension and the prosthetic use score as well as between the pain/discomfort dimension and the measures of phantom limb pain and residual limb pain. Further, the EQ-5D sum score correlated moderately (EQ-5D-3L) or strongly (EQ-5D-5L) with the overall situation as an amputee. Moderate to strong correlations were also observed between the EQ-5D sum score and the LCI-5 and the prosthetic use score, respectively. The EQ VAS, which was available only for EQ-5D-5L, correlated moderately with the overall situation as an amputee. As expected, the correlations were generally stronger between EQ-5D-5L and the other measures compared to those between EQ-5D-3L and the other measures. Strong correlations (rho ≥ 0.5) with other measures were observed for EQ-5D-5L only.
Table 4. Spearman’s rank correlation coefficients (rho) between responses to the EQ-5D versions (sum score, dimensions, and EQ VAS [5L]), and LCI-5, prosthetic use score, residual limb pain, phantom limb pain, and overall situation as an amputee.
In line with the hypotheses regarding known-group validity, HRQoL was on average worse among those with a higher amputation level (TFA/KD) (, supplementary material 1). Only EQ-5D-5L was able to discriminate between groups defined by amputation level (p < 0.05), which was also indicated by a RE ratio of 0.538 (). Neither the index values for EQ-5D-3L nor EQ-5D-5L indicated differences in HRQoL depending on the underlying diagnosis. Worse HRQoL was observed among women, among patients in older age groups, and with a higher amputation level (TFA/KD) (supplementary material 1,3,4). Considering both amputation level and underlying diagnosis, the lowest capability to perform locomotor activities (LCI-5 scores) was found in patients with TFA/KD due to diabetes and/or vascular disease (supplementary material 5).
Table 5. Mean EQ-5D index values, t-statistics, and relative efficiency of EQ-5D-3L and EQ-5D-5L, by known groups (amputation level and underlying diagnosis).
Discussion
This study comprised an extensive analysis of real-world health outcomes data, including both generic and disease-specific measures, for a large sample of patients with an LLA. The study findings showed that both EQ-5D versions have satisfactory results regarding feasibility and validity in patients with LLA. The vast majority of respondents (>97.7%) provided complete responses on the EQ-5D descriptive system, and the proportion of respondents reporting no problems in all dimensions (“ceiling”) was less than 7%. In addition, the EQ-5D dimensions of both versions correlated with disease-specific measures according to the hypotheses.
In the comparison of the two versions, EQ-5D-5L showed similar or improved measurement properties, as indicated by the more evenly distributed responses and index values and superior informativity across all dimensions. Further, the results regarding construct validity were favorable for EQ-5D-5L. These findings are in line with previous studies demonstrating improved measurement properties of EQ-5D-5L in other patient populations [Citation24,Citation25]. Interestingly, the improvement in informativity was most evident in the mobility dimension, which is in line with the findings of previous studies including patients awaiting hip and knee replacement [Citation33,Citation34]. On both EQ-5D versions, reported problems were most commonly related to mobility, pain/discomfort, or usual activities. These findings are in line with previous studies in which patients have responded to EQ-5D after an LLA, using EQ-5D-3L [Citation16] or EQ-5D-5L [Citation10]. The findings can also be related to the broader literature on HRQoL in patients with an LLA. Two literature reviews identified studies based on a variety of outcome measures (e.g., the SF-36, RAND-36, Nottingham Health Profile, and disease-specific scales) and found factors such as limitations in physical functioning, activities of daily living, and phantom limb pain and residual limb pain to be predictors of impaired quality of life [Citation1,Citation2].
Further, the results indicate that HRQoL is worse among women, among older patients, and among patients with a higher amputation level, which is consistent with previous research [Citation1,Citation9]. Also, differences in HRQoL have been previously identified between groups of patients with dysvascular disease or trauma as the underlying condition [Citation10]. However, the current study did not demonstrate any distinct differences in HRQoL between subgroups defined by an underlying diagnosis. The lack of differences between the groups should be interpreted with caution, as the subgroup including patients with “other” underlying conditions represents a relatively heterogeneous group that also included conditions registered as “unknown.”
Implications for policy, practice, and future research
In addition to contributing to the existing knowledge on the psychometric properties of EQ-5D-3L and EQ-5D-5L, the study findings provide valuable information about patients’ HRQoL in the early rehabilitation process after a unilateral major LLA. Since the results are based on registry data collected in health care and rehabilitation settings, the results reflect real-world PROMs data for a relatively large sample of patients with a major LLA. The study findings may be used to inform the choice of outcome measures in clinical studies, health economics evaluation, and routine follow-up in health care. Furthermore, the results regarding the EQ-5D index in this patient population may constitute valuable input for health economic modelling. Nonetheless, previous studies have emphasized the need for prospective longitudinal studies to better understand the progress of patients’ HRQoL after an LLA [Citation2] and to further evaluate the responsiveness and reliability of the two EQ-5D versions [Citation24]. Thus, further research is needed to explore the development of HRQoL over time, preferably by examining both generic and disease-specific outcomes in this patient population.
Strengths and limitations
A strength of this register-based study was the large study population, which is considerably larger than those in previous studies. In addition, the use of data from a national quality registry, which has been collected in routine health care settings, enabled the inclusion of patients with a broad range of characteristics and analysis of real-world outcomes after LLA. Further, data on several patient-reported measures enabled an extensive analysis of construct validity in which the associations between two EQ-5D versions and several disease-specific instruments were analyzed.
However, the study has certain limitations that should be considered. First, data on EQ-5D-3L and EQ-5D-5L were collected during different time periods, resulting in two separate subsamples. As there may have been changes in medical practice, patient characteristics, or other factors that may influence health outcomes over time, individual reporting on both versions would have been preferred for the comparative assessment. The reason why a larger proportion of the EQ-5D-5L respondents reported phantom limb pain and residual limb pain at follow-up is currently unclear and call for future analysis. Nevertheless, the two subsamples did not differ in terms of background characteristics, and the use of multiple methods to analyze the measurement properties reduced the risk that any differences between subsamples would have a large impact on the study conclusions.
Second, the use of retrospective national registry data implicates limited control over the registration of data. The risk of random error during registration is difficult to assess yet may have consequences for the assessment of feasibility. For example, the proportion of complete EQ-5D responses may be overestimated if the EQ-5D variables are not recorded for patients who receive but do not respond to the questionnaire. Related to this, there are restrictions to the data typically available from national registers. Various other patient and clinical characteristics may influence patients’ interpretation and response to PROMs [Citation1,Citation42]. For example, in this study, there is limited information about the patient’s language skills and any assistance received when responding to the questionnaires in health care settings (e.g., by interpreter or other), comorbidities, level of support, and previous experience of disease.
Third, it should be noted that the known-group validity analyses are based on two different value sets for calculating the EQ-5D-3L and EQ-5D-5L index values, which introduce additional methodological variation into the comparison. Nevertheless, since the EQ-5D-5L crosswalk value set was developed based on the EQ-5D-3L value set, the comparison between the two eliminates any distorting effect of valuation protocol or preferences of the respondents, attributing more weight to the descriptive systems in the comparison.
Regarding the generalizability of results, it should be noted that the study sample predominantly comprised of patients with a unilateral amputation due to peripheral vascular disease and who had started prosthetic rehabilitation. Thus, the findings regarding HRQoL may not be generalizable to patients with bilateral amputations or other groups that differ considerably from our study population. In addition, not all patients registered in SwedeAmp had a follow-up that included EQ-5D, which can be explained by the fact that patients need to be in relatively good health to participate in prosthetic rehabilitation and by the relatively high mortality (19%) within the first six months after amputation [Citation3].
Conclusion
This study showed satisfactory measurement properties for both EQ-5D-3L and EQ-5D-5L in patients who have undergone a major unilateral LLA. The comparative assessment of the two versions indicates that the 5-level version is a superior measure among this group of patients, with favorable results in particular for informativity and validity. Patients commonly report problems related to mobility, pain or discomfort, and usual activities in the early rehabilitation after a major LLA. With a relatively large sample size and use of real-world data from health care settings, this study contributes to increased knowledge on health outcomes from the patient perspective six months after amputation and provides a better understanding of the performance of different outcome measures among patients with a unilateral major LLA.
Ethics approval
Registration in a Swedish national quality register is voluntary (with the possibility to opt-out). The patient has the right to receive information, to refuse registration, and to be removed from the register. Researchers are required to write a formal application regarding data extraction for research purposes, including approval from an ethical review board. The study was approved by an ethical review board and no written informed consent was required.
Supplemental Material
Download MS Word (60.7 KB)Acknowledgments
We would like to express our gratitude to all patients and personnel at the contributing units who provided data to the Amputation and Prosthetics Registry (SwedeAmp). The study was funded by Region Stockholm within a license agreement between Region Stockholm and the EuroQol Research Foundation. EH received a grant from VinnVård/FORTE (Vinnvård Improvement Science Fellow, dnr: 2015-01331). KH was funded by the Swedish state under the agreement between the Swedish government and the county councils, the ALF agreement [ALFGBG-76480]. MJ and GB were funded by the EuroQol Research Foundation. The views expressed by the authors in the publication do not necessarily reflect the views of the EuroQol Group. Some of the data in this study were summarized previously in a PhD thesis (“Making use of patient-reported outcome measures in health care: the case of EQ-5D in the Swedish national quality registries”, Karolinska Institutet, 2021).
Disclosure statement
The study was funded by Region Stockholm within a research program that is part of a license agreement between Region Stockholm and the EuroQol Research Foundation. MJ is working on a freelance basis at the EuroQol Business Office and is a EuroQol member. GB is employed by the EuroQol Research Foundation and is a EuroQol member. OE and EH have received travel grants from the EuroQol Research Foundation. KH, SK, and NZ declare no conflict of interest.
Data availability statement
Access to data is restricted by Swedish law. General information about obtaining access to data is available from the corresponding author Olivia Ernstsson upon request.
References
- Davie-Smith F, Coulter E, Kennon B, et al. Factors influencing quality of life following lower limb amputation for peripheral arterial occlusive disease: a systematic review of the literature. Prosthet Orthot Int. 2017;41(6):537–547.
- Sinha R, Van den Heuvel WJA. A systematic literature review of quality of life in lower limb amputees. Disabil Rehabil. 2011;33(11):883–899.
- Kamrad I, Soderberg B, Orneholm H, et al. SwedeAmp-the Swedish amputation and prosthetics registry: 8-year data on 5762 patients with lower limb amputation show sex differences in amputation level and in patient-reported outcome. Acta Orthop. 2020;22:1–7.
- Moxey PW, Gogalniceanu P, Hinchliffe RJ, et al. Lower extremity amputations-a review of global variability in incidence. Diabet Med. 2011;28(10):1144–1153.
- Wurdeman SR, Stevens PM, Campbell JH. Mobility analysis of AmpuTees (MAAT I): quality of life and satisfaction are strongly related to mobility for patients with a lower limb prosthesis. Prosthet Orthot Int. 2018;42(5):498–503.
- van Netten JJ, Fortington LV, Hinchliffe RJ, et al. Early post-operative mortality after major lower limb amputation: a systematic review of population and regional based studies. Eur J Vasc Endovasc Surg. 2016;51(2):248–257.
- Fortington LV, Dijkstra PU, Bosmans JC, et al. Change in health-related quality of life in the first 18 months after lower limb amputation: a prospective, longitudinal study. J Rehabil Med. 2013;45(6):587–594.
- Horgan O, MacLachlan M. Psychosocial adjustment to lower-limb amputation: a review. Disabil Rehabil. 2004;26(14–15):837–850.
- Sinha R, van den Heuvel WJA, Arokiasamy P. Factors affecting quality of life in lower limb amputees. Prosthet Orthot Int. 2011;35(1):90–96.
- Jayakaran P, Perry M, Hale L. Comparison of self-reported physical activity levels and quality of life between individuals with dysvascular and non-dysvascular below-knee amputation: a cross-sectional study. Disabil Health J. 2019;12(2):235–241.
- Fayers PM, Machin D. Quality of life: the assessment, analysis, and reporting of patient-reported outcomes. Third edition. ed. Chichester, West Sussex (UK); Hoboken (NJ): John Wiley & Sons Inc.; 2016.
- Rabin R, de Charro F. EQ-5D: a measure of health status from the EuroQol group. Ann Med. 2001;33(5):337–343.
- Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727–1736.
- Appleby J, Devlin NJ, Parkin DW. Using patient reported outcomes to improve health care. Chichester, West Sussex (UK); Hoboken (NJ): John Wiley & Sons Inc.; 2016.
- Devlin NJ, Brooks R. EQ-5D and the EuroQol group: past, present and future. Appl Health Econ Health Policy. 2017;15(2):127–137.
- Tennvall GR, Apelqvist J. Health-related quality of life in patients with diabetes mellitus and foot ulcers. J Diabetes Complicat. 2000;14(5):235–241.
- Clarke P, Gray A, Holman R. Estimating utility values for health states of type 2 diabetic patients using the EQ-5D (UKPDS 62). Medical Decision Making. 2002;22(4):340–349.
- Hayes A, Arima H, Woodward M, et al. Changes in quality of life associated with complications of diabetes: results from the ADVANCE study. Value Health. 2016;19(1):36–41.
- O'Reilly DJ, Xie F, Pullenayegum E, et al. Estimation of the impact of diabetes-related complications on health utilities for patients with type 2 diabetes in Ontario, Canada. Qual Life Res. 2011;20(6):939–943.
- Sothornwit J, Srisawasdi G, Suwannakin A, et al. Decreased health-related quality of life in patients with diabetic foot problems. DMSO. 2018;11:35–43.
- Voko Z, Gaspar K, Inotai A, et al. Osteoporotic fractures may impair life as much as the complications of diabetes. J Eval Clin Pract. 2017;23(6):1375–1380.
- Tangelder MJ, McDonnel J, Van Busschbach JJ, et al. Quality of life after infrainguinal bypass grafting surgery. Dutch bypass oral anticoagulants or aspirin (BOA) study group. J Vasc Surg. 1999;29(5):913–919.
- Ernstsson O, Janssen MF, Heintz E. Collection and use of EQ-5D for follow-up, decision-making, and quality improvement in health care – the case of the Swedish National Quality Registries. J Patient Rep Outcomes. 2020;4(1):78.
- Buchholz I, Janssen MF, Kohlmann T, et al. A systematic review of studies comparing the measurement properties of the three-level and five-level versions of the EQ-5D. Pharmacoeconomics. 2018;36(6):645–661.
- Janssen MF, Bonsel GJ, Luo N. Is EQ-5D-5L better than EQ-5D-3L? A head-to-Head comparison of descriptive systems and value sets from seven countries. Pharmacoeconomics. 2018;36(6):675–697.
- Craig BM, Pickard AS, Lubetkin EI. Health problems are more common, but less severe when measured using newer EQ-5D versions. J Clin Epidemiol. 2014;67(1):93–99.
- Shafie AA, Vasan Thakumar A, Lim CJ, et al. Psychometric performance assessment of Malay and Malaysian English version of EQ-5D-5L in the Malaysian population. Qual Life Res. 2019;28(1):153–162.
- Golicki D, Niewada M, Buczek J, et al. Validity of EQ-5D-5L in stroke. Qual Life Res. 2015;24(4):845–850.
- Kim SH, Kim HJ, Lee SI, et al. Comparing the psychometric properties of the EQ-5D-3L and EQ-5D-5L in cancer patients in Korea. Qual Life Res. 2012;21(6):1065–1073.
- Agborsangaya CB, Lahtinen M, Cooke T, et al. Comparing the EQ-5D 3L and 5L: measurement properties and association with chronic conditions and multimorbidity in the general population. Health Qual Life Out. 2014;12:74.
- Buchholz I, Thielker K, Feng YS, et al. Measuring changes in health over time using the EQ-5D 3L and 5L: a head-to-head comparison of measurement properties and sensitivity to change in a German inpatient rehabilitation sample. Qual Life Res. 2015;24(4):829–835.
- Jia YX, Cui FQ, Li L, et al. Comparison between the EQ-5D-5L and the EQ-5D-3L in patients with hepatitis B. Qual Life Res. 2014;23(8):2355–2363.
- Jin XJ, Al Sayah F, Ohinmaa A, et al. The EQ-5D-5L is superior to the-3L version in measuring health-related quality of life in patients awaiting THA or TKA. Clin Orthop Relat Res. 2019;477(7):1632–1644.
- Conner-Spady BL, Marshall DA, Bohm E, et al. Reliability and validity of the EQ-5D-5L compared to the EQ-5D-3L in patients with osteoarthritis referred for hip and knee replacement. Qual Life Res. 2015;24(7):1775–1784.
- Oppe M, Devlin NJ, van Hout B, et al. A program of methodological research to arrive at the new international EQ-5D-5L valuation protocol. Value Health. 2014;17(4):445–453.
- Dolan P. Modeling valuations for EuroQol health states. Med Care. 1997;35(11):1095–1108.
- van Hout B, Janssen MF, Feng YS, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15(5):708–715.
- Franchignoni F, Orlandini D, Ferriero G, et al. Reliability, validity, and responsiveness of the locomotor capabilities index in adults with lower-limb amputation undergoing prosthetic training. Arch Phys Med Rehabil. 2004;85(5):743–748.
- Hagberg K, Branemark R, Hagg O. Questionnaire for persons with a transfemoral amputation (Q-TFA): initial validity and reliability of a new outcome measure. J Rehabil Res Dev. 2004;41(5):695–706.
- Janssen MF, Birnie E, Bonsel GJ. Evaluating the discriminatory power of EQ-5D, HUI2 and HUI3 in a US general population survey using Shannon's indices. Qual Life Res. 2007;16(5):895–904.
- Juniper E, Gordon H, Roman J. How to develop and validate a new health-related quality of life instrument. In: Spilker B, editor. Quality of life and pharmacoeconomics in clinical trials. 2nd ed. Philadelphia: Lippincott Williams & Wilkins; 1996.
- Ernstsson O, Burstrom K, Heintz E, et al. Reporting and valuing one's own health: a think aloud study using EQ-5D-5L, EQ VAS and a time trade-off question among patients with a chronic condition. Health Qual Life Outcomes. 2020;18(1):388.