
Abstract
Purpose
Motor learning interventions for children with cerebral palsy (CP) that elicit relatively permanent and transferable improvements in motor skill capability are essential. Knowledge is needed about the augmented feedback forms that most effectively promote this. This review aims to collect and analyze the current evidence for the effectiveness of different forms of feedback for motor learning in children with CP to improve motor task performance.
Methods
PubMed, PsycInfo, and Cochrane Library were searched to identify relevant studies. Studies were included if (1) they were conducted in children with CP or compared children with CP to TD children and (2) a form of augmented feedback related to a motor task was administered.
Results
Initially, 401 records were identified for screening. Ultimately, 12 articles were included in the review. The evidence thus far supports the expectancy that children with CP generally benefit from feedback provided during or after performing a movement task.
Conclusion
Due to the heterogeneity of existing studies, it is difficult to draw firm conclusions regarding relative effectiveness of feedback forms. This review showed that more high-quality research is warranted on the effectiveness of specific feedback forms on motor learning in children with CP.
Children with CP benefit from several forms of knowledge of performance or knowledge of results feedback provided during or after performing a movement task.
Feedback should not be provided with every performed trial.
Feedback frequency can best be reduced by letting children determine after which trials they want feedback.
Learning curves under similar feedback conditions varied largely between children, warranting tailor-made forms of feedback to be applied during motor learning and rehabilitation.
Implications for Rehabilitation
Introduction
Cerebral palsy is a collection of permanent disorders involving motor, sensory, and cognitive disabilities that are attributed to non-progressive disturbances in the developing brain (i.e., perinatal brain lesions or anomalies or postnatal injuries or infections) [Citation1,Citation2]. Location and extent of the cerebral damage differ between cases and, as a consequence, so does the symptomatic expression. This heterogeneity necessitates a structured classification. Distinctions are therefore made based on type (spastic, dyskinetic, ataxic, or mixed) and patterns of neurologic involvement (primary distinction between unilateral and bilateral CP; further specified into monoplegia, hemiplegia, paraplegia, diplegia or quadriplegia) [Citation3,Citation4]. The Gross Motor Function Classification Scale (GMFCS) classifies patients into five groups based on functional mobility and independency (level I–V) [Citation5].
When it comes to movement, people with CP face multiple challenges. In addition to afferent inhibition, their selective muscle activation is impaired as well as their ability to regulate muscle activity in anticipation of movement [Citation6]. As a consequence, they can have problems with postural control, balance and gait, but also with upper extremity movements. Compared to typically developing (TD) children, children with CP have a lower ability to acquire new motor skills [Citation7,Citation8]. Their deficits can limit daily activity considerably and have a large negative impact on individual wellbeing and social interaction [Citation9,Citation10]. This is especially true for difficulties in acquiring motor skills in children with CP, since throughout the span of childhood, motor learning plays a major role in children’s ability to participate in daily life activities as they become increasingly independent. From balance to locomotion to fine motor tasks like drawing, grasping, or cutting food, children grow, learn, and improve their performance continuously. Children with CP who have limited motor capacity and manual ability are at risk for restrictions in participation in domestic life and interpersonal relationships in adolescence and adulthood [Citation11].
Motor learning is defined as the (re)acquisition or performance enhancement of activities or tasks that require voluntary movement control to achieve a goal [Citation12]. When practicing a motor task, the sensory information that is naturally available during the movement is used to improve performance. The learning process can be accelerated by providing additional information on execution or outcome of the movement, termed “augmented feedback” [Citation13]. Because of the sensory deficits many people with CP encounter, they may have limited access to task-intrinsic information, which makes external sources of information more important or even crucial to facilitate motor learning. This is why augmented feedback is of interest in children with sensorimotor impairments such as CP. For that reason, this review is aimed at identifying effective forms of feedback in children with CP.
The family tree of augmented feedback is quite an elaborate one. For a graphic display, see . First of all, different modalities can be used to deliver feedback (visual, auditory, sensory, verbal, etc.). Furthermore, all augmented feedback can be divided into two categories: knowledge of results (KR; information about the outcome of the attempt) and knowledge of performance (KP; information about the movement characteristics that led to the outcome). Both can have positive effects on skill learning [Citation14], but KP is more beneficial than KR if successful skill performance requires specified movement characteristics [Citation15,Citation16].
Figure 1. Visual display of different forms of extrinsic feedback.
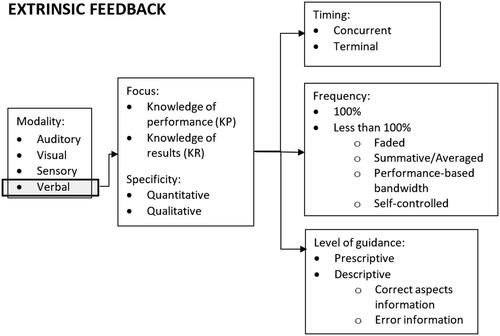
KP feedback can take different shapes. When delivered verbally, it can be either descriptive (simply describing the error) or prescriptive (instructing on how to correct the error in addition to identifying it). It can also be provided through video recordings (possibly with additional verbal feedback), which is more effective than verbal feedback alone [Citation17]. Using kinetic or kinematic KP in motor learning has become more popular with the rise of sophisticated technology and it can enable people to quickly acquire complex coordination patterns [Citation18,Citation19].
Besides the KR/KP categorization, more distinctions can be made based on the content of the augmented feedback. For example, information can be provided on either the errors or the correct aspects of a performance. For facilitation of skill learning, error information is more effective for improving performance during practice, whereas information about the correct aspects of the movement has more positive effects on a person’s motivation [Citation20]. Furthermore, feedback can be quantitative (giving a numeric value from a performance characteristic), qualitative (giving non-numeric information on a performance characteristic), or both.
Timing and frequency of feedback provision are also of considerable influence on skill acquisition and retention. When a person receives augmented feedback during task execution (concurrent feedback), a negative learning effect may occur; performance improves steeply during practice but declines dramatically on retention and transfer tests [Citation21]. In contrast, giving augmented feedback after trials (terminal feedback) can lead to positive learning effects on retention and transfer tests [Citation21]. Furthermore, learning effects depend on how often augmented feedback is provided: a frequency of 100% (after every single trial) often leads to a lower amount of learning than a lower frequency [Citation22,Citation23]. Several techniques exist to lower the frequency in a systematic way. For instance, feedback can be given within a performance-based bandwidth, feedback can be summed of averaged over several trials, feedback frequency can be lowered over time (“faded”), or self-controlled by the participant.
These differential effects of timing and frequency of feedback on motor performance on the one hand and motor learning on the other, as observed in general populations, illustrate the importance of a comprehensive research design in motor learning studies. Measuring performance on a given task under given feedback conditions at a certain point in time provides information about the influence of this feedback on participants’ motor performance, but gives little insight in their motor learning. The full scope of feedback effects on motor learning (which includes persistence, adaptability, stability, and lowered attention demands) can only be made overt if retention tests, transfer tests, and dual-task conditions are administered.
It is clear that the way augmented feedback is provided influences the learning process. On top of that, the learning effects of varying forms depend on other factors. For example, task complexity determines through which modality feedback should be provided to get the best learning effects (e.g., for more complex tasks, visual feedback is more beneficial if it is delivered concurrently instead of terminally [Citation24]). Also, effects may be dissimilar for learners of different skill levels. Novices benefit most from prescriptive and qualitative feedback, whereas advanced learners show larger improvements with descriptive and quantitative feedback [Citation13]. Moreover, the effects of feedback may depend on any motor or cognitive impairment a person may have. This begs the question whether the “feedback rules” from the able-bodied population are generalizable to children with CP. Motor planning deficits [Citation25] might make it difficult for them to make optimal use of some forms, but augmented feedback could also enhance their learning, providing compensation for sensory impairments. Studies involving patients with other motor disorders, such as Parkinson’s disease (PD), have found divergent results. For example, the “rules” for concurrent versus terminal feedback are similar for able-bodied participants and PD patients [Citation26], whereas the “reduced frequency benefit” has not been demonstrated for PD patients [Citation27].
Therapy programs in children with CP ultimately aim to elicit relatively permanent improvements in motor skill capability that can be transferred and generalized to new learning situations. For this, knowledge is needed about which augmented feedback forms can be utilized to improve motor skills. Robert et al. conducted a review in 2017 [Citation28], where feedback effects in upper extremity tasks were examined in children with CP and TD children. They concluded that there was a lack of consistency in modalities and frequencies of feedback studies and stressed the need for a better and more comprehensive understanding of the influence of feedback on motor learning in children with CP. This review will therefore attempt to expand the picture drawn by Robert and colleagues through collecting and analyzing the current evidence for the effectiveness of different forms of feedback in children with CP in motor tasks involving the upper and lower extremities, as well as whole-body tasks (gait, postural control, balance).
Methods
Design
A systematic review was conducted following the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-analyses [Citation29]). The protocol was registered in PROSPERO (CRD42020213425).
Search strategy
PubMed, PsycInfo, and Cochrane Library were searched to identify relevant studies in English, with full text availability. No restriction was set concerning the year of publication and articles until November 2021 were included. The search terms used in PubMed were as follows: ("Cerebral Palsy"[Mesh] OR Cerebral Palsy [tiab] OR cp [tiab]) AND ("Feedback, Psychological"[Mesh] OR "Feedback, Physiological"[Mesh] OR psychological feedback [tiab] OR augmented feedback [tiab] OR physiological feedback [tiab] OR verbal feedback [tiab] OR visual feedback [tiab] OR auditory feedback [tiab] OR “knowledge of performance” OR “knowledge of results” OR enhanced feedback [tiab] OR sensory feedback [tiab] OR feedback strateg* [tiab] OR extrinsic feedback [tiab]). Reference lists of primary articles were checked to identify relevant studies that had been missed by the electronic search.
Study selection
Study selection was performed by two researchers, independent from each other. Discrepancies were resolved by discussion. Titles, abstracts, and full texts were screened for eligibility. Studies were included if (1) they were conducted among children with CP or they compared children with CP to TD children; (2) a specified form of extrinsic feedback was administered in a motor learning intervention; and (3) outcome measures related to motor skill performance were reported. Studies were excluded if (1) they were conducted in adults (participants >18 years old); (2) the sample included children with etiologies other than CP; (3) the intervention revolved around biofeedback, proprioceptive feedback, mirror therapy, or virtual reality multimodal feedback; (4) the reported outcomes consisted solely of brain imaging results.
We did not include biofeedback, proprioceptive feedback, mirror therapy, or virtual reality multimodal feedback in the current review for two reasons. Firstly, these feedback forms are of such a distinctive nature that it would be difficult to draw clear comparisons between studies investigating very different feedback forms. Secondly, the number of studies on each of these four topics proved to be very large in our search results, which would have led to a very high, hardly manageable number of included studies for a single review. Therefore, the authors feel that these forms would come out better in separate review articles.
Data extraction and risk of bias
Data were extracted on study and sample characteristics and outcomes. Sample characteristics included sample size, sex ratio, age range, type of CP (uni-/bilateral, mono-/hemi-/di-/quadriplegic, and spastic/ataxic/athetoid/mixed) and GMFCS level. Motor tasks were defined in complexity, functional body segments involved (upper/lower extremities, trunk), and gross or fine motor control. Tasks were considered complex when they had two or more degrees of freedom and a multi-limb coordination pattern had to be acquired. The number of trials was noted, as well as the assessment time points. Feedback administration was categorized based on KP/KR and modality (i.e., visual, auditory, sensory, verbal) and feedback schedule per group was described. Effects on outcome measures were extracted and in case of significant findings, effect sizes were noted if reported or calculated with data published in the article if possible.
Studies were assessed on risk of bias using the Cochrane risk of bias tool 2 (RoB 2) [Citation30]. Ratings of “low risk of bias,” “some concerns,” and “high risk of bias” were assigned to each of the following five domains: (1) bias arising from the randomization process; (2) bias due to deviations from intended interventions; (3) bias due to missing outcome data; (4) bias in measurement of outcome; and (5) bias in selection of the reported outcome. Based on the five domains, each included study was given a judgement of overall risk of bias.
Results
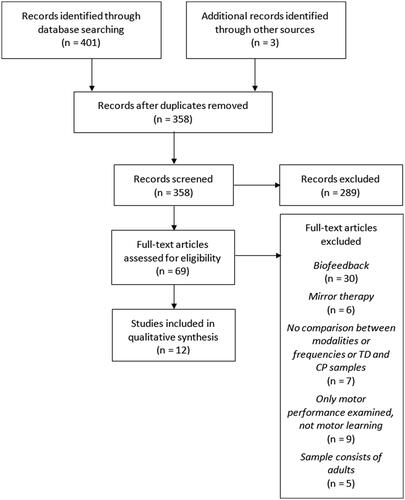
The search strategy resulted in a total of 401 records. In addition, three publications were identified through the screening of primary articles for any other potentially relevant citations. After removing duplicates, 358 articles were screened on title and abstract. A remainder of 69 articles was assessed for eligibility based on full text, resulting in the ultimate inclusion of 12 studies (see ).
Figure 2. Flow chart depicting the process of inclusion of studies.
Participants
In total, 311 participants (aged 5–26 years) were involved in the studies, including 264 children diagnosed with CP and 62 TD children. One of the studies covered an age range of 5–26 years [Citation31] but was included in the review nonetheless since only 1 participant was 26 years old. Without this participant, the maximum age reported was 18.
The most prevalent CP diagnosis of the included participants was spastic hemiplegia (at least 108 cases in 5 studies [Citation32–36]). Diplegic and quadriplegic CP was studied less often (at least 58 participants in 4 studies [Citation34,Citation37–39]). However, two studies did not report the type of CP [Citation38,Citation40], one study lacked information on the limbs affected [Citation41] and one study failed to report characteristics of the CP diagnosis of the included children [Citation31]. Only four of the studies provided information on GFMCS level of their participants (I–IV, I–III, II–III, and III, respectively [Citation34,Citation36–38]).
Characteristics of included studies
Effects of different frequencies in feedback schedules were compared in five of the studies [Citation32,Citation35,Citation36,Citation40,Citation41]. A comparison was made between CP and TD groups in four studies [Citation31,Citation32,Citation34,Citation39]. Effects of different sensory modalities through which feedback was provided were compared in one study [Citation31]. None of the included studies made any comparison between KR and KP, error information, and information about the correct aspects of the movement, quantitative and qualitative feedback, concurrent and terminal feedback, or investigated feedback effects on tasks of different complexity.
The type of movement that was practiced varied between studies; four studies examined gait tasks [Citation31,Citation33,Citation37,Citation38], whereas the remaining studies examined unimanual upper extremity tasks. These unimanual tasks were exclusively examined on the less-affected side. For a detailed description of all study characteristics, see and .
Table 1. Extracted details of the included studies applying knowledge of results feedback.
Table 2. Extracted details of the included studies applying knowledge of performance feedback.
Risk of bias
The results of the analysis of risk of bias are shown in (per study) and (overall). Four studies were judged at high risk in at least one domain. Furthermore, all included studies showed “some concerns” in varying domains. In the domain “randomization process” in particular, only two studies were assessed at “low risk of bias”. In the overall assessment, only one study was assessed at “low risk of bias”.
Figure 3. Results of risk-of-bias assessment for each study. Green = low risk of bias; red = high risk of bias; yellow = some concerns.
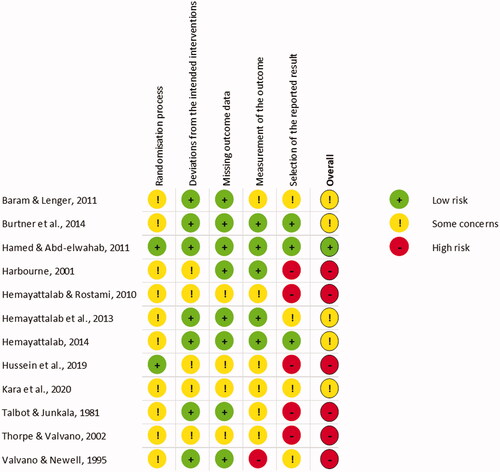
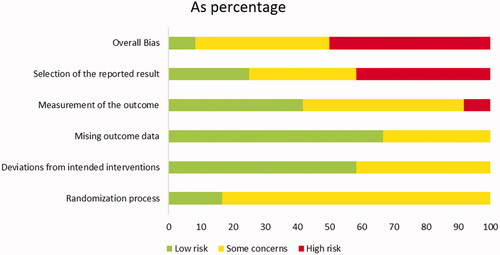
Figure 4. Results of risk-of-bias assessment per domain. Green = low risk of bias; red = high risk of bias; yellow = some concerns.
Comparison between modalities
Only one study compared the effectiveness of feedback provision through different modalities [Citation31]. They administered gait training with either visual feedback (projection of transverse lines in space) or auditory feedback (clicking sound at heel strike). The results showed that children with CP benefitted equally from visual or auditory feedback during gait. Their improvement in stride length and walking speed was of equal proportions in both feedback conditions. No retention test was administered.
Hamed and Abd-elwahab [Citation33] compared an auditory feedback condition to a no-feedback condition. They found that auditory feedback during walking (music following the speed and rhythm of a participant) resulted in improved velocity, stride length, cadence, and cycle time in children with spastic hemiplegic CP, in comparison to no feedback. No retention test was administered.
Hussein et al. [Citation37] found that gait training with visual feedback of foot pressure patterns led to significantly larger improvements on spatial and temporal gait parameters than gait training without augmented feedback in children with spastic diplegic CP. Step length, step width, foot angle, cadence, gait velocity, and gait time improved significantly more after training with visual feedback. There was no significant difference in kinetic gait parameters between the visual feedback and no-feedback group.
Descriptive vs. prescriptive
One study from Thorpe and Valvano [Citation38] involving children with diplegic or quadriplegic CP practicing a gait-related backwards locomotion task compared effects of two verbal KP feedback conditions and a no-feedback condition on total distance traveled. The children would receive either no feedback, descriptive KP, or prescriptive KP after a trial and each child was exposed to every condition. Of the 13 participants, eight were unable to learn the task – their performance did not improve. Four of the remaining participants were able to improve with practice alone. One child improved most during the descriptive KP condition, whereas three participants showed the biggest improvement during the prescriptive KP condition. A 48-h retention test was administered, where performance achievements from the acquisition phase were retained in all participants. However, no group-wise comparisons were made, and each participant completed a different number of trials in each condition.
Frequency
In the study of Burtner et al. [Citation32], a group of children with spastic hemiplegic CP replicated a target trajectory by moving a lever. Participants received visual feedback after either 100% of the trials or in a faded manner, so that overall, they received feedback after 62% of their trials. Both frequency conditions led to similar rates of improvement over a pretest, posttest, retention test, reacquisition test period. Three studies of the same first author investigated the effects of different feedback frequencies on learning a throwing task in children with spastic hemiplegic CP: two studies examined dart-throwing [Citation35,Citation40], whereas the third examined throwing a bean bag [Citation36]. There was no overlap of participants included in the three studies. In the study of Hemayattalab and Rostami [Citation35], children were provided with KR in 100%, 50%, or 0% of their trials. Children who received 100% scored better at the acquisition test, but at the retention test, the 50% group outperformed the other groups. The 0% group received no feedback but improved their performance over time nonetheless – although not as much as the other groups. Hemayattalab et al. [Citation36] gave half of their CP group KR at a self-controlled frequency, whereas the other half received KR at a yoked frequency. From pre to posttest, both groups improved their performance at a similar rate. At the 24-h retention test and at the transfer test (where the target distance was changed), the self-controlled group performed better. In the study of Hemayattalab [Citation40], visual KR was provided after 50% of the trials. After which trials KR was given, was determined either by participants themselves or by an instructor. A control group received no feedback. The self-controlled feedback group outperformed the other two groups at posttest, 24-h retention test and transfer test (where the target distance was changed). The instructor-controlled group and control group did not differ in their performance.
Finally, a study that compared feedback (100%), no-feedback (0%), and no-practice conditions was done by Talbot and Junkala [Citation41]. Children with spastic CP performed a line tracing task at pretest, posttest, and a three-month retention test. The feedback group was provided with auditory concurrent KP after 100% of the trials. This group outperformed the other two on the posttest, as well as on the retention test (although not significantly). The practice-only group improved only slightly, and the no-practice group did not improve at all.
Group-wise comparisons: CP vs. TD
Valvano and Newell [Citation39] compared the effects of 50% KR feedback frequency between a TD and a CP group who practiced a pinch grip force matching task. During acquisition, the TD group improved their accuracy at a higher rate than the CP group. On the five-day retention test, both groups upheld the performance levels that they were able to reach during acquisition.
The effects of verbal KR at a frequency of 75% were compared between a TD and CP group by Harbourne [Citation34]. The task consisted of moving a lever along a slide in 150 ms and subsequently guessing one’s own movement time. Compared to the CP group, the TD group systematically showed lower speed error and better error detection on the posttest. However, no pretest scores were extracted to compare the posttest values to. Looking at an individual level, Harbourne found that the children from the CP group showed varying learning curves: two showed a curve indistinguishable from that of TD children; four children showed large errors regardless of KR provision; three children showed large errors without KR and only small errors with KR.
Baram and Lenger [Citation31] found that with visual feedback during gait training, children with CP and TD children increased their walking speed to a similar extent. For stride length, the CP group improved more than the TD group. After training with auditory feedback, the improvements in both walking velocity and stride length were larger in children with CP.
In the lever task of Burtner et al. [Citation32], performance of the CP group was systematically lower than that of the TD group. However, there was also a similarity between CP and TD: for both groups, the 100% feedback condition led to similar learning outcomes as the 62% feedback condition.
Discussion
This review aimed to assemble and analyze the current evidence for the effectiveness of different forms of feedback in children with CP in motor tasks. There was a large heterogeneity between the included studies in terms of study design, tasks that were practiced, reported outcome measures, and analyses of the outcome measures. Combined with the “high risk” and prevalent “some concerns” outcomes of the risk of bias assessment, this warrants elaboration and improvement of research on augmented feedback in children with CP. For that reason, the scope of feedback aspects that can be discussed in depth in this review is limited. By the same token, as the majority of the included children was diagnosed with spastic hemiplegic CP and other types were underrepresented in the trials included, the results discussed below cannot be generalized to any other CP subgroup than the group that was included in the studies concerned.
Summary of results
Modality
Gait training with visual feedback [Citation37] or with auditory feedback [Citation33] leads to larger performance improvements than training without augmented feedback. Comparing these two modalities, Baram and Lenger [Citation31] found that children with CP benefit equally from either visual or auditory feedback during gait. These findings are in accordance with those of studies examining similar interventions in other populations with sensory-motor deficits (i.e., PD, multiple sclerosis, hemiplegic stroke [Citation42–46], and able-bodied adults [Citation47,Citation48]). The latter indicated that sex may influence the relative benefits of visual and auditory feedback, respectively.
Baram and Lenger’s finding that auditory feedback or visual feedback results in better learning in children with CP than in TD children [Citation31] is remarkable. Are children with CP somehow better in using these feedback forms for task acquisition in this particular case? The explanation may be quite simple since this study examined a gait task; and where children with CP often have considerable room for improvement in their gait pattern, the gait pattern of TD children is arguably already quite close to optimal. The larger improvement of the CP group may thus not be fully attributable to the modality of the feedback, but rather to the relative room for improvement in the given task. To attribute differences in learning effects to the feedback that is given, the task that is practiced should be relatively novel for all groups that are being studied.
It is noteworthy that effect sizes were considerably larger in the auditory feedback study of Hamed and Abd-elwahab [Citation33] than in the studies of Hussein et al. [Citation37] and Baram and Lenger [Citation31]. The first two studies implemented a music-based auditory feedback paradigm, whereas Baram and Lenger [Citation31] used a simple clicking sound. Indeed, a more comprehensive and rich stimulation is quite enjoyable for children and may have additional motivational value in stimulating their learning compared to the use of plain, isolated auditory cues. Also in other populations, such as stroke, promising results of music-based auditory feedback were reported [Citation49].
Descriptive and prescriptive feedback
Thorpe and Valvano [Citation38] showed that in gait-related task training, children with CP differed in whether prescriptive, descriptive, or no feedback was most beneficial for learning. According to Magill and Anderson [Citation13], these results are similar to findings in able-bodied participants. They argue that the proficiency of the learner is a determining factor for the influence of prescriptive or descriptive feedback and which of the two leads to larger performance improvements. It is likely that this will also be the case for children with CP.
Feedback frequency
As for the findings on frequency of feedback, most of the results of the included studies are in accordance with outcomes of publications on able-bodied populations. Burtner et al. [Citation32] showed that providing feedback after every trial is equally beneficial as providing feedback after 62% of the trials, in a faded manner. Similar effects are observed in TD children and able-bodied young adults [Citation50]. Furthermore, children with CP showed more learning benefits from frequency of 50% compared to a frequency of 100% or 0% [Citation35]. Similar results have been found in TD children, who showed better retention after 50% faded feedback compared to 100% feedback [Citation22].
Even though it seems plausible that children with CP would benefit more from a higher feedback frequency due to their sensorimotor impairments, the results of the included studies showed this is not (always) the case. These findings exemplify that the effects found in these studies might be specific to the complexity of the motor tasks that were used. As Sidaway et al. [Citation51] showed in his study involving TD children, efficacy is determined by an interaction between task complexity and feedback frequency. That is, in case of a complex task, it is more beneficial to provide children with feedback at a high frequency (at 100% of the trials) whereas for a simple task, it is more beneficial to provide feedback with a low frequency (33% of trials). Similar results were found by Fuji et al. [Citation52], where able-bodied participants practicing a complex motor task obtained better learning outcomes in the 100% feedback condition than in the 50% feedback condition. Yet, Hemayattalab and Rostami’s task can be considered complex by use of the defined characteristics of a complex task noted in the methods section: (1) involving two or more degrees of freedom and (2) demanding the acquisition of a multi-limb coordination pattern. Nevertheless, defining a task’s complexity could be done more accurately based on a continuous scale, rather than categorizing tasks as being either complex or simple, in a dichotomous matter. Indeed, it is not difficult to think of tasks that are far more complex (i.e., positioned farther towards the extreme of the spectrum) than the one used by Hemayattalab and Rostami. For tasks that require more complicated coordination patterns, children with CP might show better learning when they receive feedback more frequently. However, none of the articles included in this review investigated the influence of task complexity related to feedback frequency; hence, it is not possible to draw any firm conclusions.
Hemayattalab et al. [Citation36] showed that children with CP benefit more from a self-controlled frequency than from a yoked frequency. Furthermore, the possibility to self-regulate after which trials feedback is given also leads to better learning than when this is regulated by an instructor [Citation40]. Both findings are similar to the results of Janelle et al. [Citation53,Citation54] in able-bodied adults and of Chiviacowsky et al. [Citation55] in able-bodied children. When evaluating these three studies, it is noteworthy that, in the situation where participants could control the feedback frequency, children asked for feedback more often than adults − 35% for children [Citation55] and 9% or 11% for adults [Citation53,Citation54]. And they seem to actually profit from requesting feedback more often, as shown by Chiviacowsky et al. [Citation56]. In this line of logic, one might expect that children with a sensorimotor deficit and a lower amount of movement experience and skill (as is generally the case in children with CP) will show better learning if they ask for feedback more often. Unfortunately, we can neither confirm nor refute this hypothesis on grounds of the current evidence, since Hemayattalab et al. [Citation36] did not report how often the participants with CP asked for feedback.
The findings of studies performed in able-bodied populations are generally confirmed in the included studies that made a direct comparison between children with CP and age-matched TD children. However, Valvano and Newell [Citation39] showed that a 50% frequency was more beneficial for TD participants than for participants with CP. This is an interesting finding for which several explanations are possible. Perhaps the children with CP had reached the ceiling of their capacity and they were unable to improve any further in this task due to physical and neurological constraints, whereas the TD children were not restricted in improving their performance by any such limitations. Alternatively, the frequency is optimal for them, but they are unable to learn as fast as their able-bodied peers and they just need more time to show the same amount of improvement. A third possibility is that a frequency higher than 50% may enable children with CP to improve as much as TD children did with 50%, since they needed compensation for their limited resources for task-intrinsic feedback. A higher frequency, then, might lead to more equal effects for both groups, or even prove more beneficial for children with CP than for TD children. However, the study of Harbourne [Citation34], who provided feedback with a frequency of 75%, showed inconsistent results within the CP group: there was large inter-individual variation between learning curves. This highlights the need for differentiation between skill levels, severity of CP, age, and other possible factors that may account for inter-individual variability. Further study is warranted before firm conclusions can be drawn with regard to the effectiveness of varying feedback frequencies relative to TD children.
Motor learning in absence of augmented feedback
The studies that included a no-feedback practice condition showed that children with CP can improve their performance in dart throwing, as well as their gait characteristics, without any augmented feedback [Citation33,Citation35,Citation40]. In contrast, children were unable to improve their line-tracing task performance in a no-feedback condition [Citation41]. Learning without feedback is only possible if there is sufficient task-intrinsic feedback available that can be used by the child for error detection and improvement of one’s performance. Probably, the dart throwing and gait tasks generate enough sensory information for CP children to adjust their movements and improve their performance, whereas the task-intrinsic feedback of the line-tracing task is limited. However, more recent research has shown that TD children are able to learn a tracing task without any augmented feedback, as are children with DCD [Citation57], which suggests that there is apparently enough task-intrinsic feedback available for both TD children and children with motor learning impairments. The discrepancy between these findings and those in children with CP may be attributable to differences in study design and sensitivity of measurement instruments, but it may also be the case that a tracing task is more difficult for children with CP than it is for TD children and children with DCD.
Limitations of included studies
Due to the heterogeneity of the reviewed studies, it is difficult to draw firm conclusions about the effectiveness of different feedback forms on motor learning in children with CP. Studies varied greatly in motor learning study design, motor tasks employed, reported outcome measures, the way they analyzed and interpreted their outcome measures, and the characteristics of their CP samples. Some studies failed to report important details of their sample, such as type of CP, severity, limbs affected and age range, making it even more difficult to interpret and relate their findings to one another. Overall, CP forms other than spastic hemiplegia were underrepresented in the articles. More research is warranted, especially in participants who are more severely affected.
Four of the studies employed an incomplete motor learning research design (i.e., pre-test-posttest-retention test in a no-feedback condition, ad minimum – a proper design should additionally contain transfer and dual task conditions); three of which did not administer any retention test. Moreover, of the 10 studies, only two administered a transfer test. The relevance of their findings for therapeutic practice is therefore, unfortunately, limited, since the ultimate aim of therapy is to enable the child to retain any acquired improvement and to integrate the learned motor task into their activities of daily living.
An important aspect to mention is that in six of the seven studies that examined unimanual upper extremity movements, children were allowed to perform the task with their less-affected arm. However, children with CP will encounter fewer problems in learning motor tasks that involve the less-affected side since their sensorimotor impairments are not (as) prominent, in contrast to their affected side. They are most likely better able to make use of task-intrinsic feedback when practicing tasks with their less affected side (because of intact sensorimotor pathways) and the relative benefits of augmented feedback are probably small compared to their affected side. This makes the outcomes less relevant for therapeutic practice, where the focus is generally on improving the (more severely) affected side.
Furthermore, the majority of these studies investigated a sample with large variation in age. Effects of the feedback provided, however, may be dissimilar for young children on the one hand and older adolescents on the other. Even so, none of the studies corrected for age or compared individual learning curves between participants on either extreme of the included age spectrum. One study [Citation40] only reported mean and standard deviations of the CP group’s age and not a minimum or maximum, making it tremendously difficult to generalize the results to any CP group. In the same line, some studies investigated a CP group that was very heterogeneous in terms of severity. Since children who are more severely affected by CP show poorer selective motor control [Citation58], the outcomes of motor learning studies investigating feedback effects can vary largely between individual children within the sample. For example, one study’s sample consisted of children with GMFCS level I–IV. This study indeed reports large variability in results of the CP group, with some children scoring within the range of the TD group. In such heterogeneous groups, showing individual learning curves would provide important additional information besides the group-wise comparisons. Moreover, in eight of the studies, GMFCS level was not even reported, making it very difficult to understand to which CP subpopulation the results would apply to.
Moreover, the risk of bias assessment pointed out that half of the studies contained an overall high risk of bias, which was most often a consequence from a high risk of bias in the domain “selection of the reported result”. In this domain, studies were assessed on whether there had been any bias in selecting the result that was reported, according to any pre-specified analysis plan (if existent) and the range of eligible outcome measurements and analysis options [Citation30]. It was expected that this aspect would be better in studies that were published more recently. Regrettably, this was not the case. Specifically, choices in statistical analyses seemed suboptimal in some studies. If learning curves (rather than performance levels) of different groups are of interest, it does not suffice to check differences between both groups for each point in time in isolation. After all, differences in performance level (e.g., between CP and TD group) at any fixed point in time provide no information whatsoever on whether and how much the groups have improved their performance. Rather, changes within groups over two or more time points should be compared between groups. Additionally, not only mean group values but also variance should be reported, as well as effect sizes, to give an estimation for the magnitude of the (significant) differences – this way, information can be provided on the clinical relevance of the effects that were found.
Implications for therapeutic practice
Overall, the evidence gathered supports the expectancy that children with CP generally benefit from augmented feedback provided during or after performing a movement task. Even though they seem capable of learning certain tasks without any augmented feedback, providing such feedback enhances their learning [Citation33,Citation35,Citation40].
Unfortunately, no strong recommendations can be given regarding the relative effectiveness of different feedback forms due to lack of information, heterogeneity, and low study quality. Regarding feedback frequency, however, two important things should be taken into account. Firstly, it is not recommended to provide feedback after every practice trial. Doing so would most likely lead to dependency of the feedback provided [Citation32,Citation35]. Instead, it may be better to let the child regularly perform the task without feedback; this will also unveil the progress the child has made so far in independent performance of the task concerned. Secondly, letting children determine how often and after which trials they want feedback seems the best frequency-reducing strategy, based on the current evidence [Citation36,Citation40].
Finally, it is important to note that learning curves have been shown to vary wildly within a CP group. Even patients who classified within the same category of severity of CP showed dissimilar graphs of progress [Citation38]. Results on group level may therefore not be applicable to individual patients and it is essential to assess a child’s capabilities and needs and to build a fitting support system accordingly, as well as to check their progress regularly and adjust practice paradigms if improvements are not forthcoming.
Strengths and limitations of this review
The conclusions drawn in this review on the effectiveness of any feedback form on motor learning in children with CP should be interpreted with caution, since the amount of evidence is meagre. The restricted number of articles, mediocre quality of evidence and large heterogeneity of the studies has limited the extent to which reliable recommendations can be given for therapeutic practice. Furthermore, a considerable number of the articles included in this review has a questionable risk of bias. They were not removed from the analyses, however, for the reason that removal would shrink the total amount of data to a nearly unserviceable level. Besides, not only are some study results quite aged, the results also fail to cover all types and severity levels within the CP spectrum. The findings of this review can thus not simply be generalized to the entire population of children with CP. Regrettably, quantitative comparison of the studies’ results was not possible due to the divergence of the designs and reported outcome measures.
In comparison to the review recently published by Robert et al. [Citation28], the current review has extended the existing overview of scientific literature by including motor tasks that also involve the lower extremities or the entire body. In addition, four of the articles on upper extremity tasks that were discussed in this paper were not included in the review of Robert et al. In follow-up of the review of Robert et al., this review has taken a critical look at the current state of scientific affairs on the topic of motor learning and feedback in children with CP and placed the relevance of findings in the perspective of therapeutic practice.
Recommendations for future research
First of all, it seems clear that more research of higher quality on the effectiveness of feedback in motor learning for children with CP is vital. So far, no studies have focused on comparisons between KP and KR; error information and information on correct aspects; qualitative and quantitative feedback; and concurrent and terminal feedback. Future studies should address these aspects. Furthermore, study protocols should be established that enable examination of the effects of task complexity on the relative benefits of different forms and frequencies of feedback. Moreover, specific CP subgroups deserve more attention; participants with quadriplegia are underrepresented in the scientific literature on motor learning, as are children with athetoid and dyskinetic types of CP.
Future studies that aim to provide a valuable contribution to the scientific knowledge on the young CP population and well-grounded recommendations for therapeutic practice should bear a number of things in mind. Firstly, comprehensive experimental protocols (i.e., pretest, posttest, retention test, transfer test, dual task condition) provide the most complete view of the learning effects as a result of training a certain motor task. Adopting such a protocol as the standard for motor learning studies’ design would also enable proper (quantitative) comparison of effects of varying feedback forms and frequencies and would help establish evidence-based feedback guidelines for therapists. Secondly, if a CP group is compared to a TD group, the motor task to be trained should encompass enough room for improvement for both groups. It is recommended to choose a task both groups are relative novices in. Thirdly, if the sample consists of participants with hemiplegic CP, the affected side should be involved in the task training. Fourthly, including a practice-only condition (without augmented feedback) will show how meaningful the feedback learning effects are relative to participants’ own ability to learn the task through mere practice (with access to only task-intrinsic feedback). Finally, although group-wise statistical comparisons allow for generalization (at least to some extent), differences in individual learning curves should not be ignored. As the results of this review show, it is possible that subgroups, defined by motor learning abilities, may exist within the CP population. Future research should verify the presence of such subgroups and subsequently investigate factors that determine to which subgroup a patient belongs.
Conclusion
This review has laid bare the lack of high-quality scientific research on the effectiveness of different feedback forms in children with CP. Due to the heterogeneity of the existing studies, it is difficult to draw firm conclusions from the findings.
Overall, the gathered evidence is consistent with the hypothesis that children with CP benefit from augmented feedback in motor learning. Some results suggest that children with CP do not necessarily show optimal learning when provided with a feedback frequency of 100%. Rather, a lower frequency appears to lead to better retention, which is in line with findings in the TD population. These effects may, however, be dependent on the complexity of the practiced motor task.
More high-quality scientific research is needed on this topic. Future studies should include other feedback related topics, such as relative benefits of KP and PR; error information and information on correct aspects; qualitative and quantitative feedback; and concurrent and terminal feedback. Furthermore, they should focus on the influence of task complexity on the relative benefits of different forms and frequencies of feedback.
Acknowledgements
The authors thank Annemieke Wargers for helping with the inclusion and risk of bias assessment of the articles.
Disclosure statement
The authors report no conflicts of interest.
References
- Rosenbaum P, Paneth N, Leviton A, et al. A report: the definition and classification of cerebral palsy April 2006. Dev Med Child Neurol Suppl. 2007;109:8–14.
- Mac Keith RC, Polani PE, Kessel L, et al. Cerebral palsy. The Lancet. 1958;271(7027):961–962.
- Keenan MAE, Mehta S, McMahon PJ. Chapter 12. Rehabilitation. In: Skinner HB, McMahon PJ, editors. Current diagnosis & treatment in orthopedics 5th ed. New York (NY): The McGraw-Hill Companies; 2014. p. 531–540.
- Kim H., Shoval HA. Pediatric musculoskeletal medicine. In: Mitra R, editor. Principles of rehabilitation medicine. New York, NY: McGraw-Hill Education; 2019. p. 1005–1028.
- Palisano RJ, Hanna SE, Rosenbaum PL, et al. Validation of a model of gross motor function for children with cerebral palsy. Phys Ther. 2000;80(10):974–985.
- Berger W, Quintern J, Dietz V. Pathophysiology of gait in children with cerebral palsy. Electroencephalogr Clin Neurophysiol. 1982; 53(5):538–548.
- Olney SJ, MacPhail HE, Hedden DM, et al. Work and power in hemiplegic cerebral palsy gait. Phys Ther. 1990;70(7):431–438.
- Giuliani CA. Dorsal rhizotomy for children with cerebral palsy: support for concepts of motor control. Phys Ther. 1991;71(3):248–259.
- Williams HG, Pfeiffer KA, O'Neill JR, et al. Motor skill performance and physical activity in preschool children. Obesity. 2008;16(6):1421–1426.
- Lloyd M, Saunders TJ, Bremer E, et al. Long-term importance of fundamental motor skills: a 20-year follow-up study. Adapt Phys Activ Q. 2014;31(1):67–78.
- van Gorp M, E Roebroeck M, van Eck M, et al. Childhood factors predict participation of young adults with cerebral palsy in domestic life and interpersonal relationships: a prospective cohort study. Disabil Rehabil. 2020;42(22):3162–3171.
- Haibach-Beach PS, Reid G, Collier DH. Motor learning and development. 2nd ed. Champaign (IL): Human Kinetics; 2018. English.
- Magill R, Anderson D. Motor learning and control. New York (NY): McGraw-Hill Publishing; 2010.
- Silverman S, Woods AM, Subramaniam PR. Task structures, feedback to individual students, and student skill level in physical education. Res Q Exerc Sport. 1998;69(4):420–424.
- Carlton L, Proteau L, Elliott D. Vision and motor control. Amsterdam: Elsevier; 1992.
- Zubiaur M, Oña A, Delgado J. Learning volleyball serves: a preliminary study of the effects of knowledge of performance and of results. Percept Mot Skills. 1999;89(1):223–232.
- Selder DJ, Del Rolan N. Knowledge of performance, skill level and performance on the balance beam. Can J Appl Sport Sci. 1979;4(3):226–229.
- Wood CA. Alternate forms of knowledge of results: Interaction of augmented feedback modality on learning [gedruckte ressource]. [alternative formen der ergebniskenntnis: Interaktion der modalitaet des verstaerkten feedbacks auf das lernen]. J Hum Move Stud. 1992;22(6):213–230.
- Kovacs AJ, Buchanan JJ, Shea CH. Impossible is nothing: 5:3 and 4:3 multi-frequency bimanual coordination. Exp Brain Res. 2010;201(2):249–259.
- Wulf G, Shea C, Lewthwaite R. Motor skill learning and performance: a review of influential factors. Med Educ. 2010;44(1):75–84.
- Vander Linden DW, Cauraugh JH, Greene TA. The effect of frequency of kinetic feedback on learning an isometric force production task in nondisabled subjects. Phys Ther. 1993;73(2):79–87.
- Winstein CJ, Schmidt RA. Reduced frequency of knowledge of results enhances motor skill learning. J Exp Psychol. 1990;16(4):677–691.
- RAS. Frequent augmented feedback can degrade learning: Evidence and interpretations. In: Requin JSGE, editor. Tutorials in motor neuroscience. NATO ASI series (series D: Behavioural and social sciences). Vol. 62. Dordrecht: Springer; 1991. p. 59–76.
- Sigrist R, Rauter G, Riener R, et al. Augmented visual, auditory, haptic, and multimodal feedback in motor learning: a review. Psychon Bull Rev. 2013;20(1):21–53.
- Mutsaarts M, Steenbergen B, Bekkering H. Anticipatory planning deficits and task context effects in hemiparetic cerebral palsy. Exp Brain Res. 2006;172(2):151–162.
- Verschueren SMP, Swinnen SP, Dom R, et al. Interlimb coordination in patients with Parkinson’s disease: motor learning deficits and the importance of augmented information feedback. Exp Brain Res. 1997; 113(3):497–508.
- Guadagnoli MA, Leis B, Van Gemmert AW, et al. The relationship between knowledge of results and motor learning in parkinsonian patients. Parkinsonism Relat Disord. 2002;9(2):89–95.
- Robert MT, Sambasivan K, Levin MF. Extrinsic feedback and upper limb motor skill learning in typically-developing children and children with cerebral palsy: review. Restor Neurol Neurosci. 2017;35(2):171–184.
- Moher D, Liberati A, Tetzlaff J, PRISMA Group, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
- Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898
- Baram Y, Lenger R. Gait improvement in patients with cerebral palsy by visual and auditory feedback. Neuromodulation. 2012;15(1):48–52; discussion 52.
- Burtner PA, Leinwand R, Sullivan KJ, et al. Motor learning in children with hemiplegic cerebral palsy: feedback effects on skill acquisition. Dev Med Child Neurol. 2014;56(3):259–266.
- Hamed NS, Abd-Elwahab MS. Pedometer-based gait training in children with spastic hemiparetic cerebral palsy: a randomized controlled study. Clin Rehabil. 2011;25(2):157–165.
- Harbourne RT. Accuracy of movement speed and error detection skills in adolescents with cerebral palsy. Percept Mot Skills. 2001;93(2):419–431.
- Hemayattalab R, Rostami LR. Effects of frequency of feedback on the learning of motor skill in individuals with cerebral palsy. Res Dev Disabil. 2010; 31(1):212–217.
- Hemayattalab R, Arabameri E, Pourazar M, et al. Effects of self-controlled feedback on learning of a throwing task in children with spastic hemiplegic cerebral palsy. Res Dev Disabil. 2013;34(9):2884–2889.
- Hussein ZA, Salem IA, Ali MS. Effect of simultaneous proprioceptive-visual feedback on gait of children with spastic diplegic cerebral palsy. J Musculoskelet Neuron Interact. 2019;19(4):500–506.
- Thorpe DE, Valvano J. The effects of knowledge of performance and cognitive strategies on motor skill learning in children with cerebral palsy. Pediatr Phys Ther. 2002;14(1):2–15.
- Valvano J, Newell KM. Practice of a precision isometric grip-force task by children with spastic cerebral palsy. Dev Med Child Neurol. 1998;40(7):464–473.
- Hemayattalab R. Effects of self-control and instructor-control feedback on motor learning in individuals with cerebral palsy. Res Dev Disabil. 2014;35(11):2766–2772.
- Talbot ML, Junkala J. The effects of auditorally augmented feedback on the eye-hand coordination of students with cerebral palsy. Am J Occup Ther. 1981; 35(8):525–528.
- Baram Y, Aharon-Peretz J, Simionovici Y, et al. Walking on virtual tiles. Neural Process Lett. 2002;16(3):227–233.
- Baram Y, Miller A. Virtual reality cues for improvement of gait in patients with multiple sclerosis. Neurology. 2006;66(2):178–181.
- van Vliet PM, Wulf G. Extrinsic feedback for motor learning after stroke: what is the evidence? Disabil Rehabil. 2006; 28(13-14):831–840.
- Shin J, Chung Y. Influence of visual feedback and rhythmic auditory cue on walking of chronic stroke patient induced by treadmill walking in real-time basis. NRE. 2017;41(2):445–452.
- Cha YJ, Kim JD, Choi YR, et al. Effects of gait training with auditory feedback on walking and balancing ability in adults after hemiplegic stroke: a preliminary, randomized, controlled study. Int J Rehab Res. 2018;41(3):239–243.
- Oscari F, Secoli R, Avanzini F, et al. Substituting auditory for visual feedback to adapt to altered dynamic and kinematic environments during reaching. Exp Brain Res. 2012;221(1):33–41.
- Tarnas J, Stemplewski R, Krutki P. Sex differences in maintaining the requested handgrip force enhanced by auditory or visual feedback. IJERPH. 2020;17(14):5158.
- Chen JL, Fujii S, Schlaug G. The use of augmented auditory feedback to improve arm reaching in stroke: a case series. Disabil Rehabil. 2016;38(11):1115–1124.
- Goh HT, Kantak SS, Sullivan KJ. Movement pattern and parameter learning in children: effects of feedback frequency. Res Q Exerc Sport. 2012;83(2):346–352.
- Sidaway B, Bates J, Occhiogrosso B, et al. Interaction of feedback frequency and task difficulty in children's motor skill learning. Phys Ther. 2012;92(7):948–957.,.
- Fujii S, Lulic T, Chen JL. More feedback is better than less: Learning a novel upper limb joint coordination pattern with augmented auditory feedback. Front Neurosci. 2016;10:251.
- Janelle CM, Kim J, Singer RN. Subject-controlled performance feedback and learning of a closed motor skill. Percept Mot Skills. 1995;81(2):627–634.
- Janelle CM, Barba DA, Frehlich SG, et al. Maximizing performance feedback effectiveness through videotape replay and a self-controlled learning environment. Res Q Exerc Sport. 1997;68(4):269–279.
- Chiviacowsky S, Wulf G, de Medeiros FL, et al. Learning benefits of self-controlled knowledge of results in 10-year-old children. Res Q Exerc Sport. 2008;79(3):405–410.
- Chiviacowsky S, Wulf G, de Medeiros FL, et al. Self-controlled feedback in 10-year-old children: higher feedback frequencies enhance learning. Res Q Exerc Sport. 2008;79(1):122–127.
- Snapp-Childs W, Fath AJ, Watson CA, et al. Training to improve manual control in 7-8 and 10-12 year old children: Training eliminates performance differences between ages. Hum Mov Sci. 2015;43:90–99.
- Cahill-Rowley K, Rose J. Etiology of impaired selective motor control: emerging evidence and its implications for research and treatment in cerebral palsy. Dev Med Child Neurol. 2014;56(6):522–528.