
Abstract
Purpose
To identify determinants of spoken language comprehension (SLC) in children with cerebral palsy (CP).
Materials and methods
Cross-sectional data of 207 children with CP were included: 82 toddlers (18 months–3;11 years), 59 preschool children (4;0–5;11 years), and 66 schoolchildren (6;0–8;11 years), across all Gross Motor Function Classification System (GMFCS) levels. SLC was assessed using the Computer-Based instrument for Low motor Language Testing (C-BiLLT). Potential determinants were retrieved from medical files and through parental questionnaires. Per developmental stage, multivariable regression analyses were used to assess determinants of SLC.
Results
Fifty-nine percent of the children showed below average SLC. Significant determinants for SLC differed per developmental stage. In toddlers: age, motor type, functional communication and speech function (R2 = 0.637); in preschool children: functional communication, speech function and language activities (R2 = 0.820), and in schoolchildren: functional communication, intellectual functioning and arm-hand functioning (R2 = 0.807). For all developmental stages, functional mobility was not a significant determinant.
Conclusions
A large proportion of children with CP across all GMFCS levels have SLC impairments. Findings indicate that SLC is strongly determined by functional communication classified with CFCS. We recommend standardized assessment and monitoring of SLC in all children with CP.
Children across all GMFCS levels can experience difficulties in spoken language comprehension.
At all developmental stages, functional communication (classified with CFCS) is an important determinant of spoken language comprehension.
Standardized assessment and monitoring of spoken language comprehension, language production, speech, and communication of all children with CP, is strongly recommended.
When children show below average performances, especially in spoken language comprehension, intervening with speech and language therapy and guidance for parents, is advised.
IMPLICATIONS FOR REHABILITATION
Introduction
Children with cerebral palsy (CP) often experience impairments that may prevent them from fully developing speech, language, and literacy skills needed for effective communication. Challenges in communication are common in children with CP, occurring in 58–81%, with the highest prevalence in children with the most severe motor limitations [Citation1,Citation2] (levels IV and V of the Gross Motor Function Classification System, GMFCS [Citation3]). Communication challenges are particularly complex because the difficulties may have motor, as well as cognitive-linguistic and social underpinnings [Citation4,Citation5]. It is therefore important to differentiate between speech, cognition, language comprehension, language production, and daily communication when addressing communication functions in children with CP [Citation6–8]. Spoken language comprehension is one of the important determinants of effective communication [Citation9]. Additionally, spoken language comprehension and communication skills are essential for social participation, academic participation and success, and overall improvement of quality of life [Citation10,Citation11]. Awareness of the level of spoken language comprehension and understanding of its determinants is important to be able to provide targeted interventions, aimed at improving participation in daily communication (including the use of augmentative and alternative communication, AAC) [Citation8,Citation12,Citation13].
The International Classification of Functioning, Disability, and Health for children and Youth (ICF-CY) [Citation14] is a dimensional framework to describe the interaction between CP (the health condition), communicative participation, spoken language comprehension, and potential determinants (i.e., influencing factors) [Citation8]. Determinants of spoken language comprehension that have been reported in the literature are mostly in the domain of body functions and structures as defined by the ICF-CY [Citation15]. These determinants concern the neural, motor, and cognitive aspects of CP, e.g., structural brain abnormalities, motor type, motor distribution, intellectual functioning, and speech functions (speaking or not speaking) [Citation15]. In the activities and participation domain, the association of functional mobility with spoken language comprehension in children with CP has been most commonly reported, with better spoken language comprehension in children with better functional mobility [Citation15]. Nevertheless, not all determinants of spoken language comprehension in children with CP have been elucidated. Some important CP-related determinants have not (convincingly) been found to be associated (epilepsy [Citation4,Citation16–18], arm-hand functioning [Citation4,Citation18–21]), or have not been studied at all (speech production [Citation15]). Additionally, to our knowledge, the role of an important determinant of spoken language comprehension in typically developing (TD) children, i.e., language activities, such as singing songs, reading books together, (re)telling stories, and rhyming, has not yet been studied in CP [Citation15].
Valid assessment of spoken language comprehension in children with CP is challenging due to methodological issues [Citation22]. Most standardized language comprehension tests require at least some motor activity for a reliable response (i.e., to manipulate test material) [Citation22]. As a consequence, studies focusing on spoken language comprehension in children with CP often depend on observational tools and parental questionnaires rather than direct assessment tools [Citation15]. Acknowledging the importance of standardized language testing in all children with CP [Citation23], in the past years, much effort has been expended to adapt existing measures. Following the development and implementation of the Computer-Based instrument for Low motor Language Testing (C-BiLLT) [Citation24], valid and reliable standardized assessment of spoken language comprehension became possible in children with CP across a wide range of motor impairments.
To our knowledge, determinants of spoken language comprehension using a valid and standardized language assessment tool have not previously been investigated in a large cohort of children with CP across all GMFCS levels. This study aims to study spoken language comprehension in children with CP across all GMFCS levels and to identify its determinants in the ICF-CY body structures, body functions, and activities and participation domains. We include toddlers, preschool, and schoolchildren (18 months to 8;11 years) to identify specific determinants that can guide speech and language rehabilitation per developmental stage.
Materials and methods
Design and participants
Cross-sectional baseline data were retrieved from a larger data set that was gathered by means of the Cerebral Palsy-Communication and Language Learning (CP-CaLL) project. The CP-CaLL project is a nationwide multi-site prospective longitudinal cohort study investigating the development of spoken language comprehension and its determinants in children with CP in The Netherlands. Three groups representing different developmental stages were discerned, for pragmatic reasons based on the Dutch educational system: toddlers (18 months to 3;11 years); preschool children (4;0 to 5;11 years); and schoolchildren (6;0 to 8;11 years).
Children and their parents were recruited through convenience sampling of rehabilitation and day-care centres throughout The Netherlands from November 2017 to August 2018. Inclusion criteria were (1) a confirmed diagnosis of CP, (2) age between 18 months and 8;11 years, and (3) at least one parent fluent in Dutch. Exclusion criteria were (1) severe auditory problems (hearing threshold of ≥31 dB for the best ear), (2) severe visual problems (<0.3 corrected with spectacles for the best eye), (3) diagnosis of severe cerebral visual impairment (CVI) or cortical blindness, and (4) diagnosis of neurological disorders other than CP.
The Medical Ethical Committee of Amsterdam University Medical Centers, location VUmc, reviewed the study. The committee stated that the Medical Research Involving Human Subjects Act (WMO) does not apply to this study. This study complies with the General Data Protection Regulation (GDPR) and all procedures are performed in accordance with the Helsinki Declaration (updated in 2013). Written informed consent was obtained from the parents/caregivers of the child.
Sample size
An estimated target sample of 210 children, i.e., 70 children per developmental stage, was needed to achieve 80% power at a significance level of α = 0.05 using multivariable regression analysis (10 children per variable, minimum of seven variables) [Citation25].
Procedures
Spoken language comprehension assessment was administered in the child’s educational environment or at their home, by clinically-trained researchers (EV, JG) or a certified speech-language therapist (SLT) from the child’s own rehabilitation or day-care centre. Demographic (age and sex) and clinical data (i.e., motor type, motor distribution, epilepsy, intellectual functioning, speech functions (speaking or non-speaking), classifications of speech production (Viking Speech Scale, VSS [Citation26]), functional communication (Communication Function Classification System, CFCS [Citation27]), arm-hand functioning (Manual Ability Classification System, MACS [Citation28]), and functional mobility (GMFCS [Citation3])) were collected from medical records. Parents completed an online questionnaire via Castor EDC [Citation29] comprising questions of the FOCUS-34 [Citation30] and CPCHILD-DV [Citation31] concerning communication and language activities at home (e.g., the child’s ability to tell stories, without or with the use of AAC). Functional communication and language activities, e.g., the child’s ability to tell a story, are expected to improve when a child becomes older. In typical development, it is not likely that toddlers will obtain the highest functional communication levels and tell stories independently. However, in TD schoolchildren it is to be expected that they reach the highest functional communication levels and can tell stories “almost always without help.” See for an overview of potential determinants included in the study, ordered by ICF-CY level.
Table 1. Potential determinants of spoken language comprehension included in the study, ordered by level of the International Classification of Functioning, Disability, and Health for Children and Youth.
Assessment of spoken language comprehension
The Computer-Based instrument for Low motor Language Testing (C-BiLLT) [Citation24] consists of a pretest and a computer test. The pretest is administered to ensure that the child can communicate a choice between two objects and/or photos, based on object naming. When the pretest is successful, the computer test is administered. The computer test consists of 86 items with increasing difficulty in linguistic complexity, following the spoken language comprehension stages from two-word sentences to compound-complex sentences. The C-BiLLT provides norm data and corresponding percentile scores from the age of 18 months to 6;11 years. For children older than 7 years, test results are expressed as age equivalents based on attained raw scores. The C-BiLLT was initially only validated for children with GMFCS levels IV and V. In the current study, the C-BiLLT was also used for children with GMFCS levels I–III. For validation, the Peabody Picture Vocabulary Test-III-NL [Citation32] and the Dutch Schlichting Test for Language Comprehension (Schlichting Test voor Taalbegrip) [Citation33] were also applied. C-BiLLT raw scores correlate significantly with raw scores of the Peabody Picture Vocabulary Test-III-NL [Citation32] (n = 142; r = 0.835, p = 0.000) and with the Dutch Schlichting Test for Language Comprehension (Schlichting Test voor Taalbegrip) [Citation33] (n = 80; r = 0.807, p = 0.000).
Statistical analysis
Descriptive statistics were used to describe age, sex, potential ICF-CY determinants, and spoken language comprehension scores. Statistical analyses were performed using SPSS version 26.0 [Citation34]. Statistical significance was set at p < 0.05. Missing data were addressed using listwise deletion.
Spoken language comprehension outcomes
Scatterplots were used to investigate the relation between C-BiLLT raw scores by age and VSS, CFCS, MACS, GMFCS levels. Normed C-BiLLT scores were also classified as “below average” (i.e., percentile scores <16 for children younger than 7 years; and raw scores <74 in children older than 7 years) and “average” (i.e., percentile scores ≥16 in children younger than 7 years; and raw scores ≥74 in children older than 7 years). For clinical purposes, the distribution of normed C-BiLLT performances (i.e., below average and average) per determinant was shown per developmental stage, using the Mann–Whitney U test (continuous determinants), Fisher’s Exact test (two categories), and Kruskal–Wallis test (three or more categories).
Determinants of spoken language comprehension per developmental stage
To approach the data of all developmental stages equally, more detailed regression analyses were executed using the C-BiLLT raw scores, since percentile scores (i.e., normed data) are not available for children from the age of 7 years. Univariate linear regression analyses were performed for each of the 12 determinants separately to yield estimates of their impact on spoken language comprehension. To further investigate the role of age in each developmental stage, age was included as a continuous determinant. From these univariate analyses, significant determinants (p < 0.20) were entered in multivariable linear regression models (stepwise forward procedure) ordered by their p-value. A stepwise forward procedure was used to guarantee 80% power at a significance level of α = 0.05. In final models, determinants should have a statistical significance of p < 0.05. Collinearity was checked in the total cohort and per developmental stage, using Pearson’s correlation coefficient (parametric data) and Spearman’s correlation coefficient (non-parametric data); correlation coefficients >0.7 were considered as collinear. All analyses were completed on developmental stages separately.
Results
Participants
A total of 234 potential participants were identified. Parents/caregivers of 207 children [88%; boys (n = 122), girls (n = 85)] gave consent for participation, generating a total cohort representative of children with CP in terms of motor type and GMFCS classification ().
Table 2. Demographic and cerebral palsy-related characteristics of the participants.
Spoken language comprehension outcomes
Test requirements for C-BiLLT were met by all children (100%) in the total cohort. Significant differences in spoken language comprehension were found between developmental stages; C-BiLLT raw scores increased with age (p = 0.000, ). Overall, age was a significant determinant for C-BiLLT score (B = 0.543, p = 0.000; ). Percentages for “average” vs. “below average” C-BiLLT performances varied per developmental stage, with the highest percentage of below average performances seen in the toddler group (). Below average performances occurred at all GMFCS levels (). The majority of the 61 children with epilepsy showed below average spoken language comprehension, as did children with intellectual disabilities and children without speech functions at all developmental stages. VSS level (in preschool and schoolchildren), CFCS, and MACS levels (at all developmental stages) were significantly associated with spoken language comprehension (see also Figures 1S–3S, Online Supplementary Material).
Figure 1. C-BiLLT raw score by age in months, filtered by GMFCS level.
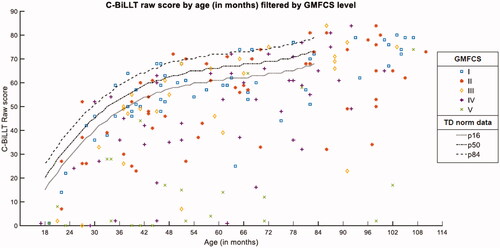
Table 3. C-BiLLT performances per developmental stage and potential determinants.
Table 4. Univariate analysis of determinants per developmental stage of spoken language comprehension (C-BiLLT raw scores).
Determinants of spoken language comprehension per developmental stage
Per developmental stage, determinants of spoken language comprehension as measured by the C-BiLLT were first explored by univariate analyses. Collinearity (ρ > 0.70) was found between age and VSS level (ρ=-0.800) in the total cohort; in toddlers, between CFCS and MACS levels (ρ = 0.808); in preschool children, between VSS levels and speech functions (ρ=-0.766), CFCS (ρ = 0.777) and MACS levels (ρ = 0.728); and in schoolchildren, between VSS and CFCS levels (ρ = 0.701). Both determinants in collinearity pairs were entered in univariate regression analyses, but only one of these determinants could be utilized in the final multivariable regression model. See for univariate regression analyses and for multivariable regression analyses.
Table 5. Multivariable analysis of determinants per developmental stage of spoken language comprehension (C-BiLLT raw scores).
Toddlers: 18 months–3;11 years
Univariate analyses showed p-values <0.20 for motor type (p = 0.015), motor distribution (p = 0.059), intellectual functioning (p = 0.000), speech functions (p = 0.000), CFCS (II: p = 0.544; III: p = 0.748; IV: p = 0.026; V: p = 0.000), MACS (II: p = 0.492; III: p = 0.148; IV: p = 0.110; V: p = 0.000), GMFCS (II: p = 0.146; III: p = 0.434; IV: p = 0.006; V: p = 0.000), language activities—telling stories (with help: p = 0.000; always without help: p = 0.000) and age (p = 0.000). In the final multivariable regression model, motor type (p = 0.011), speech functions (p = 0.000), CFCS (II: p = 0.211; III: p = 0.401; IV: p = 0.296; V: p = 0.002) and age (p = 0.000) were found to be significant determinants (p < 0.05) of spoken language comprehension, together explaining 64% of the variance in C-BiLLT scores (R2 = 0.637). Within-group comparisons demonstrate that non-speaking children, young children, children with non-spastic CP, and children with higher CFCS levels showed poorer spoken language comprehension.
Preschool children: 4;0–5;11 years
Univariate analyses showed p-values <0.20 for motor distribution (p = 0.015), epilepsy (p = 0.000), intellectual functioning (p = 0.000), speech functions (p = 0.000), VSS (II: p = 0.360; III: p = 0.011; IV: p = 0.000), CFCS (II: p = 0.081; III: p = 0.002; IV: p = 0.000; V: p = 0.000), MACS (II: p = 0.484; III: p = 0.034; IV: p = 0.020; p = 0.002), GMFCS (II: p = 0.803; III: p = 0.388; IV: p = 0.071; V: p = 0.000), language activities—telling stories (with help: p = 0.000; always without help: p = 0.000) and sex (p = 0.003). Multivariable regression analysis specified speech functions (p = 0.023), CFCS (II: p = 0.294; III: p = 0.862; IV: p = 0.035; V: n.a.), and language activities—telling stories (with help: p = 0.002; always without help: p = 0.005) as significant determinants (p < 0.05) of spoken language comprehension, together explaining 82% of the variance in C-BiLLT scores (R2 = 0.820). Within-group comparisons demonstrate that non-speaking children, children with higher CFCS levels and children who cannot tell stories (without or with the use of AAC) showed poorer spoken language comprehension.
Schoolchildren: 6;0–8;11 years
Univariate analyses showed p-values <0.20 for motor type (p = 0.164), motor distribution (p = 0.109), epilepsy (p = 0.000), intellectual functioning (p = 0.000), speech functions (p = 0.000), VSS (II: p = 0.340; III: p = 0.000; IV: p = 0.000), CFCS (II: p = 0.011; III: p = 0.021; IV: p = 0.000; V: p = 0.000), MACS (II: p = 0.058; III: p = 0.023; IV: p = 0.000; V: p = 0.008), GMFCS (II: p = 0.443; III: p = 0.742; IV: p = 0.164; V: p = 0.001), language activities—telling stories (with help: p = 0.005; always without help: p = 0.000) and sex (p = 0.038). Intellectual functioning (p = 0.032), CFCS (II: p = 0.092; III: p = 0.434; IV: p = 0.001; V: n.a.), and MACS (II: p = 0.016; III: p = 0.003; IV: p = 0.001; V: p = 0.000) were significant determinants (p < 0.05) of spoken language comprehension in the final multivariable regression model, together explaining 81% of the variance in C-BiLLT scores (R2 = 0.807). Within-group comparisons demonstrate that children with higher CFCS levels, higher MACS levels, and children with intellectual disabilities showed poorer spoken language comprehension.
Discussion
This study describes spoken language comprehension in toddlers, preschool, and schoolchildren with CP, and its significant determinants (classified according to the ICF-CY framework). Spoken language comprehension difficulties are present in a large proportion of children with CP, across developmental stages and across GMFCS levels. Determinants of spoken language comprehension in children with CP differ per developmental stage. In addition to the level of functional communication classified with the CFCS, significant determinants are speech dysfunction (in toddlers and preschool children), poorer quality of speech production classified with VSS (in preschool and schoolchildren), intellectual disability, and in need of help during language activities (in schoolchildren).
Spoken language comprehension outcomes
The majority (60%) of toddlers and preschool children and around half (52%) of the schoolchildren with CP showed below average spoken language comprehension. This finding suggests that below average spoken language comprehension is more common in children younger than 6 years than in schoolchildren. We believe this finding could be explained by an improvement of function in schoolchildren regarding spoken language comprehension. Whether the delays in spoken language comprehension still exist or show the same discrepancy with their TD peers when a child becomes older, is currently investigated in the longitudinal CP-CaLL project including the same cohort. In general, we assume that toddlers and preschool children with CP develop spoken language comprehension at a slower pace than their TD peers, but may catch up during school-age years. These expectations are also supported by earlier studies in children with CP [Citation35,Citation36].
Up to 50% of the children with milder motor impairment (GMFCS I to III) and up to 75% of the children with more severe motor impairment (GMFCS IV and V) showed below average abilities in terms of spoken language comprehension. Our finding that a large part of the children at GMFCS level I to III also show below average spoken language comprehension, emphasizes the importance of paying attention to both expressive and receptive language—also in those children with milder motor impairments.
Determinants of spoken language comprehension per developmental stage
Motor type
The motor type was found to be an important determinant of spoken language comprehension in toddlers. In this developmental stage, children with dyskinetic CP showed poorer spoken language comprehension than children with spastic CP. By contrast, in an earlier study of children aged 2–12 years with GMFCS levels IV and V, spoken language comprehension was found to be superior in children with dyskinetic CP [Citation18]. Additional analyses in our cohort of schoolchildren at level GMFCS IV–V (data not shown) showed a significant difference between children with spastic and dyskinetic CP, in which children with a dyskinetic CP show higher spoken language comprehension scores. Other studies that included all GMFCS levels did not report an association between motor type and spoken language comprehension [Citation13,Citation14,Citation33,Citation34]. These contrasting findings may, at least in part, be due to the dominant motor type not fully being determined in toddlers with CP [Citation37].
Speech functions and speech production
In toddlers and preschool children with CP, speech (dys)function was found to be an important determinant of spoken language comprehension. This finding is in line with an earlier study, which found non-speaking children to be more at risk for poor spoken language comprehension than speaking children [Citation38]. Non-speaking children tend to receive less language input from their communication partners than their speaking peers [Citation39], potentially threatening their spoken language comprehension [Citation40]. On the other hand, non-speaking children with CP can develop spoken language comprehension at the same level as their typically developing peers [Citation18]. In line with earlier findings [Citation9], in preschool and schoolchildren quality of speech production (classified with VSS) was not a significant determinant of spoken language comprehension. However, in our study, VSS and speech functions, and VSS and CFCS, respectively, were highly correlated in preschool and schoolchildren. So it is more likely to conclude that spoken language comprehension is associated with all aspects of effective communication.
Intellectual functioning
In schoolchildren with CP, intellectual disability (IQ<70) appeared to be one of the important determinants of poor spoken language comprehension in the final multivariable regression model, a finding that corresponds with earlier studies [Citation5,Citation16,Citation36]. However, this finding needs to be addressed more comprehensively, as data on intellectual functioning in our study were available in only a subset of children (n = 115) and IQ outcomes were extracted from medical files, with various types of intelligence assessment measures, and heterogeneous reporting of test results. Following the ICF-CY, spoken language comprehension is described as specific cognitive functions of language, in the body functions domain [Citation14]. Intellectual functioning and spoken language comprehension are strongly intertwined [Citation5,Citation16,Citation21,Citation36,Citation41,Citation42]. However, in younger children with CP (toddlers and preschool children), the final multivariable regression models showed that other determinants seem to affect spoken language comprehension (e.g., speech functions, age, communication). We assume that the effect of intellectual functioning is more observable in schoolchildren since scholastic skills (e.g., technical and comprehensive reading, writing) become more present and required for overall functioning at this developmental stage.
Functional mobility
Although functional mobility (classified with GMFCS) was identified in the univariate analyses as a significant determinant for spoken language comprehension, this was not the case in the multivariable models. Multiple studies that included children across all GMFCS levels, without intellectual disability, have shown that children with CP develop adequate receptive communication, despite limitations in motor capacity and activity performance [Citation2,Citation36]. It is important to note that these studies did not specifically study spoken language comprehension, but used the Vineland Adaptive Behaviour Scale (VABS) as a measure of adaptive functioning, with communication as one of the important domains. The VABS is based on parental reporting of behaviour observed in a natural context but involves the risk of not detecting more complex linguistic comprehension skills that might have been identified using direct language assessments, such as the C-BiLLT [Citation17,Citation36]. In the present study, measuring spoken language comprehension using a direct language assessment showed that the level of functional mobility is not a distinctive determinant in the final regression models for spoken language comprehension, as found in earlier research [Citation35]. It showed that children with higher GMFCS levels are not specifically prone to impaired spoken language comprehension, but also children with lower GMFCS levels could be at risk for below average spoken language comprehension. In addition, in the present study, we used a direct language assessment in which all children with CP were able to answer the questions independently. As a result, it was possible to achieve a more representative sample of children with CP with regard to the severity in terms of CP-related characteristics at all developmental stages than in previous studies [Citation2,Citation5,Citation16,Citation17,Citation19,Citation21,Citation36].
Language activities and functional communication
The associations between spoken language comprehension, a child’s ability to tell stories (language activities) and functional communication (classified with CFCS) are in line with expectations. After all, language and communication are strongly intertwined skills. In addition, language activities and functional communication both depend on more than cognition alone; social skills are also important. Language activities become more important and develop further in preschool children, and play an essential role in language learning in the educational environment of the child [Citation43]. The multivariable role of language activities in preschool children with CP is, therefore, more likely due to developmental factors [Citation44,Citation45] rather than CP-related factors. In current speech and language therapy practice, communicative skills are considered a very important condition for the development of language [Citation46]. Children with poor communication skills experience greater challenges when reacting or responding to communicative and language input [Citation6]. Consequently, the development of spoken language comprehension may be more demanding for children with both cognitive and social difficulties [Citation39].
Epilepsy
Comparing distributions of children showing average vs. below average spoken language comprehension abilities, epilepsy appeared to be a discriminative univariate determinant in preschool and schoolchildren. As previously reported, speech functions and intellectual functioning were stronger determinants for spoken language comprehension than epilepsy [Citation4,Citation16–18]. Since a majority of children with CP suffer from epilepsy, overall functioning cannot be seen as completely independent of epilepsy. While epilepsy did not show collinearity with other determinants (ρ > 0.70), epilepsy was significantly correlated with intellectual functioning, speech functions and speech production, functional communication, functional mobility, arm-hand functioning, and language activities (i.e., telling stories) in the total cohort (data not shown). Although it is of interest to investigate the role of single determinants (e.g., epilepsy), to understand the complex interplay between determinants a multivariable approach is required [Citation47]. Moreover, current epilepsy treatments, such as anti-epileptic drugs and surgery are effective, with ∼70% of the patients being seizure-free [Citation48]. When children do not suffer from epileptic seizures anymore, epilepsy seems no longer to significantly influence daily functioning and spoken language comprehension [Citation4,Citation9,Citation16,Citation49].
Age and sex
Variation in age was only found to be important in the toddler stage. This requires more in-depth research, with a focus on the linguistic aspects of language development. A possible explanation could be that, as in typical development, language comprehension develops rapidly in the first years of life but due to restrictions in motor development and cognition may be compromised in children with CP as they grow older. Limited access and possibilities for interaction with the social and educational environment may jeopardize the development of more complex comprehension skills [Citation4]. Sex did not appear in multivariable models for any developmental stage. Similar results were reported in a recent study where sex was a weak determinant for speech and communication performance at 5 years of age in children with CP [Citation9].
Arm-hand functioning
In schoolchildren, arm-hand functioning (classified using MACS) was significantly associated with spoken language comprehension. This is an interesting finding, with likely neuroanatomical underpinnings. In young TD children, arm-hand functioning was found to be strongly related to cognitive skills, more than, for example, gross motor skills [Citation50]. Previous research in children with CP also found an important relationship between cognition and arm-hand functioning [Citation16]. A potential explanation for these findings might be the close neuroanatomical relation between the cortical motor areas for hand and face, and cross-communication between dorsal and ventral visual streams including one of the major language pathways [Citation51]. In view of the interaction between cognition and language, it is not unexpected that arm-hand functioning is stronger associated with speech production and communication than functional mobility [Citation9].
Strengths and limitations
The results of this study should be interpreted in light of some limitations. Although the target sample size was not reached at each developmental stage (i.e., preschool children and schoolchildren), we wanted to assure that the sample sizes did not affect the results of the present study. Therefore, a stepwise forward method was used to yield a reliable multivariable regression analysis at all developmental stages. In the total cohort, a relatively small number of children were at GMFCS level V. Although the proportion of children at GMFCS level V is representative of the total population of children with CP [Citation52], this might hamper the intended longitudinal follow-up and in-depth analysis of spoken language comprehension development in these children.
Conclusions and clinical implications
In conclusion, a large proportion of children with CP across all GMFCS levels have spoken language comprehension impairments. Functional communication (classified using CFCS) is relevant for spoken language comprehension across all developmental stages. Other determinants of spoken language comprehension differ between developmental stages. Whereas motor type and age seem relevant in toddlers, language activities, arm-hand functioning and intellectual functioning are particularly determinative at later ages. Considering that typical language comprehension develops fast in the first years of life, it is of utmost importance to engage children with CP in communication situations early, to expose them to language input, and to stimulate spoken language comprehension as much as possible. Moreover, given the large proportion of children across all GMFCS levels that have spoken language comprehension impairments, we recommend that children of all GMFCS levels should be assessed and monitored, at least once a year to every six months in toddlers, by an experienced SLT for spoken language comprehension, language production, speech, and communication. When children show below average performances, especially in spoken language comprehension, intervening with speech and language therapy including guidance for parents, is strongly recommended.
2022-03-16_T0_article_disreh_supplementalfile_figure3s_color.pdf
Download PDF (237.5 KB)2022-03-16_T0_article_disreh_supplementalfile_figure2s_color.pdf
Download PDF (65.6 KB)2022-03-16_T0_article_disreh_supplementalfile_figure1s_color.pdf
Download PDF (37.9 KB)Acknowledgements
We thank the participants, their parents, and the speech-language therapists involved in the study. We recognize Chantal Meerding and Karen van Meeteren from Stichting OuderInzicht for their valuable input.
Disclosure statement
The authors have stated that they had no financial or non-financial competing interests.
Data availability statement
The data that support the findings of this study are available from the corresponding author (EV), upon reasonable request.
Additional information
Funding
References
- Mei C, Fern B, Reilly S, et al. Communication behaviours of children with cerebral palsy who are minimally verbal. Child Care Health Dev. 2020;46(5):617–626.
- Voorman JM, Dallmeijer AJ, Van Eck M, et al. Social functioning and communication in children with cerebral palsy: association with disease characteristics and personal and environmental factors. Dev Med Child Neurol. 2009;52(5):441–447.
- Palisano R, Rosenbaum P, Walter S, et al. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. 1997;39(4):214–223.
- Geytenbeek JJM, Heim MJM, Knol DL, et al. Spoken language comprehension of phrases, simple and compound-active sentences in non-speaking children with severe cerebral palsy. Int J Lang Commun Disord. 2015;50(4):499–515.
- Mei C, Reilly S, Reddihough D, et al. Language outcomes of children with cerebral palsy aged 5 years and 6 years: a population-based study. Dev Med Child Neurol. 2016;58(6):605–611.
- Geytenbeek J. Differentiating between language domains, cognition, and communication in children with cerebral palsy. Dev Med Child Neurol. 2016;58(6):e536.
- Pennington L. Speech, language, communication, and cerebral palsy. Dev Med Child Neurol. 2016;58(6):534–535.
- Simeonsson RJ, Björck-Åkessön E, Lollar DJ. Communication, disability, and the ICF-CY. Augment Altern Commun. 2012;28(1):3–10.
- Pennington L, Dave M, Rudd J, et al. Communication disorders in young children with cerebral palsy. Dev Med Child Neurol. 2020;62(10):1161–1169.
- Raghavendra P, Olsson C, Sampson J, et al. School participation and social networks of children with complex communication needs, physical disabilities, and typically developing peers. Augment Altern Commun. 2012;28(1):33–43.
- Sevcik RA. Comprehension: an overlooked component in augmented language development. Disabil Rehabil. 2006;28(3):159–167.
- Light J. “Communication is the essence of human life”: reflections on communicative competence. Augment Altern Commun. 1997;13(2):61–70.
- Light J, Mcnaughton D. Designing AAC research and intervention to improve outcomes for individuals with complex communication needs. Augment Altern Commun. 2015;31(2),85-96.
- World Health Organization. International classification of functioning, disability, and health: children & youth version: ICF-CY. Geneva (Switzerland): World Health Organization; 2007.
- Vaillant E, Geytenbeek JJM, Jansma EP, et al. Factors associated with spoken language comprehension in children with cerebral palsy: a systematic review. Dev Med Child Neurol. 2020;62(12):1363–1373.
- Choi JY, Choi YS, Park ES. Language development and brain magnetic resonance imaging characteristics in preschool children with cerebral palsy. J Speech Lang Hear Res. 2017;60(5):1330–1338.
- Coleman A, Weir KA, Ware RS, et al. Relationship between communication skills and gross motor function in preschool-aged children with cerebral palsy. Arch Phys Med Rehabil. 2013;94(11):2210–2217.
- Geytenbeek JJM, Vermeulen RJ, Becher JG, et al. Comprehension of spoken language in non‐speaking children with severe cerebral palsy: an explorative study on associations with motor type and disabilities. Dev Med Child Neurol. 2015;57(3):294–300.
- Chen K-H, et al. Follow-up of developmental profiles in children with spastic quadriplegic cerebral palsy. Chang Gung Med J. 2009;32(6):628–635.
- Lee Y-C, Wu C-Y, Liaw M-Y, et al. Developmental profiles of preschool children with spastic diplegic and quadriplegic cerebral palsy. Kaohsiung J Med Sci. 2010;26(7):341–349.
- van der Heijden-Maessen H, Lankhorst GJ. The prevalence of speech and language disorders among children with hemiplegic cerebral palsy. J Rehabil Sci. 1990;3:3–6.
- Geytenbeek J, Harlaar L, Stam M, et al. Utility of language comprehension tests for unintelligible or non-speaking children with cerebral palsy: a systematic review. Dev Med Child Neurol. 2010;52(12):e267–e277.
- Kerr C, Shields N, Quarmby L, et al. Supports and barriers to implementation of routine clinical assessment for children with cerebral palsy: a mixed-methods study. Disabil Rehabil. 2018;40(4):425–434.
- Geytenbeek JJ, Mokkink LB, Knol DL, et al. Reliability and validity of the C-BiLLT: a new instrument to assess comprehension of spoken language in young children with cerebral palsy and complex communication needs. Augment Altern Commun. 2014;30(3):252–266.
- Cohen J. Statistical power analysis for the behavioral sciences. London (UK): Academic Press; 2013.
- Pennington L, Virella D, Mjøen T, et al. Development of the Viking speech scale to classify the speech of children with cerebral palsy. Res Dev Disabil. 2013;34(10):3202–3210.
- Hidecker MJC, Paneth N, Rosenbaum PL, et al. Developing and validating the communication function classification system for individuals with cerebral palsy. Dev Med Child Neurol. 2011;53(8):704–710.
- Eliasson A-C, Krumlinde-Sundholm L, Rösblad B, et al. The manual ability classification system (MACS) for children with cerebral palsy: scale development and evidence of validity and reliability. Dev Med Child Neurol. 2006;48(7):549–554.
- Castor EDC. Castor electronic data capture. Amsterdam; 2019. Available from: https://castoredc.com
- Oddson B, Thomas-Stonell N, Robertson B, et al. Validity of a streamlined version of the focus on the outcomes of communication under six: process and outcome. Child Care Health Dev. 2019;45(4):600–605.
- Zalmstra TA, Elema A, Boonstra AM, et al. Validation of the Caregiver Priorities and Child Health Index of Life with Disabilities (CPCHILD) in a sample of Dutch non-ambulatory children with cerebral palsy. Disabil Rehabil. 2015;37(5):411–416.
- Dunn LM. Peabody picture vocabulary Test-III-NL. Amsterdam: Pearson Assessment and Information B.V.; 2005.
- Schlichting LH. Schlichting test voor Taalbegrip. Houten: Bohn Stafleu van Loghum; 2010.
- IBM SPSS statistics for windows. Armonk (NY): IBM Corp; 2019.
- Tan SS, van Gorp M, Voorman JM, et al. Development curves of communication and social interaction in individuals with cerebral palsy. Dev Med Child Neurol. 2020;62(1):132–139.
- Vos RC, Dallmeijer AJ, Verhoef M, et al. Developmental trajectories of receptive and expressive communication in children and young adults with cerebral palsy. Dev Med Child Neurol. 2014;56(10):951–959.
- te Velde A, et al. Early diagnosis and classification of cerebral palsy: an historical perspective and barriers to an early diagnosis. J Clin Med. 2019;8(10):1599.
- Hustad KC, Sakash A, Broman AT, et al. Longitudinal growth of receptive language in children with cerebral palsy between 18 months and 54 months of age. Dev Med Child Neurol. 2018;60(11):1156–1164.
- Pennington L, McConachie H. Interaction between children with cerebral palsy and their mothers: the effects of speech intelligibility. Int J Lang Commun Disord. 2001;36(3):371–393.
- Vygotsky LS. Thought and language. Cambridge (MA): MIT Press; 2012.
- Bishop DV, Brown BB, Robson J. The relationship between phoneme discrimination, speech production, and language comprehension in cerebral-palsied individuals. J Speech Hear Res. 1990;33(2):210–219.
- Pirila S, van der Meere J, Pentikainen T, et al. Language and motor speech skills in children with cerebral palsy. J Commun Disord. 2007;40(2):116–128.
- Stadler MA, Ward GC. Supporting the narrative development of young children. Early Childhood Educ J. 2006;33(2):73–80.
- Applebee A. The child's concept of story: ages two to seventeen. Chicago (IL): University of Chicago Press; 1978.
- Morrow LM. Retelling stories: a strategy for improving young children's comprehension, concept of story structure, and oral language complexity. Element School J. 1985;85(5):647–661.
- Pennington L, Goldbart J, Marshall J. Speech and language therapy to improve the communication skills of children with cerebral palsy. Cochrane Database Syst Rev. 2004;2004(3):CD003466.
- Sellier E, Surman G, Himmelmann K, et al. Trends in prevalence of cerebral palsy in children born with a birthweight of 2,500 g or over in Europe from 1980 to 1998. Eur J Epidemiol. 2010;25(9):635–642.
- Barba C, Cross JH, Braun K, et al. Trends in pediatric epilepsy surgery in Europe between 2008 and 2015: country‐, center‐, and age‐specific variation. Epilepsia. 2020;61(2):216–227.
- Stadskleiv K, Jahnsen R, Andersen GL, et al. Neuropsychological profiles of children with cerebral palsy. Dev Neurorehabil. 2018;21(2):108–120.
- Grissmer D, Grimm KJ, Aiyer SM, et al. Fine motor skills and early comprehension of the world: two new school readiness indicators. Dev Psychol. 2010;46(5):1008–1017.
- Budisavljevic S, Dell'Acqua F, Castiello U. Cross-talk connections underlying dorsal and ventral stream integration during hand actions. Cortex. 2018;103:224–239.
- Smithers‐Sheedy H, et al. A special supplement: findings from the Australian Cerebral Palsy Register, birth years 1993 to 2006. Dev Med Child Neurol. 2016;58:5–10.