
Abstract
Purpose
To explore the acceptability and potential efficacy of orthotic shorts in people with multiple sclerosis.
Materials and methods
This mixed-methods, cross-over study utilised qualitative data to investigate acceptability, including perceived effectiveness. Quantitative data included wear times, self-selected walking speed, spatiotemporal gait parameters, and participant-perceived walking ability. Fifteen participants were assessed with and without two pairs of custom-made shorts: one designed as an orthotic and a second looser pair. Each were worn at home for two weeks. Semi-structured interviews were conducted at the first and final appointments. Quantitative data were analysed using Cohen’s d; qualitative analysis used a thematic framework. A triangulation protocol integrated qualitative and quantitative data.
Results
Orthotic shorts were acceptable to most users who described improved control, stability, and function. Where shorts were less acceptable, this was due to restriction of hip flexion or appearance. Effect sizes were in the moderate category for participant-perceived walking ability and for those spatiotemporal gait parameters that reflect mediolateral stability. Small effect sizes were seen for walking speed and related spatiotemporal parameters, such as step length.
Conclusion
Orthotic shorts are acceptable and potentially efficacious for improving walking, stability, and function in people with multiple sclerosis. Further research and design development are warranted.
Orthotic shorts are a type of fabric orthosis that have not been previously researched but might assist pelvic stability.
Orthotic shorts appear to be acceptable to those people with multiple sclerosis who perceive themselves to be unstable around the trunk and hips.
Orthotic shorts might improve gait stability and self-perceived walking ability.
Implications for rehabilitation
Introduction
An estimated 76% of people with multiple sclerosis (PwMS) complain of mobility problems [Citation1] and 50–70% report that walking is the most challenging aspect of multiple sclerosis (MS) that they face [Citation2]. Walking ability predicts employment status and the need for caregiver support and healthcare resources [Citation2,Citation3]. PwMS have a slower gait, a wider base of support and more variability in their spatiotemporal gait parameters than non-neurologically impaired people [Citation4]. As a result of different patterns of neurological damage, gait impairment presents differently across different PwMS [Citation5].
Orthotic shorts are a type of fabric orthosis, designed to support the hips and lower trunk. Fabric orthoses are made from elasticated fabrics. They are suggested to improve stability, proprioceptive awareness and posture via compression and directional support [Citation6]. Fabric orthoses may be helpful for PwMS because these proposed benefits might compensate for muscle weakness and the slowed, diminished sensory feedback found in MS [Citation7,Citation8]. Orthotic shorts might be beneficial in MS because hip and pelvic instability appear to be common gait problems [Citation9]. In addition, the elasticity of close-fitting shorts has been shown to increase flexion and extension torque at the end of range of hip extension and flexion, respectively [Citation10]. This could provide assistance to swing phase and forward propulsion.
Very little previous research has been conducted into the use of fabric orthoses [Citation11]. Much of the previous research investigated the longer term training effects of orthoses rather than the direct impact on movement control [Citation11], the so-called “direct orthotic effect” [Citation12]. Only two previous studies have investigated proximal orthoses in adults with neurological conditions. Serrao et al. [Citation13] investigated the effect of a short suit, covering shoulders to above the knee, on gait stability in people with degenerative cerebellar ataxia. They compared gait without the suit at baseline, with gait whilst wearing the suit following a one-month period of regular use. They found decreased range of motion at the trunk and pelvis and a decrease in stride time variability, but were unable to determine whether this was a training effect or an orthotic effect. Direct orthotic effect is likely to be important because an orthosis seems unlikely to have a training effect without a direct orthotic effect. Furthermore, we had conducted earlier qualitative research, with a different participant group, that suggested that users are more likely to find an orthotic acceptable if they perceive it to be effective on first use [Citation14]. Only one previous study [Citation15] has investigated the direct orthotic effects of a proximal fabric orthosis in adults. Maguire et al. [Citation15] investigated Theratogs, a fabric orthosis where an elasticated base layer is supplemented with inelastic strapping, to support pelvic stability in stroke survivors. They found small increases in gait speed and hip abductor activity with the Theratogs, although temporal asymmetry increased with more time spent on the non-hemiplegic leg. No previous research has investigated the effectiveness of orthotic shorts, although these may be easier to don and doff than a suit or Theratog.
The Medical Research Council guidelines for Developing a Complex Intervention [Citation16] suggest that early feasibility and pilot work should contribute to intervention development. Feasibility studies include assessment of acceptability and limited efficacy testing, which is particularly important where no previous research exists [Citation17]. Acceptability has been defined as “a multi-faceted construct that reflects the extent to which people delivering or receiving a healthcare intervention consider it to be appropriate, based upon anticipated or experienced cognitive and emotional responses to the intervention” [Citation18, p. 1]. Acceptability of assistive devices influences effectiveness because an unacceptable device will not be used [Citation19,Citation20]. There is widespread agreement that adherence to any healthcare advice, including assistive device use, is influenced by important psychosocial aspects [Citation19–21]. These include users’ feelings and beliefs and social influences on behaviour [Citation19–21]. Mixed-methods research is required to understand these elements.
This study aimed to explore whether orthotic shorts would be acceptable to PwMS and to estimate their potential efficacy.
Materials and methods
Study design
This was an exploratory, descriptive feasibility study employing a convergent, parallel mixed-methods cross-over design.
This study was approved by the National Research Ethics Service Committee for Leeds East in May 2017 and the Health Research Authority in December 2017. The trial protocol is available at Clinical Trials.gov (Ref: NCT03164031).
Participants
Participants were recruited through a local NHS Trust, MS Therapy Centre and via a protocol on the Clinical Trials.gov webpage. Eligibility criteria were diagnosed with MS of any type; had no relapses in the previous four weeks or commenced any new drug therapies in the previous three months; self-identified as having difficulty walking with a feeling of instability around the hips or lower trunk; be able to walk for at least 2 min and have no skin or circulatory problems that might preclude wearing tight clothing. Criteria were deliberately inclusive to enable us to explore clinical features that might influence acceptability and efficacy.
A sample size of sixteen had been set a priori. This was considered to be an adequate sample size to achieve representation across genders, motor impairments, age, and MS type and to obtain adequate data on potential efficacy [Citation22].
Intervention
Each participant trialled two pairs of shorts, custom-made by a company who are specialists in design and manufacture of fabric orthoses. One pair was designed to be “orthotic” (see ). These were constructed from a base layer that fitted snugly and provided some compression, plus added panelling. Panels were constructed from elastic material, orientated such that directional forces (1) provided compression around the pelvis and (2) facilitated external rotation and extension of the hips. Participants were provided with one of two different designs of orthotic shorts: “standard” or “abduction assist.” “Abduction assist” shorts included additional panelling intended to abduct the hips. All shorts extended down to approximately 4 cm above the knee and were waist high or extended upwards to include the lumbar area. Participants’ gait was observed by the first author (NS) and a representative from the orthotics company to determine whether to include abduction assistance and lumbar support. If participants appeared to have difficulty maintaining alignment between their trunk and pelvis, the lumbar support was included. If participants appeared to have a narrow step width, then “abduction assistance” was provided. Participants chose the colour of their shorts, presence or absence of side zips and presence or absence of a toileting hole. Base layer and panels were the same colour to minimise visible differences between the two pairs of shorts provided.
Figure 1. Image of orthotic shorts.

The second pair of shorts was originally conceived as a placebo but are referred to as “baselayer” shorts because, as will be discussed later, their effectiveness as a placebo is uncertain. These consisted of the base layer fabric only and were a slightly larger fit than the orthotic shorts.
Pressure beneath the shorts was assessed over the left gluteus maximus muscle using a Kikuhime pressure monitor, which is commonly used for measuring pressure beneath compression garments [Citation23]. Pressure applied by the garment provides some estimate of how restrictive the orthosis is. Measuring pressure is recommended because physiological effects have been found to vary with pressure applied [Citation11]. Pressure beneath the shorts ranged from 2 to 6 mmHg for the baselayer shorts and 6–13 mmHg for the orthotic shorts. The fit was assessed by the orthotics company representative and adjusted where required. The fit was considered to be equally snug between the two pairs of shorts.
Procedure
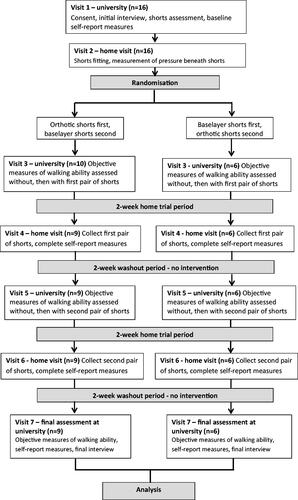
All participants trialled both orthotic and baselayer shorts, one pair at a time. shows an overview of the study design. Participants’ walking ability was measured without and then with the shorts, which were then taken home for a two-week trial. Participants were asked to gradually increase the time they wore the shorts each day, up to 14 h a day and kept a diary of wear times and experiences they felt were important. After each two-week home trial, the first author (NS) visited the participants and took the shorts away. There was then a gap of two weeks before walking ability was reassessed to determine baseline stability. The final interview took place on the final appointment. Participants were given the option of keeping one or both pairs of shorts after the study.
Figure 2. Overview of study design.
Randomisation and assessor blinding
The first author (NS) acted as Principal Investigator and assessor. A colleague allocated participants to the order in which they would test their shorts using a blocked randomisation schedule designed to counterbalance order of testing. Unfortunately, there was an error in using the schedule, meaning that ten participants trialled the orthotics shorts first. Participants changed into their allocated shorts behind a screen and replaced their top clothing, to blind the assessor as to which shorts were being tested.
Qualitative data collection
Qualitative data were collected using individual semi-structured interviews at the first and final study visits. The first interview lasted an average of 23 min (range 10 to 38 min) and explored participants’ motivations for joining the study, their current daily activities, challenges, previous orthotic experiences, and expectations of the shorts. The final interview lasted an average of 44 min (range 29 to 75 min) and explored participants’ experiences with the shorts. If participants chose to keep their shorts, they were asked for their reasoning and plans for future use. The second interview included prompts related to that participant’s initial interview and wear diary. All interviews were conducted and transcribed verbatim by the first author (NS).
Measures
Gait was assessed using (1) a GAITRite (CIR Systems, Inc) instrumented walkway for self-selected gait speed and spatiotemporal gait parameters and (2) Opal Sensors (APDM Wearable Technologies), which are a type of Inertial Measurement Unit for assessing trunk and pelvic stability. The 12-item Multiple Sclerosis Walking Scale (MSWS-12) assessed participant-perceived walking ability.
The GAITRite system used was the GAITRite 3.8, comprising a 5.18 m long walkway. The GAITRite provides excellent reliability for assessing most spatiotemporal gait parameters in MS [Citation24]. Because step width is more variable, reliable assessment requires multiple passes of the GAITRite mat [Citation25]. Each participant completed four passes of the mat at each test, providing a mean of 24 steps per test (SD 4.3; range 16–31). Participants were asked to walk at a comfortable but purposeful pace. They commenced walking 2 m before the start of the mat and finished each walk 2 m after the end of the mat. Mean values for gait speed were downloaded from the GAITRite software. Values of step length, step width. and stride time were downloaded for each step or stride and used to calculate means and variability. Variability was expressed as coefficient of variation and standard deviation.
Inertial measurement units are sensors that consist of accelerometers, gyroscopes, and magnetometers. These were attached to the sacrum and to the sternal angle with straps fitted over clothing, plus ankle sensors to detect footfall. Participants walked at a comfortable speed along a 30 m corridor. Trunk and pelvis three-dimensional position data for up to 30 s of steady-state walking were extracted and analysed in order to determine mediolateral 95% sway range [Citation26]. These samples included a mean of 49 steps (SD 11; range 18–65).
The MSWS-12 is the only tool designed specifically to assess participant-perceived walking ability in MS [Citation27]. It asks participants to self-report the degree to which their MS has limited their mobility over the previous two weeks. It has been shown to have strong psychometric properties [Citation27,Citation28]. A change of 11 points is suggested to represent clinically important change [Citation29].
Qualitative data analysis
Data were analysed using Framework Analysis [Citation30,Citation31]. This requires five analysis stages [Citation30,Citation31]: familiarisation, identifying a thematic framework, indexing, charting, and interpretation. Familiarisation involved transcribing the interviews, re-reading, and producing a list of emergent themes. The thematic framework used was the Theoretical Framework of Acceptability (TFA, ) [Citation18], with the construct of “perceived effectiveness” divided into three subthemes, obtained from a previous qualitative fabric orthosis study [Citation14]: “reclaiming my body,” “reclaiming autonomy,” and “managing self-image.” The framework was applied to the data using indexing and charting and progressed through several iterations as codes were renamed and refined by NS and HP. Interpretation involved explicating the meaning of the component constructs of the TFA as reflected in our data.
Table 1. The component constructs of the Theoretical Framework of Acceptability [Citation13].
Credibility of the analysis was optimised by in-depth interviews, prolonged engagement with the transcripts, careful attention to the extent to which the data supported each finding and verification of the final thematic framework and coding by an experienced researcher (HP).
Quantitative data analysis
Tests of normal distribution were performed using the Shapiro-Wilk test. All ratio data was normally distributed except for stride time variability. Effect sizes were used to estimate the magnitude of effect of the shorts on each variable. For all objective measures, effect sizes and mean differences were calculated for the within-day effect of “no shorts” versus “shorts” and the between-day comparison orthotic shorts compared to baselayer shorts. For the MSWS-12, effect sizes were calculated comparing initial baseline to the value at the end of each home trial. For normally distributed, ratio data, Cohen’s d was calculated by dividing the difference between the two conditions by the pooled standard deviation for both shorts conditions. For ordinal and non-normally distributed ratio measures, a non-parametric effect size was calculated by dividing the Z value obtained from the Wilcoxon signed rank test by the square root of the number of observations [Citation32]. Effect sizes around 0.2 were considered to reflect a small effect, around 0.5 a moderate effect and 0.8 and above is considered a large effect [Citation33]. Other inferential analyses were not considered appropriate in a small feasibility study for which no sample size calculation had been performed.
Mixed-methods integration
Integration of key quantitative and qualitative approaches occurred at the stage of interpretation, meaning that qualitative and quantitative data were analysed separately, and key findings compared using a triangulation protocol [Citation34,Citation35]. A convergence coding matrix was created by wording research questions in such a way that both qualitative and quantitative data were relevant. The findings were classified as being convergent, divergent or “silent.” Divergent findings were further classified as complementary or dissonant.
Results
Participants and shorts provided
Fifteen participants completed the study (). Each is assigned a gender-specific pseudonym. There were 4 men and 11 women with a mean age of 48 (range from 34 to 57). Ten people had relapsing-remitting MS, three had secondary progressive, and two had primary progressive. Two male participants were South Asian British, the remainder were white British. A further participant withdrew after testing the orthotic shorts because they were visible beneath her clothing.
Table 2. Overview of participant characteristics.
Male participants all chose black or bold primary colours for their shorts, females were more likely to choose beige (six) or pastel (four). A toileting hole was provided for one male and five female participants. Participants’ choices around whether to have a zip or toileting hole were informed by their stated hand and bladder function. During the qualitative interviews, 7 of the 15 participants said they expected one of the pairs of shorts to be a “placebo” and 6 of these correctly identified the baselayer pair as the placebo.
Acceptability—quantitative data
Twelve participants (75%) chose to keep the orthotic shorts after the study and eight of these also kept the baselayer shorts. Adherence to the recommended wear times was good, with the orthotic shorts worn for 86% of the recommended time and the baselayer shorts worn for 88% of the recommended time.
Acceptability—qualitative data
As recommended by Sekhon et al. [Citation18], we considered both “anticipated” and “experienced” acceptability. “Anticipated acceptability” refers to acceptability of a healthcare intervention prior to the intervention being experienced directly, whereas “experienced acceptability” refers to acceptability of a healthcare intervention after that intervention has been experienced directly.
Anticipated acceptability
For the orthotic shorts, anticipated acceptability was revealed through the constructs of “intervention coherence” and “ethicality.” “Intervention coherence” refers to an individual’s understanding of how an intervention might work and whether the mechanism of action is congruent with their understanding of their condition. In the initial interview, participants were asked how they might respond to the shorts. They used terms such as “stability,” “balance,” “posture,” and “strength” to describe the expected effect. For example, Ben explained “they might keep me balanced… firmer.” Many participants referred to the concept of “core stability,” highlighting that their “core” was a particularly weak area or that core control directly influenced their balance or leg control.
Three participants had purchased close-fitting shorts or supportive underwear prior to hearing about the current study, “to see if it would help.” None found these previously purchased garments helpful, either because they were a poor fit or did not seem strong enough to be supportive. Nevertheless, they had suspected that tight clothing might be of benefit.
The component construct of “ethicality” refers to the extent to which an intervention fits with an individual’s value system. Four elements were considered to reflect value systems: the importance of taking opportunities to help yourself; the perceived value of exercise; the preference for simple, low-risk, non-pharmaceutical interventions and the desire for assistance invisible to others. “Taking opportunities” came across where participants explained that they take any opportunity to get involved in research and to explore new treatments. Participants felt that everyone with MS should try anything that might possibly help. For example, Dawn explained: “anything’s worth a go. And everybody’s different, aren’t they?” All participants explained the value of exercise for managing their MS and most reported being actively engaged in some form of regular exercise, either in their own home, at a therapy centre or in a gym. Several participants linked the importance of exercise to how they perceived the shorts. For example, Erica explained: “the attractive thing about the shorts is that it feels like something you might wear if you were going to the gym.” Several participants highlighted a preference for simple, low-risk, non-pharmaceutical approaches to managing MS symptoms, either because they had negative experiences with disease modifying drugs, did not like the idea of using drugs or wanted something non-pharmaceutical in addition to drug therapy. A final element of values is the preference for assistance that is not visible to others, a desire to hide your challenges and to avoid the stigma associated with aids. For some participants, this was an extremely important aspect of the shorts.
When I used my rollator, I can walk further…and I don’t have such severe back pain. I am hoping that, in a sense, the shorts are going to do that but they’re underneath me skirt and nobody sees them. (Ingrid)
Nobody’s going to say, “Oh, why have you got those funky, weird knickers on?” Umm… they are hidden. I like that they are hidden. I love that they are hidden. (Melissa)
Experienced acceptability—perceived effectiveness
For the orthotic shorts, experienced acceptability was revealed through the constructs of perceived effectiveness, burden, and affective attitude. “Perceived effectiveness” refers to the extent to which an intervention is perceived to be likely to achieve its purpose and included subthemes of “reclaiming my body,” “reclaiming autonomy,” and “managing self-image.”
The “reclaiming my body” subtheme includes participants’ perceptions of physical changes brought about by the shorts. Many participants reported improvements in posture, feeling “straighter” and more “upright.” Around half the participants described improvements in their walking ability. For example, they could walk “in a straight line,” rather than wavering from side to side. Kathy and Melissa described being better able to control their foot placement. Kathy explained that with her shorts she was able “to negotiate rubbish on the floor” and Melissa described that without her shorts, she would tread on her son’s toys on the living room floor. With the shorts, she could avoid them. Jon explained a similar feeling of improved control over stepping:
There was something there to constantly remind my legs that they should be going in a particular direction… in the past, when I’ve turned my head, my legs will just splay out in the direction that I am looking at… (the shorts) allowed me to go straighter… allowed my legs to point in the right direction.
Some participants explained that the shorts enabled them to walk further, faster, and more smoothly. Frank and Oliver explained that they could lift their feet more easily with the shorts on. Frank linked this improvement to a more upright posture:
When you’ve got the shorts on and you… straighten yourself and get yourself in the right position… because of the shorts, I feel better. That then leads you to not catch your feet as much, not drag as much and then you are able to push a bit further.
Some participants perceived that the shorts improved their leg strength. Four participants described being better able to control hip extension in functions such as sitting down, standing up, and squatting. One participant described her legs as stronger, sturdier, and “rock hard” with the shorts.
The second subtheme of “reclaiming my autonomy” describes several psychosocial benefits related to confidence and independence. Alison, Frank, Kathy, and Oliver described being able to stand for longer, turn or reach sideways with greater stability and be more active in standing, which in turn enabled them to better perform household tasks. As Oliver explained:
The benefits were general walking around, getting about, day-to-day stuff, working… You know, standing in the kitchen, washing and putting the pots away, things like that… umm… and general confidence. You do tend to find yourself doing more and not thinking about it.
All participants used terms such as “secure,” “stable,” “controlled,” “supported” or “strong” to describe how they felt when wearing the shorts. These terms can be applied to physical ability and emotional status and both meanings may be relevant; most participants appeared comfortable explaining perceived psychological effects. As Frank explained “yes it was physical but even if part of it was psychosomatic, I don’t care, it’s done its job.”
An increase in confidence was the most reported effect. Some related this to a specific function, such as walking or balance, whereas for others it seemed to be a more holistic effect, making people “generally confident,” “positive,” and “less ill.” As Linda explained: “security wise, wearing these shorts, I felt a bit more confident in doing things. That little bit more support.”
The final subtheme within “perceived effectiveness” is that of “managing self-image.” Caroline, Dawn, and Ingrid explained that improving the appearance of their walking was one of their motivations for trialling the shorts. Although Ingrid did not experience a positive effect on the appearance of her walking, both Dawn and Caroline felt this improved with the shorts. In addition, Kathy’s renewed ability to walk outside without her rollator had a positive influence on her self-image because of the stigma she associated with her walking aid.
For some, the appearance of the shorts themselves had a negative influence on self-image and this is explored in the “affective attitude” subtheme below.
Experienced acceptability—burden
The construct of “burden” refers to the perceived effort required to participate in an intervention. Many participants felt the burden of using the shorts was low, reporting that the shorts were mostly comfortable, easy to get on and off and easy to launder. Burdensome elements of the shorts are described below and related to managing temperature, dressing and undressing, discomfort, and movement restriction.
Those participants who trialled the shorts during the summer explained that they were too warm on hot days. Some felt that it took them longer to get dressed or undressed with the shorts. Whether dressing was perceived as hard or easy could be related to participants’ usual clothing choices. As Alison explained, putting on the shorts was “just like putting a pair of tights on” and Jon felt they were “no more difficult than some other clothing that I’ve got.” Some participants referred to a period of familiarisation, explaining that they “got used to” the shorts.
Many participants described the shorts as “tight,” but a few used more negative terms such as “restrictive,” “constrictive,” and “uncomfortable.” Alison, Ben, Erica, and Gwen felt a sensation of heaviness with the shorts. The movements felt to be most restricted involved trunk and hip flexion such as climbing stairs, bending over, using an exercise bike and sit-ups. For Gwen, this restriction significantly reduced acceptability. She explained that “an awful lot of muscular effort had to go into bending the hip… you know, in order to lift the leg properly.” Where participants described the shorts as uncomfortable, this was mostly around the abdomen and often related to flexed postures.
Experienced acceptability—affective attitude
“Affective attitude” refers to the emotional response to an intervention. About half the participants explained that they liked the shorts and used only positive language, including “fantastic,” “brilliant,” and “a pleasure to wear.” Included within this group were the three participants who had tried and been disappointed by other forms of tight clothing. In contrast, Erica and Gwen gave consistently negative feedback and used negative language to describe their emotional response. Gwen disliked the shorts because of the restriction she felt when climbing stairs, exclaiming: “bloody things… making my life hell.”
The appearance of the shorts had a strong influence on affective attitude for some female participants. None of the females wanted the shorts to be visible and were concerned around choice of clothing to achieve this. They discussed the length of their skirts and the tightness of their trousers. Colour choice seemed important. The men, who had chosen either red, dark blue or black, and the women who had chosen black, commented little on appearance. However, some women who had chosen paler colours, either beige or pastels, appeared to dislike the shorts. This was particularly evident for Erica who explained that she had been drawn to the study partly because of the sporty appearance of the shorts on the flyer (see ). She chose beige so that they would be less visible under clothing but clearly regretted this choice, saying that the shorts made her feel “a bit like an old granny,” describing the colour as “pretty disgusting” and that wearing them was “a bit of a downer.” Paradoxically, the same colour choice was both acceptable and unacceptable, depending upon whether appearance was judged with or without a top layer of clothing. The appearance of shorts under clothing and their appearance without outer clothing both seemed important.
Baseline characteristics
The participant group demonstrated a wide range of abilities, with a mean self-selected gait speed at Visit 3 of 1.1 ± 0.37 m/s (range 0.56 m/s to 1.99 m/s). There were changes in the “no shorts” conditions across Visits 3, 5, and 7 with increases in self-selected gait speed and decreases in stride time variability and step width variability over time (). There was a marked improvement in participant-perceived walking ability between Visit 1 and Visit 7 ().
Table 3. “No shorts” values at Visits 3, 5, and 7 for spatiotemporal gait parameters that improved during the study.
Impact of orthotic shorts on self-selected gait speed and spatiotemporal gait parameters
For a cross-over study to enable a valid comparison of variables in the two different conditions assessed (orthotic shorts versus baselayer shorts) there should be a return to baseline ability following the removal of the shorts. The direct comparison planned between the two pairs of shorts is less valid, because of the changes in participants’ abilities in the “no shorts” conditions over time and because more participants trialled the orthotic shorts first. Nevertheless, as this was an exploratory, descriptive feasibility study aimed at informing future trials, objective data are presented in for both the within-day and between-day comparisons, i.e., comparing shorts on versus off on the same day, as well as orthotic versus baselayer shorts.
Table 4. Impact of shorts on self-selected gait speed and spatiotemporal gait parameters.
Table 5. Impact of shorts on trunk and pelvic mediolateral sway.
Table 6. Mean changes and effect sizes for participant-perceived walking ability.
Effect sizes (ES) showed a small increase in self-selected gait speed with the orthotic shorts (ES = 0.27), with a correspondingly small increase in step length (ES = 0.27) and a small decrease in stride time (ES = −0.22) (). There were very small or negligible changes in these variables in the baselayer shorts.
There was a moderate decrease in step width (ES = −0.5) with the orthotic shorts but not with the baselayer shorts (ES = 0.03). With the orthotic shorts, the group mean for step width narrowed by 1.5 cm.
Step width did not narrow in the orthotic shorts for all participants. shows the different baseline values for each participant, along with the step width in each pair of shorts and comparison values for mean step width obtained by Comber et al. for healthy and MS groups in their systematic review [Citation36]. Several individuals with a relatively narrow step width at baseline, did not decrease step width further in the orthotic shorts (e.g., Helen, Erica, Caroline).
Figure 3. Mean step width compared to normal range in orthotic shorts compared to baseline and baselayer shorts. (Means for normal, non-neurologically impaired people and people with MS are provided for comparison, with 95% confidence intervals (95% CI) for means, using data obtained from Comber et al. [Citation36]. This normal range is shaded. Orthotic shorts test data are missing for Frank, due to heat-induced fatigue during data collection).
![Figure 3. Mean step width compared to normal range in orthotic shorts compared to baseline and baselayer shorts. (Means for normal, non-neurologically impaired people and people with MS are provided for comparison, with 95% confidence intervals (95% CI) for means, using data obtained from Comber et al. [Citation36]. This normal range is shaded. Orthotic shorts test data are missing for Frank, due to heat-induced fatigue during data collection).](/cms/asset/bdf2f1b4-7cd4-409f-8804-ea2854b4a3f3/idre_a_2114018_f0003_c.jpg)
Variability of spatiotemporal gait parameters decreased in both the orthotic and baselayer shorts (). The most notable change is the decrease in step width variability seen with the orthotic shorts (ES = −0.57).
Impact of orthotic shorts on trunk and pelvis sway range
Although there was a moderate decrease in step width, the orthotic shorts had a negligible impact on mediolateral pelvic sway range (ES = −0.05, ). Some participants decreased step width and mediolateral pelvic sway in the shorts; however, many decreased step width with either no change in mediolateral pelvic sway range or a slightly increased sway range. There was a small decrease in mediolateral trunk sway range in both orthotic and baselayer shorts.
Impact of orthotic shorts on participant-perceived walking ability
Both orthotic and baselayer shorts appeared to have a moderate positive effect on participant-perceived walking ability (). Most participants improved during the orthotic shorts trial, with a group mean difference of 21 points (ES = 0.6). The baselayer shorts had only slightly less influence, with a mean improvement from baseline of 18 points (ES = 0.52). Group means for both shorts were improved by more than the 11 points suggested to represent clinically important change [Citation29].
Integration of qualitative and quantitative findings
The convergent coding matrix, used to aid integration, is shown in . Both datasets converge on the conclusion that the orthotic shorts are an acceptable intervention. The quantitative results show good adherence to wear and a high proportion of participants chose to keep their shorts after the trial. The qualitative data explicate what is meant by acceptability and how acceptability might be improved in the future. Those individuals who did not keep their shorts after the trial either struggled with hip flexion, particularly on the stairs, or disliked the appearance of the shorts.
Table 7. Convergent coding matrix for integration of qualitative and quantitative findings.
There is convergence of qualitative and quantitative findings around potential efficacy. An effect on confidence was described qualitatively and is reflected in the improved participant-perceived walking ability, measured using the MSWS-12. We suggest that the small improvements seen in self-selected gait speed, step length, and stride time are reflective of improved confidence.
There is convergence of qualitative and quantitative data regarding the improvements on controlling leg direction whilst stepping. Several participants described this sensation clearly, and we suggest that the improvements seen in step width and step width variability are reflective of this same skill.
There is convergence between qualitative and quantitative data suggesting that active inner-range hip flexion is more challenging in the orthotic shorts. Step length improved slightly when walking so resistance to hip flexion does not appear to interfere with that task; however, lifting the leg further into inner-range was reported to be difficult and the MSWS-12 data for these participants suggested challenges with hip flexion whilst wearing the shorts.
The potential effect of the shorts on stability was more complex. Qualitative data suggests that many participants felt more stable and controlled. Quantitative data for step width, step width variability, and mediolateral trunk sway all support the idea that the orthotic shorts might improve gait stability. However, there was no change in the mean for mediolateral pelvic sway. Comparing our data for those obtained in previous research, it appears that the group mean at baseline in the present study was already within normal range [Citation37]. This might explain why no improvement in mean pelvic sway was observed.
Discussion
This study is the first to investigate the use of orthotic shorts for improving gait and walking in PwMS. Findings around acceptability and the improvements in participant-perceived walking ability support the need for further investigation and development of what could potentially be a useful and cost-effective intervention.
Acceptability was good, particularly that of “anticipated acceptability,” meaning people’s impressions of how satisfied they might be with this intervention, simply based upon its description. Three elements suggest that anticipated acceptability may be strong in the wider MS population. Firstly, participants suggested the shorts might improve their core stability, and poor core stability appears to be a common presentation in MS and is a common focus of exercise programmes [Citation38]. Second, participants liked the shorts partly because they associated them with exercise and exercise appears to be well-accepted by PwMS as an important part of self-management [Citation39–41]. Finally, participants were attracted by the idea of support that was invisible to others, and reports of stigma associated with walking aids and other assistive devices are common in MS [Citation42,Citation43]. Good “anticipated acceptability” would likely reflect in strong recruitment rates to future trials. Experienced acceptability was also good, except for some negative reactions to the appearance of the shorts and restriction of hip and trunk flexion. It should be remembered that the extremely positive “anticipated acceptability” may in itself have led to a positive “experienced acceptability” as a result of expectancy effects.
The importance of improved confidence and perceived walking ability should not be underestimated because these could lead to improved exercise self-efficacy and increased engagement with physical activity [Citation39]. Mothes et al. [Citation44] demonstrated that an external device has a more powerful motivating influence in people with low self-efficacy in the first instance, which is known to be the case in MS [Citation45,Citation46].
There are ways in which orthotic shorts could be developed to further improve acceptability, such as improvements to colour and design, particularly for female users. It may be possible to adapt the support to hip extension so that it is at an optimal level for each individual, balancing support for extension with restriction of hip flexion.
There are a number of ways in which this study has informed the design of future trials. Firstly, we felt that the placebo garment comparison was of debateable value. In our study, seven participants expected a placebo comparator and six correctly identified the “placebo” shorts. More importantly, our quantitative findings suggested that the baselayer garment may have had a measurable effect on step length variability, which is difficult to explain as a placebo effect. There may be a proprioceptive response to the baselayer garment, similar to effects reported for orthotic joint supports [Citation47]. In other words, the so-called “placebo” might possess one of the key active ingredients of the orthotic. A similar issue occurred in a study investigating an orthotic sleeve for people with ataxic tremor [Citation48]. Compression garments, such as those frequently used in sport, are similarly difficult to research. In response, many compression garment researchers compare to a “no-intervention” control [Citation11]. Placebo effects can be minimised by manipulating participant expectations [Citation49] and using outcome measures that are objective and less susceptible to changes in voluntary effort. Whilst a valid control is required in a future trial, we would not recommend simply comparing an orthotic garment to a “placebo” garment as this may conceal valid treatment effects.
This study has suggested that the spatiotemporal gait parameters more likely to respond to orthotic shorts are those relevant to mediolateral stability. Although there was a small improvement in the anteroposterior gait parameters of step length, stride time, and self-selected walking speed, these were only small and possibly explained by increased voluntary effort elicited by improved confidence or participant expectations. Mediolateral stability is likely to be closely related to balance and falls risk [Citation50], so a future study should include a balance measure, possibly as the primary outcome. It may be worthwhile focussing such a trial on that subgroup of PwMS described by Filli et al. [Citation5], whose gait is characterised by instability. Development of screening tools for identification of gait instability is recommended to identify this population clinically.
In the present study, orthotic shorts were provided as per the current practice of the orthotics company, developed through their clinical experience. One disadvantage of this is that the shorts provided varied across the participant group. Although we believe that customisation of side zips and toileting holes are crucial to ensure acceptability, there were no indications that the “abduction assist” and lumbar support provided any additional effect compared to the standard shorts. It may be better for a future trial to use a more standardised intervention and avoid introducing confounding variables.
Strengths and limitations
The study sample was adequate for gaining insight into a range of participant experiences. The TFA was a useful theoretical framework for the qualitative study. It highlighted the importance of factors such as intervention coherence and ethicality that might otherwise not have been recognised and drew our attention to the importance of “anticipated acceptability.” The mixed-methods approach was valuable, enabling increased validity for the claim that these orthotic shorts are acceptable. Assessor blinding was successful, with the assessor unable to determine which shorts were being worn during objective testing.
The main limitation of this study relates to challenges with the cross-over study design. The investigation into potential efficacy was mainly informed by the within-day changes because of the problems with randomisation, improvement in baseline ability, and the possible proprioceptive effects of the baselayer shorts comparator. Future cross-over studies that aim to compare two different orthotic devices should investigate direct orthotic effect first, with objective assessments conducted within a relatively short time scale and completed before any home trials, in order to minimise changes in baseline abilities. It is important to note that the variability and effect size estimates obtained were from a relatively small sample size and therefore might over-estimate or under-estimate the numbers required in a fully powered study.
A further limitation is that the qualitative interviews were conducted by the principal investigator. Although participants’ comments did appear balanced and considered, the relationship between participants and researcher could have discouraged negative feedback.
Conclusion
Orthotic shorts might improve gait and participant-perceived walking ability in PwMS. Spatiotemporal gait parameters appear to respond more in the mediolateral plane than in the anteroposterior plane, with moderate decreases in step width and step width variability. There was a marked improvement in participant-perceived walking ability with the shorts that may have been reflected in the small increases in self-selected walking speed. The shorts were acceptable to most users who described improved control, stability, and foot placement. Where the shorts were less acceptable, this was either related to their appearance or to restriction of inner-range hip flexion.
To determine whether the orthotic shorts are effective in MS, a fully powered randomised controlled trial should be conducted. Our findings suggest that recruitment to such a study would be strong, and that the primary outcome should measure either mediolateral stability in gait or functional balance.
Acknowledgements
The authors acknowledge the assistance of DM Orthotics Ltd, who provided the orthotic shorts tested in this study; the MS Therapy Centre, MS Society UK and Sheffield Teaching Hospitals NHS Foundation Trust, who assisted with recruitment, and the participants who trialled the shorts and shared their experiences.
Disclosure statement
The orthotic and baselayer shorts tested in this study were provided free of charge by DM Orthotics Ltd but they had no direct involvement with the conduct of the study, data analysis or interpretation. There are no other potential conflicts of interest.
Data availability statement
References
- Jones K, Ford D, Jones P, et al. How people with multiple sclerosis rate their quality of life: an EQ-5D survey via the UK MS register. PLoS One. 2013;8(6):e65640.
- LaRocca N. Impact of walking impairment in multiple sclerosis. Patient. 2011;4(3):189–201.
- Pike J, Jones E, Rajagopalan K, et al. Social and economic burden of walking and mobility problems in multiple sclerosis. BMC Neurol. 2012;12(1):94.
- Givon U, Zeilig G, Achiron A. Gait analysis in multiple sclerosis: characterization of temporal-spatial parameters using GAITRite functional ambulation system. Gait Posture. 2009;29(1):138–142.
- Filli L, Sutter T, Easthope CS, et al. Profiling walking dysfunction in multiple sclerosis: characterisation, classification and progression over time. Sci Rep. 2018;8(1):4984.
- Matthews M, Blandford S, Marsden J, et al. The use of dynamic elastomeric fabric orthosis suits as an orthotic intervention in the management of children with neuropathic onset scoliosis: a retrospective audit of routine clinical case notes. Scoliosis Spinal Disord. 2016;11(1):14–24.
- Hoang P, Gandevia S, Herbert R. Prevalence of joint contractures and muscle weakness in people with multiple sclerosis. Disabil Rehabil. 2014;36(19):1588–1593.
- Cameron M, Horak F, Herndon R, et al. Imbalance in multiple sclerosis: a result of slowed spinal somatosensory conduction. Somatosens Mot Res. 2008;25(2):113–122.
- Huisinga J, Mancini M, St. George R, et al. Accelerometry reveals differences in gait variability between patients with multiple sclerosis and healthy controls. Ann Biomed Eng. 2013;41(8):1670–1679.
- Doan BK, Kwon YH, Newton RU, et al. Evaluation of a lower-body compression garment. J Sports Sci. 2003;21(8):601–610.
- Snowdon N, Sier D, Potia T, et al. Compression garments and fabric orthoses for rehabilitation and function: a systematic mapping review. Int J Ther Rehabil. 2018;25(12):655–664.
- Street T, Swain I, Taylor P. Training and orthotic effects related to functional electrical stimulation of the peroneal nerve in stroke. J Rehabil Med. 2017;49(2):113–119.
- Serrao M, Casali C, Ranavolo A, et al. Use of dynamic movement orthoses to improve gait stability and trunk control in ataxic patients. Eur J Phys Rehabil Med. 2017;53(5):735–743.
- Snowdon N, Booth S, McLean S, et al. The meaning of fabric orthoses to long-term users with multiple sclerosis: an interpretative phenomenological analysis. Prosthet Orthot Int. 2021;45(3):246–253.
- Maguire C, Sieben J, Frank M, et al. Hip abductor control in walking following stroke — the immediate effect of canes, taping and TheraTogs on gait. Clin Rehabil. 2010;24(1):37–45.
- Skivington K, Matthews L, Craig P, et al. Developing and evaluating complex interventions: updating medical research council guidance to take account of new methodological and theoretical approaches. Lancet. 2018;392:S2–S2.
- Bowen D, Kreuter M, Spring B, et al. How we design feasibility studies. Am J Prev Med. 2009;36(5):452–457.
- Sekhon M, Cartwright M, Francis J. Acceptability of healthcare interventions: an overview of reviews and development of a theoretical framework. BMC Health Serv Res. 2017;17(1):88.
- Martin LR, Williams SL, Haskard KB, et al. The challenge of patient adherence. Ther Clin Risk Manag. 2005;1(3):189–199.
- Tuazon JR, Jahan A, Jutai JW. Understanding adherence to assistive devices among older adults: a conceptual review. Disabil Rehabil Assist Technol. 2018;14(5):1–10.
- Scherer MJ, Sax C, Vanbiervliet A, et al. Predictors of assistive technology use: the importance of personal and psychosocial factors. Disabil Rehabil. 2005;27(21):1321–1331.
- Julious SA. Sample size of 12 per group rule of thumb for a pilot study. Pharmaceut Statist. 2005;4(4):287–291.
- Brophy-Williams N, Driller M, Halson S, et al. Evaluating the kikuhime pressure monitor for use with sports compression clothing. Sports Eng. 2014;17(1):55–60.
- Sosnoff J, Klaren R, Pilutti L, et al. Reliability of gait in multiple sclerosis over 6 months. Gait Posture. 2015;41(3):860–862.
- Wong J, Jasani H, Poon V, et al. Inter- and intra-rater reliability of the GAITRite system among individuals with Sub-acute stroke. Gait Posture. 2014;40(1):59–261.
- Psarakis M, Greene D, Cole M, et al. Wearable technology reveals gait compensations, unstable walking patterns and fatigue in people with multiple sclerosis. Physiol Meas. 2018;39(7):075004.
- Kieseier BC, Pozzilli C. Assessing walking disability in multiple sclerosis. Mult Scler. 2012;18(7):914–924.
- Hobart C, Riazi L, Lamping J, et al. Measuring the impact of MS on walking ability: the 12-Item MS walking scale (MSWS-12). Neurology. 2003;60(1):31–36.
- Baert I, Freeman J, Smedal T, et al. Responsiveness and clinically meaningful improvement, according to disability level, of five walking measures after rehabilitation in multiple sclerosis: a European Multicenter Study. Neurorehabil Neural Repair. 2014;28(7):621–631.
- Caelli K, Ray L, Mill J. “Clear as mud”: toward greater clarity in generic qualitative research. Int J Qual. 2016;2(2):1–13.
- Ritchie J, Lewis J, McNaughton Nicholls C, et al. Qualitative research practice: a guide for social science students and researchers. 2nd ed. London (UK): Sage; 2013.
- Pallant J. SPSS survival manual: a step-by-step guide to data analysis using SPSS for windows. 3rd ed. Maidenhead (UK): Open University Press; 2007.
- Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale (NJ): Lawrence Erlbaum Associates; 1988.
- O’Cathain A, Murphy E, Nicholl J. Three techniques for integrating data in mixed methods studies. Br Med J. 2010;341(7783):1147–1150.
- Farmer T, Robinson K, Elliott S, et al. Developing and implementing a triangulation protocol for qualitative health research. Qual Health Res. 2006;16(3):377–394.
- Comber L, Sosnoff J, Galvin R, et al. Postural control deficits in people with multiple sclerosis: a systematic review and meta-analysis. Gait Posture. 2018;61:445–452. 2018
- Orendurff M, Segal A, Klute G, et al. The effect of walking speed on center of mass displacement. JRRD. 2004;41(6):829–834.
- Fox E, Hough A, Creanor S, et al. Effects of pilates-based core stability training in ambulant people with multiple sclerosis: multicenter, assessor-blinded, randomized controlled trial. Phys Ther. 2016;96(8):1170–1178.
- Ferrier S, Dunlop N, Blanchard C. The role of outcome expectations and self-efficacy in explaining physical activity behaviors of individuals with multiple sclerosis. Behav Med. 2010;36(1):7–11.
- Kasser S. Exercising with multiple sclerosis: insights into meaning and motivation. Adapt Phys Activ Q. 2009;26(3):274–289.
- Stennett A, De Souza L, Norris M. Physical activity and exercise priorities in community dwelling people with multiple sclerosis: a Delphi study. Disabil Rehabil. 2018;40(14):1686–1693.
- Ploughman M, Godwin M, Stefanelli M, et al. The path to self-management: a qualitative study involving older people with multiple sclerosis. Physiother Can. 2012;64(1):6–17.
- Squires L, Williams N, Morrison V. Matching and accepting assistive technology in multiple sclerosis: a focus group study with people with multiple sclerosis, carers and occupational therapists. J Health Psychol. 2019;24(4):480–494.
- Mothes H, Leukel C, Seelig H, et al. Do placebo expectations influence perceived exertion during physical exercise? PLoS One. 2017;12(6):e0180434.
- Backus D. Increasing physical activity and participation in people with multiple sclerosis: a review. Arch Phys Med Rehabil. 2016;97(9 Suppl):S210–S217.
- Moffat F, Paul L. Barriers and solutions to participation in exercise for people with multiple sclerosis (MS): a consensus study using nominal group technique. Physiotherapy. 2016;102(S1):e266–e266.
- Ghai S, Driller M, Ghai I. Effects of joint stabilizers on proprioception and stability: a systematic review and meta-analysis. Phys Ther Sport. 2017;25:65–75.
- Miller L, van Wijck F, Lamont L, et al. Sensory dynamic orthoses in mild to moderate upper limb tremor in multiple sclerosis: a mixed methods feasibility study. Clin Rehabil. 2016;30(11):1060–1073.
- Evans K, Colloca L, Pecina M, et al. What can be done to control the placebo response in clinical trials? A narrative review. Contemp Clin Trials. 2021;107:106503–106503.
- Brach J, Berli J, Vanswearingen J, et al. Too much or too little step width variability is associated with a fall history in older persons who walk at or near normal gait speed. J Neuroeng Rehab. 2005;2:21.