
Abstract
Purpose
Exercise fidelity is a fundamental aspect of exercise prescription by physiotherapists. Assessing exercise fidelity via telehealth (videoconference) is potentially useful but its reproducibility has not been assessed. The objective was to evaluate agreement (reproducibility) of video rating of calf exercise fidelity within (over four weeks) and between telehealth raters and compared with live rating.
Methods
Nineteen videos of participants with AT undertaking calf exercises were rated by physiotherapists in person (live) and by watching pre-recorded videos (replicating telehealth). Three forms of agreement were assessed: (i) between live assessment and recorded video (telehealth) assessment; (ii) between telehealth raters (inter-rater); (iii) agreement within telehealth raters over four weeks (intra-rater).
Results
There was weak to almost perfect agreement (Kappa = 0.65 to 1.00, rater 1, Kappa = 0.57 to 1.00, rater 2) between the telehealth and live raters. There was moderate to almost perfect agreement (Kappa = 0.65 to 1.00) when assessing intra-rater reliability, aside from one of the six criteria (quality of movement).
Conclusion
Assessing calf exercise fidelity via videos recorded on Zoom® appears to demonstrate weak or greater agreement versus live rating and over time. Inter-rater agreement was lower, suggesting that the criteria developed may be better suited to use by individual raters over time.
Telehealth assessment (when compared with live, in person assessment) shows a moderate or greater agreement for the majority of assessment criteria when assessing calf exercise fidelity.
The calf exercise fidelity criteria developed can be used as an adjunct to assessment and management of people with Achilles Tendinopathy.
Intra-rater assessment was shown to be moderately or more consistent over a four-week period when assessing calf exercise fidelity.
Implications for rehabilitation
Introduction
Achilles tendinopathy (AT) is a common tendon overuse disorder that manifests clinically as localised tissue pathology, swelling, tenderness and activity-related tendon pain [Citation1]. Achilles tendinopathy can severely impact the ability to undertake basic human daily, sporting and recreational activities including walking, running and jumping [Citation2]. The cumulative lifetime incidence of AT in the general population has been reported to be 6% [Citation3]. The aetiology of the tendinopathy is complex and the combination of internal and external risk factors has the potential to accelerate the pathological degeneration of the tendon [Citation4]. Calf muscle exercise is recommended as a first line approach for managing AT in clinical practice guidelines [Citation5], informed by systematic reviews of level I evidence [Citation6,Citation7].
A key challenge in managing burdensome musculoskeletal conditions such as AT is providing effective and timely healthcare services to people most in need. Barriers include the availability of health professionals, particularly in rural and remote areas, and the cost and inconvenience for health consumers. Innovative service delivery options such as telehealth have the potential to reduce health inequalities related to provision of care [Citation8] and became more popular during the Covid-19 pandemic [Citation9]. Telehealth uses telephone or videoconference to provide rehabilitation services at a distance that replace or supplement face-to-face care [Citation10]. Healthcare providers are unlikely to embrace telehealth technology unless they are convinced that quality of care is equivalent to face-to-face interactions [Citation11].
Exercise fidelity (the extent to which in exercise is followed as prescribed) is thought to be an important component of exercise prescription by physiotherapists [Citation12]. For this study, exercise fidelity encompasses exercise execution parameters such as tempo, range of motion, and other factors. For example, undertaking exercise with appropriate time under tension is known to influence tendon adaptation [Citation13], and may therefore influence rehabilitation success. Appropriate exercise fidelity may also be important in clinical rehabilitation. For example, in insertional AT it is recommended that the calf exercise is not performed into end-range dorsiflexion as this may aggravate pain [Citation14].
Calf raise testing and exercise has been used widely to assess [Citation15,Citation16] and treat [Citation17–19] people with AT, but there is no consensus regarding how it should be performed [Citation20]. The utility of evaluating calf exercise fidelity via telehealth has not been assessed. To address this knowledge gap, this study aimed to: (i) Develop criteria to assess calf exercise fidelity for AT (ii) Evaluate the inter-rater reliability between live assessment by an expert physiotherapist and telehealth assessment by less experienced physiotherapists (iii) Evaluate inter-rater reliability using telehealth assessment (iv) Evaluate intra-rater reliability using telehealth assessment.
Design
This observational study investigated the reproducibility of assessing calf exercise fidelity via telehealth using videoconference software (Zoom Video Communications, San Jose, California). This study was nested in a feasibility and pilot randomised trial investigating the efficacy of exercise intensity (higher load intensity = 6 repetitions maximum versus lower load intensity = 18 repetitions maximum) and time under tension (high = 6 s versus low = 2 s per cycle in time with metronome) in the management of mid-portion AT [Citation21]. Guidelines for Reporting Reliability and Agreement Studies checklist was used to guide the reporting of this manuscript [Citation22].
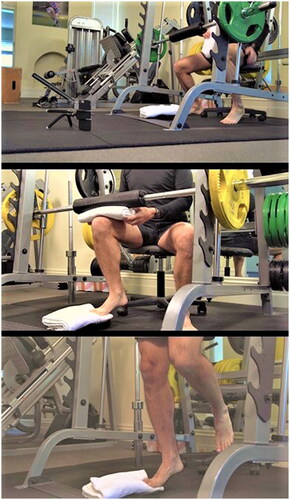
We chose to assess standing and seated isotonic (concentric and eccentric) calf raise exercises as most common AT and Achilles tendon rupture rehabilitation programs include these exercises [Citation17–19,Citation23–25]. Both exercises were performed using a Smith machine (see ) with a tempo (divided equally in the concentric and eccentric phases) of 2 or 6 s per repetition (timed with a metronome set at 60 beats per minute). Participants performed the standing calf raise with no external load (bodyweight only) and the seated calf raise with a bar (17 kg) and up to 30 kg of additional external load.
Figure 1. Smith machine set up for calf exercises.
Developing the exercise fidelity criteria
We defined exercise fidelity as the ability to execute the exercise as per instructions. There were three stages in developing the exercise fidelity criteria; (1) developing initial criteria based on evidence and the research group’s experience; (2) piloting the telehealth environment; and (3) consulting experts to guide refinement and development of the criteria and telehealth environment.
Stage 1: We identified studies that described calf raise exercises parameters [Citation16,Citation19,Citation20,Citation26–29] based on a search of the available literature and relative databases (search terms were “calf raise” and “calf exercise”). Based on this literature and the research team’s experience we developed seven initial criteria that were considered important when assessing calf raise exercise fidelity. These initial criteria assessed the following characteristics as achieved or not; (1) tempo; (2) plantarflexion range of motion (ROM); (3) dorsiflexion ROM; (4) foot position (neutral rather than abducted or adducted); (5) movement occurring in the sagittal plane; (6) lifting the toes off the ground (hyperextension) in dorsiflexion; and (7) bending the knee (for standing only).
Stage 2: We undertook extensive planning (in collaboration with experienced information technology and video production professionals from Monash University) and piloting of the telehealth environment. This included experimenting with the camera distance from the participant and the camera angle (side, front, back, from an angle), methods to support the camera (various tripods) and camera resolution and frame rate for the video recording. The goal was to develop a method that was cost and time efficient so it could be easily adopted by clinicians but also enabled accurate assessment of the fidelity criteria.
Stage 3: Eight international “experts” (physiotherapists and a podiatrist with a minimum of five years of clinical and research expertise in musculoskeletal disorders including Achilles tendinopathy) were recruited (May-June 2017). We explored their views on the initial criteria we created. The experts were provided with a description of each criterion as well as videos demonstrating adequate and inadequate execution. via semi-structured open response questionnaire (Google Survey) the experts provided feedback on the appropriateness of the telehealth environment and whether our criteria were necessary, clearly defined and easily assessable. They also had an opportunity to suggest other additional criteria and provide additional feedback in open response format.
Calf raise exercise fidelity criteria
There were modifications made to the fidelity criteria based on feedback from the experts including labelling of exercise instructions (e.g., “use the phrase heel up and down instead of concentric and eccentric movement”). Experts also suggested making the cut-off for defining adequate plantarflexion and dorsiflexion standardised and easily assessible via video (i.e., raising or lower the heel by 1 inch above or below the horizontal). Based on consensus among most experts, two original fidelity criteria were removed (lifting the toes in dorsiflexion and foot position). Qualitative feedback was that the criteria were too uncommon (lifting the toes in dorsiflexion) or related to starting position and therefore instructions rather than exercise fidelity (foot adduction). There was 100% consensus for retaining other criteria among the experts, except for whether movement was occurring in the sagittal plane. Some experts argued that movement to the lateral part of the foot is a sign that the tibialis posterior muscle is effectively functioning. Based on this we refined our definition of this fidelity error as “obvious” movement outside of the sagittal plane. No new criteria were suggested by the experts.
After further piloting with the revised criteria, the authors found individuals were able to move in time with the metronome (e.g., down for 3 s and up for 3 s) but with very poor movement quality. We defined poor movement quality as either: (1) moving in a cogwheel motion in time with the metronome or (2) having a sudden drop into dorsiflexion. We added an additional criterion that we labelled “quality” that was rated as not achieved if either of these fidelity errors were present. The final exercise fidelity criteria are shown in .
Table 1. Criteria established for assessing calf muscle exercise fidelity.
Participant recruitment and eligibility
Forty-eight participants with AT were recruited (April 2018–April 2019) via clinical networks and paid Facebook advertising for the feasibility and pilot randomised trial in which this observational study was nested. A subsample of this trial cohort was required for this nested study. A total of 19 videos of individuals performing standing and seated calf raises were selected randomly and used.
Individuals were eligible for the trial if they were male, aged 18–70 years, had pain localised to the mid-portion of the Achilles tendon for 12 weeks or longer, had morning stiffness and pain during or after activities that load the Achilles tendon (walking, running, jumping). To be eligible, they also required ultrasound imaging consistent with AT (anteroposterior thickness and/or hypoechoic regions within the midportion of the Achilles tendon with or without doppler signal [Citation5] and a score of ≤75 on the Victorian Institute of Sports Assessment—Achilles questionnaire (VISA-A). The VISA—A questionnaire assessed pain and disability where scores range from 0 to 100, and greater scores indicate lower pain and disability [Citation30].
Rating of exercise fidelity
Recording videos and real time expert rating
During baseline assessment for the randomised trial, an expert rater physiotherapist (PM) with >24 years of clinical experience (>15 specialising in the management of AT) assessed calf raise exercise fidelity. Prior to exercise prescription and instruction, participants performed one set of seated and standing heel raise exercise (random order) on each side (random order) after minimal verbal instruction (“raise up and down onto your toes in time with the metronome, 1 or 3 beats up, and 1 or 3 beats down” [tempo was dependent on group allocation]). During this initial exercise performance, the expert rated each fidelity criterion in real time. Simultaneously, exercise was recorded via Zoom® on a smart phone using the telehealth set-up described above. This software allows for a videoconference to be recorded and saved by the host as an MP4 file. The videos were recorded on a phone at a resolution of 640 by 480 pixels and at 30 frames per second (consistent with the capability of most smart phones). During testing, noise and lighting levels were standardised. The live expert rater had the opportunity to review ratings via the recorded video if required.
Video rating by physiotherapist raters
A further two registered physiotherapists, (referred to as telehealth rater 1 and telehealth rater 2 throughout) with musculoskeletal experience (telehealth rater 1 was two years post-qualification, and telehealth rater 2 was six years post-qualification, see for characteristics) independently rated the recorded videos using the defined criteria. Both telehealth raters had no prior telehealth assessment experience. Prior to rating the videos, they received two hours of face-to-face training by the live expert rater (PM). The training included teaching the physiotherapists the rating scale and the aims of the research project. The training involved demonstration of acceptable technique during calf raise exercise as well as demonstration of each of the pass and fail fidelity criteria. The instructor (PM) showed them videos that included errors for each fidelity criterion and discussed how to apply the rating scale in each case. Following this theoretical training, the physiotherapists were provided with one to one training using training videos to practice using the fidelity criteria. Physiotherapists needed to rate at least 80% of the training videos correctly to be included in the study (which they both did on the first attempt). The telehealth raters accessed the same videos (via an online folder link [Dropbox, the American company Dropbox, Inc. San Francisco, California]) and were blinded to the ratings of the live expert rater and each other. The telehealth raters were advised to play back the videos on an 11 to 20-inch computer screen to ensure the videos were large enough yet high quality. Participants could view each video as many times as required to complete their assessment. This was intended to recreate a clinical environment where several sets of a calf raise exercise may be observed to assess a patient’s fidelity.
Table 2. Telehealth rater characteristics.
Telehealth environment
The videoconference environment is shown in . The phone was placed vertically on a small and inexpensive tripod (positioned 1-meter away from the non-exercising leg at a 45°degree angle). The phone camera view captured up to the level of the knee. Some experts suggested that two cameras (behind and at the side) would be optimal for other criteria such as heel lowered and ankle rotation (eversion and inversion) but consensus among the research team was that this was impractical for time-efficient clinical assessment and for patient convenience.
Data analysis
Real-time and video reproducibility of the criteria of the exercise fidelity assessment were determined using absolute percentage agreement, as well as unweighted Kappa coefficients (strength of agreement). Kappa coefficients were interpreted using McHugh’s interpretation; 0 to 0.20 no agreement, 0.21 to 0.39 minimal, 0.40 to 0.59 weak, 0.60 to 0.79 moderate, 0.80 to 90 strong, >90 almost perfect) [Citation31]. McHugh’s interpretation was chosen as it acknowledges that 80% agreement is commonly seen as the minimum acceptable level in healthcare research whilst also acknowledging that it is typical to see a reduction in percentage agreement in Kappa results [Citation31]. Version 26 of SPSS (IBM Corp., Armonk, NY, USA) was used for statistical analysis. The target sample size was estimated to be 17 for a two-rater study to detect a statistically significant Kappa coefficient (p < 0.05) on a dichotomous variable with 80% power [Citation32]. A total of 19 videos of individuals from the pool of 23 recruited participants with mid-portion AT performing standing and seated calf raises were selected randomly and used in analyses.
Results
Description of the participants
Twenty-three participants were randomly selected from the 48 participants participating in the feasibility and pilot randomised trial in which this observational study was nested. Nineteen videos were randomly selected from the pool of 23 participants. Mean age (±SD) of participants was 44.2 (±9.3) years, and participants reported a high level of proficiency with phone applications usage (). Nine people (39%) reported undertaking walking or hiking, 11 people reported running (48%) and 17 people (74%) reported participating in other Achilles tendon sports and activities ().
Table 3. Participant characteristics (N = 23).
Table 4. Tendon loading sports and activities undertaken by participants.
Reproducibility
Telehealth rater and live rater agreement
In the standing position the sagittal criterion absolute agreement was 100% for both telehealth rater 1 and 2 when compared with the live expert rater, therefore the Kappa agreement was not calculated (see ).
Table 5. Telehealth and live rater agreement of assessing calf muscle exercise fidelity in standing and seated positions.
For the sagittal (seated position only), tempo, plantarflexion (PF), dorsiflexion (DF) and knee criterion absolute agreement was 84–100% and strength of agreement was moderate to almost perfect (Kappa telehealth rater 1 = 0.65–1.00 and Kappa telehealth rater 2 = 0.64 − 1.00). For the quality criterion, in standing telehealth rater 1 had almost perfect agreement (absolute agreement 100%, Kappa 1.00) whereas telehealth rater 2 had weak agreement (absolute agreement 79%, Kappa 0.57). For the quality criterion in the seated position rater 1 had moderate agreement (absolute agreement 84%, Kappa 0.73) and rater 2 had strong agreement (absolute agreement 95%, Kappa 0.83). Moderate or higher agreement was achieved for 95% of ratings (19/20 criteria).
Inter-rater agreement among telehealth raters
Inter-rater absolute agreement was 79 to 100% and the strength of agreement varied from weak to almost perfect (Kappa = 0.57 to 1.00) (). In the seated position, all of the criterion, excluding PF, had a weak agreement (absolute agreement 79–89%, Kappa 0.46–0.58). Almost perfect agreement was achieved for PF in seated position (see ). The tempo, DF and PF had a moderate agreement in the standing position (absolute agreement 89–95%, Kappa 0.73–0.76). In standing, the quality criterion had a weak agreement (absolute agreement 79% and Kappa 0.57). Forty-five % (5/11) ratings had moderate or greater agreement.
Table 6. Inter-rater agreement of telehealth assessment of calf muscle exercise fidelity from standing and seated positions.
Intra-rater agreement among telehealth raters
Intra-rater absolute agreement was >79% in both positions (standing: 79 to 100%; seated: 84 to 100%). Intra-rater strength of agreement was moderate to almost perfect for seated (Kappa = 0.65 to 1.00) and in standing, excluding the quality criterion, was also moderate to almost perfect (Kappa = 0.66 to 1.00). The quality criterion in standing had a weak intra-rater agreement for both raters (absolute agreement 79% and Kappa 0.46–0.57). Ninety percent (18/20) of ratings achieved moderate or higher ratings (see ).
Table 7. Intra-rater agreement of telehealth assessment of calf muscle exercise fidelity from standing and seated positions.
Discussion
We have shown that the calf exercise fidelity scale delivers moderate or stronger agreement for intra-rater reliability via telehealth assessment by relatively inexperienced telehealth raters with minimal training (2 h). In contrast, 50% of the ratings for inter-rater reliability had weak agreement between telehealth rater 1 and 2. Excluding the quality criterion, there was moderate to almost perfect agreement when comparing the live expert rater and telehealth raters assessments. Taken together, these findings suggest relatively inexperienced raters can assess calf raise exercise fidelity fairly comparably to a live experienced rater aside from the quality criterion. These raters also agree with themselves but less so with another inexperienced rater over telehealth.
There is currently no consensus regarding how calf raise testing and exercise should be performed [Citation20]. The criteria developed in this study were based on the current literature and expert consultation. Although there are no data that we are aware of linking these exercise fidelity criteria to outcomes, we propose that they may impact neuromuscular development and clinical outcomes in AT management. Performing the calf raise with adequate time under tension (tempo) influences neuromuscular [Citation33] and tendon adaptations [Citation13] and achieving adequate plantarflexion and dorsiflexion range ensures development of strength throughout range [Citation14]. Performing the calf raise in the sagittal plane increases calf work and reduces load on surrounding muscles such as the peroneals and tibialis posterior [Citation34]. Finally, bending the knee during a standing calf raise is a clinical observation related to poor strength among people with AT. The relationship between these criteria and neuromuscular and clinical outcomes should be explored in future work.
Undertaking the exercise (adherence) is a prerequisite to fidelity if it is assumed that the exercise itself has a therapeutic effect but in this study the focus was on exercise fidelity [Citation35]. Sancho et al. [Citation36] examined the feasibility of education and exercise supplemented by a pain-guided hopping intervention for male recreational runners with mid-portion AT. They reported overall fidelity to the prescribed sets, repetitions and load-intensity in their intervention was 50%, ranging from 22% to 64% for the various exercise investigated. The focus by Sancho et al. was on exercise volume and intensity which is difficult to compare to our exercise technique-related fidelity outcomes. Nevertheless, these studies do reinforce that exercise fidelity is a broad concept and achieving high exercise fidelity seems challenging and may necessitate implementation of new and specific strategies e.g., strategies to maximise behaviour change such as improved education and reinforcement via videos and specific feedback [Citation37].
There are several strengths of this study, including robust development of calf exercise fidelity criteria based on available literature and expert input. Other strengths include the pragmatic design that utilised telehealth raters with relatively limited clinical experience, use of freely and readily available videoconferencing technology, and affordable and portable phone tripods.
The findings should also be viewed in the context of the limitations of this study. The ability to detect calf raising onto the lateral foot rather than in sagittal plane was limited with the current set up. Ideally observing movement outside of the sagittal plane would require the camera to be positioned directly in front of the participant. We used one camera angle to determine the training errors which was not optimal for assessing all the fidelity criteria but may improve efficiency and clinical applicability of the assessment. There were also very few errors involving this criterion (0% in standing, 11% in seated position), hence the magnitude of Kappa is affected by the prevalence of this attribute [Citation32]. Although dedicated telehealth software with integrated features such as camera tilt and zoom are available e.g., eHAB® [Citation38], the purpose of this research was to evaluate a single camera position on ease of use and freely available software to minimise cost barriers to clinical implementation. Furthermore, we had a relatively small and homogenous sample of men with mid-portion AT, so our findings may not be generalisable to other AT populations. There is a potential that inter-rater reproducibility could be improved with increased training of the raters.
Not every internet connection is suitable for telehealth and insufficient connectivity can be a barrier for a successful telehealth assessment [Citation39]. The study did not test the influence of internet connection as assessors downloaded the videos prior to watching them, and were able to watch them as many times as needed. This does not reflect most clinical practice scenarios where physiotherapists will be watching the assessment in real time and will be relying on a suitable internet connection to make their assessment. Lastly, we did not assess validity which would have required comparison with a gold standard such as 3D motion analysis.
Implications and future directions
The calf exercise fidelity criteria developed can be used as an adjunct to assessment and management of people with Achilles tendinopathy. This research is a critical step towards developing the evidence base relating to telehealth and improving physiotherapist and consumer confidence in this emerging technology. Further work should explore whether these criteria are associated with clinical outcomes. Prior to any further testing of agreement, there should be further consideration of the “quality” (poorest over agreement) and “sagittal” criteria. The quality criterion was added by the researchers after observing cogwheeling in time with the metronome and fast dropping into dorsiflexion. If the desired tempo is achieved, these technique alterations may not influence neuromuscular development [Citation33]. The sagittal criterion was rarely observed in our cohort of people with AT, especially in standing, so thought should be given to its utility in this population. Our findings relate to people doing their exercises with a Smith machine and with an appropriate camera set up and quality. If these factors were altered this might change the generalisability of our findings. Camera set up issues could be mitigated by training; however, effective video quality and the use of a Smith machine may not always be available. Future work should also explore the reproducibility of the calf raise fidelity criteria among other health professionals (e.g., osteopaths) and other populations (e.g., post ankle sprain). Furthermore, the researchers caution against use of the calf raise fidelity criteria between different raters until future work demonstrates improved inter-rater agreement (e.g., via enhanced education and training of raters). We used less experienced telehealth raters to determine if lesser experienced physiotherapists (two and six years post qualification) can effectively assess exercise fidelity on telehealth when compared to a live expert rater. We have not, however, assessed whether having an expert physiotherapist completing the telehealth assessments would have increased inter-rater reliability between live and telehealth assessments which should be explored in the future.
Conclusion
Assessing calf exercise fidelity via videos recorded on Zoom® appears to demonstrate weak or greater agreement (vs expert live rating and over time) when undertaken by relatively experienced clinicians. Inter-rater agreement was lower suggesting this the criteria developed may be better suited to use by individual raters over time. Consideration should be given to modification or removal of criteria that were rarely observed (sagittal) or had the lowest agreement (quality).
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Grävare Silbernagel K, Crossley KM. A proposed return-to-sport program for patients with midportion Achilles tendinopathy: rationale and implementation. J Orthop Sports Phys Ther. 2015;45(11):876–886.
- de Jonge S, Van den Berg C, de Vos RJ, et al. Incidence of midportion Achilles tendinopathy in the general population. Br J Sports Med. 2011;5(13):1026–1028.
- Kujala UM, Sarna S, Kaprio J. Cumulative incidence of Achilles tendon rupture and tendinopathy in male former elite athletes. Clin J Sport Med. 2005;15(3):133–135.
- Abate M, Gravare Silbernagel K, Siljeholm C, et al. Pathogenesis of tendinopathies: inflammation or degeneration? Arthritis Res Ther. 2009;11(3):1–5.
- Martin RL, Chimenti R, Cuddeford T, et al. Achilles pain, stiffness, and muscle power deficits: midportion Achilles tendinopathy revision 2018: clinical practice guidelines linked to the international classification of functioning, disability and health from the orthopaedic section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2018;48(5):A1–A38.
- Malliaras P, Barton CJ, Reeves ND, et al. Achilles and patellar tendinopathy loading programmes. Sports Med. 2013;43(4):267–286.
- Kingma JJ, de Knikker R, Wittink HM, et al. Eccentric overload training in patients with chronic Achilles tendinopathy: a systematic review. Br J Sports Med. 2007;41(6):e3.
- Russell TG. Telerehabilitation: a coming of age. J Physiother. 2009;55(1):5–6.
- Doraiswamy S, Abraham A, Mamtani R, et al. Use of telehealth during the COVID-19 pandemic: scoping review. J Med Internet Res. 2020;22(12):e24087.
- Cottrell MA, Russell TG. Telehealth for musculoskeletal physiotherapy. Musculoskelet Sci Pract. 2020;48:102193.
- Peretti A, Amenta F, Tayebati SK, et al. Telerehabilitation: review of the state-of-the-art and areas of application. JMIR Rehabil Assist Technol. 2017;4(2):e7511.
- Hansen WB. Introduction to the special issue on adaptation and fidelity. Health Educ Res. 2013;113(4):260–263.
- Bohm S, Mersmann F, Arampatzis A. Human tendon adaptation in response to mechanical loading: a systematic review and meta-analysis of exercise intervention studies on healthy adults. Res Sports Med. 2015;1(1):1–8.
- Cook JL, Purdam C. Is compressive load a factor in the development of tendinopathy? Br J Sports Med. 2012; 146(3):163–168.
- Lunsford BR, Perry J. The standing heel-rise test for ankle plantar flexion: criterion for normal. Phys Ther. 1995; 175(8):694–698.
- Silbernagel KG, Gustavsson A, Thomeé R, et al. Evaluation of lower leg function in patients with Achilles tendinopathy. Knee Surg Sports Traumatol Arthrosc. 2006;14(11):1207–1217.
- Alfredson H, Pietilä T, Jonsson P, et al. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med. 1998;26(3):360–366.
- Beyer R, Kongsgaard M, Hougs Kjær B, et al. Heavy slow resistance versus eccentric training as treatment for Achilles tendinopathy: a randomized controlled trial. Am J Sports Med. 2015;43(7):1704–1711.
- Silbernagel KG, Thomeé R, Thomeé P, et al. Eccentric overload training for patients with chronic Achilles tendon pain–a randomised controlled study with reliability testing of the evaluation methods. Scand J Med Sci Sports. 2001;11(4):197–206.
- Hébert-Losier K, Newsham-West RJ, Schneiders AG, et al. Raising the standards of the calf-raise test: a systematic review. J Sci Med Sport. 2009;12(6):594–602. 1
- Hasani F, Haines T, Munteanu SE, et al. LOAD-intensity and time-under-tension of exercises for men who have Achilles tendinopathy (the LOADIT trial): a randomised feasibility trial. BMC Sports Sci Med Rehabilitation. 2021;13(1):1–6.
- Kottner J, Audigé L, Brorson S, et al. Guidelines for reporting reliability and agreement studies (GRRAS) were proposed. Int J Nurs Stud. 2011 1;48(6):661–671.
- Carcia CR, Martin RL, Houck J, et al. Achilles pain, stiffness, and muscle power deficits: Achilles tendinitis: clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2010;40(9):A1–26.
- de Vos RJ, Van Der Vlist AC, Zwerver J, et al. Dutch multidisciplinary guideline on Achilles tendinopathy. Br J Sports Med. 2021 1;55(20):1125–1134.
- Malliaras P, Kamal B, Nowell A, et al. Patellar tendon adaptation in relation to load-intensity and contraction type. J Biomech. 2013;46(11):1893–1899. 26
- Nawoczenski DA, DiLiberto FE, Cantor MS, et al. Ankle power and endurance outcomes following isolated gastrocnemius recession for Achilles tendinopathy. Foot Ankle Int. 2016;37(7):766–775.
- Neeter C, Thomee R, Silbernagel KG, et al. Iontophoresis with or without dexamethazone in the treatment of acute Achilles tendon pain. Scand J Med Sci Sports. 2003;13(6):376–382.
- Möller M, Lind K, Movin T, et al. Calf muscle function after Achilles tendon rupture. A prospective, randomised study comparing surgical and non‐surgical treatment. Scand J Med Sci Sports. 2002;12(1):9–16.
- Weber M, Niemann M, Lanz R, et al. Nonoperative treatment of acute rupture of the Achilles tendon: results of a new protocol and comparison with operative treatment. Am J Sports Med. 2003;31(5):685–691.
- Robinson JM, Cook JL, Purdam C, et al. The VISA-A questionnaire: a valid and reliable index of the clinical severity of Achilles tendinopathy. Br J Sports Med. 2001 1;35(5):335–341.
- McHugh ML. Interrater reliability: the kappa statistic. Biochem Med. 2012;15;22(3):276–282.
- Sim J, Wright CC. The kappa statistic in reliability studies: use, interpretation, and sample size requirements. Phys Ther. 2005; 185(3):257–268.
- Roig M, O’Brien K, Kirk G, et al. The effects of eccentric versus concentric resistance training on muscle strength and mass in healthy adults: a systematic review with meta-analysis. Br J Sports Med. 2009;43(8):556–568. 1
- Akuzawa H, Imai A, Iizuka S, et al. The influence of foot position on lower leg muscle activity during a heel raise exercise measured with fine-wire and surface EMG. Phys Ther Sport. 2017;28:23–28.
- El-Kotob R, Giangregorio LM. Pilot and feasibility studies in exercise, physical activity, or rehabilitation research. Pilot Feasibility Stud. 2018;4(1):1–7.
- Sancho I, Morrissey D, Willy RW, et al. Education and exercise supplemented by a pain-guided hopping intervention for male recreational runners with midportion Achilles tendinopathy: a single cohort feasibility study. Phys Ther Sport. 2019 1;40:107–116.
- Michie S, Johnston M, Carey R. Encyclopedia of behavioral medicine: behavior change techniques. Montreal (QC): Springer; 2020.
- Russell TG, Blumke R, Richardson B, et al. Telerehabilitation mediated physiotherapy assessment of ankle disorders. Physiother Res Int. 2010;15(3):167–175.
- Zhai Y. A call for addressing barriers to telemedicine: health disparities during the COVID-19 pandemic. Psychother Psychosom. 2021;4:1.