
Abstract
Purpose
To identify specific factors influencing the participation experiences of young people with cerebral palsy (CP) aged 15 to 26 years.
Materials and methods
A three-round Delphi survey study design was used. Consumers (young people with CP and caregivers) and health professionals were asked to generate and then rate items influencing positive and negative participation experiences. Qualitative content analysis and descriptive statistics were used to classify items across the family of Participation-Related Constructs (fPRC) framework.
Results
Sixty-eight participants completed Round I (25 consumers, 43 health professionals). Round II resulted in a consensus for all but two items, with Round III not required. The fPRC construct with the most items rated as extremely important for positive participation experiences was Environment–Availability, and for negative participation, experiences were Environment-Acceptability for both adolescents and young adults.
Conclusions
A consensus was reached on the most important items influencing the positive and negative participation experiences of young people with CP. These items should be prioritised when developing support services and allocating funding to improve the participation experiences of young people with CP.
IMPLICATIONS FOR REHABILITATION
This study is reporting consumer and professional consensus on the factors promoting positive and negative participation for young people with cerebral palsy.
Ensuring availability of appropriate activities and services is extremely important for enabling positive participation experiences.
Promoting acceptable attitudes of others is extremely important for alleviating negative participation experiences.
Introduction
Young people with cerebral palsy (CP) have been found to have reduced levels of participation compared with their typically developing peers [Citation1–5]. This has led to CP organisations promoting inclusion and active participation in all life areas as a key goal (e.g., The Australian and New Zealand CP strategy [Citation6]). To achieve this goal, it is essential to identify factors that contribute to positive or negative participation experiences for young people with CP, so that appropriate support and advocacy can be provided. Although to date, the literature on participation for people with CP has focused primarily on the school-aged years and little is known about the participation of people with CP as they transition into their young adult years [Citation2]. Therefore, it is necessary to obtain consensus on the most important factors impacting positive and negative participation experiences of young people with CP.
Participation is a complex, subjective, and multi-dimensional construct [Citation7]. The World Health Organization’s International Classification of Functioning, Disability, and Health (ICF) defines participation as “involvement in a life situation” with nine domains described across various life contexts such as education, employment, and community activities [Citation8]. In addition to these nine domains for Activities and Participation, the ICF also provides domains for Environmental Factors, Body Structures, and Body Functions. To assist with understanding how Participation occurs, the family of Participation-Related Constructs (fPRC) framework has been developed [Citation7,Citation9]. Within the fPRC, Participation is conceptualised as the interaction between Attendance and Involvement. Attendance refers to the objective element of “being there,” which can be measured by the frequency and diversity of experiences attended. Involvement refers to the subjective experience while participating, and includes affect, motivation, engagement, persistence, and social connection [Citation7,Citation9]. Like the ICF, the fPRC framework also considers constructs related to Participation such as Activity competence, Sense-of-self, Preferences, and the Environment [Citation7]. Activity competence refers to the ability to perform an activity to an expected standard. Sense-of-self refers to the individual’s confidence, satisfaction, and self-esteem. Preferences refers to the interests of the individual that hold value. The Environment refers to the influence of context and setting in terms of: (i) Availability, the provision of activities or services; (ii) Accessibility, the ability to access the activity or situation; (iii) Affordability, the financial, time, energy, and other resource constraints that impact attending; (iv) Accommodability, the ability of the situation to be adapted or modified; and (v) Acceptability, the person’s acceptance of the situation, and other people’s acceptance of the individual in the situation [Citation10]. Its thoroughness in classifying essential components of Participation makes the fPRC a useful framework for identifying and addressing the factors that can impact participation.
Recent studies have identified lower levels of participation for young people with CP when compared with typically developing peers. Young people with CP have been found to face participation challenges during the transition from adolescence to adulthood [Citation11–13] and when needing to adapt to new life roles [Citation14]. Young people with CP have been found to have particularly low levels of participation autonomy [Citation4,Citation15]. Schmidt et al. [Citation5] found the development of participation autonomy (e.g., freedom to make choices and participate based on their attitudes and reasoning) was delayed for all participants with CP (n = 189, aged 12 to 34 years) compared to typically developing peers into their adult years. Participants with more severe motor impairment (Gross Motor Function Classification System [GMFCS] Level III to V) had even less autonomous participation than those with milder motor impairment (GMFCS Level I and II), particularly in transportation, intimate relationships, employment, and housing [Citation5]. Similarly, recent studies involving young people with CP transitioning between adolescence to young adulthood have reported that greater impairments in cognition, communication, and motor abilities are correlated with decreased participation [Citation2,Citation16]. These studies have identified low participation levels for young people with CP. However, little is known about the specific factors causing this to occur.
External factors in the environment have been raised as a source of poorer participation for young people [Citation17]. A scoping review by Shahin et al. [Citation18] about workplace participation for people aged 18 to 35 years with brain-based disabilities found that all ICF environmental domains had the potential to impact workplace participation. Facilitators of better workplace participation included inclusive and flexible systems, well-defined policies, social support from family, friends, employers, and colleagues, physical accessibility, and the availability of assistive technology. A key barrier to workplace participation was the attitudes of colleagues and employers [Citation18]. In contrast, a study on the leisure participation of young adults with CP aged 18 to 41 years found that those with low participation reported environmental items had no influence, with mobility identified as a key influence [Citation19]. A longitudinal study by van Wely et al. [Citation20] followed up 53 youth with CP aged 16 to 21 years for 13 years showing that factors occurring in adolescence can predict future participation during adulthood, including gross motor ability, personal items (e.g., personality traits), and environmental factors (e.g., parenting style). Thus, it is likely that environmental factors do impact participation, however, a clear consensus on the most important factors is needed to assist in prioritising appropriate supports.
A well-utilised method for establishing consensus with consumers and professionals is the Delphi technique. Delphi studies have facilitated consensus on a variety of complex issues in CP research, such as developing tools [Citation21], establishing ICF core sets [Citation22], identifying important domains for evaluating therapeutic effects [Citation23], and research priorities [Citation24]. The Delphi process involves multiple survey rounds to generate items for consideration and then participants rate item relevance to establish group consensus [Citation25]. Delphi participants can include rehabilitation consumers, family members, clinicians, researchers, and policy makers [Citation26]. The Delphi technique offers many advantages. The anonymity between participants encourages individuals to participate, and reduces the risk of influential group dynamics, personality conflicts, or the influence of status [Citation27]. The flexibility and reflexivity of this technique allow the researcher to adapt the study to the research context, and for the participants to think through their responses at their own pace, enhancing the validity of responses, and reach to more remote participants [Citation27]. A Delphi technique provides an inclusive way to establish consensus on the most important factors impacting the participation of young people with CP. Findings would provide a better understanding of the participation experiences of young people with CP and highlight key areas for additional support, therapy priorities, and funding allocation.
Therefore, it is necessary to obtain consensus on the most important factors impacting the participation experiences of young people with CP. The objectives were to use a Delphi technique to (i) obtain consensus on the most important items contributing to either positive or negative participation experiences and (ii) compare the potential similarities and differences of these items between adolescence and young adulthood.
Method
Design
This study used a three-round Delphi survey design [Citation27]. This process involved asking consumers (young people with CP and caregivers of young people with CP) and health professionals (allied health and medical professionals) recurring questions to arrive at an informed group consensus on the most important items impacting the positive and negative participation experiences of young people with CP [Citation27].
Participants
Consumers included young people with CP (aged 15 to 26 years) and caregivers of young people with CP (aged 15 to 26 years). All participants provided responses to demographic questions during Round I. Consumers were recruited through the Queensland Cerebral Palsy Register, social media, and consumer subgroups of professional associations. Inclusion criteria for young people with CP were that they were: (i) aged between 15 to 26 years, (ii) proficient in English or able to provide an independent response with support from a translator, (iii) able to respond to an online or paper-based survey using supported communication techniques (e.g., multi-modality using both written and spoken, repeating information, paraphrasing and rewording, and/or using a communication partner), and (iv) that they had no concomitant diagnosis that would confound the results (e.g., Autism Spectrum Disorder). Inclusion criteria for caregivers were that they needed to be: (i) a primary caregiver (parent or legal guardian) of a young person with CP (as per the criteria, above) and not a temporary caregiver (e.g., provided by the Department of Child Safety, Youth, and Women) and (ii) proficient in English or able to provide an independent response with support from a translator.
Health professionals were recruited through (i) professional associations, social media, expression of interest via fliers, and emails to key groups and (ii) author contact details from papers about participation measures used with young people with CP identified in a systematic review [Citation28]. Inclusion criteria for health professionals were that they needed to be (i) clinicians or researchers with experience working with young people with CP aged 15 to 26 years and (ii) proficient in English or able to provide an independent response with support from a translator.
Procedures and analysis
In Round I, participants were asked to generate responses to open-ended questions developed by the researchers. In Round II, these responses were collated, and participants were asked to rate their importance. Each survey round was piloted with a young adult with CP before being sent to participants. Clear definitions and explanations of concepts such as Participation were provided within each survey round. Young people with CP aged 15 to 17 years and their caregivers were asked to answer questions about participation of adolescents (aged 15 to 17 years). Young adults with CP aged 18 to 26 years, their caregivers, and health professionals could respond to questions for adolescents, or young adults (aged 18 to 26 years), or both. Each participant’s communication support needs were accommodated. Participants were emailed a link to each survey round. They were able to complete the surveys using the most appropriate method for their communication skills, either: (i) electronically, via online survey software or email [Citation29]; (ii) on paper, with the survey sent through email or post; or (iii) via an interview with a speech pathologist (JQ), provided via Zoom or face-to-face.
Abductive qualitative content analysis [Citation30] was employed in that both inductive and deductive approaches were utilised to analyse data and report findings, respectively. To ensure rigour, one author (JQ) completed the initial coding. A second author (TR) examined and discussed all coding and categorisation to ensure the dependability of the interpretations [Citation31]. Authors LJ and MA also reviewed and approved all categorisation and assisted in resolving discrepancies. Data collection for this Delphi was completed between December 2020 and November 2021.
Round I: Item Generation
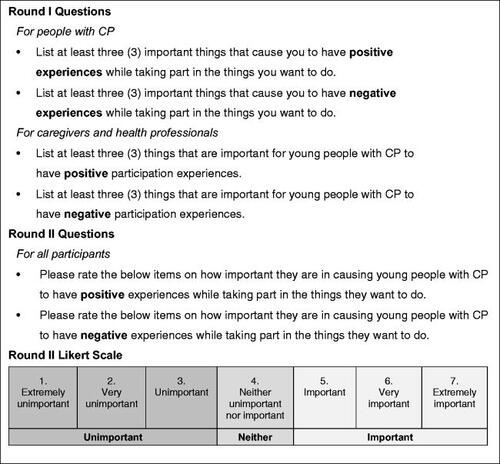
In Round I, participants were asked to generate responses to open-ended questions regarding contributors to the positive and negative participation experiences of young people with CP (). Generating items from open-ended questions instead of using a pre-determined items list was performed to reduce researcher bias in the items [Citation32]. Round I responses from consumers and health professionals were collated and analysed using inductive qualitative content analysis [Citation30,Citation33]. Each participant’s response was analysed for meaning units (words or statements that relate to a central meaning) which were then collated across participants to remove duplicates and establish items (subcategories) for rating in Round II.
Box 1. Questions asked to participants in Rounds I and II.
Round II: Consensus Round
In Round II, items generated in Round I from both consumers and health professionals were combined and presented back to all participants. To avoid any bias or order effect, items were presented to participants in a randomised order. Participants rated the importance of each item for contributing to more positive or negative participation experiences using a seven-point Likert scale from extremely unimportant to extremely important.
Responses from Round II were combined at each extremity (using Likert scale points: 1/2/3 unimportant, 4 neutral, or 5/6/7 important) and pooled for all participant groups to establish a group consensus on the most important items impacting participation for each age group [Citation34]. Consensus for an item was defined as at least 70% agreement [Citation35], in that items were considered important if at least 70% of consumers and health professionals provided a Likert scale response of 5, 6, or 7. Conversely, items were considered unimportant for causing positive or negative participation experiences when at least 70% of participants rated the item 1, 2, or 3 on the Likert scale. Discordant items that did not reach consensus were to be retained and presented again in Round III.
Round III: Final consensus Round
The purpose of Round III was to re-offer discordant items for final voting. Round III was not needed due to all but two items reaching consensus during Round II. The results presented below are therefore the outcomes following consensus in Round II.
Subsequent to obtaining consensus in Round II on items generated using inductive methods, deductive content analysis was then utilised to organise the items (subcategories) into categories. After reviewing the items as well as the possible participation frameworks in the current literature, categories corresponding to the fPRC framework constructs were determined to be the best match for data reporting, with all participant-generated items able to be appropriately categorised.
Results
Participants
Sixty-eight participants took part in this Delphi study, including 25 consumers (11 young people with CP and 14 caregivers of young people with CP) and 43 health professionals. Participant characteristics for consumers are presented in , and for health professionals in . All participants completed the survey rounds electronically.
Table 1. Consumer characteristics.
Table 2. Health Professional characteristics.
Round I: Item Generation
In Round I, participants generated 313 meaning units for adolescents, including 50 items (175 meaning units) for positive participation experiences and 33 items (138 meaning units) for negative participation experiences. Participants generated 211 meaning units for questions relating to young adults, including 46 items (116 meaning units) for positive participation experiences and 38 items (95 meaning units) for negative participation experiences Supplementary Appendix 1.
Using the fPRC framework for reporting, the most prevalent constructs identified in adolescents’ and young adults’ responses for positive participation in Round I were Environment-Availability (adolescents: 13 items, young adults: 15 items), followed by Environment-Acceptability (adolescents: 12 items, young adults: 7 items), and Participation-Involvement (adolescents: 4 items, young adults: 5 items). The most prevalent constructs identified in adolescents’ and young adults’ responses for negative participation were Environment-Acceptability (adolescents: 10 items, young adults: 12 items), followed by Environment–Accessibility (adolescents: 4 items, young adults: 4 items), and Environment–Availability (adolescents: 6 items, young adults: 9 items).
Round II: Consensus Round
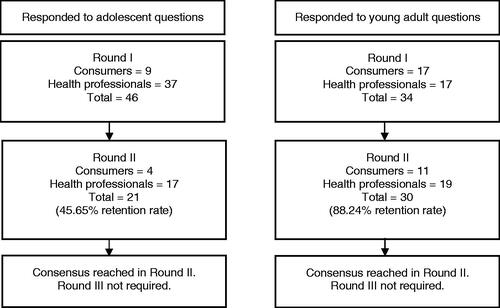
Thirty-five participants (51.47%) from Round I responded to Round II (), including 13 consumers (seven caregivers and six young people with CP) and 22 health professionals. All items reached the criteria for consensus, except two for young adults. One item was for positive experiences, “Having a good social image (e.g., having experiences to share social media),” and one item was for negative experiences, “Having to socialise (e.g., communicating, meeting new people).” The percent agreement and agreement distribution are provided for each item for adolescents in Supplementary Appendix II (a: positive experiences; b: negative experiences) and young adults in Supplementary Appendix III (a: positive experiences; b: negative experiences).
Figure 1. Participant response rates across the Delphi rounds and question sets for adolescents and young adults.
Items rated as extremely important
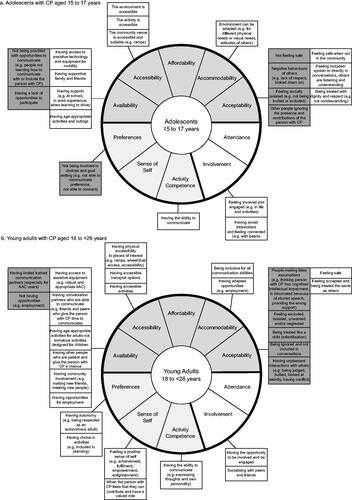
Almost all items (98.8%) were rated as important (rated 5/6/7), with no items reaching consensus for being not important (rated 1/2/3). However, several essential items received median ratings of extremely important (rated 7/7) such as “The community venue is accessible and suitable (e.g., ramps),” “Not being provided with opportunities to communicate (e.g., people not learning how to communicate with or include the person with CP),” and “Negative behaviours of others (e.g., lack of respect, looked down on).” presents the extremely important items, organised into categories using the fPRC framework.
Figure 2. Items considered extremely important to the positive (white boxes) or negative (grey boxes) participation experiences of a. Adolescents and b. Young adults with CP according to consumers (young people with CP and caregivers) and health professionals.
Discussion
This Delphi study has established consensus from consumers and health professionals about the most important items contributing to positive and negative participation experiences for young people with CP. We have also provided novel information on the factors influencing adolescents versus young adults to compare potential similarities and differences between the life stages on these items. Our findings show that similar fPRC constructs are perceived to have the most important influence on participation experiences during adolescence and young adulthood. However, there is some variation in the specific items between age groups. The fPRC construct with the most items rated as extremely important for positive experiences was Environment–Availability for both age groups. Similarly, the fPRC construct with the most items rated as extremely important for negative experiences in both adolescents and young adults was Environment-Acceptability, emphasising the importance of sociocultural factors of community attitudes, acceptance, and understanding. Although emphasis has been placed on the items that reached consensus for being extremely important, items of lesser importance to the group may still have significant relevance for individuals and should also be considered in any treatment planning.
Environment-Availability, defined as the appropriate provision of activities or services [Citation10], had the most items rated as extremely important for positive experiences for both adolescents and young adults. Availability items were diverse, such as “having access to assistive technology and equipment,” “having supportive family and friends,” “having conversation partners who are able to communicate,” “having age-appropriate activities and outings,” and “having opportunities for employment.” These findings highlight that young people want access to a broad range of age-appropriate activities and services to support more positive participation experiences. Similarly, Boucher et al. [Citation19] in Canada also identified the availability of services and adapted transport options as essential factors supporting participation in leisure activities. Both consumers and health professionals in our study identified age-appropriate activities, supports, services, and assistive technologies as critical to positive participation experiences. This finding emphasises the need to assess activity and service Availability as an integral part of the clinical reasoning process when working with young people with CP.
The fPRC construct with the most items rated as extremely important for negative participation experience was Environment-Acceptability for both adolescents and young adults. Maxwell et al. [Citation10,p. 65] explain Acceptability as “the person’s acceptance of the situation and other people’s acceptance of a person’s presence in a situation” and it was the attitudes and acceptance of others that both age groups emphasised. The finding that more Acceptability comments related to acceptance by others, versus acceptance of self in life situations, may have been influenced by the participant profile in our study, which included people with CP, caregivers, and health professionals. To obtain more in-depth information on the self-acceptance of people with CP, future studies could focus on gaining self-report from individuals with CP when reflecting on their lived experiences of participation in a range of life situations. Items rated as extremely important included a range of “negative behaviours of others,” such as a “lack of respect,” being “looked down on,” “isolated,” “excluded,” “false assumptions,” “being ignored and not included in conversations,” and “having unpleasant interactions.” These findings are supported by Towns et al. [Citation36], who highlighted how positive social influences could help establish more favourable participation environments for youth with CP. Similarly, Shahin et al. [Citation18] identified the attitudes of colleagues and employers as a key barrier to workplace participation for people aged 18 to 35 years with brain-based disabilities. Our Delphi study has extended these findings, highlighting that acceptance and attitudes impact young people with CP in many contexts during everyday participation. Our results emphasise the need to improve the function of the individual and the social environment. This need could be aided by targeted education and training focused on developing community understanding and compassion towards those with a disability, such as young people with CP. A study by Anaby et al. [Citation37] also advocated for addressing other adjustable aspects such as attitudinal, social, and institutional items. Future intervention and research need to address physical Accessibility as well as community Acceptability to ensure that interventions at the community level are part of routine management.
The construct of Participation-Involvement had several items rated as being extremely important for positive participation experiences. These items focused on “Having the opportunity to be involved and be engaged” during the experience, as well as the importance of “Having social interactions and feeling connected” and “Socialising with peers and friends.” These findings are similar to King et al. [Citation38], who emphasised how the meaningfulness of an experience influences engagement and that feeling a sense of fulfilment from the activity and feeling connected can all contribute to higher Involvement.
Facilitating Involvement in meaningful activities for young people with CP by collaborating with the individual is required to support the development of a Sense-of-self and Preferences. Several items within Sense-of-self and Preferences were extremely important to more positive participation experiences, especially when moving into young adulthood. These items emphasised the need for autonomy and choice, with the young person being “included in planning,” “being respected as an autonomous adult,” and feeling that they can “contribute and have a valued role.” However, young people with CP are less autonomous in their participation than the general population [Citation5]. These findings highlight that when working with young adults with CP, it is not only essential to have individualised and diverse support Available, but clinicians should collaborate with young people to adjust support to be age-appropriate and tailored to the individual.
Notably, the only extremely important item within Activity Competence for positive experiences was “Having the ability to communicate” across both adolescents and young adults. This finding does not mean that other items are unimportant but emphasises the value of communication across all ages. It is interesting that the importance of communication was emphasised so strongly by participants in this study, as most consumers were people with either no or mild communication difficulties. This finding highlights the importance of communication across all young people with CP, not just those with communication support needs. A recent study by Jacobson et al. [Citation2] also identified communication function as one of the most important determinants of social participation for young adults with CP (aged 20 to 22 years). Clinicians and researchers are encouraged to prioritise self-reports by young people about their participation experiences and preferences and to provide adequate interventions for communication development, communication technology, and training for communication partners [Citation28].
Recommendations
Participation is a key focus in the rights identified within the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) [Citation39]. Participation is also a key funding focus under the National Disability Insurance Scheme (NDIS) [Citation40]. Similarly, the Australia and New Zealand CP Strategy aims to promote inclusion and active participation in all life areas [Citation6]. Findings from this Delphi study support these priorities by identifying the items that make life experiences more challenging and that support positive experiences. Disability can be seen as a socially developed problem influenced by external community constraints on what are considered typical standards of functioning [Citation41]. This Delphi study emphasised that having appropriate supports available (Availability) and improving the acceptance of the individual with CP (Acceptability) could promote more positive experiences for people with CP during adolescence and young adulthood. It is essential to target socially created constraints such as these, to create positive change throughout the community and improve the participation of people with CP.
Strengths and limitations
The Delphi format facilitated the inclusion of responses from a wide range of participants, including persons with CP, their caregivers, and health professionals with clinical and research backgrounds across international locations. A comprehensive list of items was generated that can be used to advocate for appropriate support. There were some limitations. Although researchers provided participants with the option of completing the study via an interview with communication support strategies, all participants chose to complete the study independently online. This resulted in some perspectives of people with communication support needs being represented by proxy-report from caregivers. It would be beneficial for future studies to obtain the direct self-report of people with more severe communication difficulties, including users of augmentative and alternative communication (AAC).
This study also included more young adults than adolescents and attrition occurred between the survey rounds. This attrition was expected based on the response rates of previous Delphi studies. A higher number of participants in Round I were sought to counter this expected attrition in subsequent rounds and to ensure a suitably sized panel of respondents for all rounds [Citation42]. In Round II, higher rates of attrition were found for responses to questions about adolescence, with good retention for young adult questions. This higher attrition for questions about adolescence may have been impacted by participants being given a choice to rate either responses for adolescents and/or young adults, with most choosing to only rate young adult items in Round II. Although this study included health professionals from international locations, future research could include a larger number of international participants, and/or focus on comparing perspectives and experiences between countries or cultures. We would also encourage replication with more people with CP, especially from other cultures, to gain an even broader perspective. In addition, we would encourage future research to seek perspectives of other people in the community with whom young people with CP regularly interact, e.g., teachers, employers, trainers/coaches, friends, and/or extended family. This research could then incorporate other key frameworks such as the F-words for Child Development within the ICF framework seeking to gain perspective in areas such as fitness, friends, and fun [Citation43,Citation44].
Conclusion
This Delphi study extends the current understanding of the most important items impacting the positive and negative participation experiences of young people with CP by reaching a joint consensus among consumers and health professionals. There were similarities between adolescence and young adulthood in the main fPRC constructs identified, but some differences in the items. These items can be used to guide the selection of appropriate services and support to improve the participation of young people with CP. Results emphasise the importance of the Availability of diverse activities and services to support positive experiences and the need for further advocacy and education to increase the Acceptance and understanding towards young people with CP.
Ethics approval
Ethical approval was granted by the NHMRC-registered Human Research Ethics Committees of Cerebral Palsy League of Queensland (EC00417) and The University of Queensland (EC00456/7).
Supplemental Material
Download PDF (143.5 KB)Supplemental Material
Download PDF (142.4 KB)Supplemental Material
Download PDF (64.9 KB)Acknowledgements
The authors wish to thank all consumers and health professionals who participated in this study and the Queensland Cerebral Palsy Register for recruitment support.
Disclosure statement
No potential conflict of interest was reported by the author(s). The authors have stated that they had no interests that might be perceived as posing a conflict or bias.
Additional information
Funding
References
- Bjornson K, Kobayashi A, Zhou C, et al. Relationship of therapy to postsecondary education and employment in young adults with physical disabilities. Pediatr Phys Ther. 2011;23(2):179–186.
- Jacobson D, Löwing K, Hjalmarsson E, et al. Exploring social participation in young adults with cerebral palsy. J Rehabil Med. 2019;51(3):167–174.
- Reddihough DS, Jiang B, Lanigan A, et al. Social outcomes of young adults with cerebral palsy. J Intellect Dev Disabil. 2013;38(3):215–222.
- Rožkalne Z, Mukāns M, Vētra A. Transition-age young adults with cerebral palsy: level of participation and the influencing factors. Medicina. 2019;55(11):737.
- Schmidt AK, van Gorp M, van Wely L, et al. Autonomy in participation in cerebral palsy from childhood to adulthood. Dev Med Child Neurol. 2020;62(3):363–371.
- Badawi N, Honan I, Finch-Edmondson M, et al. The Australian & New Zealand cerebral palsy strategy. Dev Med Child Neurol. 2020;62(8):885.
- Imms C, Granlund M, Wilson PH, et al. Participation, both a means and an end: a conceptual analysis of processes and outcomes in childhood disability. Dev Med Child Neurol. 2017;59(1):16–25.
- World Health Organization. ICF: international classification of functioning, disability and health/World health organization. Geneva: World Health Organization; 2001.
- Imms C, Adair B, Keen D, et al. “Participation”: a systematic review of language, definitions, and constructs used in intervention research with children with disabilities. Dev Med Child Neurol. 2016;58(1):29–38.
- Maxwell G, Alves I, Granlund M. Participation and environmental aspects in education and the ICF and the ICF-CY: findings from a systematic literature review. Dev Neurorehabil. 2012;15(1):63–78.
- Gorter J, Roebroeck M. Transition to adulthood: enhancing health and quality of life for emerging adults with neurological and developmental conditions. In: Ronen GM, Rosenbaum PL, editors. Life quality outcomes in children and young people with neurological and developmental conditions. London: Mac Keith Press; 2013. p. 302–313.
- Imms C. Children with cerebral palsy participate: a review of the literature. Disabil Rehabil. 2008;30(24):1867–1884.
- Moll LR, Cott CA. The paradox of normalization through rehabilitation: growing up and growing older with cerebral palsy. Disabil Rehabil. 2013;35(15):1276–1283.
- Arnett JJ. Emerging adulthood. A theory of development from the late teens through the twenties. Am Psychol. 2000;55(5):469–480.
- Sandström K. The lived body - experiences from adults with cerebral palsy. Clin Rehabil. 2007;21(5):432–441.
- van Gorp M, Roebroeck E, van Eck M, et al. Childhood factors predict participation of young adults with cerebral palsy in domestic life and interpersonal relationships: a prospective cohort study. Disabil Rehabil. 2020;42(22):3162–3171.
- Sienko S. Understanding the factors that impact the participation in physical activity and recreation in young adults with cerebral palsy (CP). Disabil Health J. 2019;12(3):467–472.
- Shahin S, Reitzel M, Di Rezze B, et al. Environmental factors that impact the workplace participation of Transition-Aged young adults with Brain-Based disabilities: a scoping review. Int J Environ Res Public Health. 2020;17(7):2378.
- Boucher N, Dumas F, Maltais DB, et al. The influence of selected personal and environmental factors on leisure activities in adults with cerebral palsy. Disabil Rehabil. 2010;32(16):1328–1338.
- van Wely L, van Gorp M, Tan SS, et al. Teenage predictors of participation of adults with cerebral palsy in domestic life and interpersonal relationships: a 13-year follow-up study. Res Dev Disabil. 2020;96:103510.
- Hidecker MJC, Paneth N, Rosenbaum PL, et al. Developing and validating the communication function classification system for individuals with cerebral palsy. Dev Med Child Neurol. 2011;53(8):704–710.
- Raji P, Hassani Mehraban A, Aliabadi F, et al. Content validity of the comprehensive ICF core set for children with cerebral palsy aged 0-6 years: iranian occupational therapists perspective. Iran J Child Neurol. 2018;12(3):40–58.
- Vargus-Adams JN, Martin LK. Measuring what matters in cerebral palsy: a breadth of important domains and outcome measures. Arch Phys Med Rehabil. 2009;90(12):2089–2095.
- McIntyre S, Novak I, Cusick A. Consensus research priorities for cerebral palsy: a delphi survey of consumers, researchers, and clinicians. Dev Med Child Neurol. 2010;52(3):270–275.
- Murry JW, Jr, Hammons JO. Delphi: a versatile methodology for conducting qualitative research. Rev High Educ. 1995;18(4):423–436.
- Heinemann AW, Tulsky D, Dijkers M, et al. Issues in participation measurement in research and clinical applications. Arch Phys Med Rehabil. 2010;91(9 Suppl):S72–S76.
- Donohoe H, Stellefson M, Tennant B. Advantages and limitations of the e-Delphi technique. Am J Health Educ. 2013;43(1):38–46.
- Quartermaine J, Rose T, Auld M, et al. Participation measures that evaluate attendance and involvement for young people aged 15 to 25 years with cerebral palsy: a systematic review. Disabil Rehabil. 2023. DOI: 10.1080/09638288.2023.2207042
- Qualtrics. Qualtrics software. UT, USA: 2019.
- Graneheim UH, Lindgren BM, Lundman B. Methodological challenges in qualitative content analysis: a discussion paper. Nurse Educ Today. 2017;56:29–34.
- Koch T. Establishing rigour in qualitative research: the decision trail. J Adv Nurs. 2006;53(1):91–100.
- Sinha IP, Smyth RL, Williamson PR. Using the delphi technique to determine which outcomes to measure in clinical trials: recommendations for the future based on a systematic review of existing studies. PLOS Med. 2011;8(1):e1000393.
- Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112.
- Diamond IR, Grant RC, Feldman BM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of delphi studies. J Clin Epidemiol. 2014;67(4):401–409.
- De Meyer D, Kottner J, Beele H, et al. Delphi procedure in core outcome set development: rating scale and consensus criteria determined outcome selection. J Clin Epidemiol. 2019;111:23–31.
- Towns M, Lindsay S, Arbour-Nicitopoulos K, et al. Balance confidence and physical activity participation of independently ambulatory youth with cerebral palsy: an exploration of youths” and parents” perspectives. Disabil Rehabil. 2022;44(11):2305–2316.
- Anaby D. Towards a new generation of participation-based interventions for adolescents with disabilities: the impact of the environment and the need for individual-based designs. Dev Med Child Neurol. 2018;60(8):735–736.
- King G, Rigby P, Batorowicz B. Conceptualizing participation in context for children and youth with disabilities: an activity setting perspective. Disabil Rehabil. 2013;35(18):1578–1585.
- United Nations. Convention on the Rights of Persons with Disabilities. 2006. Available from https://www.un.org/development/desa/disabilities/convention-on-the-rights-of-persons-with-disabilities.html.
- Reddihough DS, Meehan E, Stott NS, et al. The national disability insurance scheme: a time for real change in Australia. Dev Med Child Neurol. 2016;58:66–70.
- Piskur B, Daniels R, Jongmans MJ, et al. Participation and social participation: are they distinct concepts? Clin Rehabil. 2014;28(3):211–220.
- de Villiers MR, de Villiers PJ, Kent AP. The delphi technique in health sciences education research. Med Teach. 2005;27(7):639–643.
- Rosenbaum P, Gorter JW. The “F-words” in childhood disability: i swear this is how we should think!. Child Care Health Dev. 2012;38(4):457–463.
- Rosenbaum PL. The F-words for child development: functioning, family, fitness, fun, friends, and future. Dev Med Child Neurol. 2022;64(2):141–142.