
Abstract
Purpose
Returning to work is an important goal after stroke, not only as a recovery indicator but also for facilitating independent living and improved social identity. The aim of this study was to explore the lived experiences of vocational rehabilitation and the return to work pathway after stroke.
Method
Qualitative data were collected through semi-structured interviews with purposively selected participants who had participated in a vocational rehabilitation trial. All participants were employed at the time of their stroke and were community-living. Interviews were undertaken by occupational therapists and were transcribed verbatim before data were thematically analysed using a framework approach.
Results
Sixteen participants were interviewed, seven received specialist vocational rehabilitation and nine received usual clinical rehabilitation. Three major themes were identified which highlighted the importance of tailored vocational rehabilitation to address the challenges that arise when returning to the workplace. Stroke survivors perceived the most beneficial components of the specialist vocational rehabilitation intervention to be employer liaison support, fatigue management, and support for cognition and executive processing skills.
Conclusions
Vocational rehabilitation was perceived to provide an opportunity to influence working after stroke, although areas of unmet need were highlighted. Findings provide direction for the development of future stroke-specific vocational rehabilitation programs.
IMPLICATIONS FOR REHABILITATION
Psychosocial (emotional) and cognitive (memory and planning) changes along with post-stroke fatigue were perceived to be the greatest barriers faced on returning to work and should be key areas for intervention within a vocational rehabilitation program.
Vocational rehabilitation interventions should be tailored to each participant, incorporating elements perceived to be important to stroke survivors, including workplace liaison, employer communication and psychological support.
Workplaces may benefit from access to information about the range of physical, cognitive and language deficits associated with stroke, and the potential impact these may have on work skills.
Introduction
Stroke is one of the leading causes of disability among adults worldwide [Citation1,Citation2] leading to subsequent physical, cognitive and language impairments. While the overall incidence of stroke is falling, the rate is rising among those of working age [Citation3], contributing to large productivity losses from premature mortality, time off work and lower employment as a result of stroke [Citation4]. An estimated 126,000 Australians aged under 65 are living with the impact of stroke [Citation4], and many of these survivors will be unable to return to work or return to their previous role. Recent data suggests that more than a third of working age stroke survivors have not returned to work by 12-months [Citation5] and that most (even those who have returned to work) identify an unmet need with respect to work [Citation6]. While some stroke survivors of working age may achieve a good physical recovery, they may still struggle with “hidden” symptoms impacting daily performance, including fatigue, sleep problems, cognitive impairment, depression and anxiety [Citation7]. Understanding both the clinical rehabilitation needs alongside work-specific rehabilitation goals is key in this population [Citation8].
Successful reintegration back to work after stroke is understood to improve long-term community participation, quality of life and maximise economic potential. Supporting resumption of meaningful activities, including employment, is a key focus for clinical rehabilitation, and synthesised evidence demonstrates the potential for targeted vocational rehabilitation to address the work disengagement that occurs after stroke [Citation8]. Two recent systematic reviews of vocational rehabilitation after stroke identified there is limited research into stroke-specific vocational interventions, particularly a lack of studies evaluating early return to work programs and assessing specific program components [Citation8,Citation9]. Furthermore, there is a lack of research exploring the experience of vocational rehabilitation from the perspective of stroke survivors themselves, so as to better understand the impact of return-to-work interventions that may be provided early in the post-stroke phase.
Several [Citation10–13] qualitative studies have previously sought to understand the lived experience of returning to work following stroke. These studies summarise the expressed barriers to participating in work following stroke and describe work-related and personal facilitators to return to work. While some mention the use of vocational services, none specifically sought to explore the experience and processes of participating in vocational rehabilitation early after stroke either within usual clinical rehabilitation or as part of a specialist clinic. This focus on understanding the views of people with lived experience is critical because these have the potential to inform rehabilitation programs designed to support the process of returning to work. Therefore, the aim of this qualitative study was to explore stroke survivors’ experiences of vocational rehabilitation and return to work pathways.
Methods
Study design
This study used a descriptive and exploratory approach and was conducted alongside a randomised controlled trial (the Work trial [Citation14]). The decision to explore experiences and perceptions of participants was made during the planning phase for the trial. Semi-structured interviews were conducted in Victoria. Alfred Health Human Research Ethics Committee approved the research (490/19) and all participants provided written, informed consent prior to interview.
Vocational rehabilitation intervention
During the trial, participants randomised to the intervention group received specialist vocational rehabilitation that was individually tailored to the return to work goals of each participant [Citation14]. Delivered in hourly sessions weekly (for up to 12 weeks), an occupational therapist began with an assessment of the individual’s stroke-related impairments and their work role. After determining their work limits and capabilities, likely challenges, and the feasibility of returning to the role, occupational therapists coordinated a tailored response with all stakeholders. The response included negotiating workplace adjustments, monitoring progress, establishing daily routines, and exploring alternative work roles if indicated [Citation14]. The usual care (clinical rehabilitation) group did not receive a specialised vocational rehabilitation intervention but may have received some vocational rehabilitation interventions to address their return to work goal from their general rehabilitation program. General rehabilitation programs in Australia typically employ occupational therapists, physiotherapists, speech therapists and, in some services, psychologists. While the focus of general rehabilitation is often at the level of impairment and activity performance, such programs do often address pre-vocational goals. They do not, however, typically involve specialist vocational rehabilitation services [Citation12]. Instead, a national disability insurance scheme and national disability employment services may provide specialist vocational support following general rehabilitation for those eligible.
Participants and recruitment
Of the 34 participants included in the randomized controlled trial, a subset that included both intervention and usual care group participants were purposively identified as possible candidates for the qualitative study, and invited to participate. Inclusion criteria for the trial were working at time of stroke (<4 months prior) and having a current goal to return to working. For the qualitative study, a sampling matrix was developed at study design to obtain views from a mix of women and men who were at different stages of their career at time of stroke and who had a range of employment arrangements (studying, casual, part-time, fulltime), job categories, and return to work outcomes (unemployed, underemployed, employed). We contacted potential participants sequentially by telephone according to the purposive sampling matrix; this recruitment procedure was used to maximize the heterogeneity of the sample while sample size was dictated by inductive thematic saturation, where no new codes or themes were being generated during the analysis [Citation15].
Data collection
Interviews were conducted via videoconferencing to participants’ homes or via telephone between December 2021 to March 2022. The three interviewers (SA, ES, KM) were accredited occupational therapists with experience in providing vocational rehabilitation, but were not involved in the design of the clinical trial and did not have any prior relationship with participants. Participants were aware of the professional background of the interviewers; however, it is unknown whether this knowledge could have impacted on participants’ willingness to talk openly about experiences, or how this knowledge might have shaped what was said. All interviewers completed formal training in working with people with speech and language impairments (e.g. aphasia) and were experienced in conducting qualitative interviews for research.
Participants were given the lead in setting the pace of the interview. By deliberately adopting a “back seat” approach in setting the scene for the interview to take place, the researchers hoped that participants would feel they were exercising a measure of control over the interview process. Members of the research team involved in conducting interviews (SA, ES, KM) were acutely sensitive to the possibility that focusing on the research topic could potentially provoke feelings of sadness and/or stress in participants concerning the disclosure of work and work outcomes. At the end of each interview, researchers took time to ensure that participants were not feeling distressed by their participation.
The semi-structured interview guide (see ) explored participants experiences of rehabilitation therapies that supported the goal of returning to work after stroke, suggested improvements to the provision of vocational rehabilitation, and their opinions about the training, support, equipment, and information provided. Participants were asked about their experiences of returning to work after stroke, and any changes in their physical and psychological wellbeing whilst taking part in the intervention. The interview guide was developed based on the research aims and previous qualitative studies conducted with stroke survivors. Probes were used to clarify or expand on the participants responses. Consent was provided for interviews to be audio recorded and transcribed.
Table 1. Semi-structured interview guide.
Data analysis
A thematic analysis was undertaken using a framework approach [Citation16]. The analysis was performed by NM who is a trained qualitative researcher with a background in clinical medicine and no prior involvement in the clinical trial. Transcripts were entered into NVivo 20 (QSR International, Doncaster), a software package used to manage and organise qualitative data. To commence the analysis, transcripts were read multiple times for familiarity while making notes based on content, meaning and the aim of the study. Using an inductive approach, analysis proceeded with line-by-line open coding of transcripts. After completing coding on the first six transcripts, the analysis team (NM, SR) met to discuss codes and develop a working analytical framework. This framework was then applied by indexing subsequent transcripts using existing categories and codes, with the addition of new codes as required. An iterative process was used to refine the analytic structure and create a final thematic framework [Citation17]. summarises the credibility and trustworthiness of the research methods. At significant points during data analysis, the researchers most closely involved in data collection (SA, ES, KM) and the analysis (NM, SR) met with members of the wider research team with extensive clinical experience (SOK, KR, NAL), to discuss codes and categories and the interpretation of quotes.
Table 2. Qualitative validation criteria.
Results
Demographics
Participant characteristics are provided in . A total of 16 people were interviewed, including seven who received specialist vocational rehabilitation in addition to their general clinical rehabilitation and nine who received only clinical rehabilitation. Approximately half were women (n = 9, 56%), and ages ranged from 23 to 71 years at the time of recruitment. All were less than four months post-stroke (range 4 days to 3 months) and six participants had post-stroke communication impairments (38%) at the time of recruitment. Of those who experienced communication impairments, all experienced difficulties with expression, discourse and social communication (n = 6), most with auditory comprehension (n = 5) and reading comprehension (n = 4) while two also experienced difficulty with written expression.
Table 3. Participant characteristics (total participants = 16), n(%) unless otherwise stated.
Themes
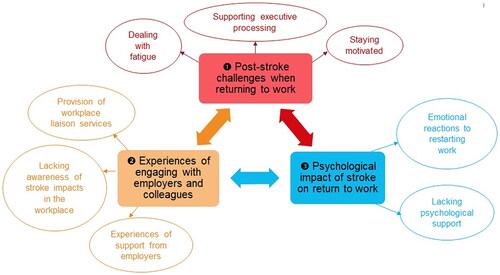
We identified three major themes as outlined in ; (1) post-stroke challenges when returning to work, (2) experiences of engaging with employers and colleagues following stroke, and (3) the psychological impact of stroke on return to work. Selected quotations to illustrate themes are provided and are followed by a participant number identifier and whether the participant was part of the intervention (specialist vocational rehabilitation) or usual care (clinical rehabilitation) group.
Figure 1. Themes and subthemes from qualitative data analysis.
Post-stroke challenges when returning to work
Dealing with fatigue
Many participants identified fatigue as a key issue which negatively impacted on their return to work following stroke. Participants struggled to function at work due to fatigue, and this also impacted their participation in usual rehabilitation as well as home life. Some participants reflected that they pushed themselves to increase their work hours too soon or felt pressured to increase work capacity due to staffing demands, which exacerbated their fatigue.
The biggest struggle for me in returning to work is the fatigue, physically it’s not a huge problem because I sit at a computer desk… It’s fatigue, and I find that is really something that has been hard to help through therapies. (Participant 1, clinical rehabilitation)
Several participants arranged reduced work hours or modified duties to combat fatigue and readjust to work. Participants who received specialist vocational rehabilitation benefitted from fatigue management strategies such as a structured and gradual return to work and adapting their work schedule to accommodate their energy levels.
We worked on the fatigue, with a report every week about the fatigue, what was difficult for me to do, and which activity. When I was ready to go back to work, having a plan and organise how much I was going to start working, my hours – to the half an hour, which was pretty awesome. Very structured to help me go back to work. (Participant 12, specialist vocational rehabilitation)
Supporting executive processing
Participants reported a variety of cognitive deficits post stroke, including memory impairment, and difficulty with reading and writing at work. Some reported that their usual work tasks took significantly longer to complete. Participants who received specialist vocational rehabilitation liked that the return to work program provided training and strategies for memory, as well as higher order executive processing, such as planning and structuring work activities.
[The occupational therapists] helped me understand why I forget things, and that’s why I do it on the whiteboard and on the calendar. (Participant 8, specialist vocational rehabilitation)
In contrast, participants who received clinical rehabilitation noticed a lack of cognitive skills therapy in their rehabilitation, and perceived they needed more advanced memory and literacy rehabilitation to prepare them for the demands of the workplace. Some participants explained that although they received rehabilitation for speech and memory, their therapy was not complex enough to prepare them for the rigors of functioning in a professional environment.
Staying motivated
Participants who received specialist vocational rehabilitation felt motivated during their recovery journey, as it provided a structured and consistent plan which kept them accountable. These participants liked having a goal to work towards, which offered stability and a sense of control over their progress.
The consistency of the therapy was very, very helpful, to have something structured and regular. I was really looking forward to the appointments. (Participant 12, specialist vocational rehabilitation)
In contrast, participants who received clinical rehabilitation felt they needed more input from therapists to maintain motivation and accountability in their return to work journey. These participants felt they lacked strategies to keep themselves motivated and focused on work-related tasks at work and would have benefitted from specific therapy to address this.
Perhaps I could have done more instigation-type therapy might have been good… Getting fire in the belly…Getting started yes, and also following it through to the end. Starting something, make sure you finish it properly. A very important aspect, because just to start something, and not see it through is a waste of time … It’s a bit hard on your own, you’ve got to instigate yourself and get things going. (Participant 16, clinical rehabilitation)
Experiences of engaging with employers and colleagues following stroke
Provision of workplace liaison services
Participants found it helpful when therapists liaised with their workplace to assist them to communicate with employers about return-to-work expectations, timelines, and negotiating modified work hours and duties. Participants described varying levels of support with workplace liaison depending on their specific needs; some participants managed communication themselves with some assistance from their trial therapist, such as receiving help to write emails to their manager. Other participants reported that their therapist took an active role in workplace liaison, including establishing initial contact and regularly speaking with employers on behalf of the patient.
[The occupational therapist] was pretty awesome because she was willing to communicate with, for example, the owners, where I work. (Participant 12, specialist vocational rehabilitation)
However, not all participants received support with employer communication as part of their specialist vocational rehabilitation. Some participants felt that they needed more guidance to manage communication in their specific employment context, such as approaching the employer to advocate for modified duties. One participant explained that they felt too nervous to approach their employer to discuss how to transition back to work and as a result they have not yet returned to work (Participant 10, specialist vocational rehabilitation).
Lacking awareness of stroke impacts in the workplace
All participants noted that there was a gap in the knowledge of employers and co-workers regarding the impact of stroke, and they highlighted the need for more education and training for workplaces. Some participants remarked that their colleagues did not know what a stroke is, what impairments might result, or what kind of support would be helpful. This was particularly relevant for participants with aphasia, who found that their colleagues expected a stroke survivor to have physical impairments rather than language.
I still had people that I worked with… [Citation18] I feel did not understand the severity of what happened, or did not understand the condition. For other people a stroke is something that happens to old people, that does not happen to young people. Physically, we probably also look better. Some disabilities, especially with aphasia, I think because you don’t physically really see it, people don’t realise just how much you can struggle with your speech or anything. (Participant 12, specialist vocational rehabilitation)
Some participants educated their colleagues themselves, by sharing their story to raise awareness of their condition. They explained to their colleagues how to help them at work, for example, asking to be prompted when stuck with word-finding. Participants suggested that employers should be provided with stroke education and/or training to increase awareness and understanding of stroke impacts. They explained that preparing employers to support stroke survivors at work would help ease their transition back to the workplace.
I think it would be quite beneficial if more employers had a bit more of an understanding of the effects after a stroke, and how to help people who have had a stroke get back into the workforce. (Participant 2, specialist vocational rehabilitation)
Experiences of support from employers
Participants experienced mixed responses from employers and colleagues when returning to work following their stroke. Most participants described a supportive workplace, with colleagues who regularly checked in to see how they were going and offered their support. Participants appreciated when employers supported them to take time off work without pressuring them to return and maintained contact to encourage them back to work when ready.
I’ve maintained contact with my workplace the whole time… They visited me in hospital, I’ve maintained contact since I’ve been out. We’ve got Christmas staff drinks tonight, but I’ll be going to the Christmas lunch. They’re really supportive, and looking forward to having me back next year, so that’s good. (Participant 7, clinical rehabilitation)
However, some participants had difficulty returning to work because of unhelpful and obstructive employers. They reported that employers were unwilling to adapt to their needs or simply refused to discuss a suitable role for them to return to. One participant explained that they left a workplace because their employer was totally out of place about what I needed for my recovery or adjusting to my needs (Participant 12, specialist vocational rehabilitation). These participants reported that their employers did not communicate openly with them about returning to work, for example, not consulting them when arranging a return-to-work plan.
When I went to work, all these ideas from my boss… he said certain things we should do and not do. They didn’t ask. They probably got told by other people what we should and shouldn’t do with groups of people… No one checked. (Participant 15, clinical rehabilitation)
Psychological impact of stroke on return to work
Emotional reactions to restarting work
Participants spoke about the emotional and psychological challenges of their post-stroke recovery and how this impacted on their return to work. They described feeling scared and overwhelmed at the prospect of going back to work and felt unsure if they were really ready. Some participants made the decision to delay going back to work or they stopped working altogether because they felt that they could no longer do their job effectively and they didn’t want to be a burden to their colleagues. Moreover, several participants suffered their stroke in the workplace, which compounded the stress of returning to work. These participants explained that going back to work triggered fears and anxiety because of reliving their traumatic experience. However, other participants felt apprehensive but also excited, because they were looking forward to seeing their work colleagues.
[Returning to work] was terrifying, it was really scary. I think just being in the real world and talking to people because the only people I talked to were my therapists and my family. When I went back it was really scary. You sort of freeze up for the first week, you just freeze because you’re so scared. I put off all my work for the first week because I was worried, and it was quite confronting as well going back. (Participant 6, specialist vocational rehabilitation)
Some participants struggled to balance their specialist vocational rehabilitation commitments with other life priorities. One participant questioned the importance of return to work rehabilitation following stroke, because they perceived other recovery and life goals were more important to them, and should be given more attention than work. This participant gave feedback regarding the timing of the program, stating that for them, it was introduced too early in their stroke recovery. They explained that they did not feel emotionally ready to address the meaning of work nor the idea of going back to work, and would have preferred to begin work-related interventions at a later stage in their rehabilitation.
I think, too, what I’m still struggling with is the value of work in regard to having a stroke and, I guess, nearly dying and wondering why are we focusing so much on returning to work when there is so much more in my life that I would like to achieve… Particularly after my stroke, I was like there are so many more fundamental things about how I’m able to function, and my mental health, and stuff like that, where it’s kind of like, yes, I think we should focus on these things a bit more rather than focusing on getting me back to work. (Participant 1, clinical rehabilitation). Other participants thought that the timing was appropriate, with one person stating, the earlier the better (Participant 4, specialist vocational rehabilitation).
Lacking psychological support
Several participants across both the specialist intervention and standard clinical rehabilitation groups expressed that there was a lack of psychological and peer support available to them during their post-stroke rehabilitation and while returning to work. These participants felt that emotional issues played a significant role in their recovery, and some suggested that this could have been addressed by linking in counselling services as part of routine care. Participants commented that referral to mental health services could be offered during their rehabilitation, including having access to a list of clinicians with a background in treating stroke patients. Also, several participants indicated their care could be better supported with improved access to peer support groups, offering the opportunity to connect with other stroke survivors and share experiences. One participant with post stroke aphasia described the experience of participating in a group speech therapy session, stating, it was good because you can converse with other people that [have] the same issues as me (Participant 13, specialist vocational rehabilitation).
The emotional needs and everything, that was something that I really needed on top of my rehabilitation. (Participant 12, specialist vocational rehabilitation)
Discussion
This study provides qualitative insights on the experience of returning to work following stroke, and the specific impact of vocational rehabilitation interventions on this experience. Participants who received specialist vocational rehabilitation identified aspects of their intervention program that were most helpful, especially support with workplace liaison, graded return to work hours, and support to gradually increase not only work hours but also work demands. They expressed that specialist vocational rehabilitation helped them develop strategies to manage common post-stroke challenges such as fatigue, memory impairment and cognitive issues. Perspectives from participants who only received usual care reinforced this finding, as they identified a lack of high-level (“complex”) cognitive therapy within their clinical rehabilitation programs, as well as a lack of motivation and accountability in their return to work journey. Previous literature supports our results that vocational rehabilitation tailored to address cognitive abilities and fatigue management is a key facilitator of returning stroke survivors back to work [Citation19]. Our findings add that the timing of these interventions are feasible, perceived as helpful in the early stages of recovery but need to be tailored to the needs of each individual stroke survivor.
Many participants across both intervention and usual care (clinical) rehabilitation groups reported a lack of awareness and understanding about stroke among their employers and colleagues. Previous qualitative studies have also highlighted limited knowledge among employers about stroke impairment, reflected in poor engagement with workplace rehabilitation [Citation20,Citation21]. Lack of understanding from co-workers may be especially relevant for people with post-stroke aphasia, as these participants found that their colleagues did not understand that stroke can impair language rather than physical abilities. This finding reinforces evidence from a recent interview study with stroke survivors with aphasia, who explained that their employers lack of knowledge about aphasia was a key barrier to returning to work [Citation22].
Addressing employer awareness and education about stroke was raised by participants as an important suggestion to improve post-stroke rehabilitation care. Other studies have reported that employers of people with acquired brain injury (inclusive of stroke) require more information about the physical and cognitive deficits associated with their brain injury [Citation12]. Participants in the current study proposed that this education could be provided by a vocational rehabilitation service, an approach suggested by other researchers [Citation23,Citation24]. Participants described both positive and negative reactions from employers and co-workers in response to their return to work after stroke. Supportive employers maintained regular contact with participants, encouraged them to take time off as needed and then facilitated their return to work by adapting to flexible work arrangements. Other studies have also highlighted the impact of employer support [Citation25], and its positive impact on motivation to return to work [Citation19], as key factors in successful return to work after stroke [Citation10,Citation26]. Employer support as a feature of the work environment, has the capacity to significantly influence stroke survivors’ return to work experiences, and therefore interventions that address the attitudes, behaviours, and knowledge of employers about stroke survivors is vital for work participation [Citation19].
Our study uncovered a range of negative emotional reactions to returning to work after stroke, particularly feelings of stress, overwhelm and anxiety. Previous research demonstrates a high prevalence of mental health and emotional challenges in younger stroke survivors [Citation27], and this has been found to be a key barrier to successful return to work [Citation12]. Consistent with this early research, participants in the current study also identified a need for more psychological and peer support to address the emotional challenges of returning to work. This unmet need has been identified in previous survey data demonstrating that stroke survivors report high levels of dissatisfaction with mental health support received [Citation27]. Given that psychiatric morbidity has been found to be a strong predictor of not returning to work after stroke [Citation28], future vocational rehabilitation programs may seek to incorporate referral to mental health services. Moreover, the establishment of a dedicated peer-support program or trained peer support colleague could enable psychological support during the return to work process. Early person-centred approaches in stroke rehabilitation that foster hope, build confidence, support engagement in vocational rehabilitation, and set a broad work goal may also lessen negative emotional reactions more than a direct focus on return to work outcomes [Citation29].
The vocational rehabilitation intervention [Citation14] explored in this qualitative research was personalised and based on assessment of individual support needs and work circumstances. Overall, participants valued having access to such a personalised therapy to suit their needs, as this provided a holistic approach to support their own unique work goals. A key finding was the importance of communication with the employer. Participants received employee liaison support found this to be very beneficial. This intermediary role worked to support individual needs while also reducing workplace environmental barriers to work participation [Citation19]. An employee liaison service can facilitate return to work by engaging both the employer and employee to maintain a connection (even when the employee is not at work) and to negotiate flexible work roles that motivate and increase stroke survivors’ confidence to work [Citation29]. It may be that support with employer communication should be a standardised element of vocational rehabilitation with the addition of personalised modifications depending on individual client needs and preferences, such as psychological/peer support.
Strengths and limitations
In this study we used semi-structured interviews to gain a deep understanding of the early phases experiences of returning to work for stroke survivors. Exploring patient experiences via interview provided valuable insights into this novel approach to vocational rehabilitation. This study contributes important findings about the benefits and areas of improvement for early vocational rehabilitation by increasing our understanding of what works well or not so well and in what context. We applied purposive sampling to ensure the perspectives of people with post-stroke aphasia were represented in the study (6 of the 16 participants). People with aphasia are frequently underrepresented in interview studies [Citation30] and their experiences may be distinct from other stroke survivors, particularly in work settings. However, people of non-English speaking background were not included in interviews, and therefore our findings do not represent the specific needs and views of people from diverse linguistic backgrounds.
Implications for practice and future research
Our results provide evidence to inform the development of future vocational rehabilitation programs aimed at improving work participation for people living with stroke. Several of the specialist vocational rehabilitation intervention components were found to be beneficial for participants such as employer liaison support, fatigue management, and support for cognition and executive processing including planning and structuring the work schedule. These could be incorporated as key elements of vocational rehabilitation, along with the addition of tailored supports such as employer education and training, as well as improved mental health support. Future research could include the perspectives of other stakeholders in the return to work process such as rehabilitation clinicians and employers, and also evaluate the acceptability and efficacy of vocational rehabilitation interventions.
Conclusion
This study provides insight into participants’ experience of early vocational rehabilitation and identify aspects perceived to be helpful such as workplace communication support as well as fatigue, memory and high-level cognitive rehabilitation. Participants who received specialist vocational rehabilitation perceived strengths in their program and satisfaction with their return to work and rehabilitation processes. But, consistent across our sample, inclusive of those who received this specialist vocational rehabilitation, was the identification of unmet needs, including education and training needs of employers and workplaces. In addition, we identified a need for improved access to mental health support to address the emotional challenges of returning to work in this population. Findings provide direction for the development of future stroke-specific vocational rehabilitation programs.
Acknowledgments
We acknowledge the Brain Recovery and Rehabilitation Stakeholder Advisory Group who improved the quality of research and ensured its conduct was more responsive to, and reflective of, the needs and experiences of working age Australians with stroke. We would also like to express our appreciation to the participants and to thank the investigators and participating trial sites.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Begg SJ, Vos T, Barker B, et al. Burden of disease and injury in Australia in the new millennium: measuring health loss from diseases, injuries and risk factors. Med J Aust. 2008;188(1):36–40. doi: 10.5694/j.1326-5377.2008.tb01503.x.
- Feigin VL, Brainin M, Norrving B, et al. World stroke organization (WSO): global stroke fact sheet 2022. Int J Stroke. 2022;17(1):18–29. doi: 10.1177/17474930211065917.
- Boot E, Ekker MS, Putaala J, et al. Ischaemic stroke in young adults: a global perspective. J Neurol Neurosurg Psychiatry. 2020;91(4):411–417. doi: 10.1136/jnnp-2019-322424.
- Deloitte Access Economics. The economic impact of stroke in Australia. 2020.
- Walters R, Collier JM, Braighi Carvalho L, et al. Exploring post acute rehabilitation service use and outcomes for working age stroke survivors (</=65 years) in Australia, UK and South East asia: data from the international AVERT trial. BMJ Open. 2020;10(6):e035850. doi: 10.1136/bmjopen-2019-035850.
- Stroke Foundation. The needs of stroke survivors in Australia 2013 2022]. Available at https://strokefoundation.org.au/media/vunlgmmz/nsf700_stroke-survivor-needs-2013_web3.pdf.
- Vlachos G, Ihle-Hansen H, Bruun Wyller T, et al. Cognitive and emotional symptoms in patients with first-ever mild stroke: the syndrome of hidden impairments. J Rehabil Med. 2021;53(1):jrm00135. doi: 10.2340/16501977-2764.
- O’Keefe S, Stanley M, Adam K, et al. A systematic scoping review of work interventions for hospitalised adults with an acquired neurological impairment. J Occup Rehabil. 2019;29(3):569–584. doi: 10.1007/s10926-018-9820-8.
- Edwards JD, Kapoor A, Linkewich E, et al. Return to work after young stroke: a systematic review. Int J Stroke. 2018;13(3):243–256. doi: 10.1177/1747493017743059.
- Schwarz B, Claros-Salinas D, Streibelt M. Meta-Synthesis of qualitative research on facilitators and barriers of return to work after stroke. J Occup Rehabil. 2018;28(1):28–44. doi: 10.1007/s10926-017-9713-2.
- Wolfenden B, Grace M. Identity continuity in the face of biographical disruption: ‘it’s the same Me’. Brain Impairment. 2012;13(2):203–211. doi: 10.1017/BrImp.2012.16.
- Brakenridge CL, Leow CKL, Kendall M, et al. Exploring the lived return-to-work experience of individuals with acquired brain injury: use of vocational services and environmental, personal and injury-related influences. Disabil Rehabil. 2022;44(16):4332–4342. doi: 10.1080/09638288.2021.1903101.
- Lindgren I, Brogårdh C, Pessah-Rasmussen H, et al. Work conditions, support, and changing personal priorities are perceived important for return to work and for stay at work after stroke – a qualitative study. Disabil Rehabil. 2022;44(11):2500–2506. doi: 10.1080/09638288.2020.1836522.
- O’Keefe S, Radford K, Farrin A, et al. A tailored occupational therapist-led vocational intervention for people with stroke: protocol for a pilot randomized controlled trial. JMIR Res Protoc. 2022;11(10):e40548. doi: 10.2196/40548.
- Saunders B, Sim J, Kingstone T, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quan. 2018;52(4):1893–1907.
- Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In: Bryman A, Burgess R, editors. Analyzing qualitative data. London: Routledge; 1994. p. 173–194.
- Gale NK, Heath G, Cameron E, et al. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13:117. doi: 10.1186/1471-2288-13-117.
- Condon JR, Garvey G, Whop LJ, et al. Aboriginal and Torres Strait Islander Australians and cancer. Cancer Forum. 2013;37(1):27–30.
- La Torre G, Lia L, Francavilla F, et al. Factors that facilitate and hinder the return to work after stroke: an overview of systematic reviews. Med Lav. 2022;113(3):e2022029.
- Medin J, Barajas J, Ekberg K. Stroke patients’ experiences of return to work. Disabil Rehabil. 2006;28(17):1051–1060. doi: 10.1080/09638280500494819.
- Lock S, Jordan * L, Bryan K, et al. Work after stroke: focusing on barriers and enablers. Disab Soc. 2005;20(1):33–47. doi: 10.1080/0968759042000283629.
- Manning M, MacFarlane A, Hickey A, et al. I hated being ghosted’ - The relevance of social participation for living well with post-stroke aphasia: qualitative interviews with working aged adults. Health Expect. 2021;24(4):1504–1515. doi: 10.1111/hex.13291.
- Hellman T, Bergstrom A, Eriksson G, et al. Return to work after stroke: important aspects shared and contrasted by five stakeholder groups. Work. 2016;55(4):901–911. doi: 10.3233/WOR-162455.
- Ost Nilsson A, Eriksson G, Johansson U, et al. Experiences of the return to work process after stroke while participating in a person-centred rehabilitation programme. Scand J Occup Ther. 2017;24(5):349–356. doi: 10.1080/11038128.2016.1249404.
- Hartke RJ, Trierweiler R. Survey of survivors’ perspective on return to work after stroke. Top Stroke Rehabil. 2015;22(5):326–334. doi: 10.1179/1074935714Z.0000000044.
- Libeson L, Downing M, Ross P, et al. The experience of return to work in individuals with traumatic brain injury (TBI): a qualitative study. Neuropsychol Rehabil. 2020;30(3):412–429. doi: 10.1080/09602011.2018.1470987.
- Walsh ME, Galvin R, Loughnane C, et al. Community re-integration and long-term need in the first five years after stroke: results from a national survey. Disabil Rehabil. 2015;37(20):1834–1838. doi: 10.3109/09638288.2014.981302.
- Glozier N, Hackett ML, Parag V, et al. The influence of psychiatric morbidity on return to paid work after stroke in younger adults: the Auckland regional community stroke (ARCOS) study, 2002 to 2003. Stroke. 2008;39(5):1526–1532. doi: 10.1161/STROKEAHA.107.503219.
- Dunn JA, Hackney JJ, Martin RA, et al. Development of a programme theory for early intervention vocational rehabilitation: a realist literature review. J Occup Rehabil. 2021;31(4):730–743. doi: 10.1007/s10926-021-10000-z.
- Lloyd V, Gatherer A, Kalsy S. Conducting qualitative interview research with people with expressive language difficulties. Qual Health Res. 2006;16(10):1386–1404. doi: 10.1177/1049732306293846.
- Maxwell JA. Understanding and validity in qualitative research. Harvard Educ. Rev. 1992;62(3):279–301. doi: 10.17763/haer.62.3.8323320856251826.
- Creswell JW, Miller DL. Determining validity in qualitative inquiry. Theory Pract. 2000;39(3):124–130. doi: 10.1207/s15430421tip3903_2.
- Morse JM. Critical analysis of strategies for determining rigor in qualitative inquiry. Qual Health Res. 2015;25(9):1212–1222. doi: 10.1177/1049732315588501.