
Abstract
Purpose
To investigate: (1) changes in body satisfaction during five months of handcycle training and one year after the training period; (2) whether longitudinal changes are dependent on sex, waist circumference and severity of the physical impairment; (3) associations between changes in physical capacity or body composition, and body satisfaction.
Materials and methods
Individuals (N = 143) with health conditions such as spinal cord injury filled out the Adult Body Satisfaction Questionnaire: at the start of the training (T1), directly after the training period (T2); and four months (T3) and one year after the training period (T4). At T1 and T2, physical capacity was determined with an upper-body graded exercise test, and waist circumference was measured. Handcycling classification was used as a proxy for the severity of impairment.
Results
Multilevel regression analyses showed that body satisfaction significantly increased during the training period and significantly decreased back to pre-training levels at follow-up. Individuals with more severe impairments showed a larger decrease at T4. Improvements in physical capacity and waist circumference were significantly associated with improvements in body satisfaction.
Conclusions
Body satisfaction significantly increased during the training period, but significantly decreased during follow-up. Additional efforts might be necessary to keep individuals engaged in long-term exercise.
Implications for Rehabilitation
Body image disturbances are frequently described in individuals with a physical impairment.
An increase in body image can be achieved by improvements in physical capacity and waist circumference as a consequence of training.
It is important to keep individuals engaged in exercise, as body satisfaction decreases after termination of the training period.
For individuals with severe physical impairments additional efforts are necessary to keep them engaged in exercise.
Introduction
Body image is a complex multidimensional concept that encompasses one’s body-related self-perceptions and self-attitudes, including thoughts, beliefs, feelings, and behaviours [Citation1]. These perceptions and attitudes encompass both body appearance and body functioning and can be experienced positively (e.g., satisfaction) or negatively (e.g., dissatisfaction) [Citation2,Citation3].
In the general population, women are generally less satisfied with their body appearance and function than men [Citation3]. In addition, body composition measures (e.g., body mass, body fat) and physical capacity are, respectively, negatively and positively associated with body satisfaction [Citation3]. In individuals with a physical impairment, body image disturbances are frequently described [Citation2,Citation4,Citation5]. Changes in body function and physical appearance, pain and discomfort, weight gain as well as changes in psychological factors, such as self-efficacy and acceptance, as a consequence of having a physical impairment, have all been shown to be associated with body image disturbances [Citation4,Citation6–10]. Consequently, the severity of the impairment has previously been described to be associated with body image [Citation6,Citation9,Citation11]. Additionally, disturbances in body image can negatively affect the performance of activities of daily living, work, social roles, and quality of life [Citation2,Citation12–14].
Previous studies with individuals with spinal cord injury (SCI) describe the adjustment period (immediately following after the injury) as the most negative time period with respect to body image [Citation6,Citation8,Citation9,Citation14,Citation15]. After this, body image seems to improve with increasing time since injury (TSI) as individuals seem to adjust to their changed body [Citation6,Citation8,Citation14–16]. In addition, minimizing musculoskeletal pain (e.g., correcting abnormal posture or exercise), may contribute to a positive body image [Citation8]. Cross-sectional SCI studies by Bassett et al. showed that women (TSI: 15 ± 13 years) have lower scores on body appearance and function than men (TSI: 15 ± 10 years) [Citation14,Citation15]. In women with SCI, a higher appearance satisfaction was associated with a smaller waist circumference and lower percentage of body fat [Citation15]. Although these cross-sectional differences between men and women with SCI are apparent, it is unknown whether men and women with SCI show similar changes in body image as a response to exercise. A study with able-bodied participants showed that men and women show similar improvements in body image during a strength-training program [Citation17].
Several studies highlighted the positive effects of exercise or physical activity on body image in the general population and in individuals with a physical impairment [Citation3,Citation8,Citation11,Citation15,Citation17–22]. Suggested mechanisms are objective and subjective improvements in muscle strength and body composition as a result of exercise, causing people to feel better about themselves as they are approaching their body ideal [Citation17]. Bailey et al. described engaging in exercise as part of adaptive self-care behaviour in individuals with SCI; a concept which in itself is associated with positive body image [Citation8]. Moreover, in individuals with SCI, exercise interventions have shown to cause an increase in body satisfaction, alongside quality of life and functional independence [Citation11,Citation18,Citation20]. Unfortunately, it is unknown whether these improvements in body satisfaction are preserved after the exercise intervention [Citation23].
The objectives of the current prospective cohort study were to examine: (1) changes in body satisfaction during five months of handcycle training, at four months after the training period and at one year after the training period, (2) whether these longitudinal changes are dependent on sex, waist circumference and severity of the impairment, and (3) associations between changes in physical capacity or body composition, and body satisfaction during the handcycle training period. It was hypothesized that (1) body satisfaction increases during the training period and remains stable during follow-up; (2) men and women show similar trajectories of body satisfaction, but that individuals with an unhealthy waist circumference or more severe impairment show greater improvements in body satisfaction during the training period; (3) the increase in body satisfaction during the training period is associated with improvements in physical capacity and body composition.
Materials and methods
The HandbikeBattle project
The HandbikeBattle event is an annual uphill hand-cycling race (20.2-km length and 863-m elevation gain) in the mountains of Austria among teams of twelve Dutch rehabilitation centers [Citation24]. The event was created to stimulate an active lifestyle by means of hand-cycling with peers and to push the participant’s physical and mental boundaries. Each team consists of former rehabilitation patients with a chronic disability such as an SCI, leg amputation, or cerebral palsy. At the start of the five-month training period, most participants are relatively untrained hand cyclists. Guidance during the training period was provided by therapists from the respective rehabilitation centers, for example, with a group training session each month. The training period was free-living, that is, no specific training program was provided by the researchers. Connected to, but not part of, the HandbikeBattle is an observational cohort study that was initiated to monitor the effects of participation in the training period and the event.
Participants
Inclusion criteria for the HandbikeBattle event were (1) being a former rehabilitation patient from one of the twelve rehabilitation centers, (2) impairment of the lower extremities, and (3) commitment to the HandbikeBattle challenge. The exclusion criterion included any contraindication to participate as diagnosed during the medical screening before the training period. An additional inclusion criterion for the HandbikeBattle study was sufficient knowledge of the Dutch language to understand the instructions. In the present study, data were used from participants of the HandbikeBattle 2017–2019 cohorts.
Procedure
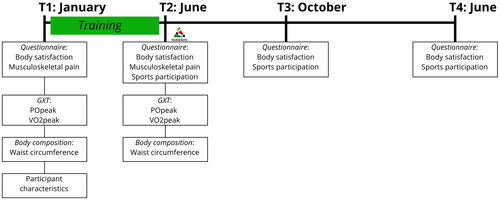
Measurements were performed at the start of the training period (January, T1); after the training period, prior to the event (June, T2); and at follow-up, four months (October, T3) and one year (June, T4) after the event (). Measurements included questionnaires at all time points and physical measurements at T1 and T2. Participants were invited by e-mail with a link and could fill out the questionnaires online. Participants of the 2019 cohort were not asked to fill out the questionnaire at T4 (June 2020) due to Covid-19, as the pandemic might have had an effect on health, physical activity and other related factors. At T1, a medical screening was performed by a rehabilitation physician at the rehabilitation center. The screening comprised a medical anamnesis, physical examination, and a handcycling or arm crank-graded exercise test (GXT). During the screening it was assessed whether it was safe for individuals to start training and to participate in the HandbikeBattle event. The screening was, therefore, a prerequisite at the start of the training period. At T2, the GXT was repeated with the same protocol and equipment. All participants voluntarily signed an informed consent form. The study was approved by the local ethics committee of the Center for Human Movement Sciences, University Medical Center Groningen, the Netherlands (ECB/2012_12.04_I_rev/Ml).
Figure 1. Study design. Measurements are performed at the start of the training period (January, T1); after the training period, prior to the event (June, T2); and follow-up, four months after the event (October, T3) and one year after the event (June, T4). abbreviations: GXT = graded exercise test, POpeak = peak power output, VO2peak = peak oxygen uptake.
Outcome measures
General information
General participant information was collected at T1 and included age (y), sex, and impairment type. The hours of sports participation per week were reported by the participant at T2, T3, and T4.
Body satisfaction
The 9-item Adult Body Satisfaction Questionnaire[Citation3] was used to measure satisfaction with their body function and body appearance. In concordance with previous studies that measured body satisfaction in a wheelchair-using population, a 10th item was added to measure satisfaction with arm muscle strength [Citation11,Citation14,Citation15,Citation18,Citation20]. Each item is rated on a 7-point scale ranging from −3 (very dissatisfied) to +3 (very satisfied). The questionnaire has two subscales: functional satisfaction (average of seven items, e.g., level of endurance) and appearance satisfaction (average of three items, e.g., weight). This measure has shown adequate internal consistency for both subscales (α > 0.70) [Citation3,Citation14,Citation18].
Determinants
Upper body physical capacity was measured during a GXT to volitional exhaustion at T1 and T2. Details on equipment and testing protocols have been described in a previous study [Citation25]. Either a 1-min stepwise protocol or continuous ramp protocol was used, and was individualized for each participant. The set-up and protocol choice were dependent on the available equipment in the rehabilitation centers, but were consistent within participants over time. Power output (PO, in Watts (W)) and gas exchange were measured during the test. For the 1-min stepwise protocol, peak PO (POpeak) was defined as the highest PO that was maintained for at least 30 s. For the ramp protocol, the highest PO achieved during the test was considered POpeak. Peak oxygen uptake (VO2peak, l/min) was defined as the highest 30-s average for oxygen consumption.
At T1 and T2 waist circumference (cm) was measured with measuring tape at the level of the umbilicus and with participants in supine position. The average of three measurements was used for analysis. To study interaction effects (objective 2), waist circumference was dichotomized (healthy (men ≤102 cm, women ≤88 cm) and unhealthy (men >102 cm, women >88 cm)) [Citation26].
Confounding variables
Possible confounding variables included in the analyses were age, sex, musculoskeletal pain, and handcycling classification.
Musculoskeletal pain comprised seven locations: left and right hand and wrist, left and right elbow, left and right shoulder, and the neck. Pain was graded with a range from 1 (no pain) to 6 (very severe pain). Having moderate-severe pain was defined as ≥4 (moderate pain) at ≥1 locations. Two groups were created: (1) no-mild pain, (2) moderate-severe pain.
Handcycling classification was used as a proxy for severity of impairment and determined by a certified para-cycling classifier. The classification resulted in five different classes, ranging from H1 (most impaired) to H5 (least impaired) [Citation27]. H1 and H2 handcyclists have limitations in arm-hand function, trunk, and lower limbs; whereas H3 handcyclists have intact arm-hand function and limitations in the trunk and lower limbs. H4 and H5 handcyclists have limitations in lower limbs only. Handcyclists with (potentially) impaired heart rate response to exercise are represented in class H1–H3. For the analyses in the present study, participants were divided into two groups of equal size: (1) H1–H3 and (2) H4–H5.
Statistical analysis
The analyses were performed with SPSS (Version 27.0; IBM Corp, Armonk, NY) and MLwiN version 2.36 [Citation28]. Descriptive statistics were calculated for outcome measures and determinants. Data were tested for normality with the Kolmogorov-Smirnov test with Lilliefors significance correction, combined with z scores for skewness and kurtosis. To ascertain possible response bias, characteristics of included participants in the present study were compared with non-participants (i.e., drop-outs or those who did not fill out all questionnaires) using t tests, Mann-Whitney U tests, and chi-square tests.
Multilevel models with three levels were created; with observations within participants as first level, participant as second level, and rehabilitation center as the third level. Multilevel analyses were conducted to be able to make adjustments for the dependency of the observations within participants and participants within centers. An additional advantage of multilevel analyses is the robustness of missing data [Citation29].
Two models were created to examine the longitudinal trajectory of body satisfaction (hypothesis 1): one with functional satisfaction and one with appearance satisfaction as dependent variable. Time (T1, T2, T3, T4) was included as a categorical variable with three dummies and T2 as reference category.
To test hypothesis 2, interaction terms with the time dummies were investigated in a series of separate models for each of the following determinants: sex (reference: male), waist circumference (reference: healthy), and handcycling classification (reference: H1-H3).
To test hypothesis 3, four models were created to examine longitudinal associations between functional satisfaction and appearance satisfaction, and changes in two determinants (POpeak, waist circumference). POpeak was chosen to represent physical capacity, as it had the least missing data and there was a high correlation (r = 0.84) between POpeak and VO2peak. These models were created as hybrid models for the training period (T1, T2) to be able to distinguish between the between-subject (cross-sectional) component and the within-subject (longitudinal) component of the association [Citation30]. Possible confounders, age, sex (reference: male), musculoskeletal pain (reference: no-mild pain), and handcycling classification (reference: H1-H3) were added separately to each model first. A confounder was included in the final model if its inclusion changed the regression coefficient(s) with more than 10% [Citation31].
Results
In total, 205 individuals started training. Twenty-five individuals dropped out due to medical reasons (N = 14), motivational problems (N = 4), being too busy with work/family (N = 4) or personal/unknown reasons (N = 3). Thirty-seven individuals did not fill out questionnaires at any time-point (N = 22), or only at one time-point (N = 15). Hence, data from 143 participants were included in the present study, whereas 62 individuals were defined as non-participants. Participants were on average older and had more often an acquired impairment such as SCI or leg amputation, in contrast to non-participants, who had more often spina bifida or cerebral palsy (). Descriptive data of the outcome measures, determinants over time, and potential confounders are depicted in .
Table 1. Characteristics and outcomes at T1 for participants and non-participants.
Table 2. Descriptive data and outcome measures of participants at all time points.
Longitudinal trajectory of functional satisfaction and appearance satisfaction
Functional and appearance satisfaction showed a significant increase between T1 (start of training) and T2 (after training), whereas a significant decrease was found for both outcome measures during follow-up (). When the models were recalculated with T1 as reference category, there were no significant changes between T1 and T3 and between T1 and T4 (functional satisfaction T1-T3 regression coefficient: 0.160, SE: 0.111, p = 0.15; T1-T4 regression coefficient: 0.100, SE: 0.135, p = 0.46; appearance satisfaction T1-T3 regression coefficient: 0.064, SE: 0.132, p = 0.63; T1-T4 regression coefficient: −0.258, SE: 0.162, p = 0.11).
Table 3. Longitudinal trajectory of body satisfaction (N = 143).
Longitudinal trajectory based on sex, waist circumference and impairment severity
Participants with a more severe impairment showed a significant decrease in functional and appearance satisfaction during follow-up compared to participants with a less severe impairment (, ). Sex and waist circumference showed no interaction effects.
Figure 2. Longitudinal trajectory of functional satisfaction (A) and appearance satisfaction (B) for different Subgroups. A1, B1 = sex: M/F. A2, B2 = waist circumference at T1: healthy (men ≤ 102 cm, women ≤ 88 cm) and unhealthy (men > 102 cm, women > 88 cm). A3, B3 = handcycling classification as a proxy for severity of the impairment: H1-H3 (most impaired)/H4-H5 (least impaired). T1 = start of the training period. T2 = after the training period, prior to the HandbikeBattle event. T3 = follow-up measurement, four months after the event. T4 = follow-up measurement, one year after the event.
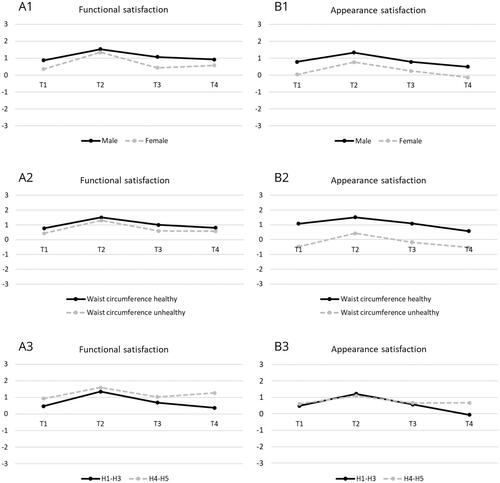
Table 4. Longitudinal trajectory of body satisfaction of groups with different sex, waist circumference or handcycling classification and interaction effects (time * group).
Longitudinal associations between physical capacity or body composition and body satisfaction
POpeak showed significant positive longitudinal associations with functional and appearance satisfaction. Waist circumference showed significant negative longitudinal associations with both outcome measures of body satisfaction ().
Table 5. Longitudinal and cross-sectional associations between physical capacity or body composition and body satisfaction during the training period (T1–T2).
Discussion
The present study showed that both functional and appearance satisfaction significantly increased during five months of handcycle training, but significantly decreased to pre-training levels during follow-up. Furthermore, it was shown that participants with more severe impairments showed a decrease in functional and appearance satisfaction during follow-up compared to participants with less severe impairments. The improvements in body satisfaction were longitudinally associated with improvements in POpeak and waist circumference.
In the present study, the baseline value of functional satisfaction (0.69) was higher compared to the values between −1 and 0 reported by several previous SCI studies [Citation11,Citation20]. This might be due to longer TSI and less severe impairment (e.g., fewer individuals with a tetraplegia) in the present study. Previous studies among participants with a longer TSI (i.e., 15 years) showed similar values for functional satisfaction (0.65 − 0.97) [Citation14,Citation15]. Similarly, appearance satisfaction ranged between −1 and +1 in previous studies [Citation11,Citation14,Citation15,Citation20,Citation22], which is comparable to or slightly lower than the baseline value in the present study (0.57).
During the training period body satisfaction significantly increased, which is in accordance with previous SCI studies [Citation11,Citation18,Citation20]. An increase in POpeak, as well as a decrease in waist circumference, were longitudinally associated with an increase in both functional and appearance satisfaction. In addition to the objective physical effects of exercise (e.g., gaining strength, losing weight), it is hypothesized that engaging in exercise and physically pushing oneself might change people’s perceptions of their physical characteristics [Citation8,Citation17,Citation32]. These subjective effects of exercise are shown to be associated with positive body image [Citation8,Citation17,Citation23,Citation32]. In addition, the increase in body satisfaction might partly be explained by the increase in social support by peers during the training period [Citation8,Citation23]. Being part of a homogenous group has been shown to be associated with body acceptance, appreciation, and gratitude in individuals with SCI [Citation8].
During follow-up, body satisfaction decreased to levels comparable with baseline. This was in contrast to our hypothesis that body satisfaction would remain stable during follow-up. Unfortunately, it is unknown whether this decrease is associated with corresponding changes in POpeak and waist circumference. To our knowledge, this is the only study with follow-up measurements of body satisfaction after a training period. Possible explanations for the decline in body satisfaction could be a decrease in exercise during the follow-up period, and consequently, a decrease in physical capacity and functional independence, an increase in body mass and waist circumference, a decrease in endorphins and less peer support. Based on the descriptive hours of sports participation () a decrease in exercise might indeed play a role. However, based on previous findings, it is expected that at least part of the group remains physically active with a stable physical capacity level during follow-up [Citation33]. In addition, it is unknown whether participants were adhering to a healthy diet during the training period and whether they kept adhering to this diet during follow-up. Another aspect that might play a role is body nostalgia. Especially after one year of follow-up participants might have nostalgic thoughts about their function and appearance at T2, glorifying their body at the end of the training period [Citation7].
Previous studies demonstrated that men with SCI showed higher appearance satisfaction than women with SCI [Citation14,Citation15]. The present study additionally demonstrates that both men and women showed an increase in functional and appearance satisfaction during the training period and showed a similar decline during follow-up (). Previous qualitative research showed that men were mostly satisfied with the increased upper-body muscle mass, as a means to express their masculinity in a socially normative way, whereas women were not satisfied with the appearance of increased upper-body muscle mass but focused on the positive effects of improved upper-body strength on functional independence [Citation7,Citation20].
In addition, in contrast to our hypothesis, waist circumference, and impairment severity did not show interaction effects with body satisfaction during the training period. However, individuals with a more severe impairment showed a clear decline in body satisfaction at one year of follow-up in contrast to individuals with a less severe impairment. Therefore, it is, especially for this group, important to keep them engaged in (group) physical activity and exercise.
Implications
The results of the present study provide important leads to improve body satisfaction in individuals with a physical impairment, especially for individuals who are dissatisfied with their bodies. However, body satisfaction immediately decreased during the first three months of follow-up. Therefore, additional efforts might be necessary to keep individuals engaged in physical activity and exercise, such as social support and new tangible training goals.
Study limitations
Unfortunately, physical capacity and body composition were not measured during follow-up. Therefore, it was not possible to study longitudinal associations with body satisfaction during follow-up. In addition, musculoskeletal pain was the only secondary health condition that was registered, while other secondary health conditions might also influence body satisfaction and physical capacity. Lastly, it is unknown whether the (subjective) experience of participants during the HandbikeBattle event was better than expected or disappointing and whether this feeling has consequences for their body satisfaction during follow-up.
Conclusions
Body satisfaction significantly increased during five months of handcycle training, but significantly decreased to pre-training levels during follow-up. The improvements in body satisfaction during the training period were longitudinally associated with improvements in POpeak and waist circumference. Furthermore, participants with more severe impairments showed a significant decrease in functional and appearance satisfaction during follow-up compared to participants with less severe impairments. Additional efforts might be necessary to keep individuals engaged in physical activity and exercise, such as social support and new tangible training goals.
Acknowledgments
We thank Kathleen Martin Ginis, PhD, School of Health and Exercise Sciences, University of British Columbia, Kelowna, BC, Canada, for her support with the Body Satisfaction Questionnaire.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data that support the findings of this study are available from the corresponding author, IK, upon reasonable request.
Additional information
Funding
References
- Cash TF. Body image: past, present, and future. Body Image. 2004;1(1):1–5. doi: 10.1016/S1740-1445(03)00011-1.
- Cash TF, Smolak L. Chapter 1: understanding body images. In: Thomas FC and Linda S, editors. Body image: a handbook of science, practice, and prevention. second edition. New York (NY) :The Guilford Press; 2011:3–11.
- Reboussin BA, Rejeski WJ, Martin KA, et al. Correlates of satisfaction with body function and body appearance in Middle- and older aged adults: the activity counseling trial (ACT). Psychol Health. 2000;15(2):239–254. doi: 10.1080/08870440008400304.
- Pfaffenberger N, Gutweniger S, Kopp M, et al. Impaired body image in patients with multiple sclerosis. Acta Neurol Scand. 2011;124(3):165–170. doi: 10.1111/j.1600-0404.2010.01460.x.
- Pruzinsky T. Enhancing quality of life in medical populations: a vision for body image assessment and rehabilitation as standards of care. Body Image. 2004;1(1):71–81. doi: 10.1016/S1740-1445(03)00010-X.
- Taleporos G, McCabe MP. Body image and physical disability - personal perspectives. Soc Sci Med. 2002;54(6):971–980. doi: 10.1016/s0277-9536(01)00069-7.
- Bailey KA, Gammage KL, van Ingen C, et al. Managing the stigma: exploring body image experiences and self-presentation among people with spinal cord injury. Health Psychol Open. 2016;3(1):1–10.
- Bailey KA, Gammage KL, van Ingen C, et al. “It’s all about acceptance”: A qualitative study exploring a model of positive body image for people with spinal cord injury. Body Image. 2015;15:24–34. doi: 10.1016/j.bodyim.2015.04.010.
- Van Diemen T, van Leeuwen C, van Nes I, et al. Body image in patients with spinal cord injury during inpatient rehabilitation. Arch Phys Med Rehabil. 2017;98(6):1126–1131. doi: 10.1016/j.apmr.2016.10.015.
- Latimer AE, Martin Ginis KA, Hicks AL, et al. An examination of the mechanisms of exercise-induced change in psychological well-being among people with spinal cord injury. J Rehabil Res Dev. 2004;41(5):643–652. doi: 10.1682/jrrd.2003.04.0043.
- Astorino TA, Harness ET. Improved quality of life and body satisfaction in response to activity-based therapy in adults with spinal cord injury. Neuroimmunol Neuroinflamm. 2020;7:40–50.
- Drench ME. Changes in body image secondary to disease and injury. Rehabil Nurs. 1994;19(1):31–36. doi: 10.1002/j.2048-7940.1994.tb01300.x.
- Duarte Torres DM, Torres Bolaños YM, Moreno Fergusson ME. Body and corporality in adolescents and young adults with spinal cord injury. Invest Educ Enferm. 2016;34(1):84–93. doi: 10.17533/udea.iee.v34n1a10.
- Bassett RL, Martin Ginis KA, The SHAPE-SCI Research Group. More than looking good: impact on quality of life moderates the relationship between functional body image and physical activity in men with SCI. Spinal Cord. 2009;47(3):252–256. doi: 10.1038/sc.2008.114.
- Bassett RL, Martin Ginis KA, Buchholz AC. A pilot study examining correlates of body image among women living with SCI. Spinal Cord. 2009;47(6):496–498. doi: 10.1038/sc.2008.174.
- Dibb B, Ellis-Hill C, Donovan-Hall M, et al. Exploring positive adjustment in people with spinal cord injury. J Health Psychol. 2014;19(8):1043–1054. doi: 10.1177/1359105313483158.
- Martin Ginis KA, Eng JJ, Arbour KP, et al. Mind over muscle? Sex differences in the relationship between body image change and subjective and objective physical changes following a 12-week strength-training program. Body Image. 2005;2(4):363–372. doi: 10.1016/j.bodyim.2005.08.003.
- Hicks AL, Martin KA, Ditor DS, et al. Long-term exercise training in persons with spinal cord injury: effects on strength, arm ergometry performance and psychological well-being. Spinal Cord. 2003;41(1):34–43. doi: 10.1038/sj.sc.3101389.
- Yuen HK, Hanson C. Body image and exercise in people with and without acquired mobility disability. Disabil Rehabil. 2002;24(6):289–296. doi: 10.1080/09638280110086477.
- Semerjian TZ, Montague SM, Dominguez JF, et al. Enhancement of quality of life and body satisfaction through the use of adapted exercise devices for individuals with spinal cord injuries. Top Spinal Cord Inj Rehabil. 2005;11(2):95–108. doi: 10.1310/BXE2-MTKU-YL15-429A.
- Stensman R. Body image among 22 persons with acquired and congenital severe mobility impairment. Paraplegia. 1989;27(1):27–35.
- Hoevenaars D, Holla JFM, de Groot S, et al. Lifestyle and health changes in wheelchair users with a chronic disability after 12 weeks of using the WHEELS mHealth application. Disabil Rehabil Assist Technol. 2022:1–10. doi: 10.1080/17483107.2022.2115563.
- Hausenblas HA, Fallon EA. Exercise and body image: a meta-analysis. Psychol Health. 2006;21(1):33–47. doi: 10.1080/14768320500105270.
- De Groot S, Postma K, van Vliet L, et al. Mountain time trial in handcycling: exercise intensity and predictors of race time in people with spinal cord injury. Spinal Cord. 2014;52(6):455–461. doi: 10.1038/sc.2014.58.
- Kouwijzer I, Valent L, Osterthun R, et al. Peak power output in handcycling of individuals with a chronic spinal cord injury: predictive modeling, validation and reference values. Disabil Rehabil. 2020;42(3):400–409. doi: 10.1080/09638288.2018.1501097.
- Grundy SM, Brewer HB, Cleeman JI, et al. Definition of metabolic syndrome: report of the national heart, lung, and blood institute/American heart association conference on scientific issues related to definition. Circulation. 2004;109(3):433–438. doi: 10.1161/01.CIR.0000111245.75752.C6.
- UCI Regulations Part XVI: Para-cycling. Assessed 25-11-2021. https://www.uci.org/regulations/3MyLDDrwJCJJ0BGGOFzOat#part-xvi-para-cycling.
- Rasbash J, Charlton C, Browne WJ, et al. MLwiN Version 2.36. Centre for Multilevel Modelling, University of Bristol, 2009.
- Maas CJM, Snijders TAB. The multilevel approach to repeated measures for complete and incomplete data. Qual Quant. 2003;37(1):71–89. doi: 10.1023/A:1022545930672.
- Twisk JWR, de Vente W. Hybrid models were found to be very elegant to disentangle longitudinal within- and between-subject relationships. J Clin Epidemiol. 2019;107:66–70. doi: 10.1016/j.jclinepi.2018.11.021.
- Twisk JWR. Applied longitudinal data analysis for epidemiology. a practical guide. 4th edition. Cambridge (UK): Cambridge University Press; 2003.
- Martin Ginis KA, Strong HA, Arent SM, et al. The effects of aerobic- versus strength-training on body image among young women with pre-existing body image concerns. Body Image. 2014;11(3):219–227. doi: 10.1016/j.bodyim.2014.02.004.
- Kouwijzer I, Valent LJM, Post MWM, et al. The course of physical capacity in wheelchair users during training for the HandbikeBattle and at 1-Yr follow-up. Am J Phys Med Rehabil. 2021;100(9):858–865. doi: 10.1097/PHM.0000000000001658.