
Abstract
Purpose
To explore the lived experience of physical exertion for persons living with advanced multiple sclerosis (MS)
Method
An interpretive (hermeneutic) phenomenological approach was undertaken with 8 persons living with advanced MS. Interviews were conducted with exploratory questions that explored participants’ experiences of physical exertion. Data was analysed using phenomenological methods and the findings presented as hermeneutic stories.
Results
Participants conveyed physical exertion as a means of influencing their connection with the world. Interpretation identified four subthemes; Lived Body, Sense of Self, Purpose of exertion, and Attributes of the World and an overarching superordinate theme Body-World engagement. Hermeneutic stories illuminated the intertwined relationship between the themes and the idiographic nature of physical exertion.
Conclusion
The experience of physical exertion was meaningfully related to participants’ sense of self, agency, and ‘being in the world’.
IMPLICATIONS FOR REHABILITATION
For persons living with advanced MS:
Physical exertion has the potential to enhance sense of self through regaining a lost, or creating a new identity.
Physical exertion can enhance bodily consciousness and cause individuals to dwell on inability, consequently health care professionals should consider how their language and therapy focus may intensify this.
Attempting to meet societally accepted standards of normal had a shaping influence on the exertional experience.
The meaning of physical exertion is influenced by an individual’s preconceptions and healthcare professionals should take time to understanding these, in order to optimise engagement in physical exertion.
Introduction
Multiple sclerosis (MS) is one of the most common neurological conditions affecting adults in the United Kingdom, with over 130,000 persons living with the condition [Citation1]. It is a progressive, autoimmune condition which causes inflammation within the central nervous system (CNS), resulting in damage to nerve conduction pathways. Symptoms of MS are dependent on lesion location within the CNS, lesion load, and brain atrophy; all of which contribute to neuro degeneration [Citation2,Citation3]. Disease course can be unpredictable, making persons’ lived experience unique, but common impairments experienced include motor and sensory dysfunction, fatigue, pain, cognitive impairment, bladder and bowel difficulties, and sexual dysfunction [Citation4–6]. Earlier diagnosis and prescription of disease-modifying medication has led to improvements in survival rates for persons living with MS (plwMS), but disease progression and longer life expectancy is frequently accompanied by more complex disability. Dependence on assistive equipment or support of others can alter persons’ ability to engage in valued activities and alter attitude towards self, whilst variable and fluctuating symptoms exposes a need for plwMS to constantly adapt to new ways of being [Citation7].
Exercise and physical activity (PA) have been identified as effective means of managing the consequences of MS, by maintaining function and optimising quality of life [Citation8]. PlwMS describe a diverse range of tasks as PA and exercise, including structured exercise, social interactions, and activities of daily living [Citation9–11] and thus health care professionals (HCP) have been encouraged to take a broader approach to PA that encapsulates lifestyle and everyday activities [Citation12,Citation13]. Despite the benefits of exercise and PA, plwMS remain less physically active than the general age-matched population, with the highest levels of inactivity found in persons with the greatest disease severity [Citation12,Citation14]. Qualitative research has identified environmental and social barriers relating to access and suitability of exercise programmes [Citation9,Citation15–17] and highlighted conflicting experiences of PA and exercise on wellbeing in plwMS. On the one hand they expressed anxiety that engaging in PA may exacerbating their MS-related symptoms, yet they also identified the role of exercise and PA in enhancing their physical function and strength [Citation15]. Some plwMS expressed frustration at not being able to engage in the activity as desired which contributed to a sense of loss, yet accounts also illuminated the role of exercise as a means of coping with the unpredictability of living with a progressive disease [Citation10,Citation15]. Researchers have sought to understand the impact of PA and exercise on wellbeing by applying a theoretical lens to analysis, and incorporating social and behavioural change frameworks. This has identified the role of society, culture and past experiences and disease severity in shaping exercise perception and impacting individuals’ self-esteem and self-efficacy [Citation11,Citation15].
It has been suggested that the severity of disability influences how plwMS engage in PA and exercise [Citation8], and that perception of exercise can change over the duration of living with MS [Citation14]. Dependency on others, such as care givers or spouses, creates an interpersonal relationship to PA that can assist in overcoming barriers but also be a cause of increase stress and dependency [Citation18,Citation19]. A study exploring PA from the perspective of plwMS with moderate to severe disability, and persons who identified as care givers to plwMS described the breadth of activity that they defined as PA as a “continuum” that encompassed structured to unstructured activity [Citation18, p. 185]. As structured activities became harder to access due to barriers such as a lack of supported programmes or reduced mobility, participants adapted physical activity to fit into their activities of daily living or routine and prioritised social interactions [Citation18]. Whilst these findings cannot be generalised to all persons with higher disability levels, they suggest plwMS have a change in perspective towards exercise and PA as their disease progresses and/or disability worsens, when they become driven by a need to prioritise effort towards meaningful activity [Citation20–22].
It is recognised that plwMS with more severe disability have different PA requirements compared to those with milder disability and further investigation is needed to ensure optimal exercise prescription and health promotion [Citation8,Citation9,Citation14]. “Advanced MS” has been suggested as a term that encapsulates individuals who have multiple symptoms of MS, who are dependent on others for daily needs and have significant functional impairment. It considers the burden of the disease to the individual [Citation23]. The term is most likely to include persons living with progressive MS, but by definition, it could also include persons living with relapsing MS with very active disease who may fully recover from disabling relapses.
Studies involving plwMS with more advanced disability have highlighted participants’ desire to be more active and embrace PA as a self-management strategy and means of enhancing independence [Citation12,Citation18,Citation24]. They also emphasise the need for support to overcome barriers, such as inaccessibility, fear of exacerbating MS symptoms, and behaviour change [Citation12,Citation18]. Health Care Professionals (HCP) have been identified as having an important role in guiding plwMS to be more active [Citation25], however, research has reported incidents of HCP demonstrating minimal insight into the role of PA in MS, suggesting a discrepancy between HCP prescription and adherence by plwMS [Citation12,Citation26]. To date qualitative research has focused upon understanding the barriers and facilitators of engaging plwMS in PA and exercise, frequently applying behavioural change/cognitive theory lens to their approaches [Citation12,Citation15,Citation17,Citation18]. Whilst this has enabled valuable insight, arguably the framing may lead to the loss of nuanced meaning and insight into PA and exercise experiences, particularly as research has identified that the needs and opinions of plwMS can differ as disability progresses [Citation8,Citation14].
HCP are encouraged to consider innovative and contemporary approaches to treatment, adopting a holistic approach that listens to patient’s stories and consider experiences from the perspective of those experiencing it and the society and culture in which we live [Citation27,Citation28]. Thus, enabling HCP to frame and personalise treatment approaches and strengthen the therapeutic alliance and enhance trust and self-efficacy [Citation29]. A means of exploring the ambiguity and layers of an individual’s experience has been identified in the form of phenomenologically informed qualitative research [Citation30]. The philosophically rooted principles of phenomenology seek to listen to individuals’ stories, to understand the subjective lived world of everyday experience. To explore how a phenomenon manifests its self to the individual through experience, and its intertwined relationship between person- body- others and the world [Citation31].
Phenomenological research seeks to illuminate the textured, nuanced and embodied characteristics of a phenomenon which can provide valuable insight that may challenge taken-for-granted ways of working for HCP [Citation30,Citation32]. To date literature has not explore the phenomenon of PA and exercise from this perspective for persons living with advanced MS, nor explored the wider breadth of meaning towards physical exertion, beyond the confines of predefined classification of exercise or PA. Thus, this inquiry sought to apply a phenomenology approach to explore this gap in knowledge by investigating the phenomenon of physical exertion from the perspective of persons living with advanced MS.
Materials and methods
An interpretive (hermeneutic) phenomenological approach was adopted to explore the meaning and structure of physical exertion, as it manifests through participants’ lived experiences. Drawing upon the philosophical underpinning of Martin Heidegger’s hermeneutic approach towards phenomenology, the principal researcher took an interpretivist approach, one that recognised that knowledge is unique and subjective [Citation30]. Adopting a world view of minimal hermeneutic realism, they acknowledge that meaning and reality are contextual and personal [Citation33]. That individual’s realities evolve from interpretive process that are influenced by and inseparable from the world that they live. The approach acknowledges that the world becomes part of their subjective, pre-reflective, way of being-in-the-world, where the hyphens between each word represent the connection between the being and the external world [Citation30,Citation34,Citation35].
The principal researcher sought to uncover the hidden, implicit meaning of experience within participants’ accounts, by adopting a “phenomenological attitude”. An open-minded approach to exploring the phenomenon from a new perspective by bridling (or holding back) their past knowledge and preconceptions, and being open to being surprised [Citation34]. The principal researcher’s preconceptions, were identified through a process of introspective self- reflexivity, whereby existing beliefs and opinions were identified and critically evaluated as to their influence on their understanding and interpretation [Citation36]. The principal researcher approached the inquiry as an able-bodied, white, heterosexual, female who has been educated and worked within a Western medical model as a Physiotherapist and had extensive experience of treating plwMS. The principal researcher acknowledged that their pre-understanding could not be fully removed from the interpretation, instead, they sought to develop a respectful attitude towards the phenomenon, by remaining attentive and sensitive to participants’ experiences but acknowledged their role in giving body to the phenomenon and in the explication of meaning [Citation34].
Recruitment
Eight participants were purposefully recruited to the inquiry from an MS therapy centre in the South of England. The therapy centre was a charitable organisation, with membership demographics of predominantly white, Caucasian, English-speaking persons. Participants were recruited from the principal researcher’s place of work, where pre-existing therapeutic relationships could have existed. An email was distributed to the whole centre membership providing information about the study, participant criteria, and recruitment procedures; and information posters displayed in the centre building. Individuals who expressed interest to participate were screened for eligibility and provided with a participant information sheet to read before providing written consent to participation. To minimise the risk of participant coercion, the Centre Manager acted as a gate keeper for recruitment and it was made explicit to participants that the research was in no way connected to, or would influence their treatment at the therapy centre.
Participants
The number of participants varies within phenomenological research, but the literature suggests that interpretative approaches lend themselves towards smaller numbers to avoid losing the voice of participants [Citation37]. Smith et al. [Citation38] suggest 3–6 participants is sufficient to enable in-depth and rich analysis of individual cases whilst exploring the variation in meaning. Existing literature that has explored PA and MS and applied a phenomenological approach have interviewed up to 15 participants [Citation21,Citation39]. In this inquiry, a small homogenous group of 8 participants were recruited in order to achieve depth of phenomenon description and sufficient to explore similarity and differences between participants [Citation30]. Persons were eligible for the study if they met the criteria for having advanced MS, which for the purpose of the inquiry, was determined by a self-reported diagnosis of MS and an inability to walk unaided (with a maximal walking ability of 20 metres with walking aid). In the absence of a consistent classification system within research, the inclusion of demographical and clinical characteristics was included to aid the clinical application of findings () [Citation15]. Individuals were excluded who competed in the sport at a regional, national, or international level; and those with an unstable health status within the prior 3 months, or with a health condition that could impact their ability to physically exert themselves (such as cardiovascular, respiratory disease, arthritic or orthopaedic conditions). This was based upon factors which could have influenced exertional experience beyond that of their MS. Regular use of mood-related medication was noted as the researcher acknowledged it could influence exertional experience, however it was not deemed to be an exclusion criterion due to the recognised high prevalence of anxiety and depression in plwMS [Citation40].
Table 1. Participant demographic information.
Data collection
At the time of data collection, the United Kingdom was under social distancing restrictions due to the global Covid-19 pandemic, and face-to-face interviews were not permitted, therefore interviews were conducted online using Microsoft Teams. Participants were encouraged to keep cameras on to enhance communication which enabled the researcher to note any pertinent changes in body language within the context of conversation [Citation41]. The interviews were audio recorded and lasted on average 45 min. They were transcribed verbatim, and pseudonyms were used to protect participant identity and confidentiality. All data was stored securely on a university’s OneDrive in accordance to the Data Protection Act and Data Management Policy. Ethical approval was received for the study from the University of Brighton Ethics and Governance Committee prior to commencing participant recruitment.
(Reference 2020-6999).
An interview guide, that was formulated from a practise interview between the researchers prior to commencing the study, acted as an initial framework for conversation (see supplementary information 1). During the interviews notes were taken which acted as a prompt for the principal researcher to return to points of interest, but questioning remained purposefully open to facilitate participants to explore physical exertion from their perspective. Conversation was initiated through the collection of demographic data and acted as an ice breaker to the interview. To ensure conversation was directed to the phenomenon of interest, an opening question asked participants their understanding of the term “physical exertion” and they were asked to give specific examples of their experiences of physical exertion which posed to clarify their thoughts and ideas of what the term meant. Next concrete lived-through experiences were sought by using variations of the question “Can you think back to a time when you experienced physical exertion……take your time to go back to a specific moment….can you tell me about that in as much detail as possible, as though I could imagine I was there?”. The principal researcher adopted an empathetic, active listening approach, using probes such as “If I were to relive the experience in your shoes how would it have felt… what was going through your mind….what were your actions at that time…. What did you do and how did you do it?”. This enabled experiences to unfold and rich descriptions to develop, whilst steering conversation to remain as close as possible to the phenomenon of interest and used concrete descriptions to elicit detail [Citation30].
Data analysis
The principal researcher adopted a sequential, stepped approach to analysis, allowing the meaning of physical exertion to develop, whilst continually holding back existing and evolving perceptions. An idiographic approach was adopted in the analysis, which recognised the individuality of each participant’s experiences, and care was taken to treat each transcript distinctly and rein in evolving understanding before moving onto the next transcript. The researcher initially immersed themself in the data by relistening to recordings and rereading the transcript, making initial notes, and dwelling in the data over a period of days. Each transcript was divided into discrete meaningful units and the semantics of the language explored through its descriptive, linguistic, and conceptual attributes (see supplementary information 2). Connections were explored to illuminate patterns and contradictions within individual accounts. Reference was made to interview notes which described participants’ body language and emotional responses, and were used to convey deeper meaning [Citation41]. As themes developed from within the data, transcript extracts were used to describe the characteristics and authenticate the meaning of physical exertion (see supplementary information 3). The integration of the hermeneutic cycle into the analysis enhanced the depth and rigour of the findings. The cycle of continually moving between parts (such as words or extracts) and the whole (sentences or whole interview), enabled the exploration of both explicit and implicit meaning [Citation34].
The next stage of analysis sought to find similarities and differences between all participants by synthesising and integrating themes, whilst remaining conscious of the philosophical underpinnings of interpretive phenomenology. An overarching superordinate theme, and four underpinning subthemes developed, that represented the meaning and structure of physical exertion for the participants. The final stage of analysis involved the crafting of hermeneutic stories which were used to bring alive the phenomenon and illuminate the intertwined relationship between superordinate and subthemes [Citation31]. Stories representing each individual participant’s account were crafted by retaining sentences containing meaning and then removing elements of repetition or extraneous detail. Linking words were used to bring sentences together and, where necessary, sentence order was changed to enhance the flow of the story [Citation42]. The explicit, detailed, stepped approach to analysis enhanced the systematic rigour of the inquiry. Quotations were used to illustrate characteristics of themes and to illuminate implicit meaning and perception that was embedded within the language. Attributes of themes were collated in tables as points of reference (see supplementary information 4). The second researcher, an experienced qualitative researcher, reviewed all transcripts and commented on all steps of the analysis, at each point entering a dialogue with the principal researcher to explore alternative interpretations and variations on perspectives. The principal researcher’s reflections were kept as written records and acted as a constant source of reference through the research process and became integral to the analysis of findings and hermeneutic circle of interpretation [Citation31,Citation43].
Results
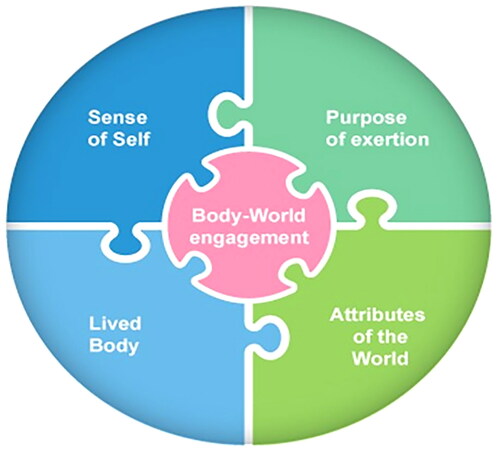
The results summarised the findings of the 8 participants, of which 6 identified as female and 2 as male, and were aged between 45 and 75 years old, and had been living with MS for between 10 and 25 years. They all identified as being unable to walk more than 20 m with a walking aid but 3 identify as full-time wheelchair users, and one of which required a hoist to transfer. The participants conveyed their experiences of physical exertion as a means of engaging with the world through their body. Four subthemes; Sense of Self, Lived Body, Attributes of the World and Purpose of exertion, and a core (superordinate) theme, Body-World engagement were identified, that described the structure, and encapsulated the meaning of physical exertion for the participants. Each subtheme was conveyed through unique explicit and implied characteristics of participants’ experiences and are illustrated as a jigsaw puzzle (), where the dovetail connections between pieces demonstrates the intertwining relationship between the subthemes and the central superordinate theme.
Figure 1. The ‘physical exertion jigsaw puzzle’, illuminates the intertwined relationship between the subtheme pieces and core superordinate theme, where the dovetails between jigsaw pieces imply a sense of connection.
The subtheme, Lived Body encapsulated the sense of the body as a physical object. It was conveyed strongly through participants’ exertional experiences where their accounts illuminate an acute bodily consciousness. Their descriptions of having to “drag” legs, limbs feeling “heavy” and “stubbing toes” highlighted how their physical body had been pushed to the forefront of consciousness. Participant’s appraisal of their body was frequently critical and negatively perceived. They recognised differences in themselves when compared to their pre- MS self, or to others. Their bodies were portrayed as unpredictable, and impairments such as fatigue and loss of movement control, exposed a sense of vulnerability, as illuminated by Adele in her recollection of biking over undulating terrain, when exhaustion set in
“I felt marooned and couldn’t get myself out of the situation” (Adele). Recollection of exertional experiences conjured a wealth of emotional responses from participants, their bodily ability acting as a catalyst to emotional outpourings. These were conveyed in the subtheme Sense of Self, where participants’ subjective feelings and attitudes towards themselves during physical exertion were collated, such as independence through “doing something for myself” (Adele), or frustration at having “force yourself to put one foot in front of another” (John).
An inability to move as desired accompanied descriptions of frustration and conjured a sense of loss of their identity as an upright, able-bodied person and illuminated their beliefs about perceived ways of being-in-the-world. Conversely, all the participants recalled select exertional experiences that had enhanced their Sense of Self. Their descriptions of recreating past physical sensations, such as muscular aches, or achieving physical targets of lifting weights, illuminated the impact of exertion on their sense of wellbeing and agency over their bodies and actions. Participants’ accounts described, and implicitly portrayed, a sense of seeking a perceived “normal” in how they viewed themselves, or how they were identified by others. Their accounts conveyed a sense that physical exertion could both hinder, or enable, their quest for normality, as highlighted by Isobel’s contrasting descriptions of feeling like a “puppet on a string” when being assisted to transfer by carers, yet using an arm cycling machine gave “a sense of satisfaction that you are actually doing it and not somebody else doing it for you” (Isobel).
The subtheme Purpose of exertion encompassed the multiple purposes, or intentions, behind their experiences. It included a range of activity from structured exercise, to accessing the community, engaging with friends, and activities of daily living. Their accounts conveyed an implied sense that purpose was the catalyst to how they approached deliberate exertional activity and this shaped their self-beliefs towards the experience. In contrast, every participant recounted exertion within activities of daily living and they were frequently portrayed with descriptions of frustration and anxiety. Performing activities fundamental to life were conveyed as unavoidable necessities, involving excessive effort.
“Skinning and chopping an onion can probably take me 20 min….you feel like you want to give up. It’s exhausting because you become so frustrated” (Louise).
They often involved the use of assistive devices, such as walking aids, or the support of other people. These adjuncts, along with characteristics such as the environment and the structure of tasks, were highlighted as significantly meaningful and thus are summarised in the subtheme Attributes of the World. This subtheme illuminated the influential effect these characteristics could have on the participants’ ability to engage with the world through exertion, such as Adele’s description of her powered trike being able to give her legs a “boost”. Their influence was portrayed as double-edged, having the potential to be both enhancing and disempowering, depending upon the context and impact of the other components of the physical exertion jigsaw puzzle.
The superordinate theme, Body-World engagement, encapsulated how physical exertion could influence participants’ sense of connection with the world. It was portrayed as a spectrum, where physical exertion could strengthen the connection, illuminated by participant’s positively portrayed accounts which included descriptions of emotional wellbeing and pride in achievements and created a sense their being-at-one-with-the-world. In sharp contrast, at the opposite end of the spectrum, participants’ less positively perceived exertional experiences conveyed a sense of participants’ being-in-discord-with-world. Their accounts describing characteristics of subthemes that became barriers to their engagement in physical exertion and weaken their connection with the world. To illuminate the spectrum of Body-World engagement that naturally occurred in participants’ accounts, their descriptions were individually crafted into (hermeneutic) stories, which revealed the idiographic meaning of physical exertion, and illuminated the unique and contextual relationship between subthemes. The following 4 participant stories have been selected to illuminate this relationship. The remaining 4 participants stories are included as supplementary information (see supplementary information 5).
David’s story
Some days the energy is just gone. Getting out of bed is hard work. I feel worn out on waking and I need to sit down to rest and recover after getting dressed. Standing up is hard, I am constantly moving to try and stay upright. It is so much effort. My bad leg just doesn’t want to go, and the effort makes my breathing heavy and I have to sit down and recover.
After breakfast, I try to do some work in the garden. I can’t stand up but sitting down I can’t manoeuvre things. All of a sudden, I run out of energy, the tank goes to negative. I’m left feeling useless with nothing left in me. If I carry on, I know I would wreck it. I have knackered myself. There’s no use crying about it, I just have to sit and rest for 5 min and then I see if I can carry on. It makes me feel fed up, annoyed, but I just have to cope with it. With MS you have bad days and OK days, you really do not know what is going to happen. It makes planning your life very difficult but over the years you just have to accept what is happening.
Despite the unpredictability of my energy levels, I like to maintain my fitness by going to the gym and lifting weights or rowing. When I work out in the gym, I feel a “good worn outness”, I’ve done something normal, like everyone else. It’s not the same as the fatigue I get at home. It’s like when you do any form of cardiovascular exercise and you push yourself, there comes that point when you are worn out, a physical knackeredness, a tired feeling.
I like doing group rowing sessions with a coach. I really push myself, something I never do outside the gym. I think when you are exercising by yourself it is very easy to give up but, in a team, there’s a herd feeling of being part of something and it is encouraging. We are all putting ourselves through it and pushing each other. The interval sessions are hard work. We go faster and faster, pushing harder and harder, but you know there is always a definite stopping point when you can rest and recover. The endpoint is important, knowing it is coming is mentally encouraging and you feel as though you can do more. I come out of the gym feeling drained but it’s the worn-out that anybody experiences in the gym. It makes me feel normal.
David story naturally conveyed two contrasting experiences. His recollection of physical exertion through activities of daily living, and structured exercise in a gym, illuminated the breadth of activities he characterised as exertion. David’s story strongly conveys the influence of his Lived Body, on his Sense of Self. When his abilities fail to meet his expectations, such as standing to the garden, his Lived body is pushed to the forefront of his consciousness, his language articulating his frustration. His story attributes a strong desire to stand, and his inability to engage with the world from an upright position resonating a sense of lost identity. David refers to his “drained” energy tank twice in his story. When recalled in the context of working in his garden, it is conveyed as problematic, a sensation that illuminates his disability and accompanied a sense of frustration and despondence towards his Lived Body. Yet, when he describes coming out of the gym feeling “drained”, he attributes it to feeling “normal”, conveying a sense of regaining his lost identity. His description of “good wornoutness” conveys his body in the forefront of his consciousness but in a desirable manner and association with recreating past sensations of achievement and enjoyment.
David drew positively upon Attributes of the World, such as the conveyed comradery of exercising as part of a group and the structure of the interval sessions. They were portrayed as a means of overcoming barriers, by having an enabling influence which strengthened the connection between the body and the world. Not all attributes were consistently perceived. Rest points, pre-set by the coach were conveyed as acceptable within the gym session, yet those initiated by himself, such as when he recalled needing to sit and rest in the garden, were less positively perceived. Here, his recollection of needing to rest conveyed a sense of being a reminder of his inability and loss of bodily control. Similarly, the influence of exertion on David’s wellbeing was contextual. The undesirable effort he portrays during activities of daily living reflected a sense diminished body-world engagement and being-in-discord-with-world. Whereas his portrayal of gym-based effort was as an opportunity for him to take control of his MS by facilitating a sense of agency over his actions, and in doing so, strengthen his Body-World engagement and enhance his connection with the world.
Julie’s story
I can’t walk far these days, but it’s different in my garden. I love being in my garden and it doesn’t feel like a hardship when I’m walking in it with my rollator. I love taking in the views and picking blackberries. I try and do several circuits every day. My mind often thinks I can do more but physically I know I couldn’t. I keep trying though as I have been inspired by Captain Tom. I figure if he can do it at 100 years old then I can do it at my age! My walker has a seat, so I keep going until I need to sit down and have a rest. Fifteen minutes is usually enough rest then I have a go at another 20 steps or so before I need to sit down again. I’ve become very patient, I am conscious of moving slowly, concentrating on lifting my legs. I imagine a wall that I’ve got to get over. I can stop as many times as I want but I am determined that I will get over it. The concentration can be exhausting but the elation of achievement succeeds it. I just love being-in-my-garden, feeling safe surrounded by the trees.
If you put me in a town centre and told me to walk with my frame, even if it were the same distance as the garden, I would instantly feel horrified. All I would see is concrete everywhere, and fear would develop that my legs were going to turn to jelly and I’d end up stranded, stuck, and unable to get back. If I did start walking, I’d worry my muscles would stop suddenly, unresponsive to my request to move; I’d be paralysed… terrified that I couldn’t move my body. I’m learning to recognise the signs that paralysis is close. Butterflies in my stomach, pins and needles in my hands and my breathing becomes shallower. I start to stub my toes as I walk and I know I need to stop, sit down, rest until I regain control and feel ready to start again. It all feels so different in the garden, I know if I fall in the garden, I haven’t got far to get up. Someone, family or friend, will help me by lending me an elbow, a prop to get back up. Even if they don’t come straight away, I know they will find me. That makes me feel safe.
Julie’s story illuminates the breadth of characteristics of Attributes of the World, such as the environment, walking aids and other people, and their impact on her Sense of Self during her exertional experiences. Her story demonstrates the importance of environmental aesthetics in enabling her to feel safe and of having autonomy over her actions. Exerting herself in her garden were meaningfully related to a sense of being-at-one-with-the-world and strong Body- World engagement. Her repeated use of “love” and description of being free of walking “hardship” in the garden, conveyed a sense that her Lived Body was no longer at the forefront of her consciousness, instead, she was able to dwell upon the scenery and activities. Her recollection of her rollator, evoked a sense of it becoming embodied to her exertional experience. The tree-lined border of the garden conveyed a sense of security, a boundary, and a sense of being concealed from the critical gaze of other people. Conversely, her recollection of exertion in the town centre depicts a sense of disharmony with the world. Her description of “concrete everywhere” conveyed an implied sense of exposure and vulnerability. The environmental aesthetics suddenly interrupting any enabling influence of Attributes of the World, and negotiating her Lived body through it became the focus of her attention.
There is a sense of acute bodily consciousness resonating through Julie’s story, portrayed through her description of learning to identify and adjust to change in her Lived Body. She recalls past experiences and their influence on her beginning to recognise how her Lived Body and Sense of Self are interconnected. She seeks to identify methods of maintaining control, such as moving slowly and resting, as a means of self-preservation. Julie’s story portrays a sense of being-at-one in her own company when exerting herself, where being alone enables her freedom to engage with the world at her own pace. Unlike David who thrived on exertion amongst likeminded people, Julie’s reference to other people was in the context of “props”, which conveyed a sense of them as an alternative source of assistive device. She recalls the walking achievements of Captain Tom as a source of inspiration, yet also comparison, which suggests an implied inward critical gaze towards herself.
Anne’s story
I think it is very easy to underestimate the effort of everyday activity. At home I push myself in my wheelchair, it’s tough, my limbs feel like they have got weights tied onto them, making everything harder. Then someone leaves their shoes out, or a door closed, the obstacles make it harder, and I get so angry, the frustration uses up energy and it’s like a catalogue of events, that ends in an energy wipe out. Other times I’ve sat for a quarter of an hour looking at a cup, just to focus my mind and summon the energy to pick it up to drink. You wouldn’t believe how much energy it takes to concentrate on my fingers. It sounds pathetic but it is so incredibly challenging, it’s mind over matter. I will be determined to do it, and when I get my fingers to move, it’s a lovely feeling.
I underestimate familiarity and the ease it adds to movement. Negotiating unfamiliar toilets is exhausting. Trying to get yourself in the right position to open the door, then move around poorly positioned sinks or bins is stress-provoking. Panic sets in, manoeuvring backwards and forwards in poorly ventilated rooms, getting hotter and hotter, tireder and tireder until I pause; refocus, and take a moment, gather my thoughts, and plan my escape. There’s a sense of sheer relief once I get out. Being with other people can be helpful, but then you need to consider their thoughts and wishes, which means more to coordinate and plan.
I like going to the centre and standing in a frame in therapy sessions. I know that I am using energy, I feel tired when I get home but standing feels like I am putting energy into my body, to hold it in position. Standing up feels like I have re-joined the “normal” world. I’m doing something that everyone else takes for granted. Being upright and talking with friends is exciting and time flies. Even if it feels harder than normal, I won’t get down. I’m too stubborn, I enjoy it too much! I’ll recover at home in the chair. I’ll close my eyes and before I know it, I’ve fallen asleep for half an hour! Rested and ready to re-engage.
Anne’s story illuminates the intertwined relationship between the Lived Body and Sense of Self through her descriptions of the physical and mental effort required for her to exert herself. Her recollection of energy highlights a sense of it as her fuel for effort. Activities of daily living were conveyed as energy-sapping and highly effortful, yet expending effort to use a standing frame was portrayed as energising. Her description of “re-joining the normal world” when using the standing frame, illuminated her self-beliefs and suggests a sense of reclaiming a lost “upright” identity, where enabled her disability to be pushed into the background of the experience. Not all Attributes of the World were empowering and her story conveyed the subtle changes in characteristics that had a significant disconnecting effect on her exertional experience, such as a misplaced shoe or poorly positioned bin. The resultant “energy wipe out” illuminated a loss of Body-World engagement and sense of total disconnect with the world.
Carrie’s story
I have always been active, I used to play sport competitively and took it pretty seriously, winning various trophies. It was a major bereavement when I could no longer play when my physical ability was utterly pooped by MS. I try doing an interval weights programme in the gym. I was sceptical at first, I hadn’t done anything like that before. Gradually the weights increased and I enjoined the challenge of increasing my strength, recording the changes on my phone. I regained my competitiveness, that I had lost when sport stopped. I hadn’t realised that I missed it, but the one-and-a-half years’ worth of statistics on my phone has become a source of pride and achievement for me.
When I use the weights, it gives me a very erect back and keeps my shoulders back. It makes me hold my core in a decent position, upright rather than slumping in my wheelchair. I feel safe in the gym, and that gives me permission to push myself. Sometimes I’m gripping onto the weights thinking “oh my god can I do this?”…… and I do, and I feel really good about it. When I use the leg press and feel the exhaustion in my buttock and hip muscles, it reminds me of being active in the past. I enjoy being able to recreate that feeling of something that I used to be good at, challenging myself and the feeling of exhaustion afterwards.
The left side of my body is “the weakest link”, “it” is a source of crapulence for me. There are activities in the gym that really highlight the discrepancy between “it” and “my” right side and I find that absolutely bereaving. It’s terrible knowledge, and it feels like my MS is being rubbed in my face. When I’m doing weighted pull-downs, I can see I’m losing my grip in the left hand, but I can’t re- engage the curve of the fingers to hold on properly. I have a feeling of surmounting terror that there is going to be a ghastly crash as the thing goes flying back and I’m terrified at the thought of drawing attention to myself. It makes me feel like a failure; my hands physical inability and my incompetence to avoid it happening, like I have been caught out.
Carrie’s story illuminates how the Purpose of exertion, weight training in the gym, enables her to enhance her Lived Body and regain her competitiveness, which she reflects was a core component of her pre-MS identity. The account conveys a fragility to her Body- World engagement, one that is influenced by the ability of physical exertion to draw the Lived Body to the forefront of her consciousness. The double-edged nature of physical exertion is illuminated by her description of how physical exertion could enhance her Body-World engagement by disguising her perceived disability, but when uncovered it enhanced her self-criticism and sense of disconnect from the world. The importance of Attributes of the World on her Sense of Self is conveyed by her description of how the accessible gym environment was portrayed as a place that she felt safe to expose both her physical and emotional vulnerabilities, whilst providing an opportunity to recreate a sense of self, otherwise lost to MS.
Discussion
This inquiry portrayed the meaning of physical exertion for persons living with advanced MS, as an opportunity to influence their connection between their body and the world. Participants’ accounts illuminated their holistic view of the body through the integral relationship portrayed between the themes Sense of Self and Lived Body. The concept of phenomenological embodiment considers the body as something that a person both interacts with the world through (the objective body) and, how they view the world (the subjective body) [Citation30]. Characteristics of the Lived Body echo those of the objective body, as a physical object which engages with the world. Whilst characteristics of the Sense of Self, are comparable with those of the subjective body; a person’s bodily sense, that is influenced by memory, perception, emotion, and cognitive relations [Citation34]. Participants’ accounts illuminated their role as “beings-in-the-world”, not self-contained objects but beings that were immersed in, and open to the world around them [Citation30].
The sense of connection conveyed through Body-World engagement resonates with the concept of connectivity, where persons define themselves through their connection with entities around them [Citation27]. A strong connection made the relationship between subthemes appear seamless and conveyed a sense that participants were “being-at-one-with-the-world”, where their feelings implied a sense of belonging, within a taken-for-granted world [Citation30]. Whereas exertional experiences portraying a diminished connection, illuminated a fragmented relationship between subthemes, where participants conveyed a sense of being detached from the world. Connectivity concept takes a new materialist, non-anthropocentric perspective by considering the interaction of persons with assemblages, such as other people, objects, environment, and ideas [Citation27]. The characteristics of Attributes of the World illuminates the breadth of meaning of assemblages for physical exertion for participants, and included walking aids, wheelchairs, the environment, and other persons. Assistive equipment was a prominent feature of Attributes of the World and accompanied a sense of participants learning a new style of being-in-the-world, where the device could become embodied, or part of their being [Citation44,Citation45]. Participants’ acceptance of their new style was varied and aligns with the suggestion that a person’s being-in-the-world, and ability to adjust to new styles, is influenced by the meaning and value they attribute to the interaction and objects involved [Citation46].
The physical body featured frequently in participants’ accounts and was illuminated in the subtheme “Lived Body”. At times participants’ explicit descriptions conveyed a sense of the body-as-machine, an object that they analysed and judged upon its ability, yet analysis of their accounts illuminated the implicit meaning of the body that expanded beyond the biological and physiological boundary. They portrayed a sense of the body-as-it-lived, a subjective body that bore style and identity which influenced how participants engaged with the world [Citation30]. It has been suggested that illness disrupts the harmonic relationship between the body and the world [Citation47]. During less positively perceived experiences of physical exertion, participants’ accounts give a sense of bodily dissonance, where they dwelled on their bodily impairments. Their focus aligns with the concept of bodily dys-appearance, where the ability to engage freely and spontaneously with the world is disrupted, resulting in the body becoming an obstacle to their engagement with the world [Citation48,Citation49]. In these situations, participants conveyed a sense of lost self-agency, whereby they no longer had control over their own situation. In more positivity portrayed exertional experiences, participants conveyed a sense of enhanced self-agency, through an implied autonomy over their actions and ability self-regulate according to the needs of their bodies. These findings concur with previous research that found that plwMS who felt in control of their actions, were more likely to repeatedly engage in physical activity [Citation50]. In this inquiry, exertion portrayed the potential to both enhance and diminish agency, illuminating the significance of understanding the influence of all the subthemes on a person’s body-world connection.
The sense of bodily consciousness that accompanied exertional experiences illuminated how perceived bodily ability, or inability, conveyed a strong shaping effect on individuals’ perspective of the world and perception of self [Citation38]. The theme Sense of Self conveyed how exertional experiences portrayed disparity between desired and actual ability, and participants’ eagerness to “be like everyone else” or “normal”. These findings resonate with philosophical underpinnings of phenomenology, which recognise that person’s existence is dependent on interaction with others, and conforming to shared communal norms, one where the self is determined, in part, by social, cultural, and historical influences [Citation30,Citation46]. However, society’s influence on individuals’ sense of self has been argued to be biased towards valuing citizens who are persons of able body and mind, who are deemed to be productive and viable to society. The view, defined by Disability Concept, argues that society leads persons to have an ability- based (ableist) understanding of oneself; one’s body, others, and the world [Citation51]. Participants’ lived experiences conveyed a sense of desire to maintain an upright identity, which could be interpreted as a desire to maintain a bodily appearance that adheres to societal normal. However, for some participants, the influence of social identity was portrayed as a positive influence on physical exertion. David’s enthusiasm for exercising amongst likeminded individuals illuminated the influence that others can have on shaping an individual’s perception of the world, and how they view themselves [Citation30]. His expressed desire to achieve behavioural norms and values of the group concur with existing literature that suggests that for plwMS exercising amongst others can enhance well-being and motivation [Citation12,Citation52].
A diverse meaning of physical exertion was conveyed through the subtheme Purpose of exertion, and it illuminated how some participants identified exertion as a means of taking back control of their bodies from the impact of MS through regaining or creating a new identity. These findings echo existing literature that highlight the role of exercise and PA as a coping mechanism, in regaining some control and enhancing wellbeing when living with MS [Citation15,Citation53]. In this inquiry, not all physical exertion was empowering. Exertion involving activities of daily living (ADL), was frequently portrayed less positively by participants, and was associated with negatively perceived effort and emotional distress. Their accounts concur with existing literature that suggests HCP may underestimate the effort required for plwMS to perform ADL [Citation54]. It has been argued that ADL form the foundations of a person’s engagement with the world from birth, and as a consequence can become an implicit source of comparison of a persons’ pre and post-illness identity [Citation47]. Participants’ accounts conveyed an implicit sense of this, their description portraying bodies that could no longer function as they did pre-MS during tasks fundamental to life. There have been suggestions in previous research that ADL could be an untapped source of PA for plwMS, but the findings from this inquiry suggest approaching this idea with caution [Citation22].
In this inquiry participants positively portrayed their interactions with HCP, and their membership to an MS therapy centre where specialist staff may have contributed to this portrayal. Previous research has suggested a gap in HCP theoretical knowledge and practical application of exercise and PA for plwMS [Citation26]. This phenomenological inquiry provides a more in-depth, nuanced, understanding of the day-to-day realities of physical exertion for persons living with advanced MS. It did not aim to formulate theory, but to enlighten readers by giving voice to participants’ experiences, which can generate new insight and understanding [Citation31,Citation32]. It is hoped that readers will take time to dwell in these participants’ stories and consider how the physical exertion jigsaw puzzle may hold meaning for persons receiving their care. The insight can enhance HCP understanding in relation to exercise and PA prescription and encourage a holistic, person-centred approach to therapy.
The inquiry’s findings support the diversity of meaning of physical exertion, conveying a sense of opportunity, and the capacity to enable but also disempower individuals depending upon the circumstances. Self-beliefs, past experiences, and identity shaped exertional experiences, as did the importance for participants to appear “normal”. This inquiry’s findings encourage HCP to consider the wider context of the body in physical exertion, beyond the object that can, or cannot move, but one that is embodied with a persons’ sense of self. Participants were acutely aware of how their bodies failed to meet their expectations. As a result, HCP are encouraged to consider how they portray the body in their language, that could heighten their sense of failure and inhibit further the ability for a person to engage freely with the world. Instead, they could consider characteristics of the “physical exertion jigsaw” to challenge beliefs about where bodies begin and end and find means of enhancing persons’ connection with the world in different ways [Citation27]. By taking time to explore a person’s beliefs, past experiences, and identity, HCP can begin to understand the body from the perspective that encapsulates a person’s wishes, dreams, and hopes. In doing so they can begin to understand how connections between the components of the physical exertion jigsaw puzzle can be strengthened.
Limitations
This inquiry presents findings that reflect data that was co-constructed and framed between the researchers and 8 participants, some of whom had a prior therapeutic relationship with the principal researcher. This, and the principal researcher’s prior knowledge of the phenomenon, was acknowledged within the interpretive process. The principal researcher was committed to engaging in reflexivity and bridling of presumptions throughout the research process, seeking to maintain an open-minded, “phenomenological attitude” towards the phenomenon of physical exertion. The principal researcher’s engagement in the hermeneutic cycle enhanced the credibility of findings, through a process of questioning and answering relationships between implicit pre- understanding and explicit understanding [Citation30]. Participant validation of findings was not incorporated into the analysis, as it was not deemed compatible with the principal researcher’s adoption of the phenomenological attitude, but self- critical reflexive analysis by the principal researcher enhanced the dependability and conformability of the interpretation of findings [Citation30].
A systematic approach to analysis with an auditable trail of evidence contributed to the inquiry’s rigour and transparency [Citation30]. The incorporation of participants stories to present findings is a novel approach but contributes to the resonance of the phenomenon of physical exertion, by encouraging readers to dwell and be drawn into the experiences with vivid and rich detail [Citation42]. Their evocative nature sensitises readers to the complexities of physical exertion, and push boundaries of the taken for granted [Citation30,Citation55]. Whilst the researcher recognises that the findings are not representative of all persons living with advanced MS, they have relevance to HCP practice by providing insight into the challenges of living with MS.
A characteristic of all participants was their membership to an MS therapy centre that provided physical activity opportunities. This may have influenced their perception of exertion; however, their concrete examples described a spectrum of activities beyond those offered at the therapy centre. Additionally, the number of participants enabled sufficient data analysis to identify meaningful similarities and differences in their accounts of physical exertion, whilst the hermeneutic stories acknowledged the idiographic nature of the inquiry. The research was conducted under the backdrop of the Covid-19 pandemic, national lockdowns, and social distancing restrictions. Literature has suggested that globally, many adults were less physically active than usual due to Covid-19 restrictions, and this may have influenced the findings from this study [Citation56]. The inquiry aimed to explore the experiences of persons with advanced MS and recruitment was based upon participants’ self-reported assessment of physical capability and was subject to their interpretation, however, it acknowledges the interpretative basis of reality. The inclusion of participant demographics provides context and enables readers to evaluate and transfer findings to contexts more or less similar to this study, whilst acknowledging that the experiences of the participants are temporal [Citation38].
Conclusion
These findings illuminate an alternative perspective on the phenomenon of physical exertion for persons living with advanced MS, by considering it as a means of influencing the connection between the person and the world. Participants’ accounts convey the embodied relationship between their sense of self and their body, and their intertwined relationship with the world; a world that encompassed people, objects, the environment, and society. The hermeneutic stories illuminate the empowering potential of PE on enhancing the sense of self by creating agency and a source of identity, yet also highlight the impact PE can have on enhancing bodily consciousness and illuminating variation from normal, leading to a sense of disconnect from the world. HCP are encouraged to take time to explore a person’s self-beliefs, past experiences, and identity to better understand how exertional experiences can be enhanced for persons living with advanced MS.
Supplemental Material
Download MS Word (32.3 KB)Acknowledgements
The principle author received a bursary from the MS Trust towards academic study costs.
Disclosure statement
This inquiry was conducted as part of a Master in Research conducted at the University of Brighton.
Additional information
Funding
References
- Multiple Sclerosis Society. MS in the UK. MS prevalence report; 2020.
- Vellinga M, Geurts J, Rostrup E, et al. Clinical correlations of brain lesion distribution in multiple sclerosis. J Magn Reson Imaging. 2009;29(4):768–773. doi:10.1002/jmri.21679.
- Andravizou A, Dardiotis E, Artemiadis A, et al. Brain atrophy in multiple sclerosis: mechanisms, clinical relevance and treatment options. Auto Immun Highlights. 2019;10(1):7. doi:10.1186/s13317-019-0117-5.
- Crayton H, Rossman H. Managing the symptoms of multiple sclerosis: a multimodal approach. Clin Ther. 2006;28(4):445–460. doi:10.1016/j.clinthera.2006.04.005.
- Ziemssen T. Symptom management in patients with multiple sclerosis. J Neurol Sci. 2011;311(Suppl 1):48–52. doi:10.1016/S0022-510X(11)70009-0.
- Parker L, Topcu G, De Boos D, et al. The notion of “invisibility” in people’s experiences of the symptoms of multiple sclerosis: a systematic meta-synthesis. Disabil Rehabil. 2021;43(23):3276–3290. doi:10.1080/09638288.2020.1741698.
- Mozo-Dutton L, Simpson J, Boot J. MS and me: exploring the impact of multiple sclerosis on perceptions of self. Disabil Rehabil. 2012;34(14):1208–1217. doi:10.3109/09638288.2011.638032.
- Kalb R, Brown TR, Coote S, et al. Exercise and lifestyle physical activity recommendations for people with multiple sclerosis throughout the disease course. Mult Scler. 2020;26(12):1459–1469. doi:10.1177/1352458520915629.
- Learmonth Y, Chan Z, Correia H, et al. Exercise participation and promotion in the multiple sclerosis community; perspectives across varying socio-ecological levels. Disabil Rehabil. 2021;43(25):3623–3638. doi:10.1080/09638288.2020.1743778.
- Stennett A, De Souza L, Norris M. Physical activity and exercise priorities in community dwelling people with multiple sclerosis: a Delphi study. Disabil Rehabil. 2018;40(14):1686–1693. doi:10.1080/09638288.2017.1309464.
- Adamson B, Adamson M, Kinnett-Hopkins D, et al. Medicalization of exercise through vigilance, productivity, and self-care: a secondary data analysis of qualitative interviews among those with multiple sclerosis. Adapt Phys Activ Q. 2022;39(4):399–423. doi:10.1123/apaq.2021-0200.
- Learmonth YC, Rice IM, Ostler T, et al. Perspectives on physical activity among people with multiple sclerosis who are wheelchair users: informing the design of future interventions. Int J MS Care. 2015;17(3):109–119. doi:10.7224/1537-2073.2014-018.
- Dlugonski D, Joyce R, Motl R. Meanings, motivations, and strategies for engaging in physical activity among women with multiple sclerosis. Disabil Rehabil. 2012;34(25):2148–2157. doi:10.3109/09638288.2012.677935.
- Richardson E, Barstow E, Motl R. A narrative exploration of the evolving perception of exercise among people with multiple sclerosis. Qual Res Sport Exerc Health. 2019;11(1):119–137. doi:10.1080/2159676X.2018.1509369.
- Learmonth Y, Motl R. Physical activity and exercise training in multiple sclerosis: a review and content analysis of qualitative research identifying perceived determinants and consequences. Disabil Rehabil. 2016;38(13):1227–1242. doi:10.3109/09638288.2015.1077397.
- Moffat F, Paul L. Barriers and solutions to participation in exercise for moderately disabled people with multiple sclerosis not currently exercising: a consensus development study using nominal group technique. Disabil Rehabil. 2019;41(23):2775–2783. doi:10.1080/09638288.2018.1479456.
- Adamson B, Kinnett-Hopkins D, Athari Anaraki N, et al. The experiences of inaccessibility and ableism related to physical activity: a photo elicitation study among individuals with multiple sclerosis. Disabil Rehabil. 2022;44(12):2648–2659. doi:10.1080/09638288.2020.1844315.
- Fakolade A, Lamarre J, Latimer-Cheung A, et al. Understanding leisure-time physical activity: voices of people with MS who have moderate-to-severe disability and their family caregivers. Health Expect. 2018;21(1):181–191. doi:10.1111/hex.12600.
- Horton S, MacDonald D, Erickson K, et al. A qualitative investigation of exercising with MS and the impact on the spousal relationship. Eur Rev Aging Phys Act. 2015;12(1):3. doi:10.1186/s11556-015-0148-5.
- Edwards T, Pilutti L. The effect of exercise training in adults with multiple sclerosis with severe mobility disability: a systematic review and future research directions. Mult Scler Relat Disord. 2017;16:31–39. doi:10.1016/j.msard.2017.06.003.
- Borkoles E, Nicholls A, Bell K, et al. The lived experiences of people diagnosed with multiple sclerosis in relation to exercise. Psychol Health. 2008;23(4):427–441. doi:10.1080/14768320701205309.
- Stennett A, De Souza L, Norris M. The meaning of exercise and physical activity in community dwelling people with multiple sclerosis. Disabil Rehabil. 2020;42(3):317–323. doi:10.1080/09638288.2018.1497715.
- Roberts M, Mynors G, Bowen A. Improving services for people with advanced multiple sclerosis. Letchworth: Multiple Sclerosis Trust; 2016.
- Davies F, Edwards A, Brain K, et al. You are just left to get on with it: qualitative study of patient and carer experiences of the transition to secondary progressive multiple sclerosis. BMJ Open. 2015;5(7):e007674. doi:10.1136/bmjopen-2015-007674.
- National Institute for Clinical Excellence. Multiple Sclerosis in adults: management. London: NICE. 2014.
- Stennett A, De Souza L, Norris M. A qualitative exploration of physiotherapists’ perceptions about exercise and physical activity: reflections on the results from a Delphi study. Disabil Rehabil. 2020;42(22):3142–3151. doi:10.1080/09638288.2019.1585969.
- Nicholls D, Atkinson K, Bjorbækmo W, et al. Connectivity: an emerging concept for physiotherapy practice. Physiother Theory Pract. 2016;32(3):159–170. doi:10.3109/09593985.2015.1137665.
- Anjum RL, Copeland S, Rocca E. Conclusion: causeHealth recommendations for making causal evidence clinically relevant and informed. In: Anjum RL, Copeland S, Rocca E, editors. Rethinking causality, complexity and evidence for the unique patient: a CauseHealth resource for healthcare professionals and the clinical encounter. Cham: Springer International Publishing; 2020. p. 237–241.
- Low M. Above and beyond statistical evidence. Why stories matter for clinical decisions and shared decision making. In: Anjum RL, Copeland S, Rocca E, editors. Rethinking causality, complexity and evidence for the unique patient: a CauseHealth resource for healthcare professionals and the clinical encounter. Cham: Springer International Publishing; 2020. p. 127–136.
- Finlay L. Phenomenology for therapist. Researching the lived world. Oxford: Wiley- Blackwell; 2011.
- Finlay L. Engaging phenomenological analysis. Qual Res Psychol. 2014;11(2):121–141. doi:10.1080/14780887.2013.807899.
- Fernandez A. Embodiment and objectification in illness and health care: taking phenomenology from theory to practice. J Clin Nurs. 2020;29(21–22):4403–4412. doi:10.1111/jocn.15431.
- Larkin M, Watts S, Clifton E. Giving voice and making sense in interpretative phenomenological analysis. Qual Res Psychol. 2006;3(2):102–120. 2006/01/01doi: 10.1191/1478088706qp062oa.
- Dahlberg K, Dahlberg H, Nyström M. Reflective lifeworld research. 2nd ed. Lund: Studentlitteratur; 2011.
- Shaw J, Connelly D. Phenomenology and physiotherapy meaning in research and practice. Phy Ther Rev. 2012;17(6):398–408. doi:10.1179/1743288X12Y.0000000043.
- Finlay, L, Gough B, editors. Reflexivity. A practical guide for researchers in health and social science. Oxford: Blackwell Publishing; 2003.
- Bartholomew T, Joy E, Kang E, et al. A choir or cacophony? Sample sizes and quality of conveying participants’ voices in phenomenological research. Methodol Innov. 2021;14(2):205979912110400. 20597991211040063. doi:10.1177/20597991211040063.
- Smith J, Flowers P, Larkin M. Interpretative phenomenological analysis: theory, method and research. Los Angeles: Sage Publications; 2009.
- Adamson BC, Adamson MD, Littlefield MM, et al. ‘Move it or lose it’: perceptions of the impact of physical activity on multiple sclerosis symptoms, relapse and disability identity. Qual Res Sport Exerc Health. 2018;10(4):457–475. doi:10.1080/2159676X.2017.1415221.
- Jones K, Ford D, Jones P, et al. A large-scale study of anxiety and depression in people with multiple sclerosis: a survey via the web portal of the UK MS register. PLoS One. 2012;7(7):e41910. doi:10.1371/journal.pone.0041910.
- Kvale S. Interviews. An introduction to qualitative research interviewing. London: Sage Publications; 1996.
- Crowther S, Ironside P, Spence D, et al. Crafting stories in hermeneutic phenomenology research: a methodological device. Qual Health Res. 2017;27(6):826–835. doi:10.1177/1049732316656161.
- Suddick K, Cross V, Vuoskoski P, et al. The work of hermeneutic phenomenology. Int J Qual Methods. 2020;19:160940692094760. doi:10.1177/1609406920947600.
- Papadimitriou C. Becoming en‐wheeled: the situated accomplishment of re‐embodiment as a wheelchair user after spinal cord injury. Disabil Soc. 2008;23(7):691–704. doi:10.1080/09687590802469420.
- Winance M. Trying out the wheelchair: the mutual shaping of people and devices through adjustment. Sci Technol Human Values. 2006;31(1):52–72. doi:10.1177/0162243905280023.
- Gallagher S, Zahavi D. The phenomenological mind. London: Routledge; 2007
- Carel H. Illness: the crying of the flesh. 3rd ed. London: Routledge; 2013.
- Leder D. The absent body. Chicago: The University of Chicago Press; 1990.
- Zeiler K. A phenomenological analysis of bodily self-awareness in the experience of pain and pleasure: on dys-appearance and eu-appearance. Med Health Care Philos. 2010;13(4):333–342. doi:10.1007/s11019-010-9237-4.
- Learmonth Y, Heritage B. Motivations toward exercise participation: active persons with multiple sclerosis have greater self-directed and self-capable motivations. Arch Phys Med Rehabil. 2021;102(6):1232–1235. doi:10.1016/j.apmr.2020.10.138.
- Goodley D. Dis/ability studies: theorising disablism and ableism. London: Routledge; 2014.
- Plow M, Mathiowetz V, Resnik L. Multiple sclerosis: impact of physical activity on psychosocial constructs. Am J Health Behav. 2008;32(6):614–626. doi:10.5993/AJHB.32.6.6.
- Fasczewski K, Gill D, Rothberger S. Physical activity motivation and benefits in people with multiple sclerosis. Disabil Rehabil. 2018;40(13):1517–1523. doi:10.1080/09638288.2017.1300946.
- Currie A, Knox K, Glazebrook K, et al. Physical activity levels in people with multiple sclerosis in Saskatchewan. Int J MS Care. 2009;11(3):114–120. doi:10.7224/1537-2073-11.3.114.
- Todres L. Being with that: the relevance of embodied understanding for practice. Qual Health Res. 2008;18(11):1566–1573. doi: 10.1177/1049732308324249.
- Caputo E, Reichert F. Studies of physical activity and COVID-19 during the pandemic: a scoping review. J Phys Act Health. 2020;17(12):1275–1284. doi:10.1123/jpah.2020-0406.