
Abstract
Purpose
To gain a comprehensive understanding of experiences related to being physically active in participants with an uncomplicated type B aortic dissection.
Materials and methods
We performed a qualitative, phenomenological study. First-person accounts of adults, who at least one year ago had an uncomplicated type B aortic dissection, were collected using semi-structured interviews. The audio recordings of the interviews were transcribed verbatim and analyzed with interpretative phenomenological analysis.
Results
We collected, in total, 644 min interview data from 14 participants. Three patterns were interpreted: losing self-confidence, regaining self-confidence, and continuing to build self-confidence. Experiencing symptoms when pushing limits, challenges with energy management, and side effects of medication caused loss of self-confidence. Changes in identity, reaching milestones that reflect improvement, and support from others and tools helped participants regain self-confidence. To continuing to build self-confidence, participants indicated they needed success experiences and activities make life worth living.
Conclusions
Self-confidence in adults with an uncomplicated type B aortic dissection changes immediately after the diagnosis of the aortic dissection. Rehabilitation professionals can support adults regaining and continuing to build self-confidence, aiming for the perfect balance between blood pressure regulation, quality of life, and being physically active.
Rehabilitation professionals should support regaining and continuing to build self-confidence related to being physically active in adults with type B aortic dissection in the early stages of recovery and beyond.
Adults with an uncomplicated type B aortic dissection want rehabilitation professionals to tell them primarily what is possible (recommendations) rather than what is not allowed (rules).
Rehabilitation professionals should help adults with an uncomplicated type B aortic dissection to explore, push and, ultimately, accept limits related to exercise tolerance.
Implications for rehabilitation
Introduction
A type B aortic dissection is a life-threatening cardiovascular condition in which arterial blood in the aorta escapes through a tear in the intima layer, causing blood to enter between the intima and media layer along the axis of the aorta [Citation1]. The incidence of uncomplicated type B aortic dissections is estimated to be 1.6 per 100 000 per year.[Citation2] An aortic dissection is classified as type B, according to the Stanford classification, if the tear in the intima is distal to the take-off of the left subclavian artery [Citation3]. A type B aortic dissection can be managed conservatively without surgery, with open or endovascular surgery, or with a combination [Citation4]. The best management of type B aortic dissection – conservative management versus surgical management – is still uncertain and challenging [Citation5]. Cornerstones for the treatment of type B aortic dissection are blood pressure regulation, lifestyle rules, and rehabilitation [Citation6]. For example, adults with an uncomplicated, conservatively managed, type B dissection are advised to use beta-blockers, avoid heavy lifting, and exercise at low or moderate intensity [Citation6]. An uncomplicated aortic dissection and its treatment greatly affect people’s physical activity, as they may suffer from severe movement anxiety and fatigue symptoms. All interventions aim to decrease aortic wall stress; however, these interventions should also aim to keep as much quality of life as possible.
Interestingly, there is little research being performed on the quality of life of adults with a type B aortic dissection. A recent survey study by Meccanici et al. shows that adults with a type B dissection score significantly worse on six of eight quality of life domains compared to the general population [Citation7]. In particular, the authors highlight low scores in physical domains and bodily pain [Citation7]. Therefore, it seems important stimulate being physically active in this population given its major impact on quality of life. Winnerkvist et al. however, found only minor differences in functioning and well-being between adults with a type B aortic dissection and the normative population [Citation8]. This is remarkable, given the severe symptomology with which this population is familiar [Citation9]. For example, patients experience traumatizing symptoms such as back pain between the shoulder blades, which may lead to fear of movement. Other studies show that adults with a type B aortic dissection experience emotional and mental symptoms that reduce quality of life [Citation10].
The presence of severe symptoms requires expert support from rehabilitation professionals for adults with a type B aortic dissection. This could be even more the case for adults with an uncomplicated type B aortic dissection, as they have not had surgery and sometimes feel like they are walking around with a ticking time bomb. As a first step, it is important for rehabilitation professionals to be able to empathize with challenges patients face. Rehabilitation professionals need to understand lived experiences of patients in order to empathize with patients and “to see what you earlier could not see or was taken for granted” [Citation11]. Phenomenological studies facilitate in-depth exploration of patient narratives and increase understanding of lived experiences in rehabilitation professionals [Citation12]. With an increased understanding, rehabilitation professionals can respond to patients’ needs and provide better healthcare. To date, the challenges of patients with a type B aortic dissection have never been studied nor described in detail. A thorough understanding of what it is like to be physically active with an uncomplicated type B aortic dissection might help rehabilitation professionals to understand the situation that adults with an uncomplicated type B aortic dissection must learn to cope with. Therefore, the purpose of this qualitative study is to gain a comprehensive understanding of experiences related to being physically active in participants with an uncomplicated, conservatively managed, type B aortic dissection.
Materials and methods
Qualitative approach and research paradigm
We performed a phenomenological study to study experiences related to being physically active in participants with an uncomplicated type B aortic dissection. Phenomenology is a philosophical approach to study essential qualities of experiences in participants, first described by Husserl [Citation13]. We performed an interpretive phenomenology in the tradition of Heidegger [Citation14]. Rather than emphasizing description, interpretive phenomenology places more emphasis on the interpretation and comprehension of experiences. Interpretive phenomenologists acknowledge that the meaning of a phenomenon is always constructed by the researcher in collaboration with the participants, and that phenomena are always positioned within a historical, cultural, and social context [Citation15]. Interpretive phenomenology tries to reveal the hidden meanings and implications of the phenomena based on the interpretation of the participants’ narratives and the researcher’s reflexivity [Citation13]. We operationalized experiences as the appearance of the world to the individual, respecting individual differences and suspending judgments about what is real [Citation13]. Physical activity was defined as “people moving, acting and performing within culturally specific spaces and contexts, and influenced by a unique array of interests, emotions, ideas, instructions and relationships” [Citation16]. We collected first-person accounts of experiences related to being physically active with semi-structured interviews and analyzed the data with interpretative phenomenological analysis [Citation17]. In reporting this study, we followed the Standards for Reporting Qualitative Research [Citation18]. A completed reporting checklist is provided as Supplementary File A.
Ethics
We conducted this study in the context of a university medical center in the Netherlands with accreditation as a cardiothoracic surgical center specialized in the treatment of aortic dissections. The Radboud University Medical Center ethical committee (dossier number 2023-16155) judged that this study does not fall under the scope of the Dutch Medical Research Involving Human Subjects Act (WMO). General principles from the Declaration of Helsinki and Good Clinical Practice were followed [Citation19,Citation20]. Written informed consent was obtained from all participants prior to the interview. Participation was voluntary and could be ended at any time. Emotionally charged topics were discussed, such as fear, sexuality, and stress, with participants able to allow the interview to continue, pause, or end. Contact with the medical staff was possible when emotionally charged situations became intense or when serious symptoms were discussed that required medical follow-up.
Researcher characteristics and reflexivity
The study team consisted of three physical therapists (JB, PvdW, and NK) and three patient representatives (CvB, DK, and RP). JB was a junior researcher. PvdW and NK were senior researchers with experience in qualitative research. JB and NK worked as a hospital-based physical therapists providing care to individuals with an uncomplicated type B aortic dissection. None of the study participants were treated by one of the authors. CvB, DK, and RP are board members of the Stichting Aortadissectie Nederland (English: The Netherlands Aortic Dissection Foundation). They made their network available for recruitment; however, they did not function as recruiters. CvB had an uncomplicated type B aortic dissection years ago, DK a type A and type B aortic dissection, and RP a type A aortic dissection. Before the start of the data collection and data analysis, JB and NK bracketed their thoughts in a written reflection report. The main topics in these reflection reports were presumed severe symptoms and movement anxiety while being physically active.
Sampling strategy
We used a convenience sampling strategy to sample information-rich cases [Citation13]. We started the recruitment of participants by distributing a poster about the study through social media channels and spreading flyers at the annual aortic dissection peers meeting. The poster and flyers included information about the study purpose, eligibility criteria, and an e-mail address for study participation application. Eligibility criteria were: diagnosed with an uncomplicated type B aortic dissection (no previous surgery and not waiting for surgery); aged 18 years or older; about one year after diagnosis of the aortic dissection or later; able to understand, read, and speak Dutch; and no history of dementia, delirium, or depression. In total, 18 potentially eligible participants responded. After screening of eligibility criteria, we recruited 14 participants. Reasons for not selecting four potential participants were less than one year since the diagnosis (n = 1, 10 months) and having both type A and type B dissection for which surgery had been performed (n = 3).
Data collection
First-person accounts of experiences were collected by JB between January and May 2023 using semi-structured interviews. The interviews followed a predefined interview guide (Supplementary File B). Topics were experiences related to being physically active, being physically active with an aortic dissection, and examples of daily activities, sports, exercises, and work. Probing questions were body experiences, time experiences, human relationships, knowledge, and support. As a conversation aid, we also used a seven-day-diary about being physically active which participants were asked to complete during seven days before the interview (Supplementary File C). All interviews were performed in the home setting of the participant (n = 3) or via Microsoft Teams (n = 11) (Microsoft Teams 365, Microsoft Company, Albuquerque, NM). The interviews were recorded with a Digital Voice Recorder (Olympus WS-852, Olympus Corporation, Tokyo, Japan). The interviews were transcribed verbatim by JB and checked by NK. The audio recordings and transcripts formed the evidence base for data-analysis. All research data were stored in ATLAS.ti software (ATLAS.ti version 23, Scientific Software Development GmbH, Berlin, Germany). Participant characteristics were stored in Castor Electronic Data Capture and anonymized in all research files.
Data analysis
We performed the six-step interpretative phenomenological analysis as described by Smith and Fieldsend [Citation17]. In step 1, the audio-recordings and transcripts were listened to, read and re-read independently by JB and NK to get in touch with the data. In step 2, JB and NK made initial notes, line by line, highlighting experiences related to being physically active. The notes were written in first-person perspective and reflected the interpretation of the authors. However, JB and NK remained as close to the data as possible, by using words of the participants themselves. In step 3, initial notes were independently transferred into emergent themes by JB and NK while looking for the essential qualities of the experience. The emergent themes were reported in memos for each individual participant. In step 4, emergent themes were translated into case descriptions for each individual participant. These case descriptions linked emergent themes based on, among others, sequence, cause-and-effect relationships, or conceptual similarities. The case descriptions were checked by JB and NK for theoretical data saturation by marking overlap and newly obtained insights [Citation21]. In step 5, we repeated steps 1–4 for each individual participant. In step 6, the authors interpreted and translated patterns in the emergent themes during an online consensus meeting. Subsequently, written feedback was provided on the description of the themes by all authors. All patterns were translated into an understanding of the whole, answering the research question: “What are the experiences of individuals with an uncomplicated type B aortic dissection related to being physically active?”.
Trustworthiness
During the data collection and data-analysis, JB and NK bracketed their thoughts setting aside preconceptions. As a first step, we created broad interview topics and open-ended probing questions to follow the participants’ interests and concerns [Citation22]. As a second step, we wrote bracketing reports before starting the data-analysis [Citation13]. This contributed to interpretations that stayed closer to the data as displayed by the participants. The transcripts were analyzed in ATLAS.ti software supporting independent, open, and transparent data-analysis with an audit trail. The consensus meetings with patient representatives improved thoroughness of the data analysis and transferability to other settings. All quotes were backward–forward translated by a third party native English speaker. We performed no member checking and did not share findings with participants in accordance with interpretive phenomenological analysis methodology, because the process of being interviewed developed the participants’ thinking and their own interpretation of their experience.
Results
In total, 14 participants enrolled in the study and completed the interview. The sample consisted of 11 male and 3 female participants. The interviews had a mean duration of 46 min (minimum 39 min, maximum 53 min). The mean age of the participants was 58 years (minimum 41 years, maximum 73 years). Time since diagnosis of the type B aortic dissection was mean 4 years (minimum 1 year, maximum 9 years). Four participants had paid work and were working full-time, three participants had paid work and were in reintegration, six participants were unemployed, and one participant’s employment status was unknown.
Patterns
We found three patterns in the data by which participants expressed what it is like to be physically active with an uncomplicated type B aortic dissection. First, participants told us that they were losing confidence in their body. For example, a participant said: “It felt like I could not rely 100% on my body anymore” [participant 420]. Second, participants indicated that confidence in their body was regaining with expressions such as: “I had to regain confidence in my body. I was trying to move, however, without risking too much” [participant 663]. Third, participants told us that they were continuing to build confidence in their body. For example, a participant told: “I was gaining experiences and continuing to build confidence in my body by trial-and-error” [participant 106]. An overview of the patterns and emergent themes is presented in .
Figure 1. Patterns and emergent themes reflecting how it is like to be physically active with an uncomplicated type B aortic dissection.
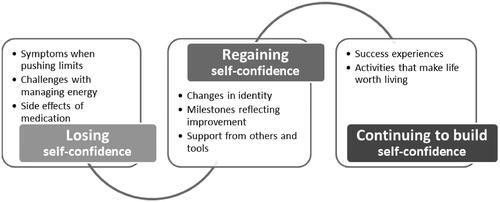
Losing self-confidence
Participants talked about experiencing symptoms while being physically active. The symptoms were particularly pronounced when pushing limits. They had symptoms such as pain between the shoulder blades, low back pain, dyspnea, shortness of breath, and extreme acidification of the upper legs. These symptoms had appeared suddenly during or after the aortic dissection. During their hospital stay and in the first weeks after returning home, participants experienced total energy loss and a feeling of having to start from nothing. Sometimes, experiencing symptoms evoked memories of the traumatic event, specifically, the acute onset of the aortic dissection symptoms. In addition, participants experienced uncertainty and anxiety while struggling to distinguish symptoms between a new onset of aortic dissection symptoms and a medically stable type B aortic dissection. The symptoms also sometimes lead to intrusive thoughts about death and mortality.
And then, yeah, I don’t know what’s happening to me, actually. And yeah, that’s psychologically difficult because, well, I lost my confidence. I’m aware that something just happened to me and apparently my life has changed. But what is my limit? And what can I still do and what can’t I do? I went dizzy when I was pushing my limits… So, then I realized: ‘Hey, it will take time to recover’. [participant 908, 40–50 years, 2–5 years since diagnosis]
Yes, fear of dying (emotional, trembling voice). I had that very much in the beginning. Because my body has failed me. Every time I feel the pain between my shoulder blades it reminds me of my mortality. [participant 663, 70–80 years, 2–5 years since diagnosis]
The challenges with managing energy were very frustrating according to participants. They told that day-to-day being tired and having energy were hard to predict. Sometimes it was possible to vacuum clean the entire house without getting exhausted. At other times, it was only possible to vacuum clean for only five minutes followed by sudden extreme exhaustion. Having energy could depend on activities the day before; however, there were also bad days suffering from fatigue without reason. Having energy went with ups and downs which was sometimes experienced as desponding or maddening. Participants reported that the challenge of managing energy made it difficult to plan activities, make appointments, and take responsibility at work. It was often necessary to take an after-lunch break to be able to manage the rest of the day.
My world got smaller after the aortic dissection. I actually have a harder time managing my energy throughout the day, uhm, and I notice that I have the energy…. Actually, if I spend a lot of energy today, I must pay for that tomorrow. […] I often did have dinner with friends and things like that, so yes, now I cancel things like that. I’ve cancelled performances, well, that’s the last thing I cancel. Because that’s very important to me. The other day I did go to a friend’s house for dinner, and the day after I had to pay for it. I was in terrible pain. I didn’t sleep all night. So yes, that just sucks. [participant 609, 60–70 years, 1–2 years since diagnosis]
Participants experienced severe side effects of medication that revealed themselves while being physically active. For example, they spoke of dizziness and lightheadedness, especially if they had to bend over or kneel. Participants specifically talked about the consequences of using beta blockers. Use of this medication led to, among others, waking up in the morning with general “lameness” [participant 273], upper leg muscles acidification when walking uphill, shortness of breath when climbing stairs, and decreased desire for sexual intercourse. The medication created a low limit in terms of exercise tolerance, making it impossible to enjoy exercising.
And uhm, and well, I feel myself very limited, particularly in fitness. I attribute that to medication, particularly the large number of beta-blockers that I use. I’m, of course, tired very quickly. Before I had the aortic dissection, I could run 10 kilometers, I actually did that the day before… Funny [participant being ironic]. And yes, running won’t happen anymore. [participant 106, 50–60 years, 5–10 years since diagnosis]
Well, I notice that I’m out of breath very quickly. I, uh, blame that myself mostly to using beta-blockers. Uhm, and I, yes, I’m just really an old, uhm an old person when I walk or climb the stairs, or when I’ve cycled. Uhm, yes, and after every activity, every bit of exercise, I really did have to recover to catch my breath again. So, I stopped exercising. [participant 951, 40–50 years, 2–5 years since diagnosis]
Regaining self-confidence
Participants said that there were changes in their identity after the aortic dissection. For example, they told us that they exercised competitively prior to the aortic dissection. Wanting to win and “going all the way to the limit and beyond” [participant 908] was part of the identity of some participants. While living with an aortic dissection, sports were more about taking part and enjoying good times together. As a result, their identity shifted from competitive athlete to recreational athlete and the motto became “participating is more important than winning” [participant 106]. Other identity changes were expressed in remarks such as “I’m no longer able to be the mother who I was” [participant 663] and “I’m not the hard worker anymore, now I’m the one cutting corners” [participant 63]. The process of changing an identity was described by participants with terms such as “a constant struggle with myself” [participant 393]. While dealing with the struggle, participants realized they needed to regain self-confidence by creating new expectations, new priorities, and accepting the new situation.
Yeah, before dissection, back then, I didn’t have to think about anything. Then I’d go exercise and I’d just go all the way. Now, I exercise just to be busy. I used to exercise until or over the limit, and now, I just exercise to be busy and just enjoy, yeah, just calm, and easy exercising. That’s, that’s the biggest difference, I think. [participant 407, 60–70 years, 2–5 years since diagnosis]
Self-confidence was also regained by achieving milestones reflecting improvement. In the beginning, even taking a small step and “a few feet more than yesterday” [participant 393] were considered milestones of progress by participants, which brought back confidence. Having more energy left over after walking, cycling, or working were also important milestones that confirmed progress for participants. On the one hand, failure to make progress could drive participants to despair, resulting in a decreasing self-confidence. On the other hand, there was increasing self-confidence if there was progress by achieving milestones, even if it was minimal progress.
That there was no progress, when once there was [progress]. Yes, yes, especially in the beginning. That did make me despair for a while. [participant 420, 60–70 years, 2–5 years since diagnosis]
No, but it goes like this… Yes, it’s slowly improving. And well, I’m actually, well, happy with that, let me put it this way. I’m confident if I keep achieving important milestones. [participant 393, 70–80 years, 2–5 years since diagnosis]
Participants also talked about support of others and tools that helped regaining confidence of the body. The need to ask for help from others could cause them to feel like being a burden to others. Participants felt guilt toward their partners when they paused on the couch instead of being busy in the household. Partners expressing gratitude for household achievements helped them regain self-confidence. Participants reported that compliments about their performance “restored the feeling that my body could do something for the family again” [participant 907]. In addition, they felt supported when employers were understanding of their medical conditions and helped them re-start paid work activities. However, participants did note that, over time, people in the work environment could not always support life-long restrictions which sometimes led to misunderstanding or shifting jobs. Furthermore, support of tools, such as e-bikes and walkers, helped them to do things that were not possible until recently. By using tools and noticing that it was safe, it became possible to be increasingly physically active, and, while doing, restore self-confidence.
Yeah, in the beginning, I couldn’t do anything, but eventually I started moving a little bit and I just started riding the regular bike. I found that it was very stressful, because after my aortic dissection I never took the bike again because I uhm, arrived everywhere heavily sweaty and totally exhausted. Yeah, it didn’t make me feel good. Uhm so that’s why I, I think after a year or so, I bought an electric bike and that’s why I started cycling a lot again. So that did give me more safety and freedom. [participant 951, 40–50 years, 2–5 years since diagnosis]
Continuing to build self-confidence
Participants talked about their success experiences over the years while living with an uncomplicated type B aortic dissection. For example, they noticed that they were able to push limits increasingly, often with fewer complaints over time. As a result, the fear of having another aortic dissection wore off over the years. Some participants told us that they consciously tried to push limits related to exercise tolerance, continuing to build their self-confidence. Others built their confidence by accepting what they could and repeating it regularly. Through success experiences, participants envisioned a future with fewer limitations and more happiness.
Respondent: The doctor at the time said to me ‘you should never bench press and heavy lifting’. And I asked, ‘what is heavy lifting?’ He said, ‘lifting a 10-liter bucket is too heavy’. But yes, I sometimes lifted two 10-liter buckets. But I thought it’s different when they’re just hanging than when you hold them straight in front of you, right?
Interviewer: Hmm, and when you first lifted the buckets, what was that like for you? With the doctor’s advice in mind?
Respondent: Yes, I, if you… At first, I thought ‘if there’s 11 liters in a bucket, I’m definitely going to die or something’. But no, yeah, I did that twice and then I noticed that I’m fine.
[…]
Interviewer: Yeah, yeah, and then what, what did that do to your body? Obviously, it’s been a while, but can you remember, what that, what that did to your body?
Respondent: Well, I just thought by myself ‘uhm, yeah, what could happen if I do that’? And meanwhile within a month I found out that nothing happens. And after six months, I thought ‘what doesn’t kill you makes you stronger’, right? [participant 273, 40–50 years, 1–2 years since diagnosis]
Participants emphasized that they were doing their best to find activities that make life worth living. By focusing on the positive things in life, they were more able to experience a fulfilling life and appreciate it, despite their limitations and symptoms. They talked about being more conscious about “the important things in life” [participant 106], such as enjoying time with family, since their aortic dissection. Singing in a band, hiking in nature, playing sports at the club, walking the dog, shopping in a city center, and cycling to work were also activities they now appreciated more compared to prior to the aortic dissection.
And since the aortic dissection, I still must keep doing my thing. What I do for a living and doing things with my family, well, those are the things I enjoy even more consciously. [participant 908, 40–50 years, 2–5 years since diagnosis]
Yes, when that [singing] works, then I get energy again. Yeah, like, then I get a kind of flow, uhm, that’s just nice when it’s all going well, and you sing nicely. Yeah, wonderful then I start floating, I can really enjoy that a lot more now. [participant 609, 60–70 years, 1–2 years since diagnosis]
Discussion
The purpose of this study was to gain a comprehensive understanding of experiences related to being physically active in adults with an uncomplicated type B aortic dissection. We found that it is no longer normal for the adults to be physically active as, since the diagnosis of the type B aortic dissection, their experiences related to physical activity level have been dramatically changed. The participants lost, regained, and continued to build self-confidence while being physically active. This is a process that takes months for some participants, and years for others. We have heard participants talking about coping strategies for, finally, being able to build self-confidence related to physical activity, such as: accepting that there are risks involved with being physically active; recognizing that without being physically active, there is no quality of life, and therefore it is necessary to be physically active; and exploring and pushing the limits of exercise tolerance by being physically active.
Self-confidence in relation to physical activity seemed to change over time. Self-confidence is, according to the Cambridge Dictionary, “the belief that you can do things well and that other people respect you”. The participants in our study were first uncertain about doing things well, mainly as the result of symptoms when pushing limits, challenges with managing energy, and side effects of medication. However, by trial-and-error and achieving milestones reflecting improvement, the participants experienced that daily activities could be done well. The significance of receiving support from others cannot be overstated, as it fosters respect from others. Self-confidence is, in this context, closely related to self-efficacy. Self-efficacy is “the perception or judgment of being able to accomplish a specific goal” [Citation23]. In patients with heart failure, self-efficacy is thoroughly studied and an important contributor to quality of life [Citation24]. Therefore, the International ACCF/AHA Guideline states that it is necessary to pay attention to self-efficacy and other psychological dimensions of patients [Citation25]. Self-confidence related to being physically active may be a crucial psychological dimension to improve quality of life in patients with an uncomplicated, conservatively managed, type B aortic dissection.
Comparing the current findings with earlier research is challenging due to the lack of research related to this topic. Feng et al. however, provide information about the exercise behavior of adults after surgery for an aortic dissection [Citation26]. Like our findings, the authors state that participants experience risks related to being physically active, and that dealing with risks became increasingly easier in later stages. Their study shows experiences that indicate lost self-confidence.
Before I was sent to hospital, I felt severe pain in my chest and back, and a sense of dying. Although the operation had been done, I still felt very painful. The doctor told me to get out of bed and walk around, but I didn’t dare. This was a feeling I had never felt before. [participant 5 [Citation26]]
Lee et al. show the needs of adults with or at risk for aortic dissection [Citation27]. The authors report that participants were grappling with mortality. In the beginning, there is a relief yet to live, followed by the realization that thoughts about mortality are forever part of daily life. The unpredictable nature of complaints after an aortic dissection is provided as the most important reason by participants for grappling with mortality. This is an experience that resonates strongly with our participants, who are reminded of their morality by symptoms while being physically active.
I think about dying every day and it totally impacts everything I do in terms of my work productivity, what I choose to do with my life, where I choose to live, how I think about my future, whether I live in a place that has good cardiological care. [participant 550 [Citation27]]
It is interesting to note that recommendations for increasing physical activity in patients suffering from thoracic aortic dissection are evolving. For instance, in surgically managed patients with thoracic aortic dissection, Schwaab et al. recommend initiating exercise-based cardiac rehabilitation [Citation28]. The recommendations in this study are limited to patients with surgically controlled thoracic aortic dissection; therefore, caution should be exercised when extrapolating the recommendations to patients with conservatively managed thoracic aortic dissection. However, increasing physical activity to preserve quality of life while balancing an increased risk of symptoms or new aortic dissection is still matter of debate [Citation29].
Strengths and limitations
An important strength of this study is the collaboration with patient representatives of the Stichting Aortadissectie Nederland. Their involvement increases the trustworthiness of our findings by mutual selection of relevant interview topics, joint interpretation of the data, and collaborative reporting of findings. Another strength is the theoretical data saturation which we achieved. After 12 interviews, we found no new patterns in the data. The patterns are grounded in data from all participants, providing compelling evidence that self-confidence is the central phenomenon related to being physically active with an uncomplicated type B aortic dissection.
A limitation of this study is the convenience sample. We did not purposively search for deviant or negative cases; therefore, it is possible that not all perspectives are represented [Citation13]. Nonetheless, the sample (n = 14) is sufficient according to recommendations for phenomenological studies (n = 9–17), and theoretical data saturation was reached [Citation30]. Another limitation is the transferability of the findings. All data were collected in Dutch adults with an uncomplicated type B aortic dissection. It is not known to which extent these experiences may differ from, for example, adults of non-Western origin or living in other countries.
Implications
Adults with an uncomplicated, conservatively managed, type B aortic dissection, ultimately, want to build self-confidence related to being physically active. The focus of rehabilitation professionals on physical activity and exercises should not come at the expense of focusing on psychological dimensions, such as self-confidence and self-efficacy. Patients need to belief that they are doing things well and they are respected by others. To achieve this, rehabilitation professionals should mark important milestones reflecting improvement and involve significant others, such as family, close-relatives, and peers. In addition, the adults want to hear from rehabilitation professionals what is possible (recommendations) rather than what is not allowed (rules). Recommendations provide more guidance and can be provided as mobilization milestones, supporting adults to achieve success experiences. In addition, it seems important to provide rehabilitation so that adults with an uncomplicated type B aortic dissection can explore, push, and accept their exercise limits. Supervised exercise-based cardiac rehabilitation might be crucial because a balance must be found between blood pressure regulation and quality of life. Exercise-based cardiac rehabilitation is safe for people after thoracic aortic surgery [Citation31], and, with modification of some principles, also seems to be beneficial for patients with an uncomplicated type B aortic dissection.
Conclusions
Adults with an uncomplicated type B aortic dissection experience that their self-confidence related to being physically active changes immediately after the diagnosis of the aortic dissection. The participants talked about months or years during which they first lose, then regain, and lastly build self-confidence related to physical activity. Supportive coping strategies, according to the participants, are accepting risks, recognizing the necessity of physical activity, and exploring exercise limits. Rehabilitation professionals should support adults regaining and continuing to build self-confidence with exercise-based cardiac rehabilitation. These programs provide opportunities for patients to find the perfect balance between blood pressure regulation, quality of life, and being physically active. It may be tempting for rehabilitation professionals to keep safe margins and opt for a strict blood pressure regulation; however, this should not be exaggerated at the expense of quality of life and exercise tolerance.
Supplemental Material
Download Zip (47.6 KB)Acknowledgements
First, we would like to thank all patients who took part in this study. Second, we thank Dr. M.F. Pisters for support during the study conceptualization and Prof. Dr. C. Veenhof for providing feedback on drafts of the manuscript. Third and last, we would like to thank R. Stekelenburg and S. Peters for providing feedback on drafts of the manuscript and improving data collection methods. We thank Tiptop Global for forward and backward translation of the quotes and In’to Languages for the text editing of our manuscript and recommendations. We acknowledge the use of Chat GPT-4o to translate the interview guide and diary from Dutch to English (supplementary File B and C).
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Data are available from the corresponding author upon reasonable request.
Additional information
Funding
References
- Erbel R, Aboyans V, Boileau C, et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J. 2014;35(41):2873–2926. doi: 10.1093/eurheartj/ehu281.
- Gouveia e Melo R, Mourão M, Caldeira D, et al. A systematic review and meta-analysis of the incidence of acute aortic dissections in population-based studies. J Vasc Surg. 2022;75(2):709–720. doi: 10.1016/j.jvs.2021.08.080.
- Daily PO, Trueblood HW, Stinson EB, et al. Management of acute aortic dissections. Ann Thorac Surg. 1970;10(3):237–247. doi: 10.1016/s0003-4975(10)65594-4.
- MacGillivray TE, Gleason TG, Patel HJ, et al. The Society of Thoracic Surgeons/American Association for thoracic surgery clinical practice guidelines on the management of type B aortic dissection. Ann Thorac Surg. 2022;113(4):1073–1092. doi: 10.1016/j.athoracsur.2021.11.002.
- Munshi B, Ritter JC, Doyle BJ, et al. Management of acute type B aortic dissection. ANZ J Surg. 2020;90(12):2425–2433. doi: 10.1111/ans.16270.
- Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the diagnosis and management of patients with thoracic aortic disease. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. J Am Coll Cardiol. 2010;55(14):e27–e129. doi: 10.1016/j.jacc.2010.02.015.
- Meccanici F, Thijssen CGE, Gökalp AL, et al. Long term health-related quality of life after acute type B aortic dissection: a cross-sectional survey study. Eur J Vasc Endovasc Surg. 2023;66(3):332–341. doi: 10.1016/j.ejvs.2023.05.037.
- Winnerkvist A, Brorsson B, Rådegran K. Quality of life in patients with chronic type B aortic dissection. Eur J Vasc Endovasc Surg. 2006;32(1):34–37. doi: 10.1016/j.ejvs.2005.12.010.
- Patel AY, Eagle KA, Vaishnava P. Acute type B aortic dissection: insights from the International Registry of Acute Aortic Dissection. Ann Cardiothorac Surg. 2014;3(4):368–374. doi: 10.3978/j.issn.2225-319X.2014.07.06.
- Ilonzo N, Taubenfeld E, Yousif MD, et al. The mental health impact of aortic dissection. Semin Vasc Surg. 2022;35(1):88–99. doi: 10.1053/j.semvascsurg.2022.02.005.
- Smit B, Onwuegbuzie AJ. Observations in qualitative inquiry: when what you see is not what you see. Los Angeles (CA): SAGE Publications; 2018. p. 1609406918816766.
- Finlay L. Exploring lived experience: principles and practice of phenomenological research. Int J Ther Rehabil. 2009;16(9):474–481. doi: 10.12968/ijtr.2009.16.9.43765.
- Husserl E, Alston WP, Nakhnikian G. The idea of phenomenology. The Hague: Nijhoff; 1964. p. 13–21.
- Heidegger M. The basic problems of phenomenology. Vol. 478. Bloomington: Indiana University Press; 1988.
- Tuohy D, Cooney A, Dowling M, et al. An overview of interpretive phenomenology as a research methodology. Nurse Res. 2013;20(6):17–20. doi: 10.7748/nr2013.07.20.6.17.e315.
- Piggin J. What is physical activity? A holistic definition for teachers, researchers and policy makers. Front Sports Act Living. 2020;2:72. doi: 10.3389/fspor.2020.00072.
- Smith JA, Fieldsend M. Interpretative phenomenological analysis. Washington (DC): American Psychological Association; 2021.
- O’Brien BC, Harris IB, Beckman TJ, et al. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi: 10.1097/ACM.0000000000000388.
- Grimes DA, Hubacher D, Nanda K, et al. The good clinical practice guideline: a bronze standard for clinical research. Lancet. 2005;366(9480):172–174. doi: 10.1016/S0140-6736(05)66875-4.
- World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi: 10.1001/jama.2013.281053.
- Walker JL. The use of saturation in qualitative research. Can J Cardiovasc Nurs. 2012;22(2):37–46.
- Chan ZC, Fung Y-L, Chien W-T. Bracketing in phenomenology: only undertaken in the data collection and analysis process. Qual Rep. 2013;18(30):1–9.
- Zulkosky K. Self‐efficacy: a concept analysis. Nursing forum. New York City: Wiley Online Library; 2009.
- Moradi M, Daneshi F, Behzadmehr R, et al. Quality of life of chronic heart failure patients: a systematic review and meta-analysis. Heart Fail Rev. 2020;25(6):993–1006. doi: 10.1007/s10741-019-09890-2.
- Heidenreich PA, Bozkurt B, Aguilar D, et al. ACC/AHA/HFSA guideline for the management of heart failure. J Card Fail. 2022;28(5):e1–e167. doi: 10.1016/j.cardfail.2022.02.010.
- Feng D, Huang S, Lang X. Attitudes and behavioral intentions of aortic dissection survivors towards exercise: an application of the health action process approach framework. Rev Cardiovasc Med. 2022;23(2):64. doi: 10.31083/j.rcm2302064.
- Lee JR, Segal C, Howitt J, et al. Lived experiences of people with or at risk for aortic dissection: a qualitative assessment. Semin Vasc Surg. 2022;35(1):78–87. doi: 10.1053/j.semvascsurg.2022.02.008.
- Schwaab B, Rauch B, Völler H, et al. Beyond randomised studies: recommendations for cardiac rehabilitation following repair of thoracic aortic aneurysm or dissection. Eur J Prev Cardiol. 2022;28(17):e17–e19. doi: 10.1177/2047487320936782.
- Spanos K, Tsilimparis N, Kölbel T. Exercise after aortic dissection: to run or not to run. Eur J Vasc Endovasc Surg. 2018;55(6):755–756. doi: 10.1016/j.ejvs.2018.03.009.
- Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2022;292:114523. doi: 10.1016/j.socscimed.2021.114523.
- Koenders N, van Zetten H, Smulders M, et al. Outcomes after cardiac rehabilitation in patients following repair of thoracic aortic aneurysm or dissection: a protocol for a systematic review and meta-analysis. Syst Rev. 2023;12(1):16. doi: 10.1186/s13643-023-02180-x.