
ABSTRACT
Autobiographical memory specificity (AMS) reduces with increasing age and is associated with depression, social problem-solving and functional limitations. However, ability to switch between general and specific, as well as between positive and negative retrieval, may be more important for the strategic use of autobiographical information in everyday life. Ability to switch between retrieval modes is likely to rely on aspects of executive function. We propose that age-related deficits in cognitive flexibility impair AMS, but the “positivity effect” protects positively valenced memories from impaired specificity. A training programme to improve the ability to flexibly retrieve different types of memories in depressed adults (MemFlex) was examined in non-depressed older adults to determine effects on AMS, valence and the executive functions underlying cognitive flexibility. Thirty-nine participants aged 70+ (MemFlex, n = 20; control, n = 19) took part. AMS and the inhibition aspect of executive function improved in both groups, suggesting these abilities are amenable to change, although not differentially affected by this type of training. Lower baseline inhibition scores correlated with increased negative, but not positive AMS, suggesting that positive AMS is an automatic process in older adults. Changes in AMS correlated with changes in social problem-solving, emphasising the usefulness of AMs in a social environment.
Background
Autobiographical memory (AM) refers to the recollection of events from across one’s lifespan and is thought to be central to social and emotional well-being in older adults. For example, Alea and Bluck (Citation2003) suggested that AM is integral to social functions such as intimacy, empathy and teaching or informing others. However, evidence indicates that many older adults have difficulty strategically recalling detailed memories of specific events (e.g., “The first day I drove a car by myself”) and instead recall general memories (e.g., “Having driving lessons as a teenager”), which has been linked to age-related decline in executive function (Holland, Ridout, Geraghty, & Walford, Citation2012; Ros, Latorre, & Serrano, Citation2010). This is important because poor autobiographical memory specificity (AMS) is a risk factor for depression (Sumner, Griffith, & Mineka, Citation2010) and is associated with loss of independence in older adults. For example, it is evidenced as a predictor of reduced functional limitations, specifically in the domain of communication (Holland et al., Citation2017). This relationship between AMS and the extent to which one’s health impacts on the ability to communicate with others may be explained by the use of AM in conversations with new people, for example, discussing shared preferences or experiences. Reduced retrieval of specific AMs has also been related to poorer social problem-solving ability (Goddard, Dritschel, & Burton, Citation1996), since recollection of more detailed information from the past is used to simulate more effective hypothetical solutions to problems.
On the other hand, higher AMS has a protective effect on mental health in non-depressed older adults (Latorre et al., Citation2013) and is associated with better social problem-solving ability (Beaman, Pushkar, Etezadi, Bye, & Conway, Citation2007). Therefore, reducing over-general memory (OGM) has been a target for memory-based interventions in older adults (e.g., Leahy, Ridout, Mushtaq, & Holland, Citation2017). However, Dritschel, Beltsos, and McClintock (Citation2013) argued that the ability to be flexible in the retrieval of specific and general memories under different circumstances may be more important than specificity for successful functioning in everyday life. Furthermore, they argued that memory flexibility could underpin important functions such as emotion regulation, for example, for up-regulating positive memories or for shifting sets, i.e., disengaging rumination on negative memories, which also has implications for mental well-being.
Maintaining mental well-being and social functioning in older adults is essential as depression and social isolation, which are common in this population (Campos et al., Citation2016; Djernes, Citation2006), have been implicated as risk factors for dementia (Bennett, Schneider, Tang, Arnold, & Wilson, Citation2006; Da Silva, Gonçalves-Pereira, Xavier, & Mukaetova-Ladinska, Citation2013). On the other hand, having a large social network has been found to reduce the manifestation of cognitive impairment, despite the presence of Alzheimer’s disease pathology (Bennett et al., Citation2006). Social functioning could therefore be an important target for cognitive ageing interventions, as it enables people to benefit from taking part in stimulating and sociable activities. Interventions that lead to improved AMS have been shown to reduce depression in younger adults (Raes, Williams, & Hermans, Citation2009) and to enhance social functioning in older adults, notably social problem-solving (Beaman et al., Citation2007; Leahy et al., Citation2017). Given the proposed importance of flexible AM retrieval for everyday functioning (Dritschel et al., Citation2013), particularly in relation to mood regulation, interventions to improve this function could be particularly beneficial for older adults.
Cognitive flexibility and AM retrieval
Older adults often face uncertain circumstances, for example, bereavement, moving home or retirement, which may adversely affect their well-being. The ability to quickly recover from challenges experienced in everyday life, often referred to as resilience, is an important factor in healthy ageing. Such resilience requires flexibility to be able to adapt to a changing environment. Flexibility is important to psychological well-being, but is a wide concept that can refer to a range of different processes. In a review, Kashdan and Rottenberg (Citation2010) highlight the process of flexibility in relation to executive function. According to Miyake et al. (Citation2000), executive functions consist of three factors: shifting, updating and inhibition. The use of these abilities to recognise and update the requirements of a specific situation and adapt to changes in demand is integral to being flexible (Kashdan & Rottenberg, Citation2010). This specific use of executive control will be referred to as “cognitive flexibility” within this paper.
Inhibition and initiation are key processes embedded within cognitive flexibility since previous habitual or automatic responses are inhibited and novel search strategies are initiated (Dritschel et al., Citation2013; Eslinger & Grattan, Citation1993). These processes are also required for verbal fluency tasks whereby participants must search for new categories of words. Cognitive flexibility has therefore been measured using verbal fluency tasks (Heeren, Van Broeck, & Philippot, Citation2009) and the Random Number Generation task (RNG; Towse & Neil, Citation1998) which requires inhibition of automatic responses and initiation of novel responses. Furthermore, this process is analogous to the hierarchical model of AM retrieval, as general memories must be inhibited and a search for more remote specific episodic details must be initiated (Conway & Pleydell-Pearce, Citation2000). Therefore, reduced flexibility may result in perseveration on general memories, and a difficulty overcoming this to access specific memories. As such, we propose that cognitive flexibility is an integral component to the retrieval of specific AMs in this hierarchical manner.
Evidence from the depression literature supports the suggestion that cognitive flexibility underlies AMS. For example, Dalgleish et al. (Citation2007) demonstrated that depression is related to an impaired ability to inhibit automatic responses, resulting in perseveration on previous rules or habitual responses. Williams and Dritschel (as cited in Heeren et al., Citation2009) also found that OGM was negatively correlated with a cognitive flexibility task (verbal fluency). Both OGM and cognitive inflexibility are integral features of depression in younger adults (Dalgleish et al., Citation2007; Grant, Thase, & Sweeney, Citation2001). Furthermore, a previous intervention study using Mindfulness-Based Cognitive Therapy with healthy adults found that improvement in cognitive flexibility (measured via a verbal fluency task) facilitated a reduction in OGM retrieval (Heeren et al., Citation2009). The authors explain this by suggesting that cognitive flexibility is required for mindfulness training to shift the focus of attention to different objects, for example, to disengage from intrusive thoughts and focus on breathing or bodily sensations. This is similar to how attention is disengaged from general memories, which capture attention automatically, towards more specific, episodic information. Therefore the authors concluded that an OGM bias may reduce if cognitive flexibility is increased.
Dritschel et al. (Citation2013) developed a measure of AM flexibility with non-depressed university students – the Autobiographical Memory Test-Alternating Instructions (AMT-AI), whereby participants had to switch between retrieving general and specific memories. Perseveration on general memories in the switching task impacted ability to retrieve specific memories in particular, whilst general retrieval was relatively unimpaired. Furthermore, only specific retrieval was negatively correlated with depressive symptomatology and rumination. This is important as it suggests flexibility particularly impairs specific retrieval and may be an important factor for interventions for people who may be vulnerable to developing depression, but whose symptoms are not currently clinically significant. However, the authors did not include a non-memory measure of cognitive flexibility meaning it is unclear whether difficulty in flexibly retrieving specific memories is related to a more general deficit in cognitive flexibility.
Older adults have been shown to exhibit age-related deficits in cognitive flexibility (measured by a number of perseverative errors on the Wisconsin Card Sorting Test; Taconnat et al., Citation2009). Thus, in addition to depression-related OGM, reduced cognitive flexibility may also explain age-related OGMs due to difficulty performing a controlled search. Given the link between cognitive flexibility and AMS, alongside evidence for reduced AMS and reduced cognitive flexibility in older adults, we aimed to examine if a novel intervention (Memory Flexibility programme [MemFlex]; Hitchcock et al., Citation2015), which targets flexibility within the domain of AM, would lead to improvements in AMS in older adults. Since flexibility in AM retrieval in relation to general cognitive flexibility has not yet been examined, our secondary aim was to examine the effects of MemFlex training on cognitive flexibility measured with a verbal fluency task, and on the executive functions that underlie cognitive flexibility, i.e., Updating and inhibition (measured using the RNG task). It is expected that if cognitive flexibility does underlie flexibility in AM retrieval, then the practice provided by MemFlex, for example, switching responses between alternating task instructions, would engage these cognitive functions and thus have an impact on performance in these skills. We expected that MemFlex would enhance older adults’ ability to perform a controlled retrieval search for specific memories via the route of improved cognitive flexibility. This may be more effective than only providing direct practice in specific recall as previous AM interventions in older adults have done (e.g., Leahy et al., Citation2017; Raes et al., Citation2009), since it is a targeted at a specific cognitive process underlying AM retrieval, as opposed to simply practising the task that is being measured (i.e., recalling specific memories in response to cue words).
Positivity effect
Cognitive flexibility may also be useful for increasing attentional control over bottom-up, automatic processes which are more likely to be guided by emotions, and is therefore particularly relevant to emotion regulation (Kashdan & Rottenberg, Citation2010). There is evidence that healthy older adults use cognitive control processes for emotion regulation to enhance positive memories and down-regulate negative memories (Mather & Knight, Citation2005). This results in biases in attentional and memory retrieval processes towards positive material in older adults, referred to as “the positivity effect” (Carstensen, Isaacowitz, & Charles, Citation1999; Mather & Carstensen, Citation2005). In support of this, in a previous AM training study, we found that older adults with poorer inhibitory control, thus less ability to regulate emotional material, benefitted most from recalling specific positive events (Leahy et al., Citation2017). However, Holland et al. (Citation2012) found that although the updating aspect of executive function predicts overall specificity in older adults, it does not predict specific positive recall, suggesting that specific positive recall is not influenced by the reduced executive control in older adults. Therefore the role of executive control in flexibility between positive and negative recall in older adults is unclear. One of the purposes of MemFlex in younger adults is to enhance flexibility between positive and negative memories, enhancing the ability to up-regulate positive memories when they are useful to the situation. In the current study, we will examine the effects of MemFlex on older adults’ ability to retrieve memories of the appropriate valence for emotion regulation. This will help to determine if the positivity effect protects from any detrimental impact of age-related reduced cognitive flexibility. We expected that since older adults are already successful at up-regulating positive recall, there would be limited effects on positive specific recall compared to negative specific recall. Furthermore, based on our previous findings (Leahy et al., Citation2017) and the combination of the evidence presented above for role of cognitive flexibility in specific retrieval, we expected that MemFlex would be particularly helpful for people with lower cognitive flexibility at baseline.
Aims and hypotheses
The current study aimed to examine the effects of MemFlex on cognitive flexibility and specific AM retrieval in non-depressed older adults. We firstly hypothesised that since cognitive flexibility is integral to the generative search process, participants in the MemFlex condition would exhibit significant improvements in cognitive flexibility (measured using a verbal fluency task), as well as the executive functions underlying this skill (i.e., Updating and inhibition), and in AMS, relative to controls. Previous AM training methods have been shown to have long-lasting effects on memory specificity (Moradi et al., Citation2014; Neshat Doost et al., Citation2014), therefore, we predicted that effects on primary outcomes would be maintained at 3-month follow-up in the MemFlex group. Changes in these two primary outcomes were expected to be positively correlated.
Due to the relationship between AMS and social problem-solving ability, independence and depression, we hypothesised that MemFlex participants would also exhibit improvements on these secondary outcome measures relative to controls, and that changes in these variables would be positively related to changes in AMS. We predicted these effects would also be maintained at 3-month follow-up since MemFlex is designed to help participants incorporate the skills learned into their everyday lives.
Based on evidence that older adults successfully use cognitive control processes to regulate emotion in line with the positivity effect (Mather & Carstensen, Citation2005), we hypothesised that there would be a bias towards recalling positive specific memories compared to negative specific memories across both groups. Since the “positivity effect” protects positive memories from impaired specificity because older adults are generally better at recalling positive material compared to negative (Kwon, Scheibe, Samanez-Larkin, Tsai, & Carstensen, Citation2009), we expected no effect on positive specific recall, but an increase in negative specific recall in MemFlex participants relative to controls, which would be related to improvement in cognitive flexibility. Training negative specific recall remains important since over-generalisation of negative memories (and reduced access to specific memories) can lead to depressive symptoms such as rumination (Hayes, Wilson, Gifford, Follette, & Strosahl, Citation1996; Raes et al., Citation2006). Furthermore, based on previous findings we hypothesised MemFlex would be particularly helpful for people with lower baseline cognitive flexibility.
\Lastly, the target population’s perceptions of an intervention in terms of how effective they find it to be, how appropriate it is in addressing the kind of difficulties they experience, and the practicality of taking part will ultimately determine adherence to an intervention and motivation to incorporate the skills learned into their everyday life. Therefore, through qualitative analysis of participants’ feedback, we aim to examine the acceptability of MemFlex to a non-depressed older adult population.
Methods
Participants
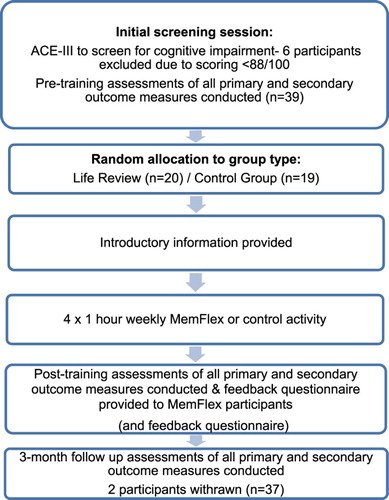
Thirty-nine independently living older adults (aged 70+) took part (MemFlex, n = 20; Control, n = 19). See for participant demographics. Participants were recruited via a panel of volunteers who had agreed to be contacted by the University about healthy ageing research and through advertisement in the community. Participants were excluded if they were aged <70 or had a diagnosis of a memory problem (including stroke, early dementia, or traumatic brain injury). Six participants who scored <88 on the Addenbrooke’s Cognitive Examination-III (ACE-III) cognitive assessment (Noone, Citation2015) were excluded due to potential cognitive impairment. One control group participant was uncontactable after the post-training follow-up. Another from the MemFlex group withdrew due to unrelated health problems before completing the 3-month follow-up (See for flow chart of the study procedure). Pre- and post-training data only for these two participants were included in the analysis, therefore the sample size at 3-month follow-up data was 37 (MemFlex = 19; Controls= 18). Participants who attended the University were reimbursed £7.50 per session for travel costs, and home visits were offered to include those who were less mobile or lived further from the University. Ethical approval was obtained from the University Ethics Committee, #709, with written informed consent being obtained from all participants.
Table 1. Participant demographics across group type.
Figure 1. Flow chart of study procedure.
Materials
Primary outcomes
Cognitive flexibility: The verbal fluency sub-score of ACE-III (Hsieh, Schubert, Hoon, Mioshi, & Hodges, Citation2013) measured the inhibition and initiation elements of cognitive flexibility, providing a combined phonemic and category fluency score (0–14). The RNG task (Towse & Neil, Citation1998) also provided a measure of cognitive flexibility. The task involved participants calling random numbers from 1 to 9 in time with a metronome set at 1 beat per second for 1 minute. It provides a redundancy (R) score of how frequently each digit occurred as a measure of updating ability, and two measures of inhibition; an RNG index of how frequently pairs or triplets of digits occurred and an adjacency (combined) score indicating the occurrence of sequences of digits. Lower scores on each indicated a higher level of randomness.
Autobiographical memory specificity: In the Autobiographical Memory Task (AMT; Dalgleish et al., Citation2007; Williams & Broadbent, Citation1986), 10 emotional cue words were read aloud and participants were asked to recall a specific memory in response to each. The same set of 10 cue words was used for all participants, with a different set being used at each time point (pre-training, post-training and 3-month follow-up). Five of the words were positive (e.g., delightful, bright, carefree, lively, reassured) and five were negative (e.g., tense, sorry, mistake, fault, clumsy), presented in an alternating order. A pilot study conducted with 12 undergraduate students found that the three sets of cue words (Set 1, M = 0.64, SD = 0.27; Set 2, M = 0.53, SD = 0.32; Set 3, M = 0.64, SD = 0.18) did not differ in terms of proportion of specific memories recalled, F(2, 20) = 0.49, p = 0.62, indicating that the words were matched in their potential to evoke a specific memory. Instructions were given to recall a memory of a specific event that lasted less than one day, and was on one particular occasion. Examples of correct (i.e., a specific memory) and incorrect responses (i.e., a non-specific memory) were given and participants completed a practice trial before beginning the task.
Audio recordings of participants’ responses were taken to be coded later. Memories of events that lasted less than a day and that occurred on one particular occasion were coded as specific. Memories that lasted longer than a day or were repeated events (e.g., “My holiday in Spain” or “Going to the beach”) were coded as over-general. If the type of memory recalled was unclear, or if the response was not a memory (e.g., it was an opinion related to the cue) participants were prompted (e.g., “Was that on one particular occasion?” or “Can you think of a memory in relation to that?”). The first rateable memory was scored as specific, general or if no memory was given the response was scored as omission. If the participant failed to respond within 1 minute, the response was also coded as omission. The total score was the proportion of specific memories retrieved out of all 10 cue words presented. Separate scores for positive and negative specific recall were also calculated by taking the proportion of specific memories recalled out of all five of each cue valence. A random sample of 60 memories (30 from the MemFlex group and 30 from the control) was rated by an independent rater who was blind to group type. Inter-rater reliability for specific vs general was calculated as Cohen’s Kappa (K) = 0.74 with a percentage agreement of 95%.
Secondary outcomes
Social problem-solving ability: In the Means End Problem-Solving Procedure (MEPS; Platt & Spivack, Citation1975) participants were asked to describe how they would solve a series of four hypothetical social problem scenarios. The problems included one’s partner leaving them after an argument, having difficulties with one’s boss, falling out with friends or moving to a new neighbourhood. Two measures obtained; the mean “number of relevant steps/means” taken to solve the problem and the mean “effectiveness” rating of the solution from 0 to 7, higher scores indicating better social problem-solving. To assess inter-rate reliability, a random sample of 48 problem solutions (24 from the MemFlex group and 24 from the controls) was rated by an independent rater who was blind to group type. The intra-class correlation coefficient was .74 for a number of relevant means, and .72 for effectiveness ratings.
Self-rated depression: The Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, Citation1983) provided 2 sub-scores: depression (0–21) and anxiety (0–21). The cut-off scores for each subscale are as follows; normal 0–7, mild 8–10, moderate 11–14 and severe 15–21 (Zigmond & Snaith, Citation1983).
Independence: The instrumental and basic activities of daily living scales (IADL, ADL) (Katz, Ford, Moskowitz, Jackson, & Jaffe, Citation1963; Lawton & Brody, Citation1969) provided total scores of independence (IADL; 0–8 and ADL; 0–6). The functional limitations profile (FLP; Pollard & Johnston, Citation2001) gave a total score (0–1150) and 10 sub-scores: walking and using stairs (0–126), body care or movement (0–124), mobility (0–114), household management (0–90), recreation (0–91), social (0–109), alertness (0–115), sleep (0–111), eating (0–143) and communication (0–127).
Interventions
Memory Flexibility programme (MemFlex) (Hitchcock et al., Citation2015)
Hitchcock et al.’s (Citation2015) MemFlex intervention in younger depressed adults aimed to reduce depressive symptoms by targeting maladaptive cognitive patterns, such as reduced cognitive flexibility and a bias towards negative material (Gotlib & Joormann, Citation2010; Williams et al., Citation2007). The programme is based on a combination of cognitive bias modification treatment, which aims to reduce attentional bias towards the negative material, and memory specificity training (MEST; Raes et al., Citation2009), which aims to improve specific memory recall through systematic practice. MemFlex has three main aims: (1) to balance between positive and negative memories in order to reduce cognitive bias; (2) to elaborate on positive memories to improve their quality and thus their use for emotion regulation; (3) to improve flexibility of memory retrieval, i.e., to selectively switch between general and specific, and positive and negative memories.
The MemFlex workbook activities in the current study were the same as those used by Hitchcock et al. (Citation2015), however, the wording was adapted for use with a non-depressed older adult population. For example, in information relating to depression, the word “depression” was replaced with the words “low mood” and the word “therapist” altered to “researcher”. The intervention consisted of a face-to-face introductory session with the researcher, followed by eight self-guided sessions which participants completed at home. In the introductory session, the researcher provided a brief outline of different memory systems (i.e., working memory, long-term memory and autobiographical specificity [AMS]) and how they are affected by ageing, age-related deficits in AMS, the relationship between AM and mood, and the importance of AM in everyday life. Examples were provided and participants were given a chance to practice to ensure they had understood before receiving the workbook to complete at home over 4 weeks. A diary sheet was provided at the start of the workbook to help participants plan the sessions around their schedule. The workbook was organised as per the protocol used by Hitchcock et al. (Citation2015). A summary of the tasks in each session is provided in (see Hitchcock et al., Citation2015 for a full description).
Table 2. Summary of the tasks in each session.
Control workbook
Participants in the control condition were similarly asked to complete a healthy ageing workbook at home over four weeks. This was to enable a comparison to the MemFlex workbook by providing information about healthy ageing, therefore promoting a positive lifestyle and maintaining well-being, but without specifically influencing memory retrieval. This is consistent with the protocol of Hitchcock et al. (Citation2015). As in this protocol, our control workbook also consisted of eight self-guided sessions (two per week). Each session of our healthy ageing book provided reading material (taken from www.ageuk.org.uk) about an age-related health topic (e.g., mental well-being, staying physically active, healthy eating) followed by a series of questions about the material, or activities related to the topic to ensure participant engagement. There was also a diary sheet to help schedule sessions, as in the MemFlex workbook.
Feedback questionnaire
An optional, anonymous feedback questionnaire was provided to MemFlex participants following the post-training session. The questionnaire consisted of seven open-ended questions about the training such as “Did you feel you benefitted in any way from taking part in the training programme, and if so, how?” The responses on the forms were analysed using the thematic analysis method suggested by Braun and Clarke (Citation2006) in order to analyse and interpret participants’ experiences of MemFlex.
Procedure
Pre-training assessments were conducted in an initial screening session. Following exclusion of participants who did not meet inclusion criteria, participants were randomly allocated between the MemFlex or control group. Random allocation to a condition was conducted in blocks using computer-generated random numbers. The ratio of participants allocated to a condition was adjusted to 2:1 (MemFlex: Control) in later blocks to balance group sizes as three participants from the MemFlex group had withdrawn before completing post-training, resulting in a disproportionate sample size compared to the control. Following random allocation, participants completed the intervention/control workbooks over the course of 4 weeks. In the week following the last intervention/control session, participants completed post-training assessments. The MemFlex group were also asked to complete the feedback questionnaire. Finally, all participants then completed a 3-month follow-up assessment. Those in the control group were offered the chance to complete an AM intervention workbook (based on MEST) at the end of the study.
Results
Participant characteristics
Independent t-tests on pre-training scores revealed no significant differences between groups in demographics (see ) or the following variables of interest: AMT scores; depression ratings; social problem-solving; or cognitive flexibility, p > 0.1 (see ). There was, however, a significant difference in total score on the FLP at baseline, t(37) = 2.96, p = 0.005, with more functional limitations in the MemFlex group than controls (see for means). Further comparisons between the FLP subscales revealed that the only two subscales where the groups differed were related to physical health; i.e., walking and using stairs (MemFlex, M = 40.5, SD = 34.14; Control, M = 17.05, SD = 27.61); t(37) = 2.35, p = 0.024, body care or movement (MemFlex, M = 48.2, SD = 33.05; Control, M = 18.68, SD = 32.85); t(37) = 2.8, p = 0.008. There were no significant differences between groups on any other FLP subscale, p > 0.05.
Table 3. Means and standard deviations of all relevant variables at pre-training, post-training and 3-month follow-up (*=p > 0.005).
Ceiling/floor effects
There were ceiling effects on the ADL and IADL measures, with 92.3% scoring equal to or above 5 out of 6 on the ADL measure, and 100% scoring 8 out of 8 on the IADL measure at baseline.
The lowest score on the FLP was 43 and the highest was 692, giving a range of 649. 71.8% scored below 324.5, which is the halfway point of this range.
A floor effect was observed with 61.5% of the sample scoring below 3 out of 21 on the HADS depression rating scale at baseline. None of the participants scored above the recommended cut-off for mild depression (8 out of 21; Zigmond & Snaith, Citation1983) at baseline, post-intervention or 3-month follow-up.
Adherence to intervention
As some of the workbook activities were left blank, the proportion of workbook sessions completed were calculated for each participant: MemFlex workbook, M = 0.85, SD = 0.23; control workbook, M= 0.97, SD = 0.12. An independent t-test revealed there was no significant difference between groups in the proportion of workbook completed, p > 0.05.
Primary outcomes
The proportion of specific memories recalled on the AMT (AMT-pS) and scores on the cognitive flexibility measures were analysed using 2 (MemFlex vs. Control) × 3 (Pre, Post, Follow-up) ANOVA in order to test the hypothesis that the MemFlex group would exhibit improvements in AMS and cognitive flexibility, relative to the control group.
Autobiographical memory specificity
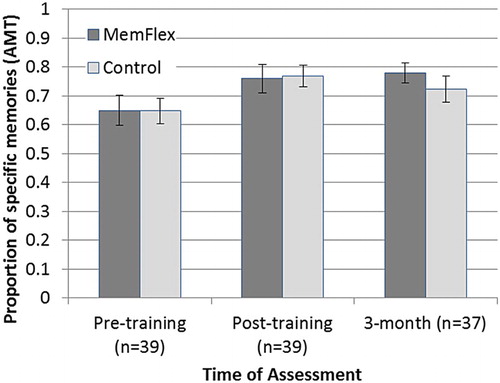
A significant main effect of time on AMT-pS showed that AMT scores improved over time regardless of group type, F(2, 70)= 6.42, p = 0.003, partial eta squared () = 0.16. A significant linear contrast was observed, F(1, 35) = 6.91, p = 0.013,
= 0.17, as well as a significant quadratic contrast F(1, 35) = 5.66, p = 0.023,
= 0.14. The mean values (see ) suggest that whilst AMT-pS increased linearly in the MemFlex group across the three time points, there was a curvilinear relationship in the control group with mean AMT-pS increasing at post-training, and decreasing slightly at the 3-month follow-up (). There was no significant interaction between time and group type, p > 0.1. The hypothesis that there would be an improvement in AMS in MemFlex participants relative to controls was thus unsupported.
Figure 2. Proportion of specific memories recalled at each time point in each group.
Cognitive flexibility
There were no significant main effects or interactions on the RNG index or the redundancy (R) score, p > 0.1. On the adjacency (combined) score there was a main effect of time, F(2, 70) = 6.86, p = 0.002,
= 0.16, with a significant linear contrast observed F(1, 35) = 10.77, p = 0.002,
= 0.24, showing that overall scores decreased (indicating an improvement) across time. However, there was no group × time interaction, p > 0.1. There were no significant group type × time interactions on the verbal fluency task, p > 0.1. The hypothesis that there would be improvements in these measures in MemFlex participants relative to controls was thus unsupported.
Relationship between changes in primary outcomes
Change scores were calculated for cognitive flexibility and AMT-pS by taking the difference between scores at 3-months and pre-training. Correlational analyses were performed in order to examine the hypothesis that changes in these two primary outcomes would be positively correlated. There was no correlation between change in any of the cognitive flexibility measures and change in AMS-pS, p > 0.1, thus the hypothesis was unsupported.
Positive vs. negative AMS
Repeated measures ANOVA showed no differences between the proportion of specific memories recalled for positive cues (AMT Positive-pS) and for negative cues (AMT Negative-pS) at any of the time points in the whole sample, p > 0.1, therefore the hypothesis that there would be a bias towards recalling positive specific memories compared to negative specific memories was unsupported.
Two 2 (MemFlex vs. Control) × 3 (Pre, Post, Follow-up) ANOVA were conducted with AMT Positive-pS and AMT Negative-pS as dependent variables separately in order to test the hypothesis that there would be an increase in negative specific recall in the MemFlex group relative to controls, but no effect on positive specific recall. There was a marginal effect of time on AMT positive-pS, F(2, 70) = 2.86, p = 0.064. Although the overall effect of time was not significant, there was a significant linear contrast, F(1, 35) = 4.37, p = 0.044,
= 0.11 showing that scores increased overall. However, there was no interaction with group type, p > 0.1. There was a significant effect of time on AMT Negative-pS, F(2, 70) = 6.37, p = 0.003,
= 0.15 with marginal linear, F(1, 35) = 4.02, p = 0.053,
= 0.1 and significant quadratic contrasts, F(1, 35) = 9.63, p = 0.004,
= 0.22. There was no interaction with group type, p > 0.1. The main effects of time support the hypothesis that there would be an increase in negative, but not positive specific recall. However, the lack of interaction with group type suggests this was a practice effect.
The mean values (see ) suggest that whilst AMT Negative-pS increased linearly in the MemFlex group and then remained stable there was a curvilinear relationship in the control group. Planned pairwise comparisons confirmed that there was a significant increase in AMT Negative-pS in the MemFlex group from pre-training to both post-training, t(19) = −3.56, p = 0.002, and 3-month follow-up t(18) = −2.7, p = 0.015. There was only a marginally significant increase from pre- to post-training in the control group, t(18) = −2.06, p = 0.054, but not from pre- to 3-month follow-up, p > 0.1. There were no significant increases in AMT Positive-pS in either group, p > 0.05. One-way ANOVAs showed no significant differences between the groups at pre-training, post-training or 3-month follow-up in either AMT Negative- or Positive-pS, p > 0.05. This provides some support for the hypothesis that there would be an increase in negative specific recall in the MemFlex group relative to controls, but no effect on positive specific recall.
Cognitive flexibility and changes in affective bias
Change scores for AMT Positive-pS AMT Negative-pS and cognitive flexibility measures were calculated by taking the difference between scores at 3-month and pre-training in order to examine the hypothesis that improvement in cognitive flexibility would be related to an increase in negative specific recall, but not in positive specific recall. Correlational analysis revealed no significant relationships between any change variables, p > 0.1, thus the hypothesised relationship between increase in negative specific recall and improvement in cognitive flexibility was unsupported.
Baseline cognitive flexibility and changes in AMS
Relationships between baseline cognitive flexibility measures and change scores for total AMT-pS, AMT Positive-pS and Negative-pS were examined in order to test the hypothesis that MemFlex would be particularly helpful for people with lower baseline cognitive flexibility. There were no relationships between these variables in the MemFlex group alone. Since there was a main effect of time in AMT-pS in the whole sample, we further examined these relationships with the whole sample. Adjacency (combined) score at pre-training was positively correlated with both overall change in AMT-pS, r = 0.34, p = 0.038, and change in AMT Negative-pS, r = 0.38, p = 0.019, but not change in AMT Positive-pS, p > 0.1. As reported earlier, there were significant improvements in overall AMT-pS and in AMT Negative-pS in the whole sample. This suggests that in the whole sample, people with the highest adjacency scores (i.e., lowest inhibition ability) had the biggest improvements in the recall of specific memories, particularly negative memories. This supports the hypothesis that lower baseline cognitive flexibility would be positively related to change in AMS, however, this was only true for negative memories.
Analysis of secondary outcomes
Mixed 2 (Group type; MemFlex vs. Control) × 3 (Time; Pre, Post, Follow-up) ANOVA were conducted separately with each of the secondary outcome measures as dependent variables in order to test the hypothesis that MemFlex participants would exhibit improvements on secondary outcome measures, relative to controls.
Social problem-solving
There were no significant main effects (p > 0.1) but there was a marginal group × time interaction in the number of means generated on the MEPS task, F(2, 70) = 2.88, p = 0.063, such that scores in the MemFlex group got worse from post-training to 3-month follow-up, t(18) = 2.11, p = 0.049, whilst scores in the control group did not, p > 0.1. There was a significant quadratic contrast for the interaction between time and group type, F(1, 35) = 8.43, p = 0.006. The mean values (see ) suggest that whilst MEPS number of means increased from pre-training to post-training, and decreased from post-training to 3-month follow-up in the MemFlex group, in the control group these scores decreased from pre-training to post-training, and then increased from post-training to 3-month follow-up. There were no main effects and no interactions on the effectiveness ratings on the MEPS task, p > 0.1.
Depression
There were no main effects or group × time interaction on HADS depression ratings, p > 0.1.
Independence
Since there was a group difference at pre-training in functional limitations, ANCOVA was conducted to examine group effects at post-training whilst controlling for pre-training scores on the FLP, however, there was no effect of group type, p > 0.1. There were no group × time interactions on any of the FLP subscales, or on the ADL or IADL measures.
Overall, the hypothesis that the MemFlex participants would exhibit improvements on secondary outcome measures relative to controls was unsupported.
Relationships between changes in AMS and secondary measures
Correlations were conducted to test the hypothesis that changes in secondary outcomes would be positively related to changes in AMS. There was a significant positive correlation between change in AMT-pS and change in MEPS number of means r = 0.39, p = 0.016, with change in AMS being positively related to change in social problem-solving ability. There were no other significant correlations between change in AMT-pS and change in any of the other variables, p > 0.05. However, after correcting for multiple comparisons using Bonferroni this was no longer significant.
Qualitative analysis of feedback questionnaire to assess acceptability
Four participants withdrew from the MemFlex condition due to difficulty understanding the workbook and completing the activities. One other participant who did complete the intervention commented on the feedback questionnaire that the language was difficult to understand:
I had to study instructions and introductory sections of the workbook very carefully, reading them several times before attempting the tasks. I think it’s mainly about switching on to the often abstract vocabulary, i.e. getting on the “wavelength”.
Feedback forms were returned anonymously by 12 participants out of the 20 who took part in the MemFlex intervention. Thematic analysis resulted in two key themes: benefits/outcomes of intervention and overall enjoyment of intervention.
Benefits/outcomes of intervention
Two participants answered “No” to the question “Did you feel you benefitted in any way from taking part in the training programme, and if so, how?” but did not expand on their answers any further. The remaining 10 participants reported positive outcomes, even if they were not sure whether they had actually benefitted from the training in terms of improving their memory. The outcomes reported were: helped recognise that their memory was not as bad as they thought; increased understanding of why memory difficulties occur; received interesting and stimulating activity; and enjoyed the experience of recalling memories from the past. For example:
Yes, the retrieval parts were important to me. It helped me to realise that maybe my overall image of my memory were not as bad as I imagined.
For me in particular it helped me to understand that I do have a momentary blank when I am feeling some stress.
“I’m not sure whether I benefitted from the training programme, but I enjoyed it and found it interesting.” “Any mental activity must help as one ages.”
Overall enjoyment of the intervention
Participants commented that recalling memories of past events was a positive, enjoyable experience. The programme gave them the opportunity to recall memories that they may not have thought about for a long time because they had not previously had any reason to recall them, therefore the workbook gave them a platform to recall old memories.
Yes, made me remember lots that I thought I had forgotten
It did drag up memories I had forgotten about, which was quite refreshing
Discussion
We hypothesised that cognitive flexibility and AMS would both improve in the MemFlex group relative to controls. Our findings show an improvement in AMS and the inhibition aspect of cognitive flexibility (indicated by decreased adjacency scores) across time in the whole sample. However, these improvements were not higher in the MemFlex group than in controls. The lack of interaction suggests improvements may be due to other factors independent of the training, such as the benefit of simply receiving mental stimulation. It could also be due to practice effects as a result of participants (in both MemFlex and control groups) completing the AMT and RNG task on multiple occasions. The qualitative analysis supports this as participants felt that completing the MemFlex workbook was generally stimulating and a positive experience, but may not have had specific effects on their memory.
The overall improvement in AMS across time suggests that AM specificity is a modifiable cognitive skill, and thus OGM commonly found in older populations (Holland et al., Citation2012; Piolino, Desgranges, Benali, & Eustache, Citation2002; Ros et al., Citation2010) is amenable to change. This is important as higher AM specificity has been related to better mental well-being in non-depressed older populations (Latorre et al., Citation2013). It also supports the findings from our previous study where MEST and life review AM training methods were successful at reducing OGM in a non-depressed older adult sample (Leahy et al., Citation2017) compared to a control group. Furthermore, previous studies with depressed younger adults have indicated that MEST has positive effects on reducing OGM and reducing depressive symptoms (Moradi et al., Citation2014; Neshat Doost et al., Citation2014; Raes et al., Citation2009). However, this is the first study to test MemFlex with a population who are both older and non-depressed. MemFlex was originally designed for younger, depressed adults, to target maladaptive cognitive patterns such as a bias towards the negative material. Therefore, it may be that the lack of expected effects was due to the target population not showing the same cognitive biases, i.e., older adults did not have a negative bias.
The social context of the training may also be of relevance. MEST has mainly been conducted in small groups of participants (Raes et al., Citation2009), whereas in the current study MemFlex and control groups completed a workbook at home. Therefore it may be that the lack of an effect of the MemFlex workbook on AMS in the current study was due to participants only receiving minimum feedback, encouragement and support in practising the cued recall tasks. The qualitative findings support this as one of the reasons participants withdrew was due to difficulty comprehending the workbook. This could potentially be overcome by receiving more help and guidance throughout each session in a face-to-face setting. This also emphasises the need for a comparison between AMS training studies and a matched control group who receive a similar level of group contact, as previous studies have also used a minimal contact control (Leahy et al., Citation2017; Moradi et al., Citation2014; Neshat Doost et al., Citation2014).
The control workbook used in the current study was different from the control workbook in the original MemFlex study. Both workbooks included psychoeducation, but in the previous study, this was about depression, whereas in the current study it was about healthy ageing. Therefore, one potential explanation for the lack of expected difference in AMS between the groups post-training is that the control workbook might have improved AMS by promoting well-being. For example, the healthy ageing workbook highlighted the importance of staying physically fit and socially active, both of which are associated with a higher cognitive function in old age (Bennett et al., Citation2006; Colcombe and Kramer Citation2003).
Alea and Bluck’s (Citation2003) conceptual model of the social functions of AM highlights how recalling personal memories often occurs in social contexts in everyday life and therefore the actual process of sharing AMs with others, rather than just thinking about them to oneself and writing them down in a workbook, may be relevant in studies examining the functional aspects of AM. Individuals also collaborate and co-construct memories with others (Edwards & Middleton, Citation1986; Gould & Dixon, Citation1993), For example, in our previous study older adults felt they benefitted from the sociable aspect of the group setting used for the MEST group (Leahy et al., Citation2017). In a group setting, listening to other people’s memories may help to prompt one’s own memories, especially if they are people from a similar generation and therefore had similar era specific memories. Since memory is functional, it may be that there was an absence of contextual and social cues that typically would facilitate recall in daily life due to the format of the training, i.e., retrieving memories at home, and possibly alone. In support of this, one of the MemFlex participants commented that it was extremely difficult to recall memories at home because she lived alone and had nobody to discuss, or possibly rehearse, memories with. Furthermore, Holland and Kensinger (Citation2010) point out that verbal elaboration is an effective emotion regulation technique and that specific AM retrieval may involve similar processes. Perhaps verbalisation of the emotional details of specific AMs may be more useful for emotion regulation purposes.
The hypothesis that participants in the MemFlex group would exhibit improvements on secondary outcome measures relative to controls was also unsupported. There were no significant improvements in social problem-solving, independence, or depression measures. In contrast to our expected findings, a marginally significant decrease in MEPS scores was observed in the MemFlex group only between post-training and 3-month follow-up. We speculate that this is because their MEPS scores increased from pre-training to post-training (although not significantly so), therefore the significant decrease from post-training to 3-month follow-up may be a simple reversion back to baseline. This is supported by the significant quadratic effect on MEPS scores between time and group, and the lack of a significant difference between MEPS scores at 3-month follow-up and pre-training. The lack of an effect on depression and independence could be explained by floor and ceiling effects as the sample had low depression ratings and high independence scores at baseline, therefore, there was little room for improvement, unlike in the study by Holland et al. (Citation2017) where there was more variance in level of functional limitations. Given the encouraging findings with depressed younger adults, it may be useful for future studies to examine the effectiveness of MemFlex with a sample of clinically depressed older adults, since this population are likely to have more pronounced OGM at baseline and higher rates of depression, thus resulting in a greater potential for improvement.
However, change in AMS was related to change in social problem-solving. This correlation was not significant after correcting for multiple comparisons and therefore caution should be taken, although it is in line with previous findings of a relationship between these variables (Beaman et al., Citation2007; Leahy et al., Citation2017), which supports the constructive episodic simulation hypothesis. This hypothesis states that the process of retrieving AMs is analogous to the process of generating solutions to social problems (Schacter & Addis, Citation2007, Citation2009). Previous research supports the suggestion that older adults’ social problem-solving performance benefitted from brief training in recollecting details of past experiences (Madore & Schacter, Citation2014). This has implications for the maintenance of well-being in later life since social functioning is essential to maintaining an active, engaged lifestyle.
We found no evidence for the hypothesised bias towards recalling specific positive memories compared to negative. However, in support of the hypothesis that there would be limited effects on positive compared to negative recall, there was a significant improvement in the whole sample in negative, but not positive, specific recall across time. The improvement in inhibition ability in the whole sample was not significantly related to the improvement in overall AMS, or to positive or negative AMS separately, therefore, the hypothesis that increases in the negative specific recall would be related to improvement in cognitive flexibility was unsupported.
We did, however, find that people with the highest adjacency scores (i.e., lowest inhibition ability) at baseline had the biggest improvements in the specific recall. This improvement was particularly in relation to negative memories, therefore, supporting the hypothesis that older adults may be protected from a detrimental impact of reduced cognitive flexibility on retrieving memories of a positive valence. This is in line with a previous finding that although executive function predicts overall specificity in older adults, it does not predict specific positive recall, suggesting that specific positive recall is not influenced by reduced executive control in older adults (Holland et al., Citation2012). This may be because preserved emotional processing in older adults provides an automatic route to specific positive memories, resulting in less demand on executive functions (Scheibe & Blanchard-Fields, Citation2009). Together with the overall practice effects, this suggests that people with lower inhibition improved more so in negative specificity because it required more practice in the generative search process of inhibiting general memories. On the other hand, positive memories were recalled automatically, bypassing executive function, thus not requiring practice. This is important because previous research has suggested that a lack of inhibition of general memories in order to access specific memories can lead to generalisation and negative rumination processes associated with depression (Williams et al., Citation2007). Thus training the executive process of inhibiting general negative memories may be useful for reducing rumination in depressed older adults. However, this suggestion should be taken with caution because there was no effect on mood in the current study.
It could be that training the inhibition element of flexibility in negative retrieval may only be useful for depression-related OGM, i.e., in those who are currently clinically depressed. This technique may, however, be less useful in non-depressed older adults if positive specific recall is protected from the impact of age-related cognitive flexibility deficit on AMS. Previous AMS training with non-depressed older adults which focussed on specific positive AMs only has been effective at improving life satisfaction and reducing depression symptoms (Latorre et al., Citation2013). As Holland et al. (Citation2012) suggested focussing on positive recall as a strategy may act as a buffer against OGM recall in healthy older adults. In addition, qualitative findings from our previous study suggested that an AM training method which focussed solely on positive events (i.e., life review) was more appropriate for healthy older adults than MEST, which included both positive and negative events (Leahy et al., Citation2017). We propose that interventions for age-related OGM may benefit from targeting positive memories instead of the executive processes associated with negative generalisation, whilst the latter may be a more useful strategy for depressed older adults.
One limitation of the study was that the sample size was small, however, it is larger than other studies which have found large effects on AMS (Heeren et al., Citation2009; Neshat Doost et al., Citation2014; Raes et al., Citation2009). The power was also sufficient to detect effects according to a power analysis conducted for a within-between interaction design with an effect size of f = 0.3 (a large effect size), a power of 0.80, with a type 1 error rate α = 0.05 which gave n = 20 per group.
Another limitation was that the MemFlex group had significantly more functional limitations at baseline than did the controls. However, the group differences related to physical health; i.e., walking and using stairs, and body care or movement, which would be less likely to influence the effectiveness of the MemFlex intervention than would variations in cognitive limitations.
It is possible that the workbook was either too difficult for participants to complete or that the language used was hard to follow or understand. This was supported by the qualitative analysis as readability and comprehension was an issued raised by some, but not all of the participants. It may be useful for future studies to consider participant involvement in the development of the workbook questions, structure and language to ensure that it is suitable for an older adult population.
A final limitation is that we measured the executive functions, which are regarded as underlying components of cognitive flexibility, such as updating, inhibition and initiation. Although the verbal fluency tasks are considered a broad measure of executive control and cognitive flexibility (e.g., Eslinger & Grattan, Citation1993), caution should be taken in generalising these functions to their use in specific AM retrieval. Future studies may wish to resolve this by employing a wider range of cognitive flexibility measures directly. For example, the Wisconsin card sorting task is often used as a measure of set shifting or flexibility as it requires participants to stop perseverating on one rule, for example, sort the cards by colour, and switch to a different rule, for example, sort the cards by number. A direct measure of AM flexibility as opposed to just the proposed underlying benefit of cognitive flexibility to AMS would also be helpful in order to investigate whether ability to flexibly retrieve different types of AM was improved by MemFlex. For example, the AMT-AI (Dritschel et al., Citation2013) measure would inform us about any effect of MemFlex on switching between retrieving general memories when instructed, to retrieving specific memories when instructed, and vice versa.
In conclusion, the results showed that AMS and inhibition ability are amenable to change in older adults. Although there were no effects on secondary outcomes, there was a relationship between change in AMS and change in social problem-solving, supporting the usefulness of AMs to social functioning, which is critical to older adults’ well-being. The finding that baseline lower inhibition ability was positively correlated with change in negative AMS supports the hypothesis that positive AMS may be an automatic process in older adults. We propose that whilst interventions for depression may benefit from practice in inhibiting general negative memories, in healthy older adults it may be more useful to focus on positive memory recall. Incorporating the sociable aspect of sharing memories with others into retrieval practice may also be helpful.
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
Fiona Leahy http://orcid.org/0000-0002-7223-3861
Nathan Ridout http://orcid.org/0000-0002-7111-2996
Carol Holland http://orcid.org/0000-0001-7109-6554
Additional information
Funding
Related Research Data
References
- Alea, N., & Bluck, S. (2003). Why are you telling me that? A conceptual model of the social function of autobiographical memory. Memory, 11(2), 165–178. doi: 10.1080/741938207
- Beaman, A., Pushkar, D., Etezadi, S., Bye, D., & Conway, M. (2007). Autobiographical memory specificity predicts problem-solving ability in old and young adults. The Quarterly Journal of Experimental Psychology, 60, 1275–1288. doi: 10.1080/17470210600943450
- Bennett, D. A., Schneider, J. A., Tang, Y., Arnold, S. E., & Wilson, R. S. (2006). The effect of social networks on the relation between Alzheimer’s disease pathology and level of cognitive function in old people: A longitudinal cohort study. The Lancet Neurology, 5(5), 406–412. doi: 10.1016/S1474-4422(06)70417-3
- Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. doi: 10.1191/1478088706qp063oa
- Campos, W., Martinez, A., Sanchez, W., Estrada, H., Favela, J., & Perez, J. (2016). Inferring social isolation in older adults through ambient intelligence and social networking sites. Computación y Sistemas, 20(1), 143–152.
- Carstensen, L. L., Isaacowitz, D. M., & Charles, S. T. (1999). Taking time seriously: A theory of socioemotional selectivity. American Psychologist, 54, 165–181. doi: 10.1037/0003-066X.54.3.165
- Colcombe, S., & Kramer, A. F. (2003). Fitness effects on the cognitive function of older adults a meta-analytic study. Psychological science, 14(2), 125–130. doi: 10.1111/1467-9280.t01-1-01430
- Conway, M. A., & Pleydell-Pearce, C. W. (2000). The construction of autobiographical memories in the self-memory system. Psychological Review, 107(2), 261. doi: 10.1037/0033-295X.107.2.261
- Dalgleish, T., Williams, J. G., Golden, A. J., Perkins, N., Barrett, L., Barnard, P. J., & Watkins, E. (2007). Reduced specificity of autobiographical memory and depression: The role of executive control. Journal of Experimental Psychology: General, 136(1), 23–42. doi: 10.1037/0096-3445.136.1.23
- Da Silva, J., Gonçalves-Pereira, M., Xavier, M., & Mukaetova-Ladinska, E. B. (2013). Affective disorders and risk of developing dementia: Systematic review. The British Journal of Psychiatry, 202(3), 177–186. doi: 10.1192/bjp.bp.111.101931
- Djernes, J. K. (2006). Prevalence and predictors of depression in populations of elderly: A review. Acta Psychiatrica Scandinavica, 113(5), 372–387. doi: 10.1111/j.1600-0447.2006.00770.x
- Dritschel, B., Beltsos, S., & McClintock, S. M. (2013). An “alternating instructions” version of the autobiographical memory test for assessing autobiographical memory specificity in non-clinical populations. Memory, 22(8), 881–889. doi: 10.1080/09658211.2013.839710
- Edwards, D., & Middleton, D. (1986). Joint remembering: Constructing an account of shared experience through conversational discourse. Discourse Processes, 9(4), 423–459. doi: 10.1080/01638538609544651
- Eslinger, P. J., & Grattan, L. M. (1993). Frontal lobe and frontal-striatal substrates for different forms of human cognitive flexibility. Neuropsychologia, 31(1), 17–28. doi: 10.1016/0028-3932(93)90077-D
- Goddard, L., Dritschel, B., & Burton, A. (1996). Role of autobiographical memory in social problem solving and depression. Journal of Abnormal Psychology, 105, 609–616. doi: 10.1037/0021-843X.105.4.609
- Gotlib, I. H., & Joormann, J. (2010). Cognition and depression: Current status and future directions. Annual Review of Clinical Psychology, 6, 285. doi: 10.1146/annurev.clinpsy.121208.131305
- Gould, O. N., & Dixon, R. A. (1993). How we spent our vacation: Collaborative storytelling by young and old adults. Psychology and Aging, 8(1), 10. doi: 10.1037/0882-7974.8.1.10
- Grant, M. M., Thase, M. E., & Sweeney, J. A. (2001). Cognitive disturbance in outpatient depressed younger adults: Evidence of modest impairment. Biological Psychiatry, 50(1), 35–43. doi: 10.1016/S0006-3223(00)01072-6
- Hayes, S. C., Wilson, K. G., Gifford, E. V., Follette, V. M., & Strosahl, K. (1996). Experiential avoidance and behavioral disorders: A functional dimensional approach to diagnosis and treatment. Journal of Consulting and Clinical Psychology, 64(6), 1152–1168. doi: 10.1037/0022-006X.64.6.1152
- Heeren, A., Van Broeck, N., & Philippot, P. (2009). The effects of mindfulness on executive processes and autobiographical memory specificity. Behaviour Research and Therapy, 47(5), 403–409. doi: 10.1016/j.brat.2009.01.017
- Hitchcock, C., Hammond, E., Rees, C., Panesar, I., Watson, P., Werner-Seidler, A., & Dalgleish, T. (2015). Memory flexibility training (MemFlex) to reduce depressive symptomatology in individuals with major depressive disorder: Study protocol for a randomised controlled trial. Trials, 16(1), 494. doi: 10.1186/s13063-015-1029-y
- Holland, C., Boukouvalas, A., Wallis, S., Clarkesmith, D., Cooke, R., Liddell, L., & Kay, A. (2017). Transition from community dwelling to retirement village in older adults: Cognitive functioning and psychological health outcomes. Ageing & Society, 37(7), 1499–1526. doi: 10.1017/S0144686X16000477
- Holland, A. C., & Kensinger, E. A. (2010). Emotion and autobiographical memory. Physics of Life Reviews, 7(1), 88–131. doi: 10.1016/j.plrev.2010.01.006
- Holland, C. A., Ridout, N., Geraghty, J., & Walford, E. (2012). Executive function and emotional focus in autobiographical specificity in older adults. Memory, 20, 779–793. doi: 10.1080/09658211.2012.703210
- Hsieh, S., Schubert, S., Hoon, C., Mioshi, E., & Hodges, J. R. (2013). Validation of the Addenbrooke’s Cognitive Examination III in frontotemporal dementia and Alzheimer’s disease. Dementia and Geriatric Cognitive Disorders, 36(3–4), 242–250. doi: 10.1159/000351671
- Kashdan, T. B., & Rottenberg, J. (2010). Psychological flexibility as a fundamental aspect of health. Clinical Psychology Review, 30(7), 865–878. doi: 10.1016/j.cpr.2010.03.001
- Katz, S., Ford, A., Moskowitz, R. W., Jackson, B. A., & Jaffe, M. W. (1963). Studies of illness in the aged. Journal of the American Medical Association, 185, 914–919. doi: 10.1001/jama.1963.03060120024016
- Kwon, Y., Scheibe, S., Samanez-Larkin, G. R., Tsai, J. L., & Carstensen, L. L. (2009). Replicating the positivity effect in picture memory in Koreans: Evidence for cross-cultural generalizability. Psychology and Aging, 24(3), 748. doi: 10.1037/a0016054
- Latorre, J. M., Ricarte, J. J., Serrano, J. P., Ros, L., Navarro, B., & Aguilar, M. J. (2013). Performance in autobiographical memory of older adults with depression symptoms. Applied Cognitive Psychology, 27, 167–172. doi: 10.1002/acp.2891
- Lawton, M. P., & Brody, E. M. (1969). Assessment of older people: Self-maintaining and instrumental activities of daily living. The Gerontologist, 9, 179–186. doi: 10.1093/geront/9.3_Part_1.179
- Leahy, F., Ridout, N., Mushtaq, F., & Holland, C. (2017). Improving specific autobiographical memory in older adults: Impacts on mood, social problem solving, and functional limitations. Aging, Neuropsychology, and Cognition, 1–29. doi: 10.1080/13825585.2017.1365815
- Madore, K. P., & Schacter, D. L. (2014). An episodic specificity induction enhances means-end problem solving in young and older adults. Psychology and Aging, 29(4), 913–924. doi: 10.1037/a0038209
- Mather, M., & Carstensen, L. L. (2005). Aging and motivated cognition: The positivity effect in attention and memory. Trends in Cognitive Sciences, 9(10), 496–502. doi: 10.1016/j.tics.2005.08.005
- Mather, M., & Knight, M. (2005). Goal-directed memory: The role of cognitive control in older adults’ emotional memory. Psychology and Aging, 20(4), 554. doi: 10.1037/0882-7974.20.4.554
- Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., & Wager, T. D. (2000). The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: A latent variable analysis. Cognitive Psychology, 41(1), 49–100. doi: 10.1006/cogp.1999.0734
- Moradi, A. R., Moshirpanahi, S., Parhon, H., Mirzaei, J., Dalgleish, T., & Jobson, L. (2014). A pilot randomized controlled trial investigating the efficacy of memory specificity training in improving symptoms of posttraumatic stress disorder. Behaviour Research and Therapy, 56, 68–74. doi: 10.1016/j.brat.2014.03.002
- Neshat Doost, H. T., Yule, W., Kalantari, M., Rezvani, S. R., Dyregrov, A., & Jobson, L. (2014). Reduced autobiographical memory specificity in bereaved Afghan adolescents. Memory, 22(6), 700–709. doi: 10.1080/09658211.2013.817590
- Noone, P. (2015). Addenbrooke’s Cognitive Examination-III. Occupational Medicine, 65(5), 418–420. doi: 10.1093/occmed/kqv041
- Piolino, P., Desgranges, B., Benali, K., & Eustache, F. (2002). Episodic and semantic remote autobiographical memory in aging. Memory, 10, 239–257. doi: 10.1080/09658210143000353
- Platt, J. J., & Spivack, G. (1975). Manual for the means-end problem solving skill. Philadelphia, PA: Hahnemans Medical College and Hospital.
- Pollard, B., & Johnston, M. (2001). Problems with the sickness impact profile: A theoretically based analysis and a proposal for a new method of implementation and scoring. Social Science & Medicine, 52(6), 921–934. doi: 10.1016/S0277-9536(00)00194-5
- Raes, F., Hermans, D., Williams, J. M. G., Beyers, W., Brunfaut, E., & Eelen, P. (2006). Reduced autobiographical memory specificity and rumination in predicting the course of depression. Journal of Abnormal Psychology, 115(4), 699–704. doi: 10.1037/0021-843X.115.4.699
- Raes, F., Williams, J. M. G., & Hermans, D. (2009). Reducing cognitive vulnerability to depression: A preliminary investigation of memory specificity training (MEST) in inpatients with depressive symptomatology. Journal of Behavior Therapy and Experimental Psychiatry, 40(1), 24–38. doi: 10.1016/j.jbtep.2008.03.001
- Ros, L., Latorre, J. M., & Serrano, J. P. (2010). Working memory capacity and overgeneral autobiographical memory in young and older adults. Aging, Neuropsychology and Cognition, 17, 89–107. doi: 10.1080/13825580903042650
- Schacter, D. L., & Addis, D. R. (2007). The cognitive neuroscience of constructive memory: Remembering the past and imagining the future. Philosophical Transactions of the Royal Society B: Biological Sciences, 362, 773–786. doi: 10.1098/rstb.2007.2087
- Schacter, D. L., & Addis, D. R. (2009). On the nature of medial temporal lobe contributions to the constructive simulation of future events. Philosophical Transactions of the Royal Society B: Biological Sciences, 364, 1245–1253. doi: 10.1098/rstb.2008.0308
- Scheibe, S., & Blanchard-Fields, F. (2009). Effects of regulating emotions on cognitive performance: What is costly for young adults is not so costly for older adults. Psychology and Aging, 24, 217–223. doi: 10.1037/a0013807
- Sumner, J. A., Griffith, J. W., & Mineka, S. (2010). Overgeneral autobiographical memory as a predictor of the course of depression: A meta-analysis. Behaviour Research and Therapy, 48(7), 614–625. doi: 10.1016/j.brat.2010.03.013
- Taconnat, L., Raz, N., Toczé, C., Bouazzaoui, B., Sauzeon, H., Fay, S., & Isingrini, M. (2009). Ageing and organisation strategies in free recall: The role of cognitive flexibility. European Journal of Cognitive Psychology, 21(2–3), 347–365. doi: 10.1080/09541440802296413
- Towse, J. N., & Neil, D. (1998). Analyzing human random generation behavior: A review of methods used and a computer program for describing performance. Behavior Research Methods, Instruments & Computers, 30, 583–591. doi: 10.3758/BF03209475
- Williams, J. G., Barnhofer, T., Crane, C., Hermans, D., Raes, F., Watkins, E., & Dalgleish, T. (2007). Autobiographical memory specificity and emotional disorder. Psychological Bulletin, 133(1), 122–148. doi: 10.1037/0033-2909.133.1.122
- Williams, J. M. G., & Broadbent, K. (1986). Autobiographical memory in suicide attempters. Journal of Abnormal Psychology, 95, 144–149. doi: 10.1037/0021-843X.95.2.144
- Zigmond, A. S., & Snaith, R. P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica, 67, 361–370. doi: 10.1111/j.1600-0447.1983.tb09716.x