
ABSTRACT
Does Eye Movement and Desensitization and Reprocessing (EMDR) therapy affect the accuracy of memories? This recurrent issue in recent memory research bears relevance to expert witness work in the courtroom. In this review, we will argue that several crucial aspects of EMDR may be detrimental to memory. First, research has shown that eye movements undermine the quality and quantity of memory. Specifically, eye movements have been shown to decrease the vividness and emotionality of autobiographical experiences and amplify spontaneous false memory levels. Second, a sizeable proportion of EMDR practitioners endorse the controversial idea of repressed memories and discuss the topic of repressed memory in therapy. Third, in the Dutch EMDR protocol, patients are instructed to select the target image by using flawed metaphors of memory (e.g., memory works as a video). Such instructions may create demand characteristics to the effect that people over-interpret imagery during therapy as veridical memories. Collectively, the corpus of research suggests that several components of EMDR therapy (i.e., performing eye movements, therapist beliefs and therapeutic instructions) may undermine the accuracy of memory, which can be risky if patients, later on, serve as witnesses in legal proceedings.
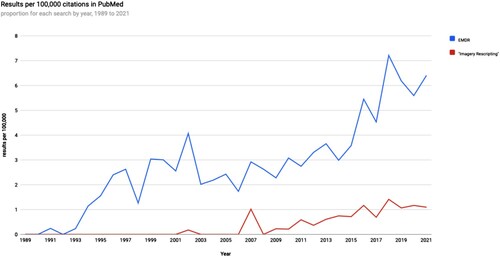
As memory experts, we are oftentimes asked whether certain therapies may compromise memory accuracy. Much of this discussion revolves around the potential suggestive nature of therapeutic interventions (e.g., hypnosis) and its impact on memory (Lynn et al., Citation2020). Certain therapeutic interventions such as Eye Movement and Desensitization and Reprocessing (EMDR) contain features (e.g., eye movements) that at first sight are not suggestive. However, legal cases concerning possible false memories of abuse have revealed that some patients turned out to suffer from false memories of being abused after EMDR therapy (Shaw & Vredeveldt, Citation2019; see also Felstead & French, Citationin press). Hence, the often raised question is whether Eye Movement and Desensitization and Reprocessing (EMDR) therapy might also undermine memory. Why the question often pertains to EMDR is because EMDR is a highly popular therapeutic intervention that receives an increasing amount of scientific interest (see ).
Figure 1. Number of (international) publications on EMDR and Imagery Rescripting using the webpage https://esperr.github.io/pubmed-by-year/ Search terms included “EMDR” and “Imagery Rescripting”.
EMDR is widely applied to treat people with Posttraumatic Stress Disorder (Cuijpers et al., Citation2020). During EMDR, a patient is requested to retrieve the most disturbing trauma memory and, while doing so, make multiple saccadic eye movements that can be elicited, for example, by the therapist moving the index finger in the patient’s visual field. Since legal cases have shown that after EMDR therapy, patients might remember traumatic experiences (e.g., sexual abuse) and make accusations based on these memories (Shaw & Vredeveldt, Citation2019), a fundamental question is whether EMDR possesses several characteristics that might undermine memory. In the present review, we have amassed the available evidence on the link between EMDR and memory performance. We will focus on different aspects of the EMDR protocol that have been studied in the context of memory. Specifically, we will discuss the role of eye movements, therapists’ beliefs about memory, and therapeutic instructions to patients. To forecast our findings, EMDR carries with it several problematic aspects that have been shown to undermine the quality and quantity of memory.
Eye movements and memory
There is a long fascination concerning the psychological and physiological effects of eye movements (e.g., Du Laurens, 1596 cited in Wade & Tatler, Citation2005). Of crucial relevance for this review was Shapiro’s discovery that saccadic eye movements tended to reduce her disturbing thoughts and memories (Shapiro, Citation1989). Shapiro used this discovery to build an intervention in which eye movements received a prominent position. Although the name of the therapy has been altered over time (i.e., Multi-Saccadic Movement Desensitization; Eye Movement Desensitization), it is now well-known as Eye Movement Desensitization and Reprocessing (EMDR). A significant component of EMDR is making (saccadic) eye movements during the retrieval of an unwanted traumatic memory.
Experimentation in how eye movements can impact memory retrieval can be broadly divided into two main research lines. One has predominantly focused on the link between eye movements and memory quality, while the second concentrated on eye movements and memory quantity. In the first research line, the default procedure is as follows. Participants are instructed to retrieve emotional autobiographical memories and rate them on vividness and emotionality (pre-test). Following this, participants in the eye movement condition are requested to retrieve these memories while simultaneously making eye movements, while control participants engage in retrieval without performing such eye movements. Then, all participants are asked to rate the vividness and emotionality of their memories again (post-test). Retrieving an autobiographical experience and performing eye movements require working memory capacity. Due to its limited capacity, the working memory account states that performing these two tasks simultaneously will result in imagination deflation leading to less vivid (and emotional) memories (van den Hout & Engelhard, Citation2012). The phenomenon of imagination deflation can be seen as the antipode of imagination inflation, referring to the phenomenon that the repeated imagination of non-experienced events can make people more confident that the events actually were experienced (e.g., Thomas & Loftus, Citation2002).
Eye movements and memory quality
Several meta-analyses have been conducted to examine the strength of eye movements to undermine the vividness and emotionality of emotional autobiographical experiences. Lee and Cuijpers (Citation2013) included 15 clinical trials and 11 laboratory studies that compared standard EMDR procedures with adapted EMDR procedures in which eye movements were left out. For the clinical trials, outcome variables were the Subjects Units of Distress Scale (SUDs) and Validity of Cognition (VoC). SUD ratings measure the level of distress evoked by traumatic memories, while VoC ratings measure the believability of a positive cognition in relation to these memories. For the laboratory studies, measurements scales were vividness and emotionality Likert scales. Lee and Cuijpers (Citation2013) found that participants who made eye movements during memory retrieval had statistically significantly lower SUDs and higher VoCs than participants who did not make eye movements, associated with Cohen’s ds of 0.53 and 0.72, respectively. Furthermore, concerning the laboratory studies, vividness and emotionality ratings were significantly lower in participants who performed eye movements than in those who did not perform eye movements, a difference linked with Cohen’s ds of 0.91 and 0.66, respectively. Importantly, recent research has also demonstrated that this effect is not affected by expectations concerning the treatment effectiveness of EMDR (Littel et al., Citation2017; Mertens et al., Citation2021).
In a recent meta-analysis, Houben and colleagues (Citation2020a) examined laboratory studies and compared the efficacy of eye movements relative to alternative dual-tasks (e.g., counting) on reducing vividness and emotionality ratings of emotional autobiographical memories. They showed that vividness and emotionality ratings were lowered in participants who engaged in eye movements than in participants without eye movements (Cohen’s ds: 0.59 and 0.28, respectively). Interestingly, the authors demonstrated that alternative dual-tasks also led to reductions in vividness and emotionality with Cohen’s ds of 0.49 and 0.32, respectively. These findings suggest that eye movements do not uniquely undermine vividness and emotionality and that this effect can be obtained by using alternative dual-tasks as well.
To recap, the body of evidence has shown that eye movements undermine the quality of emotional memories, making them less vivid and emotional. This is important for the legal arena and, more specifically, for psychologists providing expert witness testimony on memory. Specifically, memory experts tasked with the responsibility to evaluate the validity of testimonies concerning sexual abuse of patients undergoing EMDR should consider that such testimonies may well have been negatively affected by eye movements. This is also important for two reasons. First, testimonies containing highly vivid and emotional details are more likely to be perceived as credible (e.g., Bell & Loftus, Citation1985; Kaufmann et al., Citation2003; Wessel et al., Citation2016). If memories become less vivid and emotional due to eye movements, statements might be unduly regarded as not credible. Second, although emotional memories are also susceptible to distortion, negative emotions oftentimes enhance memory accuracy (Kensinger, Citation2007). Memories that become less emotional might also become less accurate or perceived as less accurate, which would undermine the reliability of testimonies.
Eye movements and memory quantity
Considerable experimental work examined the effect of eye movements on memory quantity during retrieval. What these studies have examined is how eye movements affect the remembrance of experienced (accurate memories) and non-experienced (false memories) events. One line of investigation has focused on performing eye movements before retrieval. In these studies, participants are presented with some stimuli (e.g., words), and just before retrieval, some participants performed eye movements, and some did not. Studies have shown that eye movements benefit memory performance, an effect dubbed as the Saccadic-Induced Retrieval Enhancement effect (SIRE; Christman et al., Citation2003; Lyle & Martin, Citation2010). Although SIRE has been replicated using various stimuli such as facial stimuli (Lyle & Orsborn, Citation2011) and neutral and negative words (Nieuwenhuis et al., Citation2013), failed replications have been published as well (Matzke et al., Citation2015; Roberts et al., Citation2020). A recent meta-analysis showed that SIRE had a pooled effect size of 0.45 (Cohen’s d; Qin et al., Citation2021).
Apart from the finding that eye movements might affect accurate memories, a more pertinent question is whether an eye movement intervention promotes the formation of false memories. In the context of the treatment of victims of traumas caused by perpetrators, this question is important. Oftentimes, victims are not just victims but also eyewitnesses who provide evidence to the courts. Here, false memories of eyewitnesses can lead to false accusations and contribute to wrongful convictions. As to the genesis of such false memories, an argument that has been forwarded repeatedly is that certain therapeutic interventions can be inherently suggestive, thereby fomenting the susceptibility to form false memories (e.g., Houben et al., Citation2019; Loftus, Citation1994).
Although the SIRE effect has been examined in the context of false memories (e.g., Parker et al., Citation2009; Parker & Dagnall, Citation2007), in general, the SIRE effect is severely limited to explain EMDR effects on true and false memory. The primary reason is that in experiments examining SIRE, eye movements happen just before retrieval, while in EMDR, eye movements happen during retrieval (see also Phaf, Citation2017). Because of this, Houben and colleagues (Citation2018) examined whether eye movements might facilitate the formation of false memories using a procedure more analogous to what happens in EMDR sessions. Specifically, Houben and colleagues had undergraduates watch a video depicting a car crash. After this, participants were asked to think about the video and any emotions that they experienced. Simultaneously, one-half of the participants had to perform eye movements while control participants had to keep their eyes stationary. Following this, all participants received misinformation in the form of an eyewitness narrative. Misinformation was more often reported by participants performing eye movements than participants in the control condition.
After this initial demonstration, several research labs attempted to replicate this effect (Calvillo & Emami, Citation2019; Kenchel et al., Citationin press; van Schie & Leer, Citation2019). In general, these authors failed to replicate the finding that eye movements increased the reporting of misinformation. Kenchel and colleagues also conducted a meta-analysis on all studies examining eye movements and misinformation reporting and found a non-significant effect. Reasons for the failure to replicate the effect of eye movements on misinformation reporting are various, ranging from insufficient blinding of experimenters to false positive or false negative findings. One way to remedy this is to resort to a false memory procedure that does not rely on external pressure (e.g., misinformation) and automatically evokes false memories (see also van Schie & Leer, Citation2019). This type of false memory is also called spontaneous false memories (Brainerd et al., Citation2008). False memory propensity induced by suggestion is often unrelated to the susceptibility of spontaneous false memories (Bernstein et al., Citation2018; Ost et al., Citation2013; Otgaar & Candel, Citation2011; Patihis et al., Citation2018) proposing that different mechanisms underlie the formation of suggestion-induced and spontaneous false memories.
Houben and colleagues (Citation2020b) examined the effect of eye movements on false memories using the Deese/Roediger-McDermott (DRM) paradigm (Deese, Citation1959; Roediger & McDermott, Citation1995). In this paradigm, participants have to study word lists containing words that are associatively related to each other (e.g., bed, tired, dream, etc). When participants have to recall/recognize which words they have witnessed, a significant proportion of participants falsely recollect a related non-presented word called the critical lure (i.e., sleep). These false memories are also called spontaneous false memories as they are automatically produced without any suggestive external pressure (Brainerd & Mojardin, Citation1998). In two experiments, Houben et al. presented participants with neutral and emotionally negative DRM lists and immediately (Experiment 1) or 48 h later (Experiment 2), they received a recall and recognition task. Half of the participants had to perform eye movements during the recall task, while others did not have to perform them. The canonical result was that, not immediately, but after 48 h, eye movements led to an increase in spontaneous false memory levels in both recall and recognition tests.
Leer and Engelhard (Citation2020) also found that eye movements can increase spontaneous memory errors. In their experiment, participants were involved in an aversive condition phase in which they saw two pictures of male faces followed by a shock. After this, they had to recall one face with eye movements and one without eye movements. In the final task, they received a stimulus discrimination test with slightly different faces immediately or one day later. Of relevance for the current review is the finding that, as in Houben et al.’s (Citation2020a) experiment, not immediately, but after a delay (i.e., one day later), eye movements increased false positive rates. The fact that these memory errors occurred after a delay is especially interesting as EMDR is oftentimes not immediately given after an experience, and often takes place after a certain delay. Relatedly, eyewitnesses are also not immediately interviewed after a crime by, for example, the police. Such interviewing oftentimes happens after a delay, and in the meantime, they might undergo EMDR.
Taken together, based on the available work on eye movements and false memories, we agree with Kenchel et al. (Citationin press) concluding “that eye movements do not reliably affect susceptibility to misinformation, nor do they appear to enhance memory, but they do seem to increase spontaneous false memories” (p. 1). However, we want to stress that this conclusion pertains to one particular element of EMDR. We argue that there are other aspects of EMDR as well (e.g., therapy instructions and concepts on which therapists rely), and when those are taken into account, there is ample room for a more fundamental scepticism.
EMDR therapists and repressed memory
To deliver adequate therapy, therapists should be well trained in providing treatment. Because EMDR heavily relies on changing emotional autobiographical memories, it is imperative that therapists possess up-to-date knowledge about key aspects of memory functioning. An especially important aspect here is the controversial topic of repressed memory, which refers to the idea that psychological trauma can lead to an unconscious blockage of traumatic experiences waiting to be retrieved in an almost perfect form (Loftus & Ketcham, Citation1994). The topic of repressed memory is controversial, because empirical research does not support this memory phenomenon. Rather there is every reason to assume that traumatic experiences are actually well remembered (e.g., McNally, Citation2005). Furthermore, a wealth of research and legal cases have shown that believing in this controversial topic can make therapists suggestively dredge for repressed memories, which leads to false memories of sexual abuse (Houben et al., Citation2019; Loftus & Ketcham, Citation1994).
However, in the 1990s, there was an explosion of legal cases in which patients went to therapy without having any recollection of abuse, but started to form “memories” of abuse after repeated suggestive therapeutic interventions (Loftus & Ketcham, Citation1994). These cases started a heated debate about the authenticity of these claims, also known as the memory wars (Crews, Citation1995). One side of scholars, mostly clinicians, contended that these claims were authentic referring to experienced abusive events and that therapy assisted in recovering these repressed memories of abuse. However, other scholars, mostly memory researchers, asserted that the therapeutic interventions might have inadvertently led to the creation of false memories of abuse. Although some scholars have stated that the memory wars have ended (e.g., McHugh, Citation2003), recent research shows that there is a revival of the memory wars (Otgaar et al., Citation2019; in press). A major prong in this debate is the prevalence of people believing in the controversial notion of repressed memory.
Specifically, the impetus of much research in the area of repressed memory is to examine whether people believe in the concept of repressed memories. What has often been done is to survey people’s beliefs about various aspects of memory including the controversial belief in repressed memory. From the 1990s to now, different populations have been surveyed about their belief in repressed memory. For example, Merckelbach and Wessel (Citation1998) found that 96% (n = 25) of licenced psychotherapists believed in the existence of repressed memories. More recently, Patihis and colleagues (Citation2014) showed that 60.3% (n = 35) of clinical psychologists and 69.1% (n = 56) of psychoanalysts agreed that memories of trauma are frequently repressed. Otgaar and colleagues (Citation2019) demonstrated that when all survey studies were combined, among clinical psychologists, the belief in repressed memory was 61% (n = 719), and this percentage increased to 76% (n = 1,586) from 2010 onward.
What do EMDR therapists believe about the existence of repressed memory? Wessel (Citation2018) found that 93% (n = 457) of surveyed EMDR practitioners agreed that traumatic memories could be blocked. Furthermore, Houben and colleagues (in press) examined EMDR therapists’ beliefs about memory. In two studies, they found that the majority of EMDR therapists believed in the existence of unconsciously repressed memories (Study 1: 91.7%, n = 11; Study 2: 70.7%, n = 29). When these percentages are viewed from a broader perspective, the following picture emerges. First, Otgaar and colleagues (Citation2019) recently reviewed all survey studies on the belief in repressed memory and found that on average, 58% (n = 4745) of the surveyed people (i.e., laypersons, clinical psychologists and other professionals) indicated to believe to some extent in repressed memory. It is clear that the percentages detected in Wessel and Houben et al.’s research are much higher than this percentage. Second, when Otgaar et al. focused on the percentage of clinical psychologists believing in repressed memory, a percentage of 70% (n = 2,305) was detected. Here too, two of the three percentages (93% and 91.7%) of EMDR therapists believing in repressed memory are considerably higher than the 70% in Otgaar et al.’s review. Third, in Houben et al.’s second study, students following a clinically oriented master’s and researchers in the field of clinical psychology were also surveyed on their belief in repressed memory. Houben et al. found that 87.5% (n = 21) of students and 66.7% (n = 20) of researchers agreed that memory is able to unconsciously block traumatic experiences showing that although lower than students, a higher percentage of EMDR therapists believed in repressed memory than researchers in the field of clinical psychology. Taken together, the current data showed that a large percentage of the surveyed EMDR therapists believed in the controversial topic of repressed memory and that this percentage is oftentimes higher than when other practitioners were asked about their belief in repressed memory (e.g., clinical psychologists).
Furthermore, in Houben et al.’s (Citation2020b) first study, the authors presented EMDR practitioners with a case vignette about a patient who had no traumatic memory about sexual abuse before EMDR therapy, but recovered a traumatic memory during therapy. Seventy-five percent (n = 9) of the EMDR practitioners indicated that this recovered memory was (very) likely to be authentic and that EMDR contributes to the retrieval of such memories. Taken together, many EMDR therapists seem to firmly believe in the controversial topic of unconsciously repressed memories. This can be potentially perilous, because the belief in repressed memories may encourage EMDR therapists to suggestively search for “hidden” memories, which might ultimately lead to the creation of false memories of sexual abuse. Indeed, Patihis and Pendergrast (Citation2019) found that 9% of the surveyed people from the general population of the US (N = 2326) stated that they consulted with therapists discussing the possibility of repressed abuse, and 5% reported recovering memories of abuse in therapy not known before therapy. Of relevance for this article is that EMDR was often mentioned in the context of recovered memories (see for replication with US undergraduate students; Patihis et al., Citation2020). Dodier and colleagues (Citation2019) conducted a replication among the French community and observed striking similar results. That is, they found that several types of therapy, including EMDR, were associated with discussions on repression. Specifically, Dodier et al. noted that “the therapies during which the most memories were recovered were behavioural, cognitive–behavioural, and EMDR therapies” (p. 1292).
Whenever trauma memories recovered during EMDR therapy surface in courts of law, and therapists are asked to provide background information, there is a problem. The reason why this is problematic is because the clinical/therapeutic context has several characteristics that are at odds with the role of the psychological expert witness. Greenberg and Shuman (Citation1997) discussed ten differences between clinical and forensic roles. These differences are so fundamental that Richards et al. (Citation2015) refer to the involvement of the different roles as a role bias. One difference is that for clinical psychologists, the patient him/herself is the commissioning party (albeit oftentimes indirectly via the company that the psychologist works for), whereas, in a forensic context, the judge or lawyer is oftentimes the commissioning party. Consequently, whereas in a clinical context, there is therapist–patient confidentiality, the allegiance of the legal psychologist (e.g., a memory expert) lies with the judge. Next, whereas a clinical psychologist is expected to display an empathic attitude, the legal psychologist needs to be more distant, neutral, and detached. Obviously, clinical roles require different capabilities (treatment techniques) than do forensic roles (e.g., evaluation and diagnostics). The goal of therapeutic cooperation between the clinical psychologist and the patient is to improve the patient’s wellbeing, whereas the goal of the legal psychologist is informing the courts about certain aspects of the evidence at hand. In other words, the therapeutic role is patient-centred, whereas the forensic role is truth-centred. Hence, because clinical psychologists are not truth-centered, they do not examine whether patients’ memories of abuse reflect historical facts.
EMDR therapy instructions and memory
When patients receive EMDR, they are instructed to select a target image, the so-called hot spot that will become the focus of the EMDR treatment. Interestingly, in the Dutch EMDR protocol, a therapist may choose between two metaphorical instructions. One describes memory functioning as video, while the other describes memory working as a photo (de Jongh & ten Broeke, Citation2016). Arguably, these metaphors are problematic as memory is reconstructive and does not work as a video or photograph. Houben and colleagues (in press) recently showed that such instructions could also exert adverse consequences on patients’ expectations on how they should recall the target image. Specifically, they provided student participants with a video, photo, or control instruction and were asked to indicate – amongst others – how vivid they expected to recall the traumatic memory. Participants who received the video metaphor were expected to recall the memory more vividly than participants in the photo and control groups did. By implication, patients receiving such video instructions might expect to make their target memory more vivid, thereby perhaps embellishing their memory account with false details. Reviewing the literature on demand characteristics and therapy, Kanter et al. (Citation2002) concluded that
As a therapeutic rationale is gradually imparted, patients come to define themselves in terms of it. Hence, patients of psychoanalysts eventually develop Oedipal conflicts, patients of cognitive–behaviorists predictably evidence cognitive distortions, patients of existential therapists reliably display profound existential anxiety (..).
Other therapies and potential memory errors
We primarily focused, for good reasons, on EMDR and its problematic role in the courtroom. Specifically, EMDR is a highly popular therapeutic intervention and has been discussed in the context of potential false memory cases. Of course, this does not mean that there are no other potential therapies that might cause harm. Lilienfeld (Citation2007) already described the potential harm that certain therapies could exert, ranging from increases of depressive symptoms to false accusations of abuse. Furthermore, there is growing interest in potential adverse side effects that therapeutic interventions might exert on patients (e.g., Moritz et al., Citation2015). For example, Rozental et al. (Citation2016) found that 38% of their surveyed patients (total N = 653) mentioned explicitly that “unpleasant memories surfaced” during treatment. Such work is of interest for the current discussion as we are predominantly interested in therapies that might adversely affect memory.
During the heyday of the memory wars in the 1990s, much caution was raised about recovered memory techniques potentially fomenting false memory production (Lynn et al., Citation2003). Oftentimes, such techniques were highly suggestive, leading to the formation of false memories. More recently, empirical attention on how memory can be harnessed to aid in treatment is accumulating (Phelps & Hofmann, Citation2019). Because of this increased interest, questions should also be posited on how memory editing without any suggestive pressure might contribute to adverse side effects such as false memory formation. For example, cognitive reappraisal is currently promoted as an effective way to reduce negative thoughts of a traumatic experience (Samide & Ritchey, Citation2020). During cognitive reappraisal, a past memory of, for example, abuse is reinterpreted on a more focused result. Such reappraisal can be regarded as a special case of memory modification and research has recently shown that reappraisal can lead to memory distortions (e.g., Patihis et al., Citation2019).
A popular therapeutic intervention using cognitive reappraisal techniques is imagery rescripting. During imagery rescripting, patients are asked to retrieve a traumatic memory and to “change” (rescript) it into a more positive one (Arntz, Citation2012). For example, a patient who remembers being abused by her father might imagine that just before the start, someone else stops her father from proceeding with the abusive event. Although imagery rescripting shows promising results in symptom reduction (e.g., Morina et al., Citation2017), clearly, from a memory perspective, imagery rescripting has the potential to contribute to memory distortions. That is, apart from recent evidence indicating that reappraisals lead to memory distortions, imagery rescripting relies heavily on imagination, and imagination can fuel false memory formation (e.g., Mazzoni & Memon, Citation2003).
Because of the strong reliance to date on memory-based therapies, it is crucial that follow-up research should dig into potential memory corrupting effects of these therapies. This is certainly crucial since therapies such as imagery rescripting are progressively gaining scientific attention (see ), although still to a lesser extent than EMDR. So, does, for example, imagery rescripting create larger imagination inflation and misinformation effects? Or will therapists using these techniques likely engage in suggestive tactics to uncover repressed memories? Furthermore, do therapies such as EMDR or imagery rescripting lead to demand characteristics that affects the reporting of information? Such questions are vital for an overarching view on how therapies might harm memory.
Concluding remarks
To conclude, in this article, we have argued that apart from the influence of eye movements on memory, other aspects of EMDR can be problematic for memory, too (see ). That is, what we have shown is that EMDR therapists strongly believe in the controversial topic of repressed memory and frequently discuss the topic of repressed memory in therapy. Furthermore, we have shown that certain EMDR therapeutic instructions incorrectly reflect the scientific status of memory and that such instructions might even lead to certain expectations in recalling a memory very vividly. It goes without saying that en masse, fertile ground exists for EMDR therapy, contributing to false accusations of abuse. This situation can even become worse since in general, the role of therapists is not truth-centered.
Table 1: Components of EMDR and their problematic aspects.
This problematic contribution is, for example, exemplified by recent data from the Dutch Fictitious Memory Group (Werkgroep Fictieve Herinneringen). This is a group dealing with claims of people stating to have been falsely accused of a crime due to false memories. Shaw and Vredeveldt showed that from 2011 to 2018, 77% (n = 10) of potential false memory cases included some form of psychological therapy amongst others EMDR. Of course, EMDR is a highly popular treatment, so part of these data are caused by the fact that many patients undergo EMDR. Nonetheless, these data together with the discussed problematic aspects of EMDR (e.g., eye movements and therapists’ beliefs) create a potentially dangerous situation when after EMDR, patients file a complaint of abuse to the police. In such situations, it is highly relevant to be cognizant of the possibility that the accusation might be false.
So, what should memory experts say when they are asked about victims’ trauma memories (e.g., of childhood abuse) that follow EMDR therapy? Basically, there are two scenarios. In the first scenario, patients enter EMDR therapy and already have memories of past abuse. Here, EMDR may undermine memory. That is, eye movements can foment spontaneous false memories. Also, eye movements can decrease the vividness and emotionality of autobiographical experiences. Furthermore, and at least in the Dutch protocol, the video instruction can lead people to expect recalling a detailed account. In addition, therapists believing in repressed memories might ask suggestive questions to look for possible other abuse-related causes and discuss the possibility of repressed memories.
In the second scenario, patients start EMDR therapy without having any memory of trauma, but do display various mental health problems (e.g., anxiety and depressive feelings). Because EMDR therapists often believe in unconsciously repressed memories, patients might be cued in that direction and come to think that their symptoms are the result of repressed memories of abuse. This constellation of therapists’ and patients’ beliefs and actions might fuel false memory formation. In our expert witness work, we have seen a case in which a swim instructor was suspected of abusing children during swim lessons. After the suspicion began to circulate, parents became worried and started to interview their children. In one instance, a child who denied having had any negative experience with the teacher was sent to EMDR therapy by her parents nonetheless, for prophylactic purposes. If a child in this situation is subjected to EMDR, the hot spot memory is by definition an imagination, and subsequent memory work on this imagination falls arguably nothing short of fuel for imagination inflation (see Thomas & Loftus, Citation2002).
Of course, memory experts who work as expert witnesses mostly do not know which scenario is true during a legal case. Sometimes, in legal cases, information is available about whether a patient did or did not have any recollection concerning abuse before undergoing EMDR therapy that might make a certain scenario more plausible than the other. However, and more importantly, whatever the scenario, the current collection of research suggests that EMDR can negatively affect memory and hence, undermine the accuracy of testimony in legal cases.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Correction Statement
This article has been republished with minor changes. These changes do not impact the academic content of the article.
Additional information
Funding
References
- Arntz, A. (2012). Imagery rescripting as a therapeutic technique: Review of clinical trials, basic studies, and research agenda. Journal of Experimental Psychopathology, 3(2), 189–208. https://doi.org/https://doi.org/10.5127/jep.024211
- Bell, B. E., & Loftus, E. F. (1985). Vivid persuasion in the courtroom. Journal of Personality Assessment, 49(6), 659–664. https://doi.org/https://doi.org/10.1207/s15327752jpa4906_16
- Bernstein, D. M., Scoboria, A., Desjarlais, L., & Soucie, K. (2018). “False memory” is a linguistic convenience. Psychology of Consciousness: Theory, Research, and Practice, 5(2), 161–179. https://doi.org/https://doi.org/10.1037/cns0000148
- Brainerd, C. J., Reyna, V. F., & Ceci, S. J. (2008). Developmental reversals in false memory: A review of data and theory. Psychological Bulletin, 134(3), 343–382. https://doi.org/https://doi.org/10.1037/0033-2909.134.3.343
- Brainerd, C. J., & Mojardin, A. H. (1998). Children's and adults' spontaneous false memories: Long-term persistence and mere-testing effects. Child Development, 69(5), 1361–1377.
- Calvillo, D. P., & Emami, A. S. (2019). Do lateral eye movements increase susceptibility to misinformation? A registered replication. Psychonomic Bulletin & Review, 26(6), 1905–1910. https://doi.org/https://doi.org/10.3758/s13423-019-01641-6
- Christman, S. D., Garvey, K. J., Propper, R. E., & Phaneuf, K. A. (2003). Bilateral eye movements enhance the retrieval of episodic memories. Neuropsychology, 17(2), 221. https://doi.org/https://doi.org/10.1037/0894-4105.17.2.221
- Crews, F. (1995). The memory wars: Freud’s legacy in dispute. London, England: Granta Books.
- Cuijpers, P., Veen, S. C. V., Sijbrandij, M., Yoder, W., & Cristea, I. A. (2020). Eye movement desensitization and reprocessing for mental health problems: A systematic review and meta-analysis. Cognitive Behaviour Therapy, 49(3), 165–180. https://doi.org/https://doi.org/10.1080/16506073.2019.1703801
- Deese, J. (1959). On the prediction of occurrence of particular verbal intrusions in immediate recall. Journal of Experimental Psychology, 58(1), 17–22.
- de Jongh, A., & ten Broeke, E. (2016). Handboek EMDR: Een geprotocoleerde behandelmethode voor de gevolgen van psychotrauma [EMDR handbook: A treatment protocol for the consequences of psychotrauma]. Pearson.
- Dodier, O., Patihis, L., & Payoux, M. (2019). Reports of recovered memories of childhood abuse in therapy in France. Memory (Hove, England), 27(9), 1283–1298. https://doi.org/https://doi.org/10.1080/09658211.2019.1652654
- Felstead, K., & French, C. C. (in press). Dr James Ost’s contributions to the work of the British false memory society. Memory (Hove, England). https://doi.org/https://doi.org/10.1080/09658211.2021.1880600
- Greenberg, S. A., & Shuman, D. W. (1997). Irreconcilable conflict between therapeutic and forensic roles. Professional Psychology: Research and Practice, 28(1), 50–57. https://doi.org/https://doi.org/10.1037/0735-7028.28.1.50
- Houben, S. T. L., Otgaar, H., Roelofs, J., & Merckelbach, H. (2018). Lateral eye movements increase false memory rates. Clinical Psychological Science, 6(4), 610–616. https://doi.org/https://doi.org/10.1177/2167702618757658
- Houben, S. T. L., Otgaar, H., Roelofs, J., Merckelbach, H., & Muris, P. (2020a). The effects of eye movements and alternative dual tasks on the vividness and emotionality of negative autobiographical memories: A meta-analysis of laboratory studies. Journal of Experimental Psychopathology, 11(1), 2043808720907744. https://doi.org/https://doi.org/10.1177/2043808720907744
- Houben, S. T. L., Otgaar, H., Roelofs, J., Smeets, T., & Merckelbach, H. (2020b). Increases of correct memories and spontaneous false memories due to eye movements when memories are retrieved after a time delay. Behaviour Research and Therapy, 125, 103546. https://doi.org/https://doi.org/10.1016/j.brat.2019.103546
- Houben, S. T. L., Otgaar, H., Roelofs, J., Wessel, I., Patihis, L., & Merckelbach, H. (2019). Eye movement desensitization and reprocessing (EMDR) practitioners’ beliefs about memory. Psychology of Consciousness: Theory, Research, and Practice. https://psycnet.apa.org/doi/https://doi.org/10.1037/cns0000211
- Kanter, J. W., Kohlenberg, R. J., & Loftus, E. F. (2002). Demand characteristics, treatment rationales, and cognitive therapy for depression. Prevention & Treatment, 5(1), 41c. https://doi.org/https://doi.org/10.1037/1522-3736.5.1.541c
- Kaufmann, G., Drevland, G. C., Wessel, E., Overskeid, G., & Magnussen, S. (2003). The importance of being earnest: Displayed emotions and witness credibility. Applied Cognitive Psychology, 17(1), 21–34. https://doi.org/https://doi.org/10.1002/acp.842
- Kenchel, J. M., Domagalski, K., Butler, B. J., & Loftus, E. F. (in press). The messy landscape of eye movements and false memories. Memory (Hove, England). https://doi.org/https://doi.org/10.1080/09658211.2020.1862234
- Kensinger, E. A. (2007). Negative emotion enhances memory accuracy. Current Directions in Psychological Science, 16(4), 213–218. https://doi.org/https://doi.org/10.1111/j.1467-8721.2007.00506.x
- Lee, C. W., & Cuijpers, P. (2013). A meta-analysis of the contribution of eye movements in processing emotional memories. Journal of Behavior Therapy and Experimental Psychiatry, 44(2), 231–239. https://doi.org/https://doi.org/10.1016/j.jbtep.2012.11.001
- Leer, A., & Engelhard, I. M. (2020). Side effects of induced lateral eye movements during aversive ideation. Journal of Behavior Therapy and Experimental Psychiatry, 68, 101566. https://doi.org/https://doi.org/10.1016/j.jbtep.2020.101566
- Lilienfeld, S. O. (2007). Psychological treatments that cause harm. Perspectives on Psychological Science, 2(1), 53–70. https://doi.org/https://doi.org/10.1111/j.1745-6916.2007.00029.x
- Littel, M., van Schie, K., & van den Hout, M. A. (2017). Exploring expectation effects in EMDR: Does prior treatment knowledge affect the degrading effects of eye movements on memories? European Journal of Psychotraumatology, 8(sup1), 1328954. https://doi.org/https://doi.org/10.1080/20008198.2017.1328954
- Loftus, E. F. (1994). The repressed memory controversy. American Psychologist, 49(5), 443–445. https://doi.org/https://doi.org/10.1037/0003-066X.49.5.443.b
- Loftus, E. F., & Ketcham, K. (1994). The myth of repressed memory: False memories and allegations of sexual abuse. St. Martin’s Press.
- Lyle, K. B., & Martin, J. M. (2010). Bilateral saccades increase intrahemispheric processing but not interhemispheric interaction: Implications for saccade-induced retrieval enhancement. Brain and Cognition, 73(2), 128–134. https://doi.org/https://doi.org/10.1016/j.bandc.2010.04.004
- Lyle, K. B., & Orsborn, A. E. (2011). Inconsistent handedness and saccade execution benefit face memory without affecting interhemispheric interaction. Memory (Hove, England), 19(6), 613–624. https://doi.org/https://doi.org/10.1080/09658211.2011.595418
- Lynn, S. J., Kirsch, I., Terhune, D. B., & Green, J. P. (2020). Myths and misconceptions about hypnosis and suggestion: Separating fact and fiction. Applied Cognitive Psychology, 34(6), 1253–1264. https://doi.org/https://doi.org/10.1002/acp.3730
- Lynn, S. J., Lock, T., Loftus, E. F., Krackow, E., & Lilienfeld, S. O. (2003). The remembrance of things past: Problematic memory recovery techniques in psychotherapy. In S. O. Lilienfeld, S. J. Lynn, & J. M. Lohr (Eds.), Science and pseudoscience in clinical psychology (pp. 205–239). Guilford.
- Matzke, D., Nieuwenhuis, S., van Rijn, H., Slagter, H. A., van der Molen, M. W., & Wagenmakers, E. J. (2015). The effect of horizontal eye movements on free recall: A preregistered adversarial collaboration. Journal of Experimental Psychology: General, 144(1), e1–e15. https://doi.org/https://doi.org/10.1037/xge0000038
- Mazzoni, G., & Memon, A. (2003). Imagination can create false autobiographical memories. Psychological Science, 14(2), 186–188. https://doi.org/https://doi.org/10.1046/j.1432-1327.2000.01821.x
- McHugh, P. R. (2003). The end of a delusion: The psychiatric memory wars are over. Weekly Standard, 36(8), 31–34.
- McNally, R. J. (2005). Debunking myths about trauma and memory. The Canadian Journal of Psychiatry, 50(13), 817–822. https://doi.org/https://doi.org/10.1177/070674370505001302
- Merckelbach, H., & Wessel, I. (1998). Assumptions of students and psychotherapists about memory. Psychological Reports, 82, 763–770.
- Mertens, G., van Schie, K., Lammertink, S., Littel, M., & Engelhard, I. (2021). Verbal suggestions about treatment effectiveness do not modulate the effectiveness of a laboratory model of EMDR therapy: Results of two preregistered studies. Journal of Behavior Therapy and Experimental Psychiatry, 73, 101673.
- Morina, N., Lancee, J., & Arntz, A. (2017). Imagery rescripting as a clinical intervention for aversive memories: A meta-analysis. Journal of Behavior Therapy and Experimental Psychiatry, 55, 6–15. https://doi.org/https://doi.org/10.1016/j.jbtep.2016.11.003
- Moritz, S., Fieker, M., Hottenrott, B., Seeralan, T., Cludius, B., Kolbeck, K., Gallinat, J., & Nestoriuc, Y. (2015). No pain, no gain? Adverse effects of psychotherapy in obsessive–compulsive disorder and its relationship to treatment gains. Journal of Obsessive-Compulsive and Related Disorders, 5, 61–66. https://doi.org/https://doi.org/10.1016/j.jocrd.2015.02.002
- Nieuwenhuis, S., Elzinga, B. M., Ras, P. H., Berends, F., Duijs, P., Samara, Z., & Slagter, H. A. (2013). Bilateral saccadic eye movements and tactile stimulation, but not auditory stimulation, enhance memory retrieval. Brain and Cognition, 81(1), 52–56. https://doi.org/https://doi.org/10.1016/j.bandc.2012.10.003
- Ost, J., Blank, H., Davies, J., Jones, G., Lambert, K., Salmon, K., & Lu, L. (2013). False memory ≠ false memory: DRM errors are unrelated to the misinformation effect. PloS one, 8(4), e57939. https://doi.org/https://doi.org/10.1371/journal.pone.0057939
- Otgaar, H., & Candel, I. (2011). Children’s false memories: Different false memory paradigms reveal different results. Psychology, Crime & Law, 17(6), 513–528. https://doi.org/https://doi.org/10.1080/10683160903373392
- Otgaar, H., Howe, M. L., Patihis, L., Merckelbach, H., Lynn, S. J., Lilienfeld, S. O., & Loftus, E. F. (2019). The return of the repressed: The persistent and problematic claims of long-forgotten trauma. Perspectives on Psychological Science, 14(6), 1072–1095. https://doi.org/https://doi.org/10.1177/1745691619862306
- Parker, A., Buckley, S., & Dagnall, N. (2009). Reduced misinformation effects following saccadic bilateral eye movements. Brain and Cognition, 69(1), 89–97. https://doi.org/https://doi.org/10.1016/j.bandc.2008.05.009
- Parker, A., & Dagnall, N. (2007). Effects of bilateral eye movements on gist based false recognition in the DRM paradigm. Brain and Cognition, 63(3), 221–225. https://doi.org/https://doi.org/10.1016/j.bandc.2006.08.005
- Patihis, L., Cruz, C. S., & Herrera, M. E. (2019). Changing current appraisals of mothers leads to changes in childhood memories of love toward mothers. Clinical Psychological Science, 7(5), 1125–1143. https://doi.org/https://doi.org/10.1177/2167702619842468
- Patihis, L., Frenda, S. J., & Loftus, E. F. (2018). False memory tasks do not reliably predict other false memories. Psychology of Consciousness: Theory, Research, and Practice, 5(2), 140–160. https://doi.org/https://doi.org/10.1037/cns0000147
- Patihis, L., & Pendergrast, M. H. (2019). Reports of recovered memories of abuse in therapy in a large age-representative U.S. National sample: Therapy type and decade comparisons. Clinical Psychological Science, 7(1), 3–21. https://doi.org/https://doi.org/10.1177/2167702618773315
- Patihis, L., Wood, R. S., Pendergrast, M. H., & Herrera, M. E. (2020). Reports of recovered memories in therapy in undergraduate students. Psychological Reports, https://doi.org/https://doi.org/10.1177/0033294120971756
- Patihis, L., Ho, L. Y., Tingen, I. W., Lilienfeld, S. O., & Loftus, E. F. (2014). Are the “memory wars' over? A scientist practitioner gap in beliefs about memory. Psychological Science, 25, 519–530.
- Phaf, R. H. (2017). Eye movements enhance recollection of re-imagined negative words: A link between EMDR and SIRE? Journal of Experimental Psychopathology, 8(4), 364–375. https://doi.org/https://doi.org/10.5127/jep.059916
- Phelps, E. A., & Hofmann, S. G. (2019). Memory editing from science fiction to clinical practice. Nature, 572(7767), 43–50. https://doi.org/https://doi.org/10.1038/s41586-019-1433-7
- Qin, X.-J., Yang, H.-X., Cui, J.-F., Ye, J.-Y., & Wang, Y. (2021). Horizontal but not vertical saccades enhance memory retrieval: A meta-analysis and systematic review. Quarterly Journal of Experimental Psychology, 74(5), 801–811. https://doi.org/https://doi.org/10.1177/1747021821992276
- Richards, P. M., Geiger, J. A., & Tussey, C. M. (2015). The dirty dozen: 12 sources of bias in forensic neuropsychology with ways to mitigate. Psychological Injury and Law, 8(4), 265–280. https://doi.org/https://doi.org/10.1007/s12207-015-9235-1
- Roberts, B. R., Fernandes, M. A., & MacLeod, C. M. (2020). Re-evaluating whether bilateral eye movements influence memory retrieval. PloS One, 15(1), e0227790. https://doi.org/https://doi.org/10.1371/journal.pone.0227790
- Roediger, H. L., & McDermott, K. B. (1995). Creating false memories: Remembering words not presented in lists. Journal of experimental psychology: Learning, Memory, and Cognition, 21(4), 803–814
- Rozental, A., Kottorp, A., Boettcher, J., Andersson, G., Carlbring, P., & Georgantzis, N. (2016). Negative effects of psychological treatments: An exploratory factor analysis of the negative effects questionnaire for monitoring and reporting adverse and unwanted events. PLoS ONE, 11(6), e0157503. https://doi.org/https://doi.org/10.1371/journal.pone.0157503
- Samide, R., & Ritchey, M. (2020). Reframing the past: Role of memory processes in emotion regulation. Cognitive Therapy and Research, 1–10. https://doi.org/http://doi.org/10.1007/s10608-020-10166-5
- Shapiro, F. (1989). Efficacy of the eye movement desensitization procedure in the treatment of traumatic memories. Journal of Traumatic Stress, 2(2), 199–223. https://doi.org/https://doi.org/10.1002/jts.2490020207
- Shaw, J., & Vredeveldt, A. (2019). The recovered memory debate continues in Europe: Evidence from the United Kingdom, the Netherlands, France, and Germany. Clinical Psychological Science, 7(1), 27–28. https://doi.org/https://doi.org/10.1177/2167702618803649
- Thomas, A. K., & Loftus, E. F. (2002). Creating bizarre false memories through imagination. Memory & Cognition, 30(3), 423–431. https://doi.org/https://doi.org/10.3758/BF03194942
- van den Hout, M. A., & Engelhard, I. M. (2012). How does EMDR work? Journal of Experimental Psychopathology, 3(5), 724–738. https://doi.org/https://doi.org/10.5127/jep.028212
- van Schie, K., & Leer, A. (2019). Lateral Eye movements do not increase false-memory rates: A failed direct-replication study. Clinical Psychological Science, 7(5), 1159–1167. https://doi.org/https://doi.org/10.1177/2167702619859335
- Wade, N., & Tatler, B. (2005). The moving tablet of the eye: The origins of modern eye movement research. Oxford University Press.
- Wessel, I. (2018). Hoe denken VEN-leden over de betrouwbaarheid van het geheugen [What do members of the Dutch EMDR Committee know about the reliability of memory?]. EMDR Magazine, 17, 10–14.
- Wessel, E. M., Eilertsen, D. E., Langnes, E., Magnussen, S., & Melinder, A. (2016). Disclosure of child sexual abuse: Expressed emotions and credibility judgments of a child mock victim. Psychology, Crime & Law, 22(4), 331–343. https://doi.org/https://doi.org/10.1080/1068316X.2015.1109087