
Abstract
The economist Edgar Sydenstricker, who spent most of his working life at the United States Public Health Service and at the Milbank Memorial Fund, examined a wide range of health economics issues. He contributed to the debate around the cause of the disease pellagra. This research was followed by many studies quantifying income-related health inequalities. Sydenstricker was heavily involved in the use of surveys to collect information and he was instrumental in the development of the first US National Health Survey. Other contributions include extending health insurance in the United States and methods of evaluating public health programs.
1. Introduction
It has been customary to link the emergence of health economics as a discipline to the publication of Kenneth J. Arrow’s seminal contribution on “Uncertainty and the welfare economics of medical care” in the American Economic Review in 1963 (see, e.g., Fuchs Citation1989; Savedoff Citation2004). While we do not dispute the claim that Arrow’s article was a pivotal moment in the development of health economics, in this paper we highlight the much earlier work of the American economist and statistician Edgar Sydenstricker on health. Sydenstricker spent most of his working life at the United States Public Health Service (USPHS) and at the Milbank Memorial Fund. In his research he focussed in particular on the relation between economic conditions and health outcomes, and for this he remains relatively well-known in the field of social epidemiology (Susser and Stein Citation2009, 149–162). Especially his work on the link between poverty and pellagra, a disease that was causing a significant number of deaths in the south of the United States in the early part of the 20th century (Roe Citation1973), deserves attention here. Sydenstricker also worked on a wide range of economic issues, including health insurance and the evaluation of public health interventions. Nevertheless, he is largely unknown among economists and is not mentioned in surveys of health economics (Fuchs Citation1989; Wolfe Citation2018).
The primary goal of this paper is to introduce Sydenstricker’s work to historians of economics. Sydenstricker made pioneering contributions by collecting empirical evidence on the association between the socioeconomic environment and health and his work helped shed light on the true causes of pellagra. Moreover, his perspectives on the role of statistics in public health and empirical research offer lessons that are worth remembering today. The paper can also be seen as an addition to the literature on the history of applied economics by illustrating how economists in the first half of the 20th century dealt with the empirical challenges they faced.
The paper is structured as follows. After a brief biography (section 2), we present Sydenstricker’s early work on health inequalities among garment workers in New York (section 3). We then provide an overview of his work on the measurement of economic status and its role in the debate around the causes of pellagra (section 4). Next, we consider his efforts to develop a new methodology for the derivation of equivalence scales to enable comparisons between different households (section 5), and explore his views with regard to research methods and data collection (section 6). As far as the more policy-oriented aspects of Sydenstricker’s work are concerned, we focus on health insurance (section 7) and the evaluation of health interventions (section 8). We end with a discussion of Sydenstricker’s legacy and a few tentative conclusions (section 9).
2. Edgar Sydenstricker
Sydenstricker’s life and work have been well documented. For our short biographical sketch we draw mainly upon the obituary by King (Citation1936) and a memoir by Wiehl (Citation1974).Footnote1 Edgar Sydenstricker was born on 15 July 1881 in China, as the son of the American Presbyterian missionary Absalom Sydenstricker (1852–1931) and his wife Caroline, née Stulting (1857–1921). He was sent to the United States at the age of 15. He studied at Fredericksburg College in Virginia, where he earned an A.B. degree in 1900, and at Washington and Lee University, where he earned an M.A. degree in 1902. After a stint as high school principal and newspaper editor in Virginia, he went to the University of Chicago, where he was a post-graduate fellow in political economy in the academic year 1907–1908. He then started working for the United States Immigration Commission and the United States Commission on Industrial Relations, where he investigated the labour conditions in American industries. In 1915 he moved to the USPHS, where he worked as statistician under the direction of Benjamin S. Warren (1871–1935). They did research on the health and socioeconomic status of workers in the New York garment industry, and on health insurance systems. Between 1916 and 1920 he joined forces with Joseph Goldberger (1874–1929) to do path-breaking research on pellagra in the USA’s South. In 1918 he was called to Washington to work on influenza; together with Wade H. Frost (1880–1938) he collected data on the extent and severity of the Spanish Flu epidemic in the USA and explored whether the poor were hit more severely than the rich (Boianovsky and Erreygers Citation2021). In 1921 he initiated the Hagerstown Morbidity Studies, a wide-ranging survey of health and socioeconomic conditions of the population of Hagerstown (Md.). In 1923 he took a leave of absence to work for the League of Nations in Geneva. A few years later, in 1928, he joined the Milbank Memorial Foundation as Director of Research, becoming Scientific Director in 1935. In 1934–1935 he was a member of President Roosevelt’s Committee on Economic Security. He died suddenly on 19 March 1936. According to King (Citation1936, 414), he “came as near as a human being can to be being the perfect scientist.” Even though he was a well-known and highly respected epidemiologist, he was not the most renowned member of his family: that honour went to his sister Pearl S. Buck, who won the Nobel Prize in Literature in 1938.
Most of Sydenstricker’s writings deal with issues of public health, even though his first publications were on the history of Virginia (Sydenstricker and Burger Citation1914; Sydenstricker Citation1915). The research he did for the Committee on Industrial Relations led to a publication in the Journal of Political Economy (Sydenstricker Citation1916) and was extensively summarised in a book by Lauck and Sydenstricker (Citation1917). As far as his work for the USPHS is concerned, the main source of information is the large amount of papers he wrote for Public Health Reports, the weekly journal of the USPHS, in which he reported his findings. A fairly long survey on health insurance (Warren and Sydenstricker Citation1916a) was published in the Public Health Bulletin series. He contributed regularly to a wide variety of journals in medicine, economics and statistics. After joining the Milbank Memorial Fund he published frequently in the Milbank Memorial Fund Quarterly Bulletin. For the President’s Research Committee on Social Trends, initiated by Herbert Hoover and chaired by Wesley Clair Mitchell, he wrote the book Health and Environment (Sydenstricker Citation1933a). In 1974 Richard V. Kasius edited a selection of Sydenstrickers’s public health papers under the title The Challenge of Facts (Sydenstricker Citation1974).
3. The garment workers of New York City
At the request of the Joint Board of Sanitary Control of the Cloak, Suit and Skirt, and Dress and Waist Industries of New York City, the USPHS carried out a detailed health survey among the garment workers of New York City in 1914. The survey was directed by Joseph W. Schereschewsky (1873–1940), surgeon of the USPHS. He collected a large amount of data on 2,107 male workers from the cloak, suit and skirt industries, and on 1,000 female workers predominantly active in the dress and waist industries (Schereschewsky Citation1915, 19, 41). In total about 86,000 persons were employed in New York City’s garment industry (Schereschewsky Citation1915, 90), which means that the survey covered about 3.5% of the workforce. At the end of his extensive report on the health of these workers, most of whom were Jewish, he concluded that “the general condition of health of garment workers was by no means satisfactory” (Schereschewsky Citation1915, 97), and he singled out tuberculosis, defective vision, faulty posture and bad teeth as some of the most pressing health issues.Footnote2
Although he included data on the incomes of garment workers (Schereschewsky Citation1915, 23) and alluded to the adverse effects of poverty and to the existence of a “roughly” inverse relation between tuberculosis prevalence and income (Schereschewsky Citation1915, 98), in his report Schereschewsky refrained from an in-depth discussion of the relation between income and health. That topic was left to Warren and Sydenstricker, who used the same dataset to explore what Schereschewksy in his introduction to their report called “the self-evident relation between the economic status of the worker and his condition of health” (Schereschewksy 1916, 1298). Few public health specialists seemed to doubt that low wages and irregular employment had negative effects on health; there was, nevertheless, a lack of statistical evidence in support of this claim. In their study, Warren and Sydenstricker (Citation1916b) examined whether the data showed any evidence of the existence of a correlation between economic status (measured by incomes and regularity of employment) and ill-health (measured by child mortality rates and the prevalence of poor nutrition, anaemia and tuberculosis).
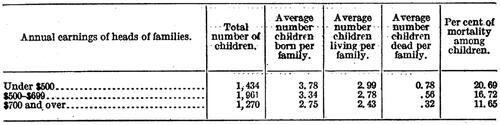
Warren and Sydenstricker assessed socioeconomic status by looking at the earnings of male married garment workers, considered as household heads and principal income earners of their families. They classified the 1,424 families into three income groups. While the average income of the highest group corresponded to what an average family of five persons (two adults, three children) needed “to maintain a healthful standard of living in New York City” (Warren and Sydenstricker Citation1916b, 1301), the incomes of those in the lowest income group were “plainly inadequate for maintaining healthful conditions of living” (Warren and Sydenstricker Citation1916b, 1302). They argued that this was a fairly robust classification of economic status.
Next, they calculated various health indicators for each of the three groups of families. With respect to child mortality, they found evidence for a clear negative correlation with income: in the lowest income group the mortality rate was almost twice as high as in the highest income group (see ). They pointed out (Warren and Sydenstricker Citation1916b, 1303n) that this was in line with findings of contemporary studies on infant mortality in Johnstown (Pa.) by Emma Duke (Citation1915), in Fall River (Mass.) by Louis Dublin (Citation1915), and in Birmingham (England) by John Robertson (Citation1913). They presented similar evidence for negative correlations between income and poor nutrition, income and anaemia, and income and tuberculosis. They also showed that income was positively correlated with employment regularity.
Figure 1. Social gradient in child mortality. Source: Warren and Sydenstricker (Citation1916b, 1303).
This was Sydenstricker’s first contribution to the measurement of socioeconomic inequality of health. There were many more to follow, but already in this relatively short paper we can discern a few salient characteristics of his work: fact-driven, well-documented and dispassionate. For instance, Warren and Sydenstricker (Citation1916b, 1305) resisted the temptation to draw causal inferences from their evidence on the association of income and health. Moreover, they abstained from using any advanced statistical techniques or jargon.
4. The measurement of economic status and the debate on the causes of pellagra
The study of the association between economic status and health runs as a constant thread through Sydenstricker’s work. It is typical for his meticulous approach that he realised that the measurement of economic status is not self-evident, and that using income for this purpose raises quite a few practical issues. As a result, in his early work Sydenstricker paid a lot of attention to the proper measurement of economic status. This research eventually led to the development of a new method to correct household incomes by equivalence scales (see section 5).
At first Sydenstricker relied on existing approaches with regard to the measurement of economic status. This is clear from two choices made by Warren and Sydenstricker in their analysis of the health of garment workers. The first was their decision to classify households according to the income of the male garment worker. They justified this choice by reference to data obtained from reports of the Federal Immigration Commission, which indicated that only a comparatively small minority of households had other income sources. They observed, for instance, that “about 4 per cent of Hebrew families had an income from the wives, and that the proportion of total family income from the earnings of wives was less than 1 per cent” (Warren and Sydenstricker Citation1916b, 1300, n. 2).
Since they chose to analyse income-related gradients by comparing statistics across categories of workers, the second issue they faced was to determine the cut-points for the annual earnings to denote low, medium and high income households. Again they relied on external evidence regarding the level of income required to maintain a “healthful standard of living” (Warren and Sydenstricker Citation1916b, 1301). For this they used earlier empirical studies on living conditions in New York, most notably the work of the economist Robert C. Chapin (1863–1913), who had been commissioned to write a report at the beginning of the 20th century (Chapin Citation1909a).Footnote3 Chapin’s report formed part of a long tradition dating back to late 18th century to measure consumption patterns at different levels of income.
Interestingly, Chapin made reference to the work of Wilbur Olin Atwater (1844–1907), which was to feature prominently in Sydenstricker’s development of an equivalence scale. Atwater was an American chemist, who allegedly introduced the word “calorie” into US English (Hargrove Citation2006). Through experimentation Atwater examined the amount of energy contained in different types of foods, and calculated and made estimates of the number of calories that needed to be consumed by humans to sustain life (Carpenter Citation1994). Chapin and later Sydenstricker used Atwater’s estimates of calories per day to define levels of minimum adequate income. To give an example:
The average cost of a well-balanced daily ration at the New York Marine Hospital for all inmates, including employees, was 35 cent per day in 1914. This ration is calculated to furnish 3,000 to 3,500 calories per day, an amount which is considered sufficient for a man at ordinary labor. On this basis, the annual cost for a family, as defined above (3.3 male units) would be $420. (Warren and Sydenstricker Citation1916b, 1301)
Using data from Chapin and other sources, Warren and Sydenstricker combined estimates of minimum food requirements with other aspects of consumption to get an estimate of the minimum adequate income for a worker in New York. This amounted to about $800-$900 per year (Warren and Sydenstricker Citation1916b), but they set the cut-off point for the highest category just under this level to allow for income from other family sources. They also explicitly noted that: “An additional fact to be considered is that the families in the lowest income group had a larger number of children per family than those in the two higher groups. This would tend to make the per capita income relatively smaller than that indicated by the statistics presented” (Warren and Sydenstricker Citation1916b 1302).
The issue of the accurate measurement of socioeconomic status became crucially important when Sydenstricker joined the USPHS team that studied pellagra and got involved in a debate about the causes of this disease. Nowadays pellagra is a rare and almost forgotten disease.Footnote4 Since the middle of the 18th century it was endemic in some regions of Europe, and at the beginning of the 20th century it was spreading fast in the southern states of the US, especially in the cotton-growing areas. Its main symptoms are severe irritations of the skin (the name pellagra comes from the Italian for “sour skin”), digestive problems and mental disorders, often indicated as the three D’s (dermatitis, diarrhoea and dementia), which could lead to death. The number of pellagra cases usually peaked in the spring, and mainly poor people were affected.
At the beginning of the 20th century the exact cause of the disease remained unknown. Two rival explanations were circulating: while the Thompson-McFadden Commission, a privately funded initiative for the study of pellagra, supported the view that pellagra was an infectious disease, a USPHS team led by Joseph Goldberger (1874–1929) was convinced that the disease was caused by a dietary deficiency, like scurvy and beriberi. The members of the Thomson-McFadden Commission derived support for their view from a large-scale epidemiological study in six villages in Spartanburg County, South Carolina (Siler, Garrison, and Macneal Citation1914, 373). Firmly believing that they had it wrong, Goldberger (Citation1914a, Citation1914b, Citation1916) and his associates (Goldberger, Waring, and Willets Citation1914, Citation1915; Goldberger and Wheeler Citation1915) provided evidence for the opposing view, but with little success (Siler, Garrison, and Macneal Citation1917a, Citation1917b). With the assistance of George A. Wheeler (1885–1981) and Sydenstricker, Goldberger therefore set up a similar epidemiological study as the one undertaken by the Thompson-McFadden Commission, taking great care to collect accurate data on food supplies, prices and incomes, at the village, household and individual levels.Footnote5 A first wave of surveys took place in 1916 and a second in 1917. In a series of papers, Goldberger, Wheeler, and Sydenstricker (Citation1918, Citation1920a, Citation1920b, Citation1920c) then argued that the analysis of the findings strongly suggested that pellagra was due to a dietary deficiency, but that they were unable to determine exactly which nutrient was crucial for the disease. The breakthrough came in 1937, when nicotinic acid (or niacin) was identified as the responsible vitamin (see the survey of the literature by Elvehjem Citation1940).
Sydenstricker played a crucial role in the collection of the survey data and in the analysis of the results (for more details, see Clarke and Erreygers Citation2023). Given the great variety in the size and composition of households, household food availability had to be expressed in comparable (i.e., “equivalent”) terms. For this they relied on Atwater’s scale of food requirements, which allowed the expression of household food availability in amounts per adult male unit (AMU). This procedure revealed that households with a high incidence of pellagra typically consumed much less animal protein foods, such as milk and fresh meat, than households without pellagra.Footnote6 The next step was to link the observed differences in diet to differences in socio-economic status. As in the case of food availability, this required the expression of household income into equivalent units. Again the Atwater scale was applied, but not without the observation that this was done in “the absence of a better common denominator for this purpose” (Goldberger, Wheeler, and Sydenstricker Citation1920c, 2683). It turned out that the incidence of pellagra varied markedly across income groups, with a strong negative correlation between the incidence rate of pellagra and income per AMU. The connections between pellagra, diet and equivalent income implied that policies aimed at improving the food availability for low income households and increasing income were called for (Goldberger, Wheeler, and Sydenstricker Citation1920c, 2710).
5. The development of equivalence scales
While collecting and interpreting the consumption and income data for the pellagra surveys, Sydenstricker came to the realisation that the existing approaches to adjust income for household composition were far from perfect. Together with another economist, Willford I. King, who had obtained a PhD from the University of Wisconsin on a study of income and wealth distribution in the US before joining the USPHS in 1917, Sydensticker published three articles describing in detail methods for the empirical measurement of equivalence scales. In one of these papers they explained how this new line of research came about, and how it related to the second wave of pellagra surveys conducted in 1917:
Observations made in 1916 during the progress of the field work led at least one of the investigators (E. S.) to believe that a fairly accurate rating of each individual as to economic status was essential to the solution of the problem at hand, namely, that of determining the forces giving rise to pellagra. Yet, despite the urgent demand for accurate information in this field, no thoroughly scientific method of obtaining an accurate classification of the population upon an income basis could be discovered in existence. It therefore became necessary to devise a plan which would accomplish this end. When, at the beginning of 1917, the other of the present writers (W. I. K.) joined the staff, the fundamental methods of procedure had already been put into practice. During 1917, however, a much more elaborate field study was carried on. It covered about 4,000 families, a number amply sufficient to give statistical regularity to the data obtained. (Sydenstricker and King Citation1921a, 573)
The fieldwork was divided into two components: the first involved scales to represent expenditure on food, and the second expenditure on all other goods (Sydenstricker and King Citation1921b, 845). The underlying reason for the division was that food was generally purchased for the household as whole, while many categories of other expenditure (e.g., clothing) could be allocated to specific individuals within the household (Sydenstricker and King Citation1920b, 2835).
In the case of food expenditure, their starting point was the size of the family expressed in AMUs, according to the Atwater scale, using males over the age of 16 that have the highest calorie needs as the reference point. They divided food expenditure by AMU and classified families according to approximate monthly income per AMU. For each family they determined its female percentage, which they then used to define subclasses within each of the income classes. They calculated average expenditures per AMU based on the sex-composition of the household. Empirically they found that the marginal expenditure on females was higher than accounted for in the Atwater scale, so they imposed a correction factor, which involved dividing the Atwater scale for females through by 0.964, to increase their relative importance in the resulting index (Sydenstricker and King Citation1921b, 846). A similar process was adopted to produce adjustments for food consumption at different ages. They referred to their new scale as fammain:
The term chosen was fammain, it being an abbreviation of the phrase food for adult male maintenance. The fammain may be accurately defined, for any given class of people, as a demand for food of a money value equal to that demanded by the average male in the given class at the age when the expense for his food reaches a maximum. (Sydenstricker and King Citation1921b, 847)
The second task was to develop scales for all other types of expenditure. This was again obtained from a fieldwork survey in which one member of each family (usually the housewife) allocated total expenses on categories such as clothing, medical expenses, recreation and schooling to each family member. With the “aid of a modified system of moving averages” they calculated “a curve for each sex showing the total amounts spent, on the average, for the individual benefit of persons of different ages” (Sydenstricker and King Citation1921a, 584).
Finally, they combined the fammain scales with the individual expenditures to produce scales representing a broad range of household expenditures. They termed these scales:
“ammain,” the word being an abbreviation of the phrase, adult male maintenance. The unit is defined as a gross demand for articles of consumption having a total money value equal to that demanded by the average male in the given class at the age when his total requirements for expense of maintenance reach a maximum. (Sydenstricker and King Citation1921a, 592)
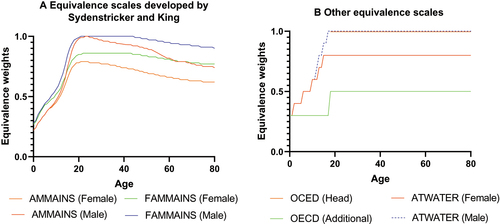
In we provide a graphical illustration of the ammain and fammain scales (panel A) alongside the Atwater and OECD-modified equivalence scales (panel B). As is visually apparent, the ammain and fammain scales differ from the Atwater scales, and have much greater variation by age and sex than the modern OECD scale, which does not distinguish between sexes and has only two levels related to age (i.e., children aged 14 and over are assigned a weight of 0.5 and children aged 0–13 a weight of 0.3).
Figure 2. Comparison of different equivalence scales. Source: The fammain, ammain and Atwater equivalence weights are based on those reported by Sydenstricker and King (Citation1921b, 850). The OECD weights are reported by Biewen and Juhasz (Citation2017).
An interesting application of the ammain concept can be found in a study of how the economic status of a wage earner changes throughout his life (Sydenstricker, King, and Wiehl Citation1924). The inspiration for this paper came from B. Seebohm Rowntree’s famous study on poverty in York, where he described the ups-and-downs of a typical labourer moving in and out of poverty throughout his life. Since the data were taken from the pellagra survey of 1917, what Sydenstricker, King and Wiehl were trying to do was to derive a longitudinal relationship from cross-sectional data. The economic status of a family and of its members was estimated by calculating the income per ammain. Households were grouped according to the number of years that had elapsed since marriage, and for each group the mean income per ammain was calculated. The variation in economic status over time could then be visualised by mapping the mean income per ammain as a function of the number of years since marriage. The results coincided to a large extent with those of Rowntree (Citation1902): for a few years after marriage, when husband and wife are both working, economic status is above the mean; as more children are born, economic status starts to decline; when the children reach the working age (around 14 years old), economic status rises again. With regard to the economic status of children and of older people, the results of the two studies are slightly different.
Sydenstricker, King and Wiehl drew one specific and one general conclusion from their study. The specific conclusion related to the incidence profile of pellagra in the cotton mill communities where the survey was held. Given the association between the incidence of pellagra and poverty, “the peculiar age incidence of pellagra may have been determined in some measure by the age incidence, so to speak, of low income under the particular conditions of food supply prevailing at the time in these communities” (Sydenstricker, King, and Wiehl Citation1924, 2139). Apart from that, they observed, “our study goes no further than to outline the general character of the “economic cycle” in the lives of an actual wage-earning population and to indicate that at certain periods in the lives of such population the pressure of economic conditions is measureably greater than at other periods. That it may be sufficient to affect the well-being of the persons concerned is a possible corollary that should be kept in mind” (Sydenstricker, King, and Wiehl Citation1924, 2139–2140).
On the whole, however, it must be said that the ammain and fammain equivalence scale approach had little success (see Clarke and Erreygers Citation2023). The lukewarm analysis by William F. Ogburn (Citation1931) provides an illustration of how the ideas of Sydenstricker and King were received. Ogburn acknowledged that the new equivalence scales might be more accurate than the Atwater scale, but doubted whether the gain in accuracy was large. By contrast, a much more sympathetic reception was the one by Milton Friedman (Citation1952).Footnote7 Friedman saw the framework of Sydenstricker and King’s as a good starting point to propose an alternative regression-based approach, but he never got further than sketching a rough outline.
6. Research methodology
As a statistician employed by the USPHS, Sydenstricker had the duty to ensure that the studies in which he was involved were methodologically sound. Unfailingly, he described in detail how the data had been collected and measured, and whether anything essential might have been overlooked in the process. When looking for correlations and causal connections, he almost always proceeded by calculating means or medians for relevant groups, e.g., by sex or income class, and presenting the data in tables and figures. He seems to have been very reluctant to use coefficients of correlation in order to identify patterns of correlation, let alone of causation, and it is striking to see how sparingly they occur in his work on health inequalities. In his studies on pellagra, for instance, coefficients of correlation are mentioned only in an article which focuses on the role of low incomes. He presented a coefficient of correlation equal to −0.91 ± 0.05 as supporting evidence of the inverse relation between household income (expressed per adult male) and the incidence of pellagra (Goldberger, Wheeler, and Sydenstricker Citation1920c, 2686, n13). In his discussion of this result, however, he also pointed out that the relation between the proportion of low-income households and the incidence of pellagra in each of the seven villages was much weaker, as illustrated by a coefficient of correlation equal to 0.33 ± 0.23 (Goldberger, Wheeler, and Sydenstricker Citation1920c, 2695). This prompted further analysis, and that eventually showed that it was the combination of low incomes with other economic factors which led to high levels of pellagra:
The most potent factors influencing pellagra incidence in the villages studied were (a) low family income, and (b) unfavorable conditions regarding the availability of food supplies, suggesting that under the conditions obtaining in some of these villages in the spring of 1916 many families were without sufficient income to enable them to procure any adequate diet, and that improvement in food availability (particularly of milk and fresh meat) is urgently needed in such localities. (Goldberger, Wheeler, and Sydenstricker Citation1920c, 2712)
Coefficients of correlation also occur in a study of the heights and weights of school children (Clark, Sydenstricker, and Collins Citation1922, 1201–1202).
Sydenstricker’s own reflections on the role of statistics in public health research confirm his reservations about statistical correlation analysis. He maintained that statistical analysis was absolutely indispensable in order to deal with a mass of facts; scientists therefore had to be statisticians. But they also had to be specialists in their own fields: “the expert in pure statistical technique (…) is a dangerous person to be let loose in fields of facts with which he is unacquainted” (Sydenstricker Citation1928b, 119). This applied in particular to scientific research based on experiments, of which he was a vocal advocate. He emphasised that great care should be taken to measure all the factors at play in an “objective, quantitative and valid” way (Sydenstricker Citation1928a, 157). Unfortunately, this was not always the case: “apparently there is an unfortunate misconception, not infrequently manifested, of the use of partial and multiple correlation, for example, which seems to express itself in great precision as to decimal numbers and probable errors but exhibits a readiness to use rather rough and not very relevant indices of the factors to be taken into account” (Sydenstricker Citation1928a, 157). Valid conclusions could only be obtained by a proper understanding of the subject. Warnings against overreliance on coefficients of correlation were also a recurrent theme in Sydenstricker (Citation1933a, 5, 10, 46, 85, 89–90, and 104–105).
With regard to the collection of data, Sydenstricker was very much in favour of carefully designed surveys and field studies. This is perhaps best illustrated by the Hagerstown Morbidity Studies which he initiated and directed for the USPHS. From 1 December 1921 to 31 March 1924 a general survey of illness was carried out in Hagerstown, Maryland. About 8,500 of the town’s 30,000 inhabitants were included in the survey, with about 3,200 persons being monitored over the whole 28 months (Sydenstricker Citation1926, 2071). The aim was to find out the incidence of illnesses among the general population. Sydenstricker reported on his findings in a series of eleven papers in Public Health Reports. He dealt with the economic aspects in the last two studies of the series. Every household which participated in the study was classified into one of five categories of economic status: “well-to-do,” “comfortable,” “moderate,” “poor” and “very poor.” That allowed the exploration of the association between economic status and health. As far as the incidence of illness and access to medical care were concerned, the evidence pointed to a social gradient: “Two facts remain fairly clear (…) – one is that the illness rate as observed was higher for the poor than for those economically better off; the other is that, in general, those families which were definitely above the average of this community in economic condition had medical attention to a considerably greater extent than the remainder of the population” (Sydenstricker Citation1929a, 1833). Unsurprisingly, the study also found that infant mortality was higher among the poor than among the rich (Sydenstricker Citation1929b, 2106).
Another example of Sydenstricker’s data collection initiatives is provided by his research on the influenza epidemic of 1918–1919. Jointly with epidemiologist Wade Hampton Frost (1880–1938) he conducted a survey among more than 100,000 persons in various locations in the US. This led to a series of publications providing statistical information on the extent and severity of the epidemic (Sydenstricker Citation1918; Frost and Sydenstricker Citation1919a, Citation1919b; Frost Citation1919; Sydenstricker Citation1921) and discussing the difficulties of calculating the civil death rates for 1918, mainly as a result of war-related movements of the population (Sydenstricker and King Citation1920a). The work of Frost and Sydenstricker was well received (Vaughan Citation1921). The biologist and statistician Raymond Pearl (1879–1940), who was one of the first to try and explain the epidemic by means of a quantitative analysis (Pearl Citation1919), even changed the definition of his variable measuring the explosiveness of the epidemic when he realised that their work implied a criticism of the choice he had made (Pearl Citation1921, 276). Remarkably, Sydenstricker waited more than ten years before he published a paper on the relation between income and influenza based on this survey. The study was meant as an examination of the claim that “the flu hit the rich and the poor alike” (Sydenstricker Citation1931, 154) Although he measured economic status by means of a “crude” classification of households into four categories (“well-to-do,” “moderate,” “poor” and “very poor”), in his analysis he mostly grouped the first two categories and the last two categories together. As with many other diseases, in this case too the evidence pointed to a social gradient. It should be noted, however, that Sydenstricker was not jumping to conclusions as far as causes were concerned:
The discovery of an association of relatively high influenza incidence with poor economic condition does not, by any means, invest poor economic condition with causal significance. It points to the probability that the incidence of the disease is influenced by one or more of the many factors that are themselves bound up, causally or otherwise, with the economic status of a population. (…) The correlation merely suggests that some of these conditions may have a bearing on the question. (Sydenstricker Citation1931, 161)
7. Health insurance
The increasing industrialisation of the US in the beginning of the 20th century and the growth of wage employment raised the issue of how wage earners could be protected against the adverse effects of illness. Through his research on the health of garment workers Sydenstricker knew very well that economic conditions and health were strongly connected: illness and disability led to loss of income, and a low income made access to health care difficult or impossible. The successful introduction of forms of illness insurance in a few European countries inspired Warren and Sydenstricker (Citation1916a, 5) to write “a brief survey of the relation of health insurance to the health of the wage earner” and to explore whether something similar might be introduced in the US. Their report provided a lot of evidence on the extent of illness and its economic burden; e.g., given that the average wage earner lost nine days per year due to illness, the loss of wage was equal to $2 per day and the cost of medical care amounted to $1 a day, they estimated that the total annual loss of income for wage earners was about three quarters of a billion $ (Warren and Sydenstricker Citation1916a, 68–69). They argued in favour of the introduction of a shared-responsibility health insurance system involving wage earners, employers and the public, aimed not only at distributing the costs of illness over these groups, but also at providing financial incentives for the prevention of illness. As the experience in other countries had shown, such a national or State-level system could integrate the agencies that already existed in terms of health insurance. In sum: “A governmental system of health insurance can be adapted to American conditions, and when adapted will prove to be a health measure of extraordinary value” (Warren and Sydenstricker 1916, 70).
But the times were not ripe for a such a reform. The early health insurance campaign ended “in complete disaster in 1920” (Falk Citation1974, 100) when the American Medical Association sided with the opponents of health insurance. For several years Sydenstricker did not write about the topic anymore. From 1927 to 1932 he was a member of the Committee on the Costs of Medical Care, a private organisation of medical care experts (Falk Citation1974, 101). In its final report the committee recommended that more health care should be provided through group practices, that all basic public health care services should be extended, and that health care financing should be based on group payment, i.e., insurance, taxation or a combination of both (Committee on the Costs of Medical Care Citation1932, xvi). For some the recommendations with regard to the organisation of medical care and health care financing went much too far (see, e.g., the Minority Report Number One, Committee on the Costs of Medical Care Citation1932, 151–183). For Sydenstricker, however, they did not go far enough, and in a brief personal statement he declared that “the recommendations do not, in my opinion, deal adequately with the fundamental economic question which the Committee was formed primarily to study and consider” (Committee on the Costs of Medical Care Citation1932, 201). He explained later which objectives he wanted to achieve, and argued that voluntary steps in the direction of group practice should be complemented with the introduction of a compulsory health insurance system (Sydenstricker Citation1934).
In the years that followed the debate on health insurance re-surfaced as a result of the Great Depression and the presidency of Franklin D. Roosevelt, and Sydenstricker became one of the main participants. When Roosevelt in 1934 created the Committee on Economic Security, Sydenstricker was appointed as the director of study of the Health Insurance Staff, with the task of studying the risks due to illness and of formulating solutions for better protection against these risks (Falk Citation1974, 97–98). Sydenstricker managed to broaden the scope of his inquiry, so that he and his associates could in fact propose an ambitious national health program, including health insurance. However, not all of the recommendations of Sydenstricker’s group were embraced by the Committee on Economic Security and just a few of them found their way into the Social Security Act of 1935 (Falk Citation1974, 98). In particular the proposals with regard to health insurance were seen as too controversial and as potentially endangering the whole social security project of the Roosevelt administration. The final report of Sydenstricker’s group was not made public and the health insurance proposal never made it to Congress, in what some have described as “the missed opportunity” and “the lost reform” (Falk Citation1974, 105–106). Although obviously disappointed, Sydenstricker himself continued to defend his health insurance ideas before and after the adoption of the Social Security Act (Sydenstricker Citation1935, Citation1936a, Citation1936b, Citation1936c), until his premature death in March 1936.
8. Evaluation of public health interventions
Following his work on both pellagra and influenza, Sydenstricker was appointed Chief of the Office of Statistical Investigations in 1920, which allowed him to expand the scope of his research over the next decade (Wiehl Citation1974, 7–8). This included studies involving large scale data collection to look at the health of school children (Clark, Sydenstricker, and Collins Citation1922) and a detailed longitudinal data collection known as the Hagerstown Morbidity Survey (discussed above), which built on the methods employed in the study of pellagra to obtain measures of incidence of a wide range of diseases over time (Sydenstricker Citation1926).
In 1925 he was approached by the Milbank Memorial Fund who sought his advice on how to evaluate public health interventions it was funding, such as its anti-tuberculosis programs (Kiser et al. Citation1971). This led to a series of methodological and empirical contributions on the measurement of the outcome of public health programs and their evaluation. His first foray into this field was to provide an overview of the issues in a paper entitled “The measurement of results of public health work. An introductory discussion” (Sydenstricker Citation1927) which he “regarded as an essential step” in the evaluation of new public health programs. The centrepiece of this article was to enunciate a series of principles: (i) to focus on specific activities rather than the program as a whole; (ii) to clearly define objectives and outcomes; (iii) to use what would now be termed quasi-experimental methods including the use of controls.
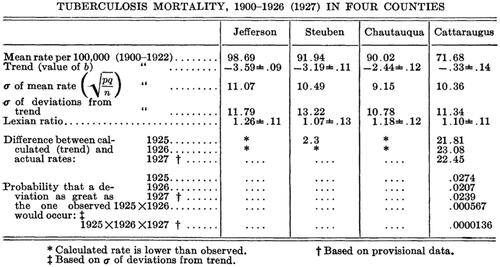
Sydenstricker applied these principles in his evaluation of the Milbank Memorial Fund’s anti-tuberculosis intervention in Cattaraugus County, New York. This consisted mainly of “a modern anti-tuberculosis administration” (Sydenstricker Citation1928a, 160) practicing “modern principles and procedures of tuberculosis prevention, relief and cure” (Sydenstricker Citation1928c, 41). He observed early on that the death-rate from tuberculosis had been declining and so the effect of an intervention could not be identified simply by comparing the tuberculosis death rates in this county before and after the intervention. The outcome in the experimental group had to be compared to the outcome in one or more control groups, and Sydenstricker emphasised that “the ‘control’ population groups shall be in all essential and relevant respects the same as the experimental group, save in the one respect which constitutes the thing to be tested or measured” (Sydenstricker Citation1928a, 158). After selecting three other counties in New York State as control groups for Cattaraugus County, Sydenstricker made a comparative analysis in which he first calculated the trend of tuberculosis mortality in each county by fitting linear trend lines to the death rates from 1900 to 1927 (see ), and then used these results to test whether the differences between the trend and the actual rates during the period of the intervention (1925–1927) were statistically significant (see ). His conclusion was that in Cattaraugus County the observed decline in the tuberculosis death rate during the period of the intervention constituted a significant deviation from the trend, while in the control groups no significant deviation from the trend occurred (Sydenstricker Citation1928a, 162).
Figure 3. Trends of tuberculosis death rates across counties in New York State. Source: Sydenstricker (Citation1928a, 161)
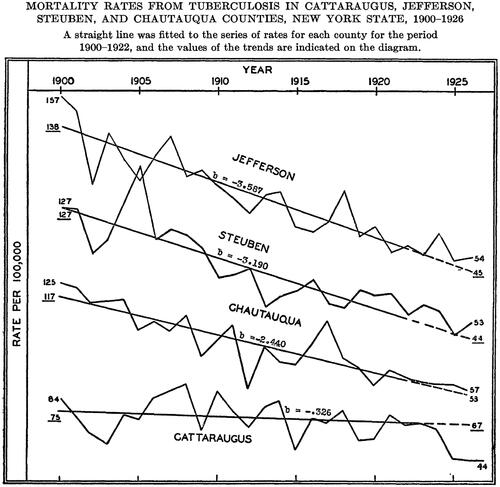
Figure 4. Statistical analysis of tuberculosis death rates. Source: Sydenstricker (Citation1928a, 161).
It is worth noting that this part of Sydenstricker’s research shows that he did not hesitate to apply advanced statistical methods if the topic required it. In his earlier work he relied predominantly on simple graphs and tables to derive conclusions from his empirical work. What we see here, however, is that for the evaluation of public health programs he opted for a more rigorous statistical approach. Sydenstricker’s efforts to develop a scientifically sound framework to evaluate large programs anticipate the quasi-experimental methods for policy evaluation developed by economists many decades later (see, e.g., Meyer Citation1995). His proposed solutions of using deviations from trend in the intervention vs. control groups has parallels with modern econometric methods such as difference-in-difference.Footnote8
The final phase of Sydenstricker’s research was influenced by the effects of the Great Depression. Sydenstricker was heavily involved with the efforts to collect data at an individual and household level to understand the impact of the depression. These efforts built on previous studies of the USPHS (with assistance from the Milbank Memorial Fund), and again used field surveys involving house-to-house canvassing to gather data on more than 10,000 families (Sydenstricker Citation1933b). The information collected covered both epidemiological and economic aspects and included records of illness and mortality, information on diet and housing conditions, physical examinations of school children of selected families, and information about current and pre-depression income.
The analysis of the surveys showed that households with the largest declines in income had the highest levels of sickness. Sydenstricker was very much interested in the direction of causality. In the article “Causal and selective factors in sickness” Perrott and Sydenstricker (Citation1935) offered a detailed discussion of this and explored whether the high rates of illness in families with the greatest income losses are caused by the income changes, or whether there is a selection process, in the sense that households with pre-existing illness were less able to remain employed as the economy contracted. They argued that focussing on the impacts on the health of both adults and children helps identify the causal effects of family income loss due to unemployment. Such reasoning parallels recent analyses of the effects of economic downturns; Schaller and Zerpa (Citation2019), for example, have used US data for the period 1996–2012, which includes the Great Recession, to study how parental job loss affects child health.
Sydenstricker was also instrumental in the design and establishment of the US National Health Survey (NHS) conducted in 1935 and 1936. This survey was a massive undertaking covering around 2.8 million people in 19 states with data being collected by 6000 unemployed workers at an initial cost of 3.5 million dollars (Weisz Citation2011). Again a key focus of this survey (an initial draft of which was developed by Sydenstricker) was on understanding rates of illness by income and on quantifying the impact of the Depression.
Those working on the USPHS and NHS surveys were very much aware of the divergent trends occurring during the depression: while overall rates of mortality were falling, they were observing a rise in morbidity for families who had lost income (Perrott and Collins Citation1935). Capturing this broader picture of population health was why they needed to undertake large morbidity surveys, as Sydensticker (1933 b) noted that the “incidence of sickness may be accepted as a more delicate index of ill health than mortality.”
One can contrast Sydensticker’s efforts with recent studies of the impact of business cycles on population health, which are dominated by the analysis of correlations between overall levels of economic activity and mortality statistics (e.g., Lam and Piérard Citation2017). Even re-analyses of the Great Depression, such as Tapia Granados and Diez Roux (Citation2010), focus entirely on mortality and make no reference to the USPHS or NHS studies focussing on illness. Such analyses are most likely constrained by available data; without access to large longitudinal surveys that collect both health and economic data, aggregate mortality statistics are often all that can be used to track changes in population health during economic downturns.
We already pointed out that the Social Security Act of 1935, which the US Congress passed as part of President Roosevelt’s New Deal, did not include Sydenstricker’s health insurance proposals. But it did include substantial appropriations for both public and child health, and Sydenstricker (Citation1936a, 17) noted that these measures “constitute probably the greatest single step forward in the development of a national public health program” in the US. In one of his final contributions Sydenstricker turned to how economic evaluation can help inform the allocation of funds flowing into public health, highlighting that “appropriations of public funds for public health place upon health authorities a very definite responsibility for the effective use of the money” (Sydenstricker Citation1936b, 7). Making reference to Charles V. Chapin’s (Citation1917) seminal attempt to use an economic approach to evaluate public health interventions, Sydenstricker observed that interventions which were in fact ineffective (such as disinfection and fumigation of houses where infections had occurred, as Chapin had shown in his study) often tended to be favoured over more cost-effective alternatives. As an example of the type of question that needed to be addressed Sydenstricker asked:
What are the scientific bases or the actual experience upon which are based some of our public health standards? We call for eight visits of a public health nurse to each and every case of whooping cough. This standard, as is well known, is rarely measured up to and more than one health officer has asked himself the question: What evidence is there of prevention of mortality from or reduction in incidence of whooping cough by eight visits rather than by four or two or one? (Sydenstricker Citation1936b, 10)
Furthermore, Sydenstricker argued that evidence should directly inform allocation decisions, noting in particular with regard to the measures included in the Social Security Act that it was the intention of the staff members and advisers of the Committee on Economic Security that “this program should be limited to federal aid for public health procedures of proven value” (Sydenstricker Citation1936b, 12). Central to Sydenstricker’s proposals was that substantial funds be set aside so that evaluation could be conducted of new public and child health programs. He pointed out that the staff of the Committee had this function in mind when it proposed to the Committee that $2,000,000 per year (i.e., around 15% of the funds allocated by Congress for the program) should be appropriated for research and personnel to “undertake and encourage the task of testing public health methods” (Sydenstricker Citation1936b, 11). Unfortunately, while this provision ended up in the Social Security Act passed by Congress in 1935, it required annual appropriations by Congress and the actual amounts allocated were consistently below what had been envisaged (Swain Citation1962). This, in combination with his sudden death in 1936, meant that Sydenstricker’s vision for evidence-based policy formation in US public health did not come to pass.
9. Legacy and conclusions
Given Sydenstricker’s substantive economic contributions it is surprising how little influence his work had on the next generation of health economists that emerged after the Second World War. Take for example Selma J. Mushkin (1913–1979), who worked as an economist in the USPHS in the period 1949–1960 (Cicarelli and Cicarelli Citation2003, 136) and tried to define the scope of health economics as a discipline in the late 1950s (Mushkin Citation1958). Her outline contains a brief history of health economic contributions made to date by a wide variety of economists. Acknowledging that traces of the application of cost-benefit ratios to evaluate health care programs can be found in the work of Jean Bodin, Richard Cantillon and Adolphe Quetelet, she noted nevertheless: “Economic studies of cost-benefit ratios of health programs have been carried out largely by health administrators and others in the health professions rather than by economists” (Mushkin Citation1958, 788). Her paper contains no reference to any of Sydenstricker’s attempts to develop an economic framework for the evaluation of public health interventions by the USPHS just over twenty years earlier. Instead, she highlighted the new impetus given to health cost-benefit analysis after the Second World War thanks to the work of Charles-Edward A. Winslow (Citation1951) and Gunnar Myrdal (Citation1952).
Similarly none of Sydenstricker’s papers are referenced in the seminal contribution of Arrow (Citation1963) or in Klarman (Citation1965), the first health economics textbook. There appears to have been no knowledge of his work among those shaping the new emerging discipline from the 1960s onward.Footnote9 What can account for this? While Sydenstricker made many economic contributions, he was formally employed as statistician by the USPHS and later as an advisor and administrator by the Milbank Memorial Fund. Following his death in 1936 there appears to have been little capacity in either institution to continue with the program of health economic research he had initiated. Hence, many of his insights have been lost only to be rediscovered decades later.
By contrast, as the posthumously published volume of a selection of his work (Sydenstricker Citation1974) shows, Sydenstricker’s contributions are well recognised in social epidemiology. There is, however, currently no broad overview of his economic work. We have attempted to address this by reviewing and summarising his key health economic contributions. Like many health economists today, Sydenstricker adopted a multidisciplinary approach and focussed on finding solutions to what were contemporary health problems. Unlike many economists of his time, he was able to employ considerable resources, such as fieldwork experiments in different settings involving the collection of substantial amounts of economic data, including detailed surveys of household expenditures and incomes. He contributed to setting up the US National Health Survey, which collected information on several million US citizens. Because of his pioneering contributions he certainly deserves a place in the history of health economics.
Acknowledgements
A previous version of the paper was presented at the 2016 HES conference and at a seminar in the University of Antwerp. We would like to thank Peter Siminski for comments on this manuscript, and we are very grateful to the reviewers for their valuable comments and suggestions.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Notes
1 Both Willford I. King (1880–1962) and Dorothy G. Wiehl (1895–1980) were former collaborators of Sydenstricker.
2 A second report focused exclusively on problems of illumination in workplaces where most of the women were employed (Schereschewsky and Tuck Citation1915).
3 Chapin appears to have made the most of this research. He used it to obtain a PhD at Columbia University, and he summarised it in an article which he managed to get published in identical form in both the American Journal of Sociology (Chapin Citation1909b) and in the American Economic Association Quarterly (Chapin Citation1909c).
4 The literature on pellagra is vast. Our account is based upon Etheridge (Citation1972) and Roe (Citation1973).
5 The differences between the two surveys are explained in detail by Mooney, Knox and Morabia (Citation2014).
6 Animal-based foods such as poultry, beef and fish are among the high sources of niacin per serving (https://ods.od.nih.gov/factsheets/Niacin-HealthProfessional/).
7 As Friedman explained in a preliminary note: “This paper was written in 1935 when I was a member of a group working under the direction of Hildegarde Kneeland at the National Resources Committee on plans for the Consumer Purchases Study and for the analysis of the consumption data it was expected to yield. (…) I planned to do further work on the problem but I never did and so the paper remained buried in my files” (Friedman Citation1952, 9). The manuscript is conserved in the Milton Friedman Papers at the Hoover Institution.
8 Lechner (Citation2010) provides an historical overview of difference-in-difference methods. While the approach can be traced as far back John Snow’s work in the 1850s on the causes of cholera, it was only sporadically used by economists until the last few decades. Sydenstricker contributions are not covered in Lechner’s historical review.
9 Prof Joseph Newhouse and Prof Martin Feldstein have also indicated no awareness of Sydenstricker’s health economic research in correspondence with one of the authors.
References
- Arrow, K. J. 1963. “Uncertainty and the Welfare Economics of Medical Care.” American Economic Review 53 (5): 941–973.
- Biewen, M, and A. Juhasz. 2017. “Direct Estimation of Equivalence Scales and More Evidence on Independence of Base.” Oxford Bulletin of Economics and Statistics 79 (5): 875–905. doi:10.1111/obes.12166.
- Boianovsky, M, and G. Erreygers. 2021. “How Economists Ignored the Spanish Flu Pandemic in 1918-1920.” Erasmus Journal for Philosophy and Economics 14 (1): 89–109. doi:10.23941/ejpe.v14i1.549.
- Carpenter, K. J. 1994. “The Life and Times of W.O. Atwater (1844-1907).” The Journal of Nutrition 124 (9 Suppl): 1707S–1714S. doi:10.1093/jn/124.suppl_9.1707S.
- Chapin, R. C. 1909a. The Standard of Living among Workingmen’s Families in New York City, New York: Charities Publication Committee.
- Chapin, R. C. 1909b. “The Influence of Income on Standards of Life.” American Journal of Sociology 14 (5): 638–647. doi:10.1086/211728.
- Chapin, R. C. 1909c. “The Influence of Income on Standards of Life.” American Economic Association Quarterly 3rd Series, 10 (1): 180–192.
- Chapin, C. V. 1917. “The Relative Values of Public Health Procedures.” Journal of the American Medical Association LXIX (2): 90–95. doi:10.1001/jama.1917.02590290012004.
- Cicarelli, J, and J. Cicarelli. 2003. Distinguished Women Economists, Westport: Greenwood.
- Clark, T., E. Sydenstricker, and S. D. Collins. 1922. “Heights and Weights of School Children: A Study of the Heights and Weights of 14,335 Native White School Children in Maryland, Virginia, and North and South Carolina.” Public Health Reports (1896-1970) 37 (20): 1185–1207. doi:10.2307/4576394.
- Clarke, P, and G. Erreygers. 2023. “Edgar Sydenstricker, equivalence scales and pellagra: when economics helped establish that a disease was not infectious,” forthcoming.
- COMMITTEE ON THE COSTS OF MEDICAL CARE 1932. Medical Care for the American People, Publications of the Committee on the Costs of Medical Care No. 28, Chicago: University of Chicago Press.
- Dublin, L. 1915. “Infant Mortality in Fall River, Massachusetts – a Survey of the Mortality among 833 Infants Born in June, July, and August 1913.” Publications of the American Statistical Association 14 (110): 505–520. doi:10.2307/2964866.
- Duke, E. 1915. Infant Mortality. Results of a Field Study in Johnstown, Pa., Based on Births in One Calendar Year (Children’s Bureau, Infant Mortality Series No. 3), Washington: Government Printing Office.
- Elvehjem, C. A. 1940. “Relation of Nicotinic Acid to Pellagra.” Physiological Reviews 20 (2): 249–271. doi:10.1152/physrev.1940.20.2.249.
- Etheridge, E. W. 1972. “The Butterfly Caste. A Social History of Pellagra in the South (Contributions in American History.” Number 17), Westport: Greenwood.
- Falk, I. S. 1974. “Commentary.”, in: R.V. Kasius (Ed.), The Challenge of Facts. Selected Public Health Papers of Edgar Sydenstricker, New York: Milbank Memorial Fund, 95–107.
- Friedman, M. 1952. “A Method of Comparing Incomes of Families Differing in Composition.” in Studies in Income and Wealth, Volume 15, Cambridge: NBER, 9–24.
- Frost, W. H. 1919. “The Epidemiology of Influenza.” Journal of the American Medical Association 73 (5): 313–318. doi:10.1001/jama.1919.02610310007003.
- Frost, W. H, and E. Sydenstricker. 1919a. “Influenza in Maryland: Preliminary Statistics of Certain Localities.” Public Health Reports (1896-1970) 34 (11): 491–504. doi:10.2307/4575056.
- Frost, W. H, and E. Sydenstricker. 1919b. “Epidemic Influenza in Foreign Countries.” Public Health Reports (1896-1970) 34 (25): 1361–1376. doi:10.2307/4575202.
- Fuchs, V. R. 1989. “Health Economics.” in J.E. Eatwell, M. Millgate and P. Newman (Eds), Social Economics (the New Palgrave: A Dictionary of Economics), London: Macmillan, 119–129.
- Goldberger, J. 1914a. “The Etiology of Pellagra: The Significance of Certain Epidemiological Observations with Respect Thereto.” Public Health Reports (1896-1970) 29 (26): 1683–1686. doi:10.2307/4570920.
- Goldberger, J. 1914b. “The Cause and Prevention of Pellagra.” Public Health Reports 29 (37): 2354–2357.
- Goldberger, J. 1916. “The Transmissibility of Pellagra: Experimental Attempts at Transmission to the Human Subject.” Public Health Reports (1896-1970) 31 (46): 3159–3173. doi:10.2307/4574262.
- Goldberger, J., C. H. Waring, and D. G. Willets. 1914. “The Treatment and Prevention of Pellagra.” Public Health Reports (1896-1970) 29 (43): 2821–2825. doi:10.2307/4571457.
- Goldberger, J, and G. A. Wheeler. 1915. “Experimental Pellagra in the Human Subject Brought about by a Restricted Diet.” Public Health Reports (1896-1970) 30 (46): 3336–3339. doi:10.2307/4572984.
- Goldberger, Joseph, C. H. Waring, and David. G. Willets. 1915. “The Prevention of Pellagra: A Test of Diet among Institutional Inmates.” Public Health Reports (1896-1970) 30 (43): 3117–3131. doi:10.2307/4572932.
- Goldberger, J., G. A. Wheeler, and E. Sydenstricker. 1918. “A Study of the Diet of Nonpellagrous and of Pellagrous Households in Textile Mill Communities in South Carolina in 1916.” Journal of the American Medical Association 71 (12): 944–949.
- Goldberger, J., G. A. Wheeler, and E. Sydenstricker. 1920a. “A Study of the Relation of Diet to Pellagra Incidence in Seven Textile-Mill Communities of South Carolina in 1916.” Public Health Reports (1896-1970) 35 (12): 648–713. doi:10.2307/4575517.
- Goldberger, J., G. A. Wheeler, and E. Sydenstricker. 1920b. “Pellagra Incidence in Relation to Sex, Age, Season, Occupation, and ‘Disabling Sickness’ in Seven Cotton-Mill Villages of South Carolina during 1916.” Public Health Reports (1896-1970) 35 (28): 1650–1664. doi:10.2307/4575643.
- Goldberger, J., G. A. Wheeler, and E. Sydenstricker. 1920c. “A Study of the Relation of Family Income and Other Economic Factors to Pellagra Incidence in Seven Cotton-Mill Villages of South Carolina in 1916.” Public Health Reports (1896-1970) 35 (46): 2673–2714. doi:10.2307/4575780.
- Hargrove, J. L. 2006. “History of the Calorie in Nutrition.” The Journal of Nutrition 136 (12): 2957–2961. doi:10.1093/jn/136.12.2957.
- King, W. I. 1936. “Edgar Sydenstricker.” Journal of the American Statistical Association 31 (194): 411–414. doi:10.1080/01621459.1936.10503344.
- Kiser, C. V., D. G. Wiehl, P. C. Glick, and W. H. Grabil. 1971. “The Work of the Milbank Memorial Fund in Population since 1928.” The Milbank Memorial Fund Quarterly 49 (4): 15–66. doi:10.2307/3349464.
- Klarman, H. 1965. The Economics of Health, New York, Columbia University Press.
- Lam, J.-P, and E. Piérard. 2017. “The Time-Varying Relationship between Mortality and Business Cycles in the USA.” Health Economics 26 (2): 164–183.
- Lauck, W. J., and E. Sydenstricker. 1917. Conditions of Labor in American Industries, New York and London: Funk & Wagnalls.
- Lechner, M. 2010. “The Estimation of Causal Effects by Difference-in-Difference Methods.” Foundations and Trends® in Econometrics 4 (3): 165–224. doi:10.1561/0800000014.
- Meyer, B. D. 1995. “Natural and Quasi-Experiments in Economics.” Journal of Business & Economic Statistics 13 (2): 151–161.
- Mooney, S. J., J. Knox, and A. Morabia. 2014. “The Thompson-McFadden Commission and Joseph Goldberger: Contrasting 2 Historical Investigations of Pellagra in Cotton Mill Villages in South Carolina.” American Journal of Epidemiology 180 (3): 235–244. doi:10.1093/aje/kwu134.
- Mushkin, S. J. 1958. “Toward a Definition of Health Economics.” Public Health Reports (1896-1970) 73 (9): 785–793. doi:10.2307/4590242.
- Myrdal, G. 1952. “Economic Aspects of Health.” in Fifth World Health Assembly, 5-22 May 1952, Technical Discussions1–28. Geneva: World Health Organization.
- Ogburn, W. F. 1931. “A Device for Measuring the Size of Families.” invented by Edward Sydenstricker and W.I. King,” in: S.A. Rice (Ed.), Methods in Social Science: A Case Book, Chicago: University of Chicago Press, 210–219.
- Pearl, R. 1919. “Influenza Studies: I. On Certain General Statistical Aspects of the 1918 Epidemic in American Cities.” Public Health Reports (1896-1970) 34 (32): 1743–1783. doi:10.2307/4575264.
- Pearl, R. 1921. “Influenza Studies.” Public Health Reports (1896-1970) 36 (7): 273–298. doi:10.2307/4575894.
- Perrott, G. S. J, and S. D. Collins. 1935. “Relation of Sickness to Income and Income Change in 10 Surveyed Communities. Health and Depression Studies No. 1: Method of Study and General Results for Each Locality.” Public Health Reports (1896-1970) 50 (18): 595–622. doi:10.2307/4581530.
- Perrott, G. S. J, and E. Sydenstricker. 1935. “Causal and Selective Factors in Sickness.” American Journal of Sociology 40 (6): 804–812. doi:10.1086/216985.
- Robertson, J. 1913. “Infant Mortality in Relation to Factory Labor.”, in: Transactions of the Fifteenth International Congress on Hygiene and Demography, Washington, September 23-28, 1912, Washington: Government Printing Office, Vol. III, 947–956.
- Roe, D. A. 1973. A Plague of Corn: The Social History of Pellagra, Ithaca: Cornell University Press.
- Rowntree, B. S. 1902. Poverty. A Study of Town Life. 2nd ed. London: Macmillan.
- Savedoff, W. D. 2004. “Kenneth Arrow and the Birth of Health Economics.” Bulletin of the World Health Organization 82 (2): 139–140.
- Schaller, J, and M. Zerpa. 2019. “Short-Run Effects of Parental Job Loss on Child Health.” American Journal of Health Economics 5 (1): 8–41. doi:10.1162/ajhe_a_00106.
- Schereschewsky, J. W. 1915. Studies in Vocational Diseases. I. The Health of Garment Workers (Public Health Bulletin No. 71), Washington, Government Printing Office, 17–103.
- Schereschewsky, J. W., B. S. Warren, and Edgar Sydenstricker. 1916. “Health of Garment Workers. The Relation of Economic Status to Health. Introduction.” Public Health Reports (1896-1970) 31 (21): 1298. doi:10.2307/4573639.
- Schereschewsky, J. W, and D. H. Tuck. 1915. Studies in Vocational Diseases. II. The Hygienic Conditions of Illumination in Workshops of the Women’s Garment Industry (Public Health Bulletin No. 71), Washington, Government Printing Office, 105–223.
- Siler, J. F., P. E. Garrison, and W. J. Macneal. 1914. “A Statistical Study of the Relation of Pellagra to Use of Certain Foods and to Location of Domicile in Six Selected Industrial Communities.” Archives of Internal Medicine 14 (3): 293–373.
- Siler, J. F., P. E. Garrison, and W. J. Macneal. 1917a. “Relation of Pellagra to Location of Domicile in Spartan Mills, S. C., and the Adjacent District.” Archives of Internal Medicine 20 (2): 198–315.
- Siler, J. F., P. E. Garrison, and W. J. Macneal. 1917b. “The Relation of Pellagra to Location of Domicile in Inman Mills, Inman, S. C.” Archives of Internal Medicine 20 (4): 521–574.
- Susser, M, and Z. Stein. 2009. Eras in Epidemiology: The Evolution of Ideas, Oxford: Oxford University Press.
- Swain, D. C. 1962. “The Rise of a Research Empire: NIH, 1930 to 1950.” Science (New York, N.Y.) 138 (3546): 1233–1235. doi:10.1126/science.138.3546.1233.
- Sydenstricker, E. 1915. A Brief History of Taxation in Virginia, Richmond: The Legislative Reference Bureau of Virginia.
- Sydenstricker, E. 1916. “The Settlement of Disputes under Agreements in the Anthracite Industry.” Journal of Political Economy 24 (3): 254–283. doi:10.1086/252801.
- Sydenstricker, E. 1918. “Preliminary Statistics of the Influenza Epidemic.” Public Health Reports (1896-1970) 33 (52): 2305–2321. doi:10.2307/4574973.
- Sydenstricker, E. 1921. “Variations in Case Fatality during the Influenza Epidemic of 1918.” Public Health Reports (1896-1970) 36 (36): 2201–2210. doi:10.2307/4576118.
- Sydenstricker, E. 1926. “A Study of Illness in a General Population Group: Hagerstown Morbidity Studies No. I: The Method of Study and General Results.” Public Health Reports (1896-1970) 41 (39): 2069–2088. doi:10.2307/4578020.
- Sydenstricker, E. 1927. “The Measurement of Results of Public Health Work. An Introductory Discussion.” in Milbank Memorial Fund Report for the Year Ended December 31, 1926, New York: Milbank Memorial Fund, 27–60.
- Sydenstricker, E. 1928a. “The Statistical Evaluation of the Results of Social Experiments in Public Health.” Journal of the American Statistical Association 23 (161): 155–165. doi:10.2307/2277580.
- Sydenstricker, E. 1928b. “The Statistician’s Place in Public Health Work.” Journal of the American Statistical Association 23 (162): 115–120. doi:10.1080/01621459.1928.10503004.
- Sydenstricker, E. 1928c. “The Decline in the Tuberculosis Date Rate in Cattaraugus County.” The Milbank Memorial Fund Quarterly Bulletin 6 (2): 41–50. doi:10.2307/3347534.
- Sydenstricker, E. 1929a. “Economic Status and the Incidence of Illness: Hagerstown Morbidity Studies No. X: Gross and Specific Illness Rates by Age and Cause among Persons Classified according to Family Economic Status.” Public Health Reports (1896-1970) 44 (30): 1821–1833. doi:10.2307/4579329.
- Sydenstricker, E. 1929b. “Differential Fertility according to Economic Status: Hagerstown Morbidity Studies No. XI: Live Birth and Still Birth Rates among Married Women of Different Ages Classified according to Family Economic Condition.” Public Health Reports (1896-1970) 44 (35): 2101–2106. doi:10.2307/4579371.
- Sydenstricker, E. 1931. “The Incidence of Influenza among Persons of Different Economic Status during the Epidemic of 1918.” Public Health Reports (1896-1970) 46 (4): 154–170. doi:10.2307/4579923.
- Sydenstricker, E. 1933a. Health and Environment, New York and London: McGraw-Hill.
- Sydenstricker, E. 1933b. “Health and the Depression.” The Milbank Memorial Fund Quarterly Bulletin 11 (4): 273–280. doi:10.2307/3347444.
- Sydenstricker, E. 1934. “Group Medicine or Health Insurance. Which Comes First?” American Labor Legislation Review 24 (2): 79–86.
- Sydenstricker, E. 1935. “Health Insurance and the Public Health.” Proceedings of the Academy of Political Science 16 (3): 12–21. doi:10.2307/1172795.
- Sydenstricker, E. 1936a. “Health under the Social Security Act.” Social Service Review 10 (1): 12–22. doi:10.1086/631785.
- Sydenstricker, E. 1936b. “Economy in Public Health.” The Milbank Memorial Fund Quarterly 14 (1): 3–12. doi:10.2307/3347820.
- Sydenstricker, E. 1936c. “Public Health Provisions of the Social Security Act.” Law and Contemporary Problems 3 (2): 263–270. doi:10.2307/1189395.
- Sydenstricker, E. 1974. “The Challenge of Facts.” Selected Public Health Papers of Edgar Sydenstricker, ed. by Richard V. Kasius, New York: Milbank Memorial Fund.
- Sydenstricker, E, and A. L. Burger. 1914. School History of Virginia, Lynchburg: Dulaney-Boatwright Company.
- Sydenstricker, E, and M. L. King. 1920a. “Difficulties in Computing Civil Death Rates for 1918, with Especial Reference to Epidemic Influenza.” Public Health Reports (1896-1970) 35 (7): 330–345. doi:10.2307/4575481.
- Sydenstricker, E, and W. I. King. 1920b. “A Method of Classifying Families according to Incomes in Studies of Disease Prevalence.” Public Health Reports (1896-1970) 35 (48): 2829–2846. doi:10.2307/4575798.
- Sydenstricker, E, and W. I. King. 1921a. “The Classification of the Population according to Income.” Journal of Political Economy 29 (7): 571–594. doi:10.1086/253372.
- Sydenstricker, E, and W. I. King. 1921b. “The Measurement of the Relative Economic Status of Families.” Quarterly Publications of the American Statistical Association 17 (135): 842–857. doi:10.2307/2965186.
- Sydenstricker, E., W. I. King, and D. Wiehl. 1924. “The Income Cycle in the Life of the Wage-Earner.” Public Health Reports 39 (34): 2133–2140.
- Tapia Granados, J. A, and A. V. Diez Roux. 2010. “Life and Death during the Great Depression.” Proceedings of the National Academy of Sciences of the United States of America, 106(41): 17290–17295.
- Vaughan, W. T. 1921. Influenza: An Epidemiologic Study, Baltimore, MD: The American Journal of Hygiene.
- Warren, B. S, and E. Sydenstricker. 1916a. Health Insurance. Its Relation to the Public Health (Public Health Bulletin, No. 76), Washington: Government Publishing Office.
- Warren, B. S, and E. Sydenstricker. 1916b. “Health of Garment Workers in Relation to Their Economic Status.” Public Health Reports 31 (21): 1298–1305.
- Weisz, G. 2011. “Epidemiology and Health Care Reform: The National Health Survey of 1935-1936.” American Journal of Public Health 101 (3): 438–447. doi:10.2105/AJPH.2010.196519.
- Wiehl, D. G. 1974. “Edgar Sydenstricker: A Memoir.” in R.V. Kasius (Ed.), The Challenge of Facts. Selected Public Health Papers of Edgar Sydenstricker, New York: Milbank Memorial Fund, 1–17.
- Winslow, C.-E. A. 1951. The Cost of Sickness and the Price of Health, (World Health Organization Monograph Series No. 7, Geneva: World Health Organization.
- Wolfe, B. 2018. “Health Economics.” in The New Palgrave Dictionary of Economics, 5696–5706. London: Macmillan.