
Abstract
How do local Norwegian work, welfare, and health services (WWH services) support the labor market integration of chronically ill people? We discuss how user organization representatives evaluate the role of municipal-level service support in facilitating labor market participation of people with chronic illnesses and disabilities, and to what extent the views of user organizations are requested and included in local service development. We thus contribute to the limited research on the role of WWH services for work inclusion from the user perspective. Our analysis rests on an original web-based survey, combining qualitative and quantitative data, and a focus group discussion. Although user representatives call for strengthening of services, they also view employers’ adaptations as being more important than local services. And despite their expertise, user organizations are only included in local service development to a limited extent.
Points of interest
This study is based on the perspectives of user organization representatives. They are leaders or secretaries for organizations in the Norwegian Federation of Organizations of Disabled People, the largest national umbrella organization for people with disabilities and chronic illnesses.
These user representatives have broad knowledge of what really matters for people with chronic illnesses who are seeking a job and how services meant to help them should work.
According to these user representatives, employer adaptations and attitudes are more important for work inclusion than local services.
Main barriers to work inclusion are limited service capacity, little personalized support, and insufficient employer adaptations.
User organizations are rarely consulted or involved in local service development. However, involving user representatives in this way could use their knowledge to improve services for people with chronic illnesses.
Introduction
Participation in working life is important for facilitating social inclusion, self-worth, wellbeing, and economic security (Andreassen, Breit, and Saltkjel Citation2022; Carmichael and Clarke Citation2022). Additionally, access to work and inclusion into working life are central values for most people. The right to work is emphasized in the UN Declaration of Human rights in article 23 (United Nations Citation1948) and is a key sustainability goal (number 8) on full and productive employment and decent work for all (United Nations Department of Economic and Social Affairs Citation2015). These rights and sustainability goals extend to people with disabilities and chronic illnesses and are encompassed by the UN Convention on the Rights of Persons with Disabilities and its article 27 on Work and Employment (United Nations Department of Economic and Social Affairs Citation2006).
Support for work inclusion of people with chronic illnesses and disabilities is thus an important policy objective, emphasized in Norwegian and international policy documents (cf. e.g. Arbeids- og velferdsdirektoratet and Helsedirektoratet Citation2021; Finnvold and Pedersen Citation2012). Nevertheless, there remains a notable gap between those with and without chronic illnesses regarding employment opportunities and work inclusion. Statistics for selected European countries on employment rates among people aged 50-59 showed an average of 74% of individuals with no chronic diseases in employment, compared to 69% for those with one chronic disease (OECD/European Union Citation2016). Our own calculations using the Norwegian Patient Register, covering those aged 15-70 (working age in Norway), indicate labor market participation rates of 80% for those with no chronic illnesses, compared to 69% for people with chronic illnesses in 2014. Considerable differences also exist at the local level across Norwegian municipalities. Research has increasingly identified the local level as being crucial for the regulation and provision of services that support social and work inclusion (Heidenreich and Rice Citation2016; Künzel Citation2012). Although some people may have illnesses or disabilities which leave them completely unable to work, others might have some capacity for work, if provided proper support. Therefore, an important issue is how work participation of people with chronic illnesses can be increased by mobilizing local service resources. Organizations of persons with disabilities play an important role in promoting the rights of people with disabilities (Banks et al. Citation2023). User representatives in these organizations have unique insights on how local services can promote work participation.
For several decades, improving work inclusion for people with disabilities and/or chronic illnesses has been on the political agenda in Norway (Finnvold and Pedersen Citation2012). The establishment of the umbrella organization now known as Funksjonshemmedes Fellesorganisasjon (FFO, Norwegian abbreviation for The Norwegian Federation of Organizations of Disabled People) in 1950 is evidence of the early connection to public measures for work inclusion, and the importance of organizing for strengthening the political voices of those with barriers to employment (Andersen Citation2001; Willoch Citation1950). This political aspect is thus closely linked to the user perspective and how this has changed historically (Guldvik and Askheim Citation2022). The importance of user involvement is succinctly expressed in the FFO’s program point on participation and active involvement: “Nothing about us without us” (FFO Citation2021, 4).
A recent review suggests there is only limited knowledge on the importance of local work, welfare, and health services (WWH services) as well as coordination and cooperation between actors in these services (Rydland et al. Citation2022). Additionally, a recent critical account of research on collaboration in health and care services concludes that user perspectives are only marginally represented in the literature, and that service provider perspectives dominate (Sandvin, Lo, and Breimo Citation2022). By including user representatives’ perspectives in our inquiry, we therefore aim to contribute to filling this gap in the literature. User representatives can provide important insights into what really matters for people with chronic illnesses regarding barriers and facilitators to labor market participation, and how services should be designed accordingly. In this article, we emphasize both the work inclusion and the user perspectives by addressing the following research questions:
What barriers and facilitators do user organization representatives identify in local WWH services’ support for labor market participation of people with chronic illnesses?
To what extent do user perspectives inform local WWH service development?
We begin by presenting the Norwegian context and previous research. Next, we describe our method and data. The results of our analyses are presented thereafter, and we conclude with a discussion of the implications of our findings.
Empirical background and previous research
Volunteer organizations context and user group involvement
Norway has a long tradition of involving labor unions, employer organizations, and voluntary organizations in policy making processes at the national level. These key actors are included in governmentally appointed commissions evaluating policy and preparing new legislation and are invited to provide input on reforms within their policy fields. This inclusion in policy making is often referred to as the “organizational channel”. Norwegian civil society organizations are particularly active in social and welfare policy (Kuhnle and Selle Citation1992; Rommetvedt Citation2022; Sivesind and Enjolras Citation2022). These organizations usually have an advocacy rather than service provision role and are considered important to welfare service development (Gathen, Slettebø, and Skjeggestad Citation2023, 3). Organizations representing people with disabilities and chronic illnesses, such as FFO, have been crucial in the work for strengthened rights and independent living, and in the struggle for establishing stronger user control of services. Still, as noted by Guldvik and Askheim (Citation2022), living conditions for people with disabilities in Norway are below average in several domains, and discrimination and lack of recognition remain a challenge in employment and social life; this thus calls into question the supposed “harmony model” of the Nordic countries.
In the period after the year 2000, a legal requirement for local user representation was introduced (Guldvik and Askheim Citation2022, 1410). One recent way of promoting user perspectives has been through the council for people with disabilities, which each municipality is required to establish. However, an assessment conducted by FFO (Citation2019) suggests that while councils are frequently consulted regarding universal design of buildings, they have a very limited role when it comes to services, service content, education, and working life. A recent report on municipal and county councils confirms the strong focus on universal design, but also finds that councils for people with disabilities are less frequently consulted on work-related issues (Proba samfunnsanalyse Citation2022). Furthermore, whereas these councils operate at the systemic level, less is known about user perspectives at the service level. This raises the question of whether user organizations are consulted on work and services more directly outside of the council channel.
According to Gathen, Slettebø, and Skjeggestad (Citation2022), we know little about how user participation may improve services. Their review study states that user participation can have both individual level impacts, such as facilitating empowerment and increasing professional knowledge, and organizational level impacts which promote attitudinal, professional practice, and policy change (ibid). This is our point of departure when asking user representatives what barriers to inclusion they identify and whether they are included in local service development.
In their study of how user participation for people with disabilities is constructed in Norway, Guldvik and Askheim (Citation2022) reference three distinct discourses. The democracy discourse concerns the societal and policymaking level and is about user participation as “a means for citizens to obtain broader influence” (Citation2022, 1399). The consumer discourse concerns the service level and focuses on adjustment and improvement of services. The co-production discourse is concerned with both democratic and higher-quality services, and rests on an understanding of users as being active in service production. In our study of user organization views on WWH services that may promote labor market participation of chronically ill people, we are particularly interested in the consumer discourse and whether services can be adjusted to better meet user needs, as well as the larger discourse on democracy and how user perspectives are included.
The Norwegian WWH service context and labor market participation
The Norwegian labor market is characterized by demands for high levels of formal skills and education, as well as an expectation of high levels of production. In Norway, WWH services at the local (municipal) level encompass a variety of services involving different professions. As there are numerous services applicable to labor market participation, providing a complete overview is beyond the scope of this article. Instead, we provide a brief description of a limited selection of relevant services and actors. Of key importance is The Norwegian Labor and Welfare Organization (NAV), composed of a central agency and parts of the municipal social service systems. NAV provides social security and facilitates transitions to activity and employment. In addition, within health services, the general practitioner (GP) occupies a key position for people with chronic illnesses at risk of sickness leave and labor market exclusion. The GP assesses the need for and issues sick leave certificates and functions as a gatekeeper for access to specialist health services. In their follow-up of sick leave, the GP cooperates with other health services (e.g. rehabilitation), work and welfare services, and employers in so-called “follow-up plans” as part of joint efforts to ensure a more inclusive working life (Nav Citation2019). In work and welfare services, the work ability assessment is central for evaluating possibilities and challenges for those with reduced work capacity, measured against working life demands. The work ability assessment, done by NAV and the user, includes the persons’ skills, requirements of their profession or vocation, and possibilities for adaptation and support in their work situation. The local NAV office also surveys job opportunities relevant for the individual and cooperates with employers.
The work ability assessment is the starting point for other follow-up services provided by NAV. These services can include methods of supported employment, such as Individual Placement and Support (IPS), directed towards people with serious mental illnesses. This emphasizes work participation early on, combining psychological treatment in parallel with follow-up by a job specialist. Together, the involved professionals comprise a treatment team around the user (cf. Lesner Citation2019, 35-38, for elaboration). Learning and mastery courses may also strengthen work participation. Here, users gain knowledge and advice on how to handle and live with illness, including users’ own experience, as part of both prevention and rehabilitation. These examples reveal how individual, interconnected services may be of importance for supporting the work inclusion of individuals with chronic illnesses.
A recent strategy document for the work and health sectors emphasizes the importance of municipal services for helping people with health challenges into work, while also acknowledging a significant unexploited potential in using municipal services for activation (Arbeids- og velferdsdirektoratet and Helsedirektoratet Citation2021). A main pillar in the updated strategy is to entrust local actors: “Municipal services are important for helping people remain in work despite suffering from health problems—there is a large untapped potential in the activation of municipal services” (Arbeids- og velferdsdirektoratet and Helsedirektoratet Citation2021, 14, authors’ translation). Since municipal work and health services are strongly emphasized in policy documents, we expect these to be a major concern for user organizations as well. Therefore, how local services support labor market participation of chronically ill people is an area which merits further investigation.
Research process: data and method
Our analyses are based on two sources of data: a survey, which included closed and open-ended questions, and a focus group discussion. The survey was administered from March to April of 2022. Respondents were representatives (leaders or secretaries) for user organizations and regional affiliates in the Norwegian Federation of Organizations of Disabled People (FFO). FFO is Norway’s largest umbrella organization for individuals with disabilities and chronic illnesses, encompassing 11 regional affiliates and 87 interest organizations, with over 350,000 members.
The degree of organization among people with disabilities appears to be quite substantial in Norway—this also coincides with high levels of organizational participation amongst the population as a whole. In 2017, 17% of the population aged 16-66 years self-reported a disability, comprising approximately 605,000 persons (Bø and Haland Citation2017). With 350,000 members, it is likely that FFO organizes many of these people with disabilities or chronic illnesses, as well as their families, or others in their support network. However, we do not have statistics on the backgrounds of these FFO members. A large proportion of organizational membership, and thus potential representativity, would stand in strong contrast to numbers reported for low- and mid-income countries (Banks et al. Citation2023).
FFO works with political authorities centrally and locally, in advocacy work on health, labor market participation, and better living conditions for people with a range of chronic illnesses and disabilities. While individual users have the best insight into their own situations, we deemed representatives from the FFO user organizations to be best able to answer questions on local WWH services from a systemic and service perspective. They are in contact with many users with disabilities or chronic illnesses and their families. This provides the user organization representatives with unique insights into the collective experiences of their user groups, leaving them well positioned to identify broad patterns of user experiences related to local level service provision. Their institutional anchorage also grants them an understanding of the interconnection between specific local services and the broader process of labor market inclusion. Possible examples could be members addressing a lack of rehabilitation services and long waiting times as a barrier to employment, or members’ positive experiences with wage subsidies for work inclusion. Moreover, FFO regularly administers surveys to their members on a variety of themes, for example, related to work inclusion, effects of the pandemic, and discrimination. We thus focused on these representatives in our inquiry.
Survey questions assessed the importance of local WWH services, the role of employers, as well as various barriers and facilitators to labor market participation of people with chronic illnesses. Additionally, questions included respondents’ assessment of their own member organization’s involvement in service development. The respondents were instructed to respond to the questions with a basis in a “normal” situation, thus disregarding the pandemic or any pandemic restrictions. Supplementary qualitative data were collected using three open-ended questions at the end of the survey. We asked about respondents’ perspectives on what municipalities do well and what they could improve on at the service level to support labor market inclusion. We also asked what the main barriers were to labor market participation. Finally, respondents were given the opportunity to add any additional comments or reflections on the topic.
The survey is focused on people of working age with reduced work capacity due to diagnoses or long- lasting illnesses such as cardiovascular diseases, cancer, mental health, chronic pain, and lung diseases. By work participation we imply a minimum of one hour of paid work each week. Some of the organizations under the FFO umbrella may not explicitly consider themselves as dealing with chronic illnesses. However, by using a broad definition including reduced work capacity due to illness, which was discussed with our partner in FFO and presented in the information to respondents, this characterization remains applicable for the organizations in our sample.
Our survey was developed with feedback from FFO to ensure relevance and to determine which organizations would be appropriate to include. Out of all the FFO organizations, we excluded 18 because they either focused primarily on children, targeted groups that were entirely unable to work, didn’t concentrate on chronic illnesses, or conveyed that labor market participation wasn’t a relevant area of focus for them. Our total targeted population includes 69 organizations and 10 regional affiliates. In all, 38 representatives responded to parts of the survey (48% response rate) and 36 of these (32 organizational representatives and 4 regional affiliates) completed the full survey (45.5% response rate). A total of 28 of the 38 respondents answered the optional open-ended questions. Respondents included representatives from larger organizations with over 10,000 members, as well as from smaller organizations representing just a few hundred people, generally with less common chronic illnesses. The total number of members represented by the organizations responding is approximately 149,000, with an average of 4,390 members per organization. The total number of members represented by organizations which did not respond was approximately 155,000, with an average of 4,420 members per organization. With a starting point in the (essentially) entire population of organizations in the largest umbrella organization for individuals with disabilities and chronic illnesses in Norway, and an acceptable organizational response rate, covering organizations representing hundreds of thousands of people with chronic illnesses, the empirical basis for our analyses is satisfactory.
While the main source of data is the web-based survey, we also draw on findings from a focus group arranged in December 2019 on the topic of barriers and opportunities for work inclusion of people with chronic illnesses. The focus group consisted of representatives from six FFO member organizations, as well as one representative from the central level of FFO. The six organizations represented members with common somatic and mental health illnesses.
Analysis of the survey data were primarily exploratory/descriptive-analytical, using summary statistics to provide an overview of patterns in the responses. Qualitative data from the open answer questions and the focus group discussion were coded and categorized using a thematic approach (Braun and Clarke Citation2006). Individual responses and quotations were first read through and broadly categorized by one member of the team. Thereafter the themes were further refined. A second team member then reviewed the themes and coding. At this time, specific quotations which supported or provided insight into patterns identified in the quantitative data, as well as exemplifying the remaining themes were selected and translated from Norwegian to English. The plan for data collection was registered at and assessed by our data protection agency (SIKT- Reference Number 309024). All respondents provided informed consent to participate in the study, in line with international and institutional ethical guidelines.
Results
Respondents represented a variety of organizations, focusing primarily on somatic illnesses (for example, myalgic encephalomyelitis (ME), cancers, multiple sclerosis), but also represented organizations focusing on mental health. The majority (89%, N = 34) of the 38 survey respondents had been working for at least two years in their organization. In all, only 11% (N = 4) had been working there for one year or less, while 34% (N = 13) had worked in the organization for more than ten years. Slightly over half of the respondents (55%, N = 21) had labor market participation as a specific area of responsibility. Our respondents’ long organizational experience and labor market focus strengthens the relevance of targeting this group.
As our emphasis is on labor market participation, we were interested in the extent to which the users represented by the organizations were currently employed, as well as how many had the potential to work either part time or full time, if given proper support and accommodations. Our survey respondents indicate that there is large gap regarding those who are currently employed and those who could work if provided proper support or adaptations. In all, 11% (N = 4) of the respondents stated that none/few of the people their organization represents are in work, while the majority–64%–responded that some are in work (N = 23). An additional 22% (N = 8) stated that the majority or almost all the people in their user groups are in work, while 3% (N = 1) were uncertain. A total of 58% (N = 21) of the respondents answered that the majority or almost all their users could be in work with proper accommodation and support, while 36% (N = 13) answered that some would be able to work. 3% (N = 1) responded that none/only a few would be able to work with proper support and 3% did not know (N = 1).
Supports and barriers to labor market participation
We identified three main themes representing supports and barriers in relation to labor market participation and the role of local services and actors, based on the qualitative data from the survey and focus group. These three themes were: Service capacity, Individually focused adaptations and support, and Employer’s role. These are complemented by the quantitative survey results, which are presented concurrently. All three themes provide insight on the intersection between local services, employers, and characteristics of individuals with chronic illnesses.
Service capacity
Service and capacity problems was a key theme, highlighted by multiple respondents as a barrier to labor market participation amongst people with chronic illnesses. More specifically, this included low quality or missing services, long waiting times, a lack of qualified or knowledgeable staff, as well as variations in services and their quality across municipalities. For example, several user representatives emphasized a lack of knowledge about chronic illness and specific services, both among service providers, as well as amongst employers. The source of knowledge about chronic illness and labor market inclusion was also highlighted by one respondent, who argued that those making policies and measures do not have the same experiences and knowledge as those living with chronic illnesses. Therefore, there is a need to: «talk with [those with chronic illnesses] rather than about them”. This exemplifies how user representatives can provide important knowledge and perspectives on barriers and facilitators to labor market participation and adaptation of local services. Cooperation can also facilitate knowledge development. In the focus group, representatives suggested that some services are especially important for people with chronic illnesses. These representatives identified municipal capacity and quality within rehabilitation, and long waiting times for physiotherapy as being problematic and in need of improvement. Similarly, survey respondents emphasized that although specific services may be offered, there may be a lack of access or long waiting times. Such barriers can exacerbate existing health problems, contribute to developing new comorbidities, and result in further distancing from participation in working life, as one survey respondent writes:
[Work ability] Assessment and treatment take too long. People end up in a cycle of chronification, which is a contributing factor in the development of mental health problems over time for many people. The longer the time spent outside working life, the higher the risk for many to end up applying for AAP [work assessment allowance for individuals with work ability reduced by at least 50%] and disability benefits.
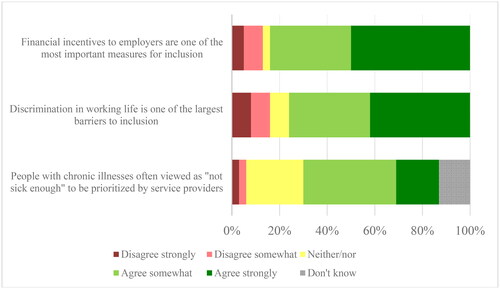
Figure 1. Percentage of respondents agreeing/disagreeing with statements regarding barriers, measures, and possibilities for labor market inclusion of people with chronic illnesses (N = 38).
Overall, investment in services may reduce service problems, according to the user organization representatives. As one focus group member suggests, a municipal-level improvement that could be made would be to “establish professional coordinator positions, with diagnosis-specific areas of responsibility, skill, and allocation of sufficient working hours [for these positions].” A survey respondent gives a similar suggestion:
The municipalities would reap great benefits by setting up an interdisciplinary team, with a much greater focus on rehabilitation and [greater use of specialists beyond the GP].
Individually focused adaptations and support in services
Another broad theme across the survey and focus group responses was a need for local services and work conditions to be individually adapted to the needs of the person’s specific situation. As multiple user representatives emphasized, people with chronic illnesses often have variations in their functioning, impacting on their work capacity. This requires understanding from employers (as discussed in the subsequent section), but also support that focuses on the individual’s abilities and needs for adaptation. One survey respondent explains: “Very many [of the people we represent] would like to work and could potentially do so with sufficient adaptations”. Another survey respondent writes that overall, “the abilities and preconditions of each individual must be given more weight”. This is particularly important in light of the challenge of needing to “combine work and ‘bad periods’ with no ability to work, or a wide variation in ability to work”. However, according to a third user representative, the municipalities “in general, have poorly individually tailored work-oriented measures and services”. Personal motivation and setting realistic goals for participation must also be considered, according to a different user representative:
Adaptations are important, but motivation is even more important. The attitude that work is a burden needs to go away. Work is about inclusion and mastering life. Also offering those who have a chronic illness to participate in something meaningful is positive and must be presented in a way that is motivating. [This includes] Creating realistic expectations regarding ability to perform and coming to an agreement about one’s limitations before starting up with work practice. (Survey respondent)
Employer’s role
We asked the survey respondents to assess which single actor was most important in facilitating labor market inclusion of people with chronic illnesses. Surprisingly, although we anticipated work/welfare or health services as being most important, it was employer adaptations for the individual worker which were deemed most important (50% of the respondents; N = 18). Municipal work and welfare services were selected as most important by 28% of respondents (N = 10), while health services were selected by the smallest percentage (11%; N = 4) of respondents. Those answering “other” (11%; N = 4) were allowed to provide more information in short answer form. Two of these four responses emphasized coordination between the different services, while one emphasized the role of employers.
In the focus group discussion, we received similar insights from a user organization representative, who identified the labor market and employers’ ability and willingness to adapt as the main challenge. This representative emphasized the importance of public financial incentives to employers, which can compensate for additional costs associated with employing people with reduced work capability due to chronic illness:
I am familiar with a couple of examples where [the use of financial incentives to employers] has prevented people from being excluded from the labor market or have been excluded later than one otherwise would have been, and to some this serves well as an admission ticket to work. (Focus group participant)
Regarding the role of employers, while incentives were described as an important facilitator for employers to hire people with chronic illnesses, several respondents explicitly mentioned discrimination and negative attitudes towards people with chronic illnesses as a significant barrier during the hiring process. This was also reflected in the quantitative results. In all, a large majority (76%; N = 29) of the survey respondents agreed with the statement that “discrimination in working life is one of the largest barriers to people with chronic illnesses’ participation”, while 16% (N = 6) disagreed, and 8% (N = 3) were neutral.
Adjusting the work environment to the individual needs of employees with chronic illnesses was an issue emphasized by multiple respondents in the qualitative survey responses. Flexible working hours was one example of a potential adjustment. Additionally, several responses highlighted a lack of flexibility and understanding amongst employers that employees might have an occasional “bad day” and need special adjustments, as individual capacity for work can be unpredictable or unstable. While many of these barriers occur at the individual level, several respondents also highlighted issues of a structural nature. One suggested that employers should emphasize the importance of “inclusion and diversity in job advertisements”. At higher levels, there was also a desire for more “political support for inclusion”. A different representative highlighted structural barriers related to full time work in the following quotation:
The lack of adapted positions, and part time positions [of employment]. Full time positions are usually too demanding on chronically ill [people]. Therefore, it is necessary to allow for part time positions and flexible working hours so that chronically ill people have an actual chance of participating in working life. (Survey respondent)
User representatives’ involvement in service development
Regarding user perspectives informing the development of local WWH services, the user representatives revealed during the focus group discussion that some municipalities had developed networks aimed at strengthening work inclusion of people with mental illnesses. User involvement was emphasized in these networks. However, the focus group discussion (in line with our previously presented results) also revealed the view that public employees in WWH services have insufficient knowledge on specific chronic illnesses, and that they thus are unable or unwilling to accommodate services and measures to the needs of the individual. We were therefore interested in the extent to which user representatives were involved in development of local WWH services, either by being consulted, or by actively participating in WWH service development. This is particularly relevant given the previously highlighted needs for service capacity and individualized focus.
When asked to what extent representatives of local WWH services asked for the organizations’ views in development of services focusing on people with chronic illness and their work participation, 64% (N = 23) answered that this occurred never or rarely, while 22% (N = 8) responded that this occurred sometimes, and 6% (N = 2) reported that this occurred often or always. In all, 8% (N = 3) didn’t know.
When asked about their actual involvement in the development of local WWH services for work participation of people with chronic illnesses, a larger majority, 72% (N = 26), answered that they were never or only rarely involved, while 3% (N = 1) responded that they were often involved. In all 17% (N = 6) were involved sometimes, and 8% (N = 3) didn’t know.
Discussion and conclusions
Our study addresses both a call from authorities, as well as a gap in the literature, by studying how user organization representatives evaluate Norwegian WWH service support for labor market integration of people with chronic illnesses. This includes how user representatives describe barriers and facilitators, and the extent to which their views are solicited and reflected in development of local services. Overall, what has the user perspective added to existing research on WWH services, and how can these insights contribute to promoting labor market inclusion by strengthening the role of local services and actors?
As a starting point, responses from the user organization representatives highlight a noticeable gap between the proportions of users who are actually in work and the proportion who have the potential to be in work if provided proper support or accommodation. This reconfirms the unexploited potential for labor market inclusion of the chronically ill people they represent and corresponds with the call for work inclusion of people with chronic illnesses in government documents (Arbeids- og velferdsdirektoratet and Helsedirektoratet Citation2021; NOU Citation2019, 7, NOU Citation2021, 2).
Our analysis sheds light on three main facilitators and barriers to labor market inclusion. First, our respondents emphasize problems with service capacity, including inadequate services, local variations, or long waiting times. Service providers, employers, and policy makers are described as having limited knowledge about chronic illnesses and specific services. Respondents view service investment as a potential solution since more resources dedicated to coordination or knowledge of illnesses could help improve services. Additionally, individually tailored services, which account for peoples’ unique characteristics and needs, are important, according to our respondents. The acknowledgment that chronic illness may result in fluctuating work capabilities, rather than a consistent level of disability, was also an important aspect related to individual tailoring of services. However, despite this perceived importance, user representatives identified an absence of individualized orientation as a barrier to work inclusion. This also seems to confirm challenges outlined in previous research and governmental strategies (Arbeids- og velferdsdirektoratet and Helsedirektoratet Citation2016, Citation2021).
An unanticipated finding is that although many of the user representatives viewed labor market services (and to a lesser extent health services) as being important for facilitating inclusion, as also suggested by government documents, it was the role of employers which was viewed as most important. While our primary focus was on local public services, the role of employers in facilitating inclusion and in collaborating with local services was a recurrent theme in the qualitative data. We note with interest that half of our user representative survey respondents consider employers’ adaptations to be more important than local services. Admittedly, these respondents also emphasize public action, e.g. by mentioning incentives for employers to hire people with chronic illnesses. However, the role of employers and the company-level remains a key issue when promoting work participation for people with chronic illness (see e.g. Bolvig and Rangvid Citation2023). While employers are highlighted as having an important role in supporting labor market inclusion, the qualitative responses suggest that there is a lack of knowledge amongst these employers. Some employers also have negative attitudes towards people with chronic illnesses, which can result in discriminatory hiring practices, as other research also suggests (Bjørnshagen and Ugreninov Citation2021; Lasalvia et al. Citation2013). This is also in line with Olsen (Citation2022), who finds that employers often lack knowledge of disabilities, and fail to make genuine efforts to employ disabled people or provide adaptations. Employers thus can act as a “bottleneck” in the process of labor market inclusion; strengthening employers’ knowledge of illnesses can ameliorate this (Schafft Citation2007). Employers’ need for support in facilitating inclusion must therefore also be considered (ibid). These results also coincide with a recent report which emphasizes the importance of preventive approaches in the workplace, but also a notable lack of policies encouraging employers to hire people with reduced work capability (NOU Citation2021, 2, 12). It refers to wage subsidies as one relevant measure that should be used more frequently. Overall, according to our respondents, with wage subsidies, workplace adaptations, and consideration for individual circumstances, more people with chronic illnesses would be able to participate in working life.
Nevertheless, other responses clearly confirm the importance of local services. One important implication for practice in our view is that the role of employers should be included to a much larger extent, as an essential part of the discussion on service coordination. According to Bredgaard (Citation2018), we know little about the role of employers in inclusion of “disadvantaged” jobseekers. An interesting study by Mandal and Ose (Citation2015) on Norwegian enterprises shows how company behavior matters for inclusion of people with disabilities. They study this in light of the agreement on a more inclusive working life (IA agreement), which had, as one objective, the inclusion of workers with reduced functional ability, and the importance of integrating this in the company health, safety, and environment (HSE) work. A main finding is that integrating efforts related to IA agreements into HSE work more broadly is beneficial for people with disabilities (ibid 184).
The importance of employers suggests a broader context for work inclusion and key actors, but also points to an extra layer of coordination challenges. These could add to tensions in the public sector collaboration between WWH services by introducing an external sector of private and public employers where different institutional logics of market actors and the public sector meet.
A main barrier highlighted in the qualitative responses is a need for additional knowledge amongst service providers (and employers), something which user organizations could potentially assist with. Despite this, our user organization representative respondents indicate that they are involved to only a limited extent in service development. Few are involved in an advisory capacity, and even fewer are involved in actual service development. Our results therefore also support a call for increased user participation in public services at the local level. Previous research on local councils for user involvement (FFO Citation2019; Haukelien, Møller, and Vike Citation2011; Proba samfunnsanalyse Citation2022) finds that councils representing the interests of people with disabilities and chronic illnesses are generally limited to areas such as universal design policies and health services, whereas issues of work inclusion are less addressed. Our findings are in line with this latter point. This contrasts with the situation at the national level where the organizational channel is well-functioning in terms of access to policy makers and even policy influence, especially for umbrella organizations such as the FFO. The FFO’s plan for strengthening local organizational work (FFO Citation2021) could be seen as a first step to improve the potential for local voices of user representatives to be heard when WWH services are adapted and changed, to increase work inclusion of people with chronic illnesses and disabilities.
Our findings also underscore how user voices can provide increased knowledge of the needs for support that users identify related to their specific illness, and how this can be utilized in improving work inclusion. One example could be strengthening municipal rehabilitation services to improve health conditions and labor market participation for instance for those with chronic illnesses. A specific suggestion put forward by our respondents is a municipal coordinator, ideally with diagnosis-specific areas of responsibility, knowledge, and dedicated time to work inclusion. Alternatively, drawing more on local user expertise by means of collaboration with organizations could be a starting point. Improving services and their coordination makes daily life easier for those with chronic illnesses, potentially contributing to increased mastery and empowerment. Our findings thus support the work of Gathen, Slettebø, and Skjeggestad (Citation2022), who view user participation as a way of facilitating empowerment, professional knowledge, and policy change.
Although our research supports increased user participation to improve local services aiming at work inclusion, there is need for further research in considering the various critical risk points raised. This includes critically questioning the blessings of user involvement, such as co-optation, shifting responsibility towards individual users, and asymmetric power relationships between user representatives and political decision makers, and a potential lack of realism in user group demands unbound by budgetary constraints (see e.g. Eriksson Citation2018; Haukelien, Møller, and Vike Citation2011).
We note that user representatives are not necessarily neutral respondents and may have their own motivations for emphasizing certain services or challenges; this may be a limitation of our study, as is the small number of respondents. However, our findings are consistent with previous research, supporting these main conclusions. A clear implication of our results is that policy makers should not view WWH services as separate from the overall labor market context; the role of employers must also be considered. Individualized services and adaptations, which consider the individual’s unique situation are foundational for better facilitating labor market inclusion. However, this can be challenging for employers to facilitate. Policy makers should also consider specific services and approaches, such as rehabilitation and municipal coordinators as identified by user representatives, as areas for future improvement. However, this conclusion implies a delicate balance, as both public and private employers must ensure that they carry out their work in the interest of inhabitants and customers. Although user organizations are not responsible for this, one must acknowledge the potential conflict between strong employer adaptations for inclusion of chronically ill on the one side, and efficiency of public and private service production on the other.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Andersen, Rune. 2001. Likestillet Med Andre" Funksjonshemmedes Fellesorganisasjons Første 50 år. Oslo: FFO.
- Andreassen, Tone Alm., Eric Breit, and Therese Saltkjel. 2022. “Inkludering, Antidiskriminering Eller Aktivering: Hvordan Politikk for Økt Arbeidsdeltakelse Studeres Fra Ulike Forskningstradisjoner.” In Samhandling og Inkludering i Arbeidslivet, edited by Therese Saltkjel, Chris Rønningstad and Mette Sønderskov, 41–71. Oslo: Cappelen Damm Akademisk.
- Arbeids- og velferdsdirektoratet & Helsedirektoratet. 2016. Arbeid og helse- et tettere samvirke. Strategi for Helsedirektoratets og Arbeids- og velferdsdirektoratets felles innsats for arbeid og helse. Oslo: Helsedirektoratet.
- Arbeids- og velferdsdirektoratet, and Helsedirektoratet. 2021. Strategi for Fagfeltet Arbeid og Helse. Oslo: Arbeids- og velferdsdirektoratet og Helsedirektoratet.
- Banks, Lena Morgon, Arne H. Eide, Xanthe Hunt, Ola Abu Alghaib, and Tom Shakespeare. 2023. “How Representative Are Organisations of Persons with Disabilities? Data from Nine Population-Based Surveys in Low- and Middle-Income Countries.” Disability & Society 1–17. https://doi.org/10.1080/09687599.2023.2215397
- Bjørnshagen, Vegar, and Elisabeth Ugreninov. 2021. “Disability Disadvantage: Experimental Evidence of Hiring Discrimination against Wheelchair Users.” European Sociological Review 37 (5): 818–833. https://doi.org/10.1093/esr/jcab004
- Bø, Tor Petter, and Inger Haland. 2017. “Funksjonshemma på Arbeidsmarknaden.” In Rapporter 2017/33. Oslo: Statistisk sentralbyrå.
- Bolvig, Iben, and Beatrice S. Rangvid. 2023. “Investigating Municipal and Company Influences on Employment of People with Chronic Health Conditions.” Scandinavian Journal of Public Health 0 (0): 14034948231151463. https://doi.org/10.1177/14034948231151463
- Braun, Virginia, and Victoria Clarke. 2006. “Using Thematic Analysis in Psychology.” Qualitative Research in Psychology 3 (2): 77–101. https://doi.org/10.1191/1478088706qp063oa
- Bredgaard, Thomas. 2018. “Employers and Active Labour Market Policies: Typologies and Evidence.” Social Policy and Society 17 (3): 365–377. https://doi.org/10.1017/S147474641700015X
- Carmichael, Fiona, and Harriet Clarke. 2022. “Why Work? Disability, Family Care and Employment.” Disability & Society 37 (5): 765–786. https://doi.org/10.1080/09687599.2020.1848802
- Eriksson, Erik. 2018. “Four Features of Cooptation.” Nordic Welfare Research 3 (1): 7–17. https://doi.org/10.18261/issn.2464-4161-2018-01-02
- FFO. 2019. Bruken av Kommunale Råd for Funksjonshemmede. Oppsummerende Rapport. Oslo: Funksjonshemmedes Fellesorganisasjon (FFO).
- FFO. 2021. FFOs Program 2022-2023. Oslo: FFO.
- Finnvold, Jon Erik, and Hilde Eirin Pedersen. 2012. “Alle Skal Med? Utdanning og Arbeid for Fysisk Funksjonshemmede.” Samfunnsspeilet (2): 39–45.
- Gathen, Jan Marius, Tor Slettebø, and Erik Skjeggestad. 2022. “User Participation among People in Vulnerable Situations at Service Level. A Scoping Review Exploring Impact for Individual Stakeholders and Services.” Nordic Welfare Research 7 (1): 52–67. https://doi.org/10.18261/nwr.7.1.4
- Gathen, Jan Marius, Tor Slettebø, and Erik Skjeggestad. 2023. “The Participation of People in Vulnerable Situations in Interest Organisations: A Qualitative Study of Representatives Views.” Journal of Social Policy: 1–18. https://doi.org/10.1017/S0047279423000089
- Guldvik, Ingrid, and Ole Petter Askheim. 2022. “Constructing User Participation for Disabled People—the Norwegian Context.” Disability & Society 37 (9): 1397–1416. https://doi.org/10.1080/09687599.2020.1867070
- Haukelien, Heidi, Geir Møller, and Hallvard Vike. 2011. Brukermedvirkning i Helse- og Omsorgssektoren" TF-Rapport nr,vol. 284. Bø: Telemarksforskning.
- Heidenreich, Martin, and Deborah Rice. 2016. “Introduction.” In Integrating Social and Employment Policies in Europe. Active Inclusion and Challenges for Local Governance, edited by Martin Heidenreich and Deborah Rice, 1–15. Cheltenham: Edward Elgar.
- Kuhnle, Stein, and Per Selle. 1992. Government and Voluntary Organizations: A Relational Perspective. Aldershot: Avebury.
- Künzel, Sebastian. 2012. “The Local Dimension of Active Inclusion Policy.” Journal of European Social Policy 22 (1): 3–16. https://doi.org/10.1177/0958928711425270
- Lasalvia, Antonio, Silvia Zoppei, Tine Van Bortel, Chiara Bonetto, Doriana Cristofalo, Kristian Wahlbeck, Simon Vasseur Bacle, et al. 2013. “Global Pattern of Experienced and Anticipated Discrimination Reported by People with Major Depressive Disorder: A Cross-Sectional Survey.” Lancet (London, England) 381 (9860): 55–62. https://doi.org/10.1016/S0140-6736(12)61379-8
- Lesner, Rune V. 2019. A Literature Review of Effectiveness of Employer Targeted Disability Employment Policies. Oslo: Rapport på oppdrag for sysselsettingsutvalgets ekspertgruppe.
- Mandal, R., and S. O. Ose. 2015. “Social Responsibility at Company Level and Inclusion of Disabled Persons: The Case of Norway.” Scandinavian Journal of Disability Research 17 (2): 167–187. https://doi.org/10.1080/15017419.2013.814586
- Nav. 2019. Follow-up of Sick Leave. Oslo: Nav.
- NOU. 2019. Arbeid og Inntektssikring. Oslo: Arbeids- og sosialdepartementet.
- NOU. 2021. Kompetanse, Aktivitet og Inntektssikring—Tiltak for Økt Sysselsetting. Oslo: Arbeids- og sosialdepartementet.
- OECD/European Union. 2016. Health at a Glance: Europe 2016. State of Health in the EU Cycle. Paris: OECD Publishing.
- Olsen, Jason. 2022. “Employers: Influencing Disabled People’s Employment through Responses to Reasonable Adjustments.” Disability & Society 1–20. https://doi.org/10.1080/09687599.2022.2099251
- Proba samfunnsanalyse. 2022. “Erfaringer Med Lovpålagte Råd for Medvirkning. Utarbeidet for KS.” In Proba-Rapport nr. 2022-01. Oslo: Proba samfunnsanalyse.
- Rommetvedt, Hilmar. 2022. Politikkens Allmenngjøring. Stortinget, Regjeringen og de Organiserte Interessene i et Nypluralistisk Demokrati. Bergen: Fagbokforlaget.
- Rydland, Håvard Thorsen, Henrik Litleré Bentsen, Rune Ervik, Kjersti Grønning, Kamrul Islam, Egil Kjerstad, Tord Skogedal Lindén, et al. 2022. “Promoting Labour Market Inclusion of the Chronically Ill: A Scoping Review of Scandinavian Countries’ Efforts.” Scandinavian Journal of Public Health 51 (8): 1097–1107. https://doi.org/10.1177/14034948221096005
- Sandvin, Johans Tveit, Christian Lo, and Janne Paulsen Breimo. 2022. “På Stedet Hvil? En Kritisk Analyse av Norsk Forskning om Samhandling i Helse- og Omsorgstjenesten.” Tidsskrift for Samfunnsforskning 63 (2): 141–153. https://doi.org/10.18261/tfs.63.2.4
- Schafft, Angelika. 2007. “Ansettelse av Personer Med Psykiske Lidelser i Ordinære Bedrifter: Vi må Forstå Arbeidsgivernes Grunner.” Tidsskrift for Psykisk Helsearbeid 4 (3): 254–261. https://doi.org/10.18261/ISSN1504-3010-2007-03-03
- Sivesind, Karl Henrik, and Bernard Enjolras. 2022. Frivillige Organisasjoners Sivilsamfunnsrolle: Påvirkningsstrategier og Tilgang Til Politiske Beslutningsfora. Rapport 2022:3. Oslo: Senter for forskning på sivilsamfunn & frivillig sektor.
- United Nations Department of Economic and Social Affairs. 2006. Convention on the Rights of Persons with Disabilities and Optional Protocol. New York: Department of Economic and Social Affairs.
- United Nations Department of Economic and Social Affairs. 2015. Sustainable Development Goals. New York: Department of Economic and Social Affairs.
- United Nations. 1948. "Universal Declaration of Human Rights.” Paris: UN, https://www.un.org/sites/un2.un.org/files/2021/03/udhr.pdf.
- Willoch, Knut. 1950. “Landsnemd for de Delvis Arbeidsføres Organisasjoner. Et Betydningsfullt Tiltak.” In Trygd og Arbeid. Organ for Tuberkuløses Hjelepeorganisasjon 10: 16–17.
