
Abstract
Previous reviews have highlighted parent–child connectedness and communication as important protective factors against adolescent substance use. However, these reviews focus on single substances such as alcohol. An integrative review of the literature was conducted to examine which elements of parent–child connectedness and substance-use specific communication are effective across adolescent alcohol, tobacco and drug use. Forty-two English language, peer reviewed articles were reviewed. Open communication occurs within the context of high connectedness between parents and their children. Conversations about health risks are associated with lower levels of substance use while more frequent conversations, those about parents’ own use, permissive messages and consequences of use are associated with higher levels of use. There are disparities regarding conversations about use of each substance: alcohol and tobacco are easier topics of conversation while drug use is rarely discussed. Parental alcohol and tobacco use can influence the credibility of their communication with their child. Parents should be encouraged to have open, constructive, credible, two-sided conversations with their adolescents about substance use. Interventions to improve parents’ communication skills around substance use, particularly drug use, should include the types of approaches and messages highlighted in this review, and, where possible, these interventions should include all family members.
Introduction
Alcohol, tobacco and drug use tends to begin in adolescence (Bonomo & Proimos, Citation2005; Howlett, Williams, & Subramaniam, Citation2012; Mirza & Mirza, Citation2008). Early initiation is associated with greater likelihood of more frequent use and substance misuse problems (Bremner, Burnett, Nunney, & Mistral, Citation2011; Feinstein, Richter, & Foster, Citation2012). Many factors have been identified which influence the likelihood that adolescents will use substances (Hawkins, Catalano, & Miller, Citation1992). Family and parenting factors receive a great deal of attention in this literature (Velleman, Templeton, & Copello, Citation2005; Velleman & Templeton, Citation2007; Velleman, Citation2009). Parent–child connectedness (PCC) and communication have been highlighted as potential protective factors against substance use and misuse in adolescence. They have recently received increased attention in social science; are highly relevant to current policy which prioritises early intervention within the context of the family (Jackson, Haw, & Frank, Citation2011; Scottish Government, Citation2008); and have been promoted in prevention programmes (Mares, van der Vorst, Engels, & Lichtwarck-Aschoff, Citation2011; van der Vorst, Burk, & Engels, Citation2010). While other parenting and non-parenting factors might be important, the purpose of this review was to examine PCC and communication as these factors are core elements of good parenting and are amenable to change via family-based interventions (DeVore & Ginsburg, Citation2005; Jackson et al., Citation2011; Newman, Harrison, Dashiff, & Davies, Citation2008). Furthermore, gaining a greater understanding of these protective factors can influence future parenting interventions to delay or reduce adolescent substance use.
PCC has gained recognition in recent years due to its apparent protective effects in terms of adolescent health and development (Barber & Schluterman, Citation2008; Townsend & McWhirter, Citation2005). PCC has been described as feelings of closeness, warmth, love and satisfaction a child has with their parents; as relationships and bonds between parents and children (Barber & Schluterman, Citation2008; Markham et al., Citation2010; Resnick et al., Citation1997; Townsend & McWhirter, Citation2005). While there is no consistent definition, Lezin and colleagues’ definition has been adopted for this paper: “by the quality of the emotional bond between parent and child and by the degree to which this bond is both mutual and sustained over time” (emphasis in original) (Lezin, Rolleri, Bean, & Taylor, Citation2004). Barber and Schluterman (Citation2008) note that the concept of attachment is assessed in an entirely different manner to PCC, although there may be similarities. Attachment refers to a one-sided relationship between parent, often mother, and child, with the caregiver playing an active role; within PCC, both parents and children play active roles in the relationship (Lezin et al., Citation2004). Thus, there are significant differences between attachment and PCC in the literature.
Parent–child communication is a key part of connectedness (Lezin et al., Citation2004) and refers to whether adolescents and parents feel they can talk to each other about a range of topics, including general areas of interest and more sensitive issues such as substance use and sex (Markham et al., Citation2010; Ryan, Jorm, & Lubman, Citation2010). The extent to which adolescents can talk to their parents about broad issues, such as their activities, feelings and topics which interest them, is often referred to as general communication (Ryan et al., Citation2010,Citation2011). Such communication has been measured in terms of satisfaction, frequency and quality, and in a number of studies, the views of both parents and adolescents have been sought. Specific communication refers to targeted conversations about alcohol, tobacco and drug use that parents have with their children, covering a range of topics, such as depictions in the media, negative effects and risks of using substances (Ryan et al., Citation2010). These types of conversations are regularly promoted in prevention campaigns (Miller-Day & Dodd, Citation2004).
Previous reviews of the literature have suggested that both PCC and communication are protective against substance use during adolescence (Kingon & O’Sullivan, Citation2001; Ryan et al., Citation2010). There is also evidence that interventions involving parenting sessions, including strengthening relationships and communication, may be effective in reducing and preventing alcohol (Foxcroft & Tsertsvadze, Citation2011) and tobacco use (Thomas, Baker, Thomas, & Lorenzetti, Citation2015); there is limited evidence in terms of drug use (Gates, McCambridge, Smith, & Foxcroft, Citation2009). However, the findings of these reviews are somewhat limited. Firstly, PCC and communication tend to be considered separately, despite an important interaction between the two (Lezin et al., Citation2004). Secondly, alcohol, tobacco and drug use have been examined separately. In their systematic review, Ryan et al. (Citation2010) only considered alcohol use. Although it is understandable that substances are examined separately, given their differing legal frameworks and social acceptability of use, we argue that it is crucial to examine alcohol, tobacco and drug use together in one review. Adolescents tend to use more than one substance at a time (Fraga, Sousa, Ramos, Dias, & Barros, Citation2011; Torabi, Bailey, & Majd-Jabbari, Citation1993) so focussing on one substance, such as alcohol, does not necessarily reflect the reality of their use. Also, given that the legal status of each substance is different, parents may have different views on smoking and alcohol compared to drugs. For example, Mallick (Citation2003) found that communication about drug use is incredibly challenging for parents, particularly due to the stigma attached to use. Finally, while communication has been shown to be protective, there is little information regarding which specific elements are effective, and should therefore be promoted. It may be that there are specific types of communication that are more effective than others. Thus, in order to address the gaps in the literature, an integrative review of the literature was conducted. This review aimed to answer the following question: What elements of connectedness and communication are important in delaying and reducing adolescent alcohol, tobacco and drug use?
Methods
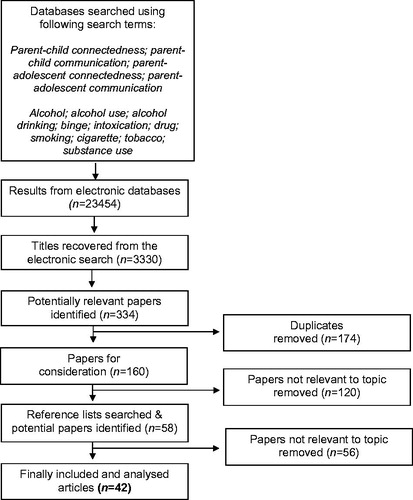
Using the method outlined by Whittemore and Knafl (Citation2005) for conducting integrative literature reviews, a comprehensive and rigorous search of the literature was conducted. Six health and social science databases were searched for papers published between January 2004 and March 2016; this time period was chosen to ensure that the literature being reviewed was contemporary. The databases searched were PsycINFO, Psychology and Behavioural Sciences Collection (PBSC), Applied Social Sciences Index and Abstracts (ASSIA), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Medical Literature Analysis and Retrieval System Online (MEDLINE) and Web of Science. The inclusion criteria were (i) adolescents (aged 10–19 years of age; reflecting the World Health Organisation (Citation2015) definition of adolescence); (ii) English language; (iii) peer-reviewed; (iv) original research, using any study design; (v) related to smoking or alcohol or drug use; and (vi) related to parent–child communication and/or connectedness. As there is a lack of universal definition of PCC, a decision was made to include studies which involved research into emotional bonds and relationships with parents. Reference lists of relevant papers were also searched by hand for potentially useful studies, eliciting ten papers. In total, 42 articles were included in the review. The details of the literature search process are presented in . Of these studies, 21 used a longitudinal survey design; 14 used a cross-sectional survey design; and seven were qualitative, utilising mostly individual interviews, with either adolescents or parents. Including both qualitative and quantitative studies, despite their different approaches and analyses, should provide a deeper and more comprehensive understanding of the topic (Whittemore & Knafl, Citation2005). Sixteen studies were conducted with adolescents only, 24 with both parents and adolescents and two studies with parents only. The follow-up period from the longitudinal studies ranged from one to 5 years. The vast majority of studies (n = 20) were conducted in the United States of America (USA) and the Netherlands (n = 18), with the remainder conducted in the United Kingdom (UK) (n = 2), Canada (n = 1) and New Zealand (n = 1).
Figure 1. Flow chart of article selection.
Papers were rejected if they did not meet the inclusion criteria. Papers were initially divided into three subject areas, PCC, general communication and substance use specific communication, and examined separately. Within these subgroups, papers were examined in terms of the methodology used; cross-sectional and longitudinal survey studies were considered independently of qualitative studies. The key features of each paper, such as sample size, methods used and outcomes measured, were recorded in a database, to assess the quality of the literature. Whittemore and Knafl (Citation2005) highlight the difficulty of quality appraisal in integrative reviews, as studies with different research designs are often included in one review. The quality of quantitative and qualitative studies were assessed separately using the tools developed by Crombie (Citation1996) and Critical Appraisal Skills Programme (Citation2013), respectively. Each paper was read a number of times to extract the key findings, which were coded and entered into a database to allow for comparison. These codes were then compared to identify patterns and similarities and differences were identified within these patterns. Finally, major themes were identified and then synthesised, to provide a “comprehensive portrayal of the topic of concern” (Whittemore & Knafl, Citation2005, p. 551).
A meta-analysis was not deemed appropriate for this review, due to the nature of the studies included. Meta-analyses are often performed using randomised controlled trials (RCTs) in which there are similar measureable outcomes (Crombie & Davies, Citation2009). The studies included in our review mostly used cross-sectional or longitudinal survey data and the outcomes were somewhat diverse. For example, some studies examined initiation of substance use, others measured rates of use while some measured attitudes towards substance use. Thus, an integrative review was deemed a more appropriate choice. The details of each paper are presented in .
Table 1. Included studies (n = 42).
Findings
Importance of PCC and the influence of parents’ behaviours
Communication is most effective within the context of high levels of PCC (Ackard, Neumark-Sztainer, Story, & Perry, Citation2006; Bandi, Cokkinides, Westmaas, & Ward, Citation2008; Carter, McGee, Taylor, & Williams, Citation2007; Guilamo-Ramos, Bouris, Dittus, & Jaccard, Citation2008; Horton & Gil, Citation2008; Kulbok et al., Citation2010; Razzino et al., Citation2004). Adolescents are more likely to display open communication with their parents about general topics when they have high PCC (Luk, Farhat, Iannotti, & Simons-Morton, Citation2010). Parents are more likely to have the opportunity to have frequent conversations and set rules effectively when PCC is high (Cleveland, Gibbons, Gerrard, Pomery, & Brody, Citation2005; Guilamo-Ramos et al., Citation2008; Harakeh, Scholte, Vermulst, de Vries, & Engels, Citation2010; Koning, Van den Eijnden, & Vollebergh, Citation2014; Maggi et al., Citation2014). In Chaplin and colleagues’ (Chaplin et al., Citation2014) observational study adolescents’ physiological responses were measured during conversations with parents; when parents displayed behaviours suggestive of low PCC, such as criticism and sarcasm, adolescents tended to display higher cortisol levels, which were indicative of greater feelings of discomfort. In terms of smoking, when there are high levels of PCC, adolescents may not wish to disappoint their parents by using cigarettes (Kulbok et al., Citation2010; Levy et al., Citation2010). When PCC is low, smoking is viewed as an act of rebellion, which may increase their motivation to start (Maggi et al., Citation2014). High PCC is effective in reducing substance use behaviours and adolescents’ fear of disappointment may be particularly motivating.
Parents’ behaviour appears to have an influence within PCC. A moderate level of control, supervision and monitoring is viewed, by both parents and academics, as ideal, particularly around alcohol use, with attempts to ensure that adolescents have a sensible relationship with alcohol (Bourdeau, Miller, Vanya, Duke, & Ames, Citation2012; Guilamo-Ramos, Jaccard, Turrisi, & Johansson, Citation2005). Parents believe that role modelling behaviour around alcohol use, either through abstinence or low alcohol use, is important in delaying or preventing adolescent alcohol use (Bourdeau et al., Citation2012). Such behaviours are unlikely to be taken on board when PCC is low. In their cross-sectional study, Tilson, McBride, Lipkus, & Catalano (Citation2004) found that the protective effect of PCC disappeared when parents smoked, suggesting an influence of parental behaviour regardless of relationship quality. Parents’ own smoking and alcohol use were found to affect their communication with adolescents in four studies (Harakeh et al., Citation2010; Levy et al., Citation2010; Maggi et al., Citation2014; Mares et al., Citation2011). Communication was particularly affected by parental smoking, with parents and adolescents describing conversations about not smoking as inappropriate when parents smoked, with adolescents ignoring these messages (Guilamo-Ramos et al., Citation2008; Levy et al., Citation2010; Maggi et al., Citation2014). Thus, parents’ behaviours towards their children and in terms of their own substance use are influenced by PCC and can affect adolescents’ substance use. These findings highlight the importance of examining PCC and communication together, as the relationships between parents and teenagers can have a considerable impact on their conversations about substance use and subsequent behaviours.
Methods of communication
Parents and adolescents have highlighted the importance of clear messages and open communication when discussing substance use (Guilamo-Ramos et al., Citation2008; Highet, Citation2005; Kulbok et al., Citation2010; Sherriff, Cox, Coleman, & Roker, Citation2008). The way in which parents talk to their children about substance use is crucial; when they are perceived as lecturing them, adolescents are often unreceptive and do not assimilate these messages (Guilamo-Ramos et al., Citation2008; Levy et al., Citation2010; Maggi et al., Citation2014; Metzger et al., Citation2013; Sherriff et al., Citation2008). Having constructive conversations in which parents and children participate equally appears to be more effective (Chaplin et al., Citation2014; Highet, Citation2005). When conversations are open and involve discussions rather than lectures, adolescents feel more comfortable and report lower rates of substance use (Chaplin et al., Citation2014). In terms of alcohol use, parents feel that it is necessary to negotiate boundaries around drinking behaviour, preferring to use a harm reduction than an abstinence based approach (Bourdeau et al., Citation2012; Highet, Citation2005; Sherriff et al., Citation2008). As might be expected, such an approach does not extend to smoking and drug use, when adolescents are specifically told not to engage in these behaviours (Highet, Citation2005; Levy et al., Citation2010; Maggi et al., Citation2014). In six studies, parents reported a range of issues when communicating with their children about substance use. Difficulties in starting conversations and concerns about providing inconsistent messages were highlighted by parents (Bourdeau et al., Citation2012; Sherriff et al., Citation2008). Parental worries about adolescent substance use often influenced how they communicated with their children, by avoiding having these discussions (Levy et al., Citation2010) and by providing lower quality communication (Koning, van den Eijnden, Glatz, & Vollebergh, Citation2013). There are disparities in terms of parents’ and adolescents’ experiences of the frequency of communication. Parents think they are talking more frequently about substance use than their children do (Nonnemaker, Silber-Ashley, Farrelly, & Dench, Citation2012; van der Vorst, Engels, Meeus, Deković, & Van Leeuwe, Citation2005), suggesting that either this communication is ineffective or adolescents fail to digest it. Parents appear to struggle to find a balance between discussing substance use with their children and lecturing them. When they lecture, adolescents are unlikely to take these messages on board. Open communication which is based on two-way conversations is crucial.
Frequency vs. Quality
Sixteen studies highlighted the differences between frequent and high quality communication about substance use. More frequent communication is associated with higher rates, more positive attitudes towards and lower self-efficacy to refuse cigarette use (de Leeuw et al., Citation2008,Citation2010; Harakeh, Scholte, de Vries, & Engels, Citation2005, Harakeh, Engels, Den Exter Blokland, Scholte, & Vermulst, Citation2009; Harakeh et al., Citation2010; Hiemstra, Otten, & Engels, Citation2012; Huver, Engels, & de Vries, Citation2006; Otten, van der Zwaluw, van der Vorst, & Engels, Citation2008); higher rates of alcohol use and associated problems (van den Eijnden, van de Mheen, Vet, & Vermulst, Citation2011; Koning et al., Citation2013; Spijkerman, van den Eijnden, & Huiberts, Citation2008; van der Vorst et al., Citation2005,Citation2010); and higher rates of cannabis use initiation (Nonnemaker et al., Citation2012). It is unclear as to the direction of this relationship: parents’ frequent communication may be ignored and adolescents start using substances; or parents communicate more frequently when they believe their adolescents are using substances. The authors have suggested that the latter may be the case but longitudinal studies are required to examine the direction of the relationship (Harakeh et al., Citation2005, 2009, 2010; Huver et al., Citation2006; van der Vorst et al., Citation2005). High quality communication, conversely, is associated with lower rates of smoking, more negative attitudes and higher self-efficacy to refuse cigarette use (de Leeuw et al., Citation2008; Harakeh et al., Citation2005,Citation2010; Otten et al., Citation2008; Ringlever, Otten, de Leeuw, & Engels, Citation2011; Scholte, Vermulst, & Engels, Citation2010); lower rates of alcohol use and higher self-efficacy to refuse (van den Eijnden et al., Citation2011; Koning et al., Citation2013; Mares, Lichtwarck-Aschoff, & Engels, Citation2013; Spijkerman et al., Citation2008). While Koning et al. (Citation2014) found no association between quality of communication and alcohol use, they still promote the use high quality conversations. Three studies found that frequent communication was indirectly protective against alcohol, tobacco and cannabis use, only when combined with high quality communication and high PCC (Cleveland et al., Citation2005; Huansuriya, Siegel, & Crano, Citation2014; Huver, Engels, Vermulst, & de Vries, Citation2007). Thus, having frequent conversations with adolescents about substance use is not enough; these conversations must also be of high quality, in which communication is reciprocal and adolescents feel they are participating equally. When adolescents are frequently told not to drink alcohol, smoke or take drugs, they may ignore the information from their parents. However, when these conversations are of high quality and are based on high PCC and open communication, the messages are more effective. Mares et al. (Citation2011) found that when parents had more alcohol related problems, they talked more to their children, with more frequent communication associated with lower rates of alcohol use and fewer alcohol related problems. For those living in environments in which alcohol use is problematic, more frequent conversations may have a positive effect, by encouraging adolescents to drink less. However, generally, more frequent communication without high quality messages and high PCC can be detrimental.
Harder vs. softer communication
Parents report using a wide range of messages when communicating with their children about substance use, including rules, health risks, consequences, moderation and the law (Bourdeau et al., Citation2012; Sherriff et al., Citation2008). Ennett, Bauman, Foshee, Pemberton, & Hicks (Citation2001) made the distinction between “harder” and “softer” communication. Harder communication involves conversations in which parents specifically tell their children not to use substances and present them with particular rules around use, while softer communication involves conversations about the possible consequences and harms (Ennett et al., Citation2001). When parents only talk to their children about rules and tell them not to use substances, adolescents feel threatened and report increased rates of alcohol, tobacco and drug use (Chaplin et al., Citation2014; Huver et al., Citation2006; Kam, Citation2011), although in one study the results were positive but not statistically significant (Nonnemaker et al., Citation2012). In a qualitative study, adolescents reported that when their parents use such communication, they tend to ignore what is said (Maggi et al., Citation2014). Conversely, younger, but not older, adolescent smokers reported higher readiness to quit when told by their parents not to smoke (Bandi et al., Citation2008). For young smokers, being told not to smoke may be beneficial. It is apparent that harder communication leads to feelings of discomfort by adolescents, they ignore these messages and may use alcohol, tobacco and drugs regardless of what their parents have told them. Softer communication, however, is viewed more positively (Guilamo-Ramos et al., Citation2008; Kulbok et al., Citation2010; Maggi et al., Citation2014). When parents include messages about health risks and potential consequences of use, adolescents are less likely to use substances (Chaplin et al., Citation2014; Huver et al., Citation2006). However, in one study, discussion of consequences had no effect on alcohol use (Reimuller, Hussong, & Ennett, Citation2013) and in another had a detrimental effect on cannabis use initiation (Nonnemaker et al., Citation2012). Talking about consequences of use has a detrimental effect unless these conversations involve discussions of health risks. Overall, harder communication is only effective when communication is of high quality; and softer communication is beneficial when adolescents are informed about health risks and when these messages are educational and informative (Chaplin et al., Citation2014; Maggi et al., Citation2014).
Disclosures
Parents often talk about their own or others’ substance use as a way of initiating conversations and to convey messages about health risks (Guilamo-Ramos et al., Citation2008; Kulbok et al., Citation2010; Sherriff et al., Citation2008). However, such an approach may be detrimental, increasing substance use. When mothers reported high levels of alcohol use, they were more likely to talk about their own negative experiences of alcohol use and when they did so, adolescents were more likely to consume greater amounts of alcohol (Handley & Chassin, Citation2013). Parental disclosures are also associated with more favourable beliefs towards substance use behaviour (Kam & Middleton, Citation2013). One study, however, found that parental disclosures were associated with higher self-efficacy to refuse alcohol (Mares et al., Citation2013). Thus, parents should exercise caution when discussing their own negative experiences, particularly around alcohol use, as they may normalise these behaviours for their children, leading to increased use.
Alcohol is acceptable but tobacco and drugs are not
A common theme throughout the literature was that parents deal with alcohol, tobacco and drug use differently. Alcohol is viewed as a normal, acceptable behaviour for adults, and to some extent adolescents, particularly in the UK. In the study by Bourdeau et al. (Citation2012) most parents stated that alcohol use by their adolescent was either forbidden or limited to particular drinks or occasions. However, a number of parents reported both types of rules, suggesting a lack of consistency in their messages around alcohol use. One of the central messages promoted by parents in another study was that alcohol, when used in moderation, is a normal part of life; parents reported trying to limit the types of alcohol their adolescents could drink and the occasions and locations in which alcohol use was allowed (Sherriff et al., Citation2008). Parents attempt to negotiate boundaries around alcohol use and ensure that adolescents drink safely and in moderation, as well as providing information about the risks and harms (Highet, Citation2005). However, inconsistent rules around alcohol use may be confusing for young people and therefore increase use (Koning et al., Citation2013). Smoking is often forbidden or opposed, even when parents themselves smoke (Kulbok et al., Citation2010; Levy et al., Citation2010), possibly due to the perceived health risks associated with smoking. Drugs are viewed as particularly harmful and, as a result, are often difficult to discuss. In one study, adolescents noted that their parents frequently discussed alcohol use, but rarely discussed cannabis use, with discussions only occurring after they had been caught using (Highet, Citation2005). Permissive messages and inconsistent rules around alcohol use can be confusing and increase use (Koning et al., Citation2013; Reimuller et al., Citation2013), while forbidding the use of tobacco and drugs can also increase use (Chaplin et al., Citation2014; Huver et al., Citation2006; Kam, Citation2011). More research is required to examine communication around drug use, with Highet (Citation2005) stressing that parents need to talk to young people about drugs before problematic use occurs.
Thus, alcohol use is viewed as normal and inevitable, tobacco use is discouraged and drug use is forbidden and hidden. This is reflected in the focus of the studies included in this review, with 14 examining alcohol use, 17 smoking and 9 examining a range of substances; only two studies focussed specifically on cannabis use. The stronger focus on alcohol and tobacco than drug use may be due to drugs being less acceptable to consume, more difficult to talk about and therefore study. Examining alcohol, tobacco and drug use together in one review provides a greater understanding of the complexities of communication about substance use.
Discussion
As far as we are aware, this is the first integrative review to examine the specific elements of parent–child connectedness and communication in the context of adolescents’ alcohol, tobacco and drug use. Previous reviews suggested that good general communication is protective against alcohol use (Ryan et al., Citation2010); and that high levels of connectedness are protective against all three substances (Kingon & O’Sullivan, Citation2001). This review adds to the evidence base in two ways: firstly, it encompassed a wider assessment of the literature, examining the three related factors across all substances. This is important as adolescents do not tend to view alcohol, tobacco and drugs as distinct substances, both legally and in terms of use, so it seems illogical for such substances to be examined separately in the literature. Secondly, it provides an enhanced understanding of the key elements of the interaction between PCC and communication and how these influence adolescent substance use.
Despite some conflicting findings, the findings of this review suggest that high levels of PCC and good quality general and substance use specific communication are protective against adolescent alcohol, tobacco and drug use. By examining PCC and communication together, this review provides new insight by highlighting the importance of PCC on communication practises. When PCC is high, communication is open, frequent and adolescents feel comfortable; when PCC is low, communication is stilted. Darling and Steinberg's (Citation1993) model contextualises and provides a theoretical understanding for our findings, that communication is effective only when PCC is high. This model highlights the moderating relationship between parenting behaviours, such as PCC, and communication about substance use. Others have used this model to contextualise their findings, that general and substance use specific parenting practises influence adolescent substance use, suggesting the importance of considering the theoretical foundation of future studies within the context of parenting practises (de Leeuw et al., Citation2010; Handley & Chassin, Citation2013; Harakeh et al., Citation2010; Huver et al., Citation2006,Citation2007; Koning et al., Citation2014). Conversations about substance use must be two-sided, involving explanations around the health implications of using substances. Parents and adolescents endorse the use of substance-use specific communication but face challenges in initiating these conversations, particularly when discussing drug use. More frequent conversations, discussing rules and consequences of use and permissive messages should be discouraged. There appears to be a difference between enforcing rules and simply talking about them: when parents enforce rules around substance use, young people report lower use, but when they just talk to them about rules, without actually making an attempt to enforce the rules, they are more likely to drink alcohol, smoke or use drugs. It may be that talking about rules makes young people feel uncomfortable, as suggested by Chaplin et al. (Citation2014); or that rules are dismissed when they are discussed but not enforced by parents. The findings of Huver et al. (Citation2006) highlight this distinction: enforcing rules is associated with lower rates of smoking, but communication about rules is associated with higher rates. Future studies should examine whether disclosures of parental use are associated with negative outcomes when PCC is high, as the evidence is mixed in terms of the effects of these conversations. The most crucial message of the literature, by far, is that simply having frequent conversations is not enough; these conversations must be of high quality in order to be protective. When communication is two-sided and young people feel they are being listened to and contributing, rather than being lectured, it is viewed as high quality. By examining alcohol, tobacco and drug use together, this review provides new insight by highlighting the different experiences in terms of talking about alcohol compared to tobacco and drug use. Alcohol appears to be much easier to talk about and parents often attempt to negotiate boundaries and monitor use. Tobacco and drug use, conversely, are much more difficult topics to address. Their use is forbidden and discouraged, making the topic much more hidden. Drug use, in particular, is a virtually hidden topic and parents and young people may be afraid to address it. Combining all three substances provides a deeper understanding of the complexity of substance use communication than would be gained studying each substance alone.
Limitations
Despite these generally consistent and comprehensive findings, a number of limitations were observed. The sample size of included studies varied greatly, ranging from 116 (Chaplin et al., Citation2014) to 11,728 (Nonnemaker et al., Citation2012) participants. Studies varied in terms of how the concepts of PCC and communication were defined and measured, as well as how substance use was measured. The findings may also be limited by the majority of studies using cross-sectional designs, in that causal inferences cannot be made. There are also a number of caveats of this integrative review. Firstly, only English language papers were included, which may bias the results. Secondly, it is important to recognise that 20 studies were conducted in the USA and 18 in the Netherlands. While the findings of these studies may be applicable to other populations, there are cultural and policy differences. For example, the legal drinking age in the Netherlands, like the majority of European countries, is 18 years, compared to 21 years in the USA (Jernigan, n.d.). The law in the Netherlands has recently changed, so that when these studies were conducted, the legal drinking age was 16 years (Dutch Institute for Alcohol Policy (STAP), Citation2013). Thus, future research is required in other countries to examine whether such findings are replicable, as well as to explore differences in parenting styles in countries with more liberal views and laws, and how such practises might affect communication about substance use. Finally, the aim of this review was to examine the diverse literature on three key potentially protective factors across a range of substance use behaviours; meta-analysis was not possible. While integrative reviews may be viewed as the lacking rigour and objectivity of systematic reviews and meta-analysis, the methods used in this review were comprehensive and rigorous, using the approaches specified by Whittemore & Knafl (Citation2005).
Conclusion and implications
The current integrative review of the literature provides important evidence that PCC, general communication and particular types of substance-use specific communication can be protective against alcohol, tobacco and drug use in adolescence. Parents should be encouraged to have open, credible, high quality conversations with their adolescents about substance use, which are facilitated by high quality general communication and high levels of PCC. High quality conversations should be “constructive and respectful” (de Leeuw et al., Citation2010, p. 1003), in which parents and adolescents feel comfortable and understood and that their opinions matter and are being taken seriously. Parents should be encouraged to talk about health risks and potential consequences of use when communicating about substance use. Having frequent conversations, involving discussions of their own use and about rules is not enough. Parents should also be provided with support to ensure that they have high levels of connectedness with their children are good and consequently, that the conversations they have are informative, of high quality and effective. This review highlights the importance of PCC and substance use specific communication on adolescent substance use; future research should examine the effect of both these factors, as currently, they are being studied separately. Future studies should also examine the nature of communication, in which adolescents and parents discuss the benefits and harms of substance use within the context of parental rule setting.
The findings suggest that family setting is important within the context of PCC and communication, with the majority of studies being conducted with two-parent families. Therefore, more research is required with single parents, particularly fathers, and with children who are not living with their biological parents, such as those looked after by the state. Further research is required to evaluate the effectiveness of interventions which include the specified elements of PCC and communication. Three Cochrane reviews have examined family-based interventions, showing positive effects for alcohol and tobacco use (Foxcroft & Tsertsvadze, Citation2011; Thomas et al., Citation2015), but not drug use (Gates et al., Citation2009). Thus, interventions can improve PCC and substance use communication between parents and children, although further research is required in terms of young people’s drug use. In light of these findings, we recommend that interventions, similar to those included in the above reviews, which aim to improve PCC and encourage parents to include the specific elements of communication identified as protective, are made available to parents.
Declaration of interest
The authors report no conflicts of interest and received no funding to conduct this review.
References
- Ackard, D.M., Neumark-Sztainer, D., Story, M., & Perry, C. (2006). Parent-child connectedness and behavioural and emotional health among adolescents. American Journal of Preventive Medicine, 30, 59–66. http://doi.org/10.1016/j.amepre.2005.09.013
- Bandi, P., Cokkinides, V.E., Westmaas, J.L., & Ward, E. (2008). Parental communication not to smoke and adolescent cigarette smokers' readiness to quit: differences by age. Journal of Adolescent Health, 43, 612–615. http://doi.org/10.1016/j.jadohealth.2008.04.019
- Barber, B.K. & Schluterman, J.M. (2008). Connectedness in the lives of children and adolescents: a call for greater conceptual clarity. Journal of Adolescent Health, 43, 209–216. http://doi.org/10.1016/j.jadohealth.2008.01.012
- Bonomo, Y. & Proimos, J. (2005). ABC of adolescence: substance misuse: Alcohol, tobacco, inhalants, and other drugs. British Medical Journal, 330, 777–780. http://doi.org/http://dx.doi.org/10.1136%2Fbmj.330.7494.777
- Bourdeau, B., Miller, B., Vanya, M., Duke, M., & Ames, G. (2012). Defining alcohol-specific rules among parents of older adolescents: moving beyond no tolerance. Journal of Family Communication, 12, 111–128. http://doi.org/10.1080/15267431.2011.561140.Defining
- Bremner, P., Burnett, J., Nunney, F., & Mistral, W. (2011). Young people, alcohol and influences. A study of young people and their relationship with alcohol. York. Retrieved from http://www.jrf.org.uk/publications/young-people-alcohol-and-influences
- Carter, M., McGee, R., Taylor, B., & Williams, S. (2007). Health outcomes in adolescence: associations with family, friends and school engagement. Journal of Adolescence, 30, 51–62. http://doi.org/10.1016/j.adolescence.2005.04.002
- Chaplin, T.M., Hansen, A., Simmons, J., Mayes, L.C., Hommer, R.E., & Crowley, M.J. (2014). Parental-adolescent drug use discussions: physiological responses and associated outcomes. Journal of Adolescent Healthealth, 55, 730–735. http://doi.org/10.1016/j.jadohealth.2014.05.001
- Cleveland, M.J., Gibbons, F.X., Gerrard, M., Pomery, E.A., & Brody, G.H. (2005). The impact of parenting on risk cognitions and risk behaviour: a study of mediation and moderation in a panel of African American adolescents. Child Development, 76, 900–916. http://doi.org/10.1111/j.1467-8624.2005.00885.x
- Critical Appraisal Skills Programme. (2013). Qualitative research checklist. Oxford. Retrieved from http://media.wix.com/ugd/dded87_29c5b002d99342f788c6ac670e49f274.pdf
- Crombie, I.K. (1996). The pocket guide to critical appraisal. London: BMJ Publishing Group
- Crombie, I.K. & Davies, H.T. (2009). What is meta-analysis? Evidence Based Medicine (Vol. 16). Oxford. Retrieved from http://www.medicine.ox.ac.uk/bandolier/painres/download/whatis/Meta-An.pdf
- Darling, N. & Steinberg, L. (1993). Parenting style as context: An integrative model. Psychological Bulletin, 113, 487–496. http://doi.org/http://psycnet.apa.org/doi/10.1037/0033-2909.113.3.487
- de Leeuw, R.N.H., Scholte, R.H.J., Harakeh, Z., van Leeuwe, J. F.J., & Engels, R. C. M. E. (2008). Parental smoking-specific communication, adolescents’ smoking behaviour and friendship selection. Journal of Youth and Adolescence, 37, 1229–1241. http://doi.org/10.1007/s10964-008-9273-z
- de Leeuw, R., Scholte, R., Vermulst, A., & Engels, R. (2010). The relation between smoking-specific parenting and smoking trajectories of adolescents: How are changes in parenting related to changes in smoking? Psychology & Health, 25, 999–1021. http://doi.org/10.1080/08870440903477204
- DeVore, E. R. & Ginsburg, K. R. (2005). The protective effects of good parenting on adolescents. Current Opinion in Pediatrics, 17, 460–465. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/16012256
- Dutch Institute for Alcohol Policy (STAP). (2013). Dutch senate adopts alcohol purchasing age of 18. Retrieved from http://www.stap.nl/en/news/news.html/3531/2497/dutch-senate-adopts-alcohol-purchasing-age-of-18#p3531
- Ennett, S. T., Bauman, K. E., Foshee, V. A., Pemberton, M., & Hicks, K. A. (2001). Parent-child communication about adolescent tobacco and alcohol use: what do parents say and does it affect youth behaviour? Journal of Marriage and Family, 63, 48–62. http://doi.org/10.1111/j.1741-3737.2001.00048.x
- Feinstein, E. C., Richter, L., & Foster, S. E. (2012). Addressing the critical health problem of adolescent substance use through health care, research, and public policy. Journal of Adolescent Health, 50, 431–436. http://doi.org/10.1016/j.jadohealth.2011.12.03
- Foxcroft, D.R. & Tsertsvadze, A. (2011). Universal family-based prevention programmes for alcohol misuse in young people. Retrieved from http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD009308/pdf
- Fraga, S., Sousa, S., Ramos, E., Dias, S., & Barros, H. (2011). Alcohol use among 13-year-old adolescents: associated factors and perceptions. Public Health, 125, 448–456. http://doi.org/10.1016/j.puhe.2011.01.004
- Gates, S., McCambridge, J., Smith, L., & Foxcroft, D. (2009). Interventions for prevention of drug use by young people delivered in non-school settings. Retrieved from http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD005030.pub2/pdf
- Guilamo-Ramos, V., Bouris, A. M., Dittus, P., & Jaccard, J. (2008). Mother-adolescent communication about tobacco use in urban Puerto Rican and Dominican families. Youth & Society, 40, 86–113. http://doi.org/10.1177/0044118X07308072
- Guilamo-Ramos, V., Jaccard, J., Turrisi, R., & Johansson, M. (2005). Parental and school correlates of binge drinking among middle school students. American Journal of Public Health, 95, 894–899. http://doi.org/10.2105/AJPH.2003.018952
- Handley, E. D. & Chassin, L. (2013). Alcohol-specific parenting as a mechanism of parental drinking and alcohol use disorder risk on adolescent alcohol use onset. Journal of Studies on Alcohol and Drugs, 74, 684–693. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/23948527
- Harakeh, Z., Engels, R., Den Exter Blokland, E., Scholte, R., & Vermulst, A. (2009). Parental communication appears not to be an effective strategy to reduce smoking in a sample of Dutch adolescents. Psychology & Health, 24, 823–841. http://doi.org/10.1080/08870440802074649
- Harakeh, Z., Scholte, R. H. J., de Vries, H., & Engels, R. C. M. E. (2005). Parental rules and communication: their association with adolescent smoking. Addiction, 100, 862–870. http://doi.org/10.1111/j.1360-0443.2005.01067.x
- Harakeh, Z., Scholte, R. H. J., Vermulst, A. A., de Vries, H., & Engels, R. C. M. E. (2010). The relations between parents’ smoking, general parenting, parental smoking communication, and adolescents' smoking. Journal of Research on Adolescence, 20, 140–165. http://doi.org/10.1111/j.1532-7795.2009.00626.x
- Hawkins, J. D., Catalano, R. F., & Miller, J. Y. (1992). Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psychological Bulletin, 112, 64–105. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1529040
- Hiemstra, M., Otten, R., & Engels, R. C. (2012). Smoking onset and the time-varying effects of self-efficacy, environmental smoking, and smoking-specific parenting by using discrete-time survival analysis. Journal of Beh, 35, 240–251. http://doi.org/10.1007/s10865-011-9355-3
- Highet, G. (2005). Alcohol and cannabis: Young people talking about how parents respond to their use of these two drugs. Drugs: Education, Prevention, and Policy, 12, 113–124. http://doi.org/10.1080/09687630412331315125
- Horton, E. G. & Gil, A. (2008). Longitudinal effects of family factors on alcohol use among African American and White non-Hispanic males during middle school. Journal of Child & Adolescent Substance Abuse, 17, 57–73. http://doi.org/10.1080/15470650802292780
- Howlett, K. D., Williams, T., & Subramaniam, G. (2012). Understanding and treating adolescent substance abuse: A preliminary review. Focus, 10, 293–299. http://doi.org/http://dx.doi.org/10.1176/appi.focus.10.3.293
- Huansuriya, T., Siegel, J. T., & Crano, W. D. (2014). Parent-child drug communication: Pathway from parents' ad exposure to youth's marijuana use intention. Journal of Health Communication, 19, 244–259. http://doi.org/10.1080/10810730.2013.811326
- Huver, R. M. E., Engels, R. C. M. E., & de Vries, H. (2006). Are anti-smoking parenting practises related to adolescent smoking cognitions and behaviour? Health Education Research, 21, 66–77. http://doi.org/10.1093/her/cyh045
- Huver, R. M. E., Engels, R. C. M. E., Vermulst, A. A., & de Vries, H. (2007). Is parenting style a context for smoking-specific parenting practices? Drug and Alcohol Dependence, 89, 116–125. http://doi.org/10.1016/j.drugalcdep.2006.12.005
- Jackson, C., Haw, S., & Frank, J. (2011). Adolescent and young adult health in Scotland. Edinburgh. Retrieved from http://www.scphrp.ac.uk/adolescent-and-young-adult-health-in-scotland/
- Jernigan, D. (n.d.). A global perspective on drinking ages and alcohol use. Hanover. Retrieved from http://www.dartmouth.edu/~dcare/pdfs/Jernigan.pdf
- Kam, J. A. (2011). Identifying changes in youth’s subgroup membership over time based on their targeted communication about substance use with parents and friends. Human Communication Research, 37, 324–349. http://doi.org/10.1111/j.1468-2958.2011.01408.x
- Kam, J. A. & Middleton, A. V. (2013). The associations between parents’ references to their own past substance use and youth's substance-use beliefs and behaviours: A comparison of Latino and European American youth. Human Communication Research, 39, 208–229. http://doi.org/10.1111/hcre.12001
- Kingon, Y. & O’sullivan, A. (2001). The family as a protective asset in adolescent development. Journal of Holistic Nursing, 19, 102–121. http://doi.org/10.1177/089801010101900202
- Koning, I. M., van den Eijnden, R. J., Glatz, T., & Vollebergh, W. A. (2013). Don’t worry! Parental worries, alcohol-specific parenting and adolescents' drinking. Cognitive Therapy and Research, 37, 1079–1088. http://doi.org/10.1007/s10608-013-9545-0
- Koning, I. M., Van den Eijnden, R. J. J. M., & Vollebergh, W. A. M. (2014). Alcohol-specific parenting, adolescents' self-control, and alcohol use: a moderated mediation model. Journal of Studies on Alcohol and Drugs, 75, 16–23. http://dx.doi.org/10.15288/jsad.2014.75.16
- Kulbok, P. A., Bovbjerg, V., Meszaros, P. S., Botchwey, N., Hinton, I., Anderson, N. L. R. … Hartman, K. (2010). Mother-daughter communication. A protective factor for nonsmoking among rural adolescents. Journal of Addictions Nursing, 21, 69–78. http://doi.org/10.3109/10884601003777604
- Levy, S. A., Westin, A. M. L., Reamy, A. M., Reyner, J. C., Syed, T., & Diamond, G. S. (2010). Communication about smoking between depressed adolescents and their parents. Nicotine & Tobacco Research, 12, 191–197. http://doi.org/10.1093/ntr/ntp192
- Lezin, N., Rolleri, L.A., Bean, S., & Taylor, J. (2004). Parent-child connectedness: Implications for research, interventions, and positive impacts on adolescent health. Santa Cruz, CA. Retrieved from http://recapp.etr.org/recapp/documents/research/litreview.pdf
- Luk, J. W., Farhat, T., Iannotti, R. J., & Simons-Morton, B. G. (2010). Parent-child communication and substance use among adolescents: Do father and mother communication play a different role for sons and daughters? Addictive Behaviours, 35, 426–431. http://doi.org/10.1016/j.addbeh.2009.12.009
- Maggi, S., Lovato, C. Y., Hill, E. M., Johnson, J. L., Ratner, P. A., & Shoveller, J. A. (2014). Adolescents’ perceptions of parental influences on their smoking behaviour: A content analysis. Youth & Society, 46, 132–149. http://doi.org/10.1177/0044118X11434414
- Mallick, J. (2003). Let’s talk drugs: The need for effective parent-child communication within drug education. International Journal of Adolescence and Youth, 11, 41–58. http://doi.org/10.1080/02673843.2003.9747916
- Mares, S. H. W., Lichtwarck-Aschoff, A., & Engels, R. C. M. E. (2013). Alcohol-specific parenting, adolescent alcohol use and the mediating effect of adolescent alcohol-related cognitions. Psychology & Health, 28, 833–848. http://doi.org/10.1080/08870446.2012.762453
- Mares, S. H. W., van der Vorst, H., Engels, R. C. M. E., & Lichtwarck-Aschoff, A. (2011). Parental alcohol use, alcohol-related problems, and alcohol-specific attitudes, alcohol-specific communication, and adolescent excessive alcohol use and alcohol-related problems: An indirect path model. Addictive Behaviours, 36, 209–216. http://doi.org/10.1016/j.addbeh.2010.10.013
- Markham, C. M., Lormand, D., Gloppen, K. M., Peskin, M. F., Flores, B., Low, B., & House, L. D. (2010). Connectedness as a predictor of sexual and reproductive health outcomes for youth. Journal of Adolescent Health, 46, S23–S41. http://doi.org/10.1016/j.jadohealth.2009.11.214
- Metzger, A., Wakschlag, L. S., Anderson, R., Darfler, A., Price, J., Flores, Z., & Mermelstein, R. (2013). Information management strategies within conversations about cigarette smoking: parenting correlates and longitudinal associations with teen smoking. Developmental Psychology, 49, 1565–1578. http://doi.org/10.1037/a0030720.Information
- Miller-Day, M. & Dodd, A. H. (2004). Toward a descriptive model of parent–offspring communication about alcohol and other drugs. Journal of Social and Personal Relationships, 21, 69–91. http://doi.org/10.1177/0265407504039846
- Mirza, K. A. H. & Mirza, S. (2008). Adolescent substance misuse. Psychiatry, 7, 357–362. http://doi.org/http://dx.doi.org/10.1016/j.mppsy.2008.05.011
- Newman, K., Harrison, L., Dashiff, C., & Davies, S. (2008). Relationships between parenting styles and risk behaviours in adolescent health: An integrative literature review. Revista Latino-Americana De Enfermagem, 16, 142–150. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/18392544
- Nonnemaker, J. M., Silber-Ashley, O., Farrelly, M. C., & Dench, D. (2012). Parent-child communication and marijuana initiation: Evidence using discrete-time survival analysis. Addictive Behaviours, 37, 1342–1348. http://doi.org/10.1016/j.addbeh.2012.07.006
- Otten, R., van der Zwaluw, C. S., van der Vorst, H., & Engels, R. C. (2008). Partner effects and bidirectional parent-child effects in family alcohol use. European Addiction Research, 14, 106–112. http://doi.org/10.1159/000XXXXXX
- Razzino, B. E., Ribordy, S. C., Grant, K., Ferrari, J. R., Bowden, B. S., & Zeisz, J. (2004). Gender-related processes and drug use: Self-expression with parents, peer group selection, and achievement motivation. Adolescence, 39, 167–177
- Reimuller, A., Hussong, A., & Ennett, S. T. (2013). The influence of alcohol-specific communication on adolescent alcohol use and alcohol-related consequences. Prevention Science, 12, 389–400. http://doi.org/10.1007/s11121-011-0227-4
- Resnick, M. D., Bearman, P. S., Blum, R. W., Bauman, K. E., Harris, K. M., Jones, J. … Udry, J. R. (1997). Protecting adolescents from harm: findings from the National Longitudinal Study on Adolescent Health. Journal of the American Medical Association, 278, 823–832. http://doi.org/10.1001/1997.03550100049038
- Ringlever, L., Otten, R., de Leeuw, R. N. H., & Engels, R. C. M. E. (2011). Effects of parents’ education and occupation on adolescent smoking and the mediating role of smoking-specific parenting and parent smoking. European Addiction Research, 17, 55–63. http://doi.org/10.1159/000321258
- Ryan, S. M., Jorm, A. F., Kelly, C. M., Hart, L. M., Morgan, A. J., & Lubman, D. I. (2011). Parenting strategies for reducing adolescent alcohol use: A Delphi consensus study. BMC Public Health, 11, 13. http://doi.org/10.1186/1471-2458-11-13
- Ryan, S. M., Jorm, A. F., & Lubman, D. I. (2010). Parenting factors associated with reduced adolescent alcohol use: A systematic review of longitudinal studies. The Australian and New Zealand Journal of Psychiatry, 44, 774–783. http://doi.org/10.1080/00048674.2010.501759
- Scottish Government. (2008). Early years and early intervention: A joint Scottish Government and COSLA policy statement. Edinburgh. Retrieved from http://www.scotland.gov.uk/Resource/Doc/215889/0057733.pdf
- Sherriff, N., Cox, L., Coleman, L., & Roker, D. (2008). Communication and supervision of alcohol in the family: Parental perspectives. Children & Society, 22, 370–382. http://doi.org/10.1111/j.1099-0860.2007.00116.x
- Spijkerman, R., van den Eijnden, R. J. J. M., & Huiberts, A. (2008). Socioeconomic differences in alcohol-specific parenting practises and adolescents’ drinking patterns. European Addiction Research, 14, 26–37. http://doi.org/10.1159/000110408
- Thomas, R.E., Baker, P., Thomas, B., & Lorenzetti, D. (2015). Family-based programmes for preventing smoking by children and adolescents. Retrieved from http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD004493.pub3/epdf
- Tilson, E. C., McBride, C. M., Lipkus, I. M., & Catalano, R. F. (2004). Testing the interaction between parent-child relationship factors and parent smoking to predict youth smoking. Journal of Adolescent Health, 35, 182–189. http://doi.org/10.1016/j.jadohealth.2003.09.014
- Torabi, M. R., Bailey, W. J., & Majd-Jabbari, M. (1993). Cigarette smoking as a predictor of alcohol and other drug use by children and adolescents: Evidence of the “gateway drug effect”. The Journal of School Health, 63, 302–306. http://doi.org/10.1111/j.1746-1561.1993.tb06150.x
- Townsend, K. C. & McWhirter, B. T. (2005). Connectedness: A review of the literature with implications for counselling, assessment, and research. Journal of Counselling & Development, 83, 191–201. http://doi.org/10.1002/j.1556-6678.2005.tb00596.x
- van den Eijnden, R., van de Mheen, D., Vet, R., & Vermulst, A. D. (2011). Alcohol-specific parenting and adolescents’ alcohol-related problems: The interacting role of alcohol availability at home and parental rules. Journal of Studies on Alcohol and Drugs, 72, 408–417. http://doi.org/http://dx.doi.org/10.15288/jsad.2011.72.408
- van der Vorst, H., Burk, W. J., & Engels, R. C. M. E. (2010). The role of parental alcohol-specific communication in early adolescents' alcohol use. Drug and Alcohol Dependence, 111, 183–190. http://doi.org/10.1016/j.drugalcdep.2010.03.023
- van der Vorst, H., Engels, R. C. M. E., Meeus, W., Deković, M., & Van Leeuwe, J. (2005). The role of alcohol-specific socialisation in adolescents’ drinking behaviour. Addiction, 100, 1464–1476. http://doi.org/10.1111/j.1360-0443.2005.01193.x
- Velleman, R. (2009). Influences on how children and young people learn about and behave towards alcohol: a review of the literature for the Joseph Rowntree Foundation (part one). York. Retrieved from http://www.jrf.org.uk/sites/files/jrf/children-alcohol-use-partone.pdf
- Velleman, R. D. B., Templeton, L. J., & Copello, A. G. (2005). The role of the family in preventing and intervening with substance use and misuse: A comprehensive review of family interventions, with a focus on young people. Drug and Alcohol Review, 24, 93–109. http://doi.org/10.1080/09595230500167478
- Velleman, R. & Templeton, L. (2007). Understanding and modifying the impact of parents’ substance misuse on children. Advances in Psychiatric Treatment, 13, 79–89. http://doi.org/10.1192/apt.bp.106.002386
- Whittemore, R. & Knafl, K. (2005). The integrative review: Updated methodology. Journal of Advanced Nursing, 52, 546–553. http://doi.org/10.1111/j.1365-2648.2005.03621.x
- World Health Organisation. (2015). Adolescent health. Retrieved June 18, 2015 from http://www.who.int/topics/adolescent_health/en/