
Abstract
Environmental drug prevention interventions are gaining momentum alongside and in concert with ‘classical’ prevention practices such as school, family and community interventions. The Icelandic Prevention Model (IPM) is particularly gaining attention because of its innovative environmental approach and because of its supposed impact on lowering (the onset of) substance use among youth during the past two decades in Iceland. Although this model is rooted in well accepted prevention principles and has been prominent in public discussions and the media across the world, much remains unknown about the active ingredients, the core elements and their contribution to lowering (the onset of) substance use among youth. In this discussion paper we highlight the model’s strengths (bottom-up approach, local assessment and dissemination, multi-component, targeting risk and protective factors, supervised leisure activities, curfew hours) and raise some critical concerns (transferability, external and internal validity) that should be considered and dealt with before implementing, adapting and evaluating the model in other contexts.
Introduction
The Icelandic Prevention Model (IPM) (Kristjansson, Mann, et al., Citation2020) appeals to prevention workers and policy makers because of its encompassing environmental approach to prevent alcohol and other substance use among young people, with its developers claiming for an impressive effect on the reduction of adolescent substance use since the 90’s (Sigfúsdóttir et al., Citation2009). IPM is gaining visibility on media worldwide (Young, Citation2017) and the scientific community outside Iceland (Santacroce, Citation2018).
Considering this hype across the world, the authors are concerned about the broad (commercial) dissemination of the Icelandic Prevention Model while adequate scientific evidence concerning the implemented measures worldwide is still scarce. We share the interest in this model because of its supposed relation to the dramatic decline of substance use among Icelandic youth (Kristjansson et al., Citation2010, Citation2016) and because of the pioneer work in consistently and consequently implementing five environmental prevention principles (targeting the social environment, community action, engaging and empowering, bottom-up team work, using community resources) (Kristjansson, Mann, et al., Citation2020).
In the transference of interventions, it is imperative that both the intervention model and its evaluation design deserves critical inspection of intervention mechanisms and contextual interactions to inform decisions on the need and the extent of adaptation that might be warranted (Movsisyan et al., Citation2019) before implementing it in other countries. In the context of the increased need of evidence-based prevention, it is paramount to critically assess environmental models before implementation and to evaluate before dissemination (Burkhart, Citation2011). For the intervention to be a success, as well as for the efficient use of public funds and adherence to ethical considerations, it is necessary to have a good insight in both the current intervention components as well as evaluation of strengths and shortcomings (Movsisyan et al., Citation2019), including the capacity of transferability of the model from a country or setting to another one (Schloemer & Schröder-Bäck, Citation2018).
The aim of this paper is to critically review and discuss the strengths (bottom-up approach, local assessment and dissemination, targeting risk and protective factors, multi-component, supervised leisure activities, curfew hours) of the Icelandic Prevention Model along with the challenges (transferability, external and internal validity) that need to be taken into account when planning its implementation in countries other than Iceland. This paper is a more elaborated and scientific version of the EUSPR position paper published in the beginning of 2020 (EUSPR, Citation2020).
The Icelandic Prevention Model (IPM) and its strengths
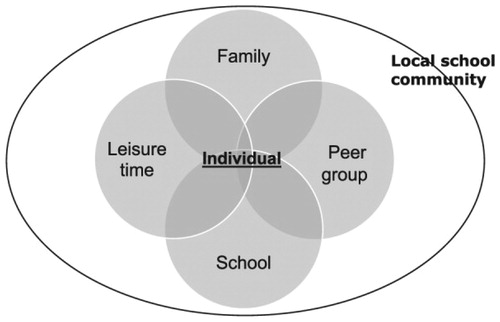
The IPM is rooted in a ‘society is the patient’ approach (Myers, 2009 in Kristjansson, Mann, et al., Citation2020). That is to say, Kristjansson, Mann, et al. (Citation2020, p. 63) outline that the IPM targets children as social products rather than rational individual actors. As presented in , the theoretical model of IPM aims to strengthen protective factors and reduce risk factors at the local community level within four environments: family, peer group, school, and leisure outside school (Kristjansson, Mann, et al., Citation2020).
Figure 1. Domains of community risk and protective factors in the icelandic prevention model (copied from Kristjansson, Mann, et al., Citation2020).
The five guiding principles of the IPM are presented in . Additionally, parental monitoring, organised leisure time activities and strengthening normative pressure play a central role besides the IPM’s environmental and process orientation, in reducing and delaying the onset of use of alcohol and other substances among young people (see: https://planetyouth.org/). Briefly and in terms of behavioural change components, the IPM employs leisure time vouchers (which enables young people to spent their free time after school in meaningful sports or culture activities), and engages with parents, so that they (a) increase their monitoring about the whereabouts and peer contacts of their offspring and (b) spend more time together with them, e.g. at family dinners; and these components of the IPM are embedded in (a) a strong alcohol policy and (b) curfew hours regulations for youth, at national level. The model’s five overlapping guiding principles are derived from scientific knowledge that these components indeed may have contributed to the decline of (the onset of) alcohol use among youth as described by Sigfusdottir et al. (2009, Citation2011) and Kristjannson et al. (Citation2016), Kristjannson, Mann, et al. (Citation2020) during the past decades.
Table 1. Five guiding principles of IPM (Kristjansson, Mann, et al., Citation2020, pp. 65–66).
Strengths of the IPM
Three strengths that we elaborate on below are linked to at least one of the guiding principles, and part of the ‘steps’ as described by Kristjansson, Mann, et al. (Citation2020), yet we have identified an additional three characteristics that are key in the IPM.
First, the IPM involves parents, youth, policymakers and researchers, as suggested in the Guiding Principle 4 (). A bottom-up approach to intervention development and implementation has indeed demonstrated to be more effective in terms of matching community needs and better resource management (Larrison, Citation2000) than a top-down approach where the intervention is instructed by others (McKenzie, Citation2017). The involvement of all stakeholders can induce more public support, especially for environmental measures that are often unpopular. This strategy also includes the theoretical structure of systemic public health interventions, since it offers space for the articulation of different agents in different instances, increasing the likelihood of positive results (Midgley, Citation2006). Moreover, it allows for better matching the needs of the target groups to the intervention (Guiding principle 5), higher quality of implementation and long-lasting interiorizing of behaviours among youth. Intervention strategies that prioritize youth engagement overcome potential obstacles perceived by youth to participate and thereby increase the relevance of and the participation of youth in the intervention (Sawyer et al., Citation2012). Once engaged, youth involved in interventions show a decrease in substance use (McConnell et al., Citation2014). Thus, by including stakeholders in intervention development and implementation, the chances for the intervention to be effective are enlarged.
Second, the use of recent and local data on alcohol consumption, leisure time and the role of parents of youth are the foundation of the IPM (Guiding principle 3). Based on these data, local prevention workers and policy makers better understand the main risk and protective factors that influence substance use in a particular area. The intervention components of the model are subsequently selected and implemented after the analysis of these data. It is fairly rare that intervention strategies are implemented based on and shortly after local scientific data collection. As demonstrated in other prevention strategies (i.e. Communities That Care; EMCDDA, Citation2017; Hawkins et al., Citation2002) it is a knowledge-based way to match interventions to the needs in specific contexts and populations. Interventions matching the needs of the target group are more likely to be effective in changing the desired outcome (Fagan et al., Citation2011) as acceptability of the intervention, contextual tailoring and readiness to change is greater. Collecting regular epidemiological data is both key source of information on substance use trends and patterns (Kraus et al., Citation2004) but, mainly, it can answer about the impact of each of the potential predictors on the behavioural outcome (Griffin & Botvin, Citation2010).
Third, parents, youth and policy are targeted in different components of the IPM, and as such, the model tends to address multiple protective and risk factors at different levels. This encompassing environmental approach is still rare in Europe when it comes to curbing substance use among young people (Imm et al., Citation2018; NJI database, Citation2020; Xchange database, Citation2020). Research demonstrates that multi-component interventions are indeed more effective than single-component interventions (Foxcroft & Tsertsvadze, Citation2011; Koning et al., Citation2009, Citation2011; Smit et al., Citation2008). Additionally, the combination of local prevention efforts framed within a strong national alcohol policy that already restricts the accessibility to alcohol and exposure to alcohol marketing (as is the case in Iceland) are related to lower drinking rates among youth in a number of studies (Holder, Citation2000; Paschall et al., Citation2009). Prevention efforts that deliver interventions in multiple settings, for example, in school, family and community settings, are more effective than targeting either of these settings.
Fourth, the targeted factors of the Icelandic Prevention Model (i.e. parental monitoring and decreased opportunities to engage in risk behaviours) are documented to play a protective key role in the pathways that lead to the use of substances (Foxcroft & Tsertsvadze, Citation2011; Hawkins et al., Citation1992; Kiesner et al., Citation2010; Rusby et al., Citation2018; Ryan et al., Citation2010; Valente et al., Citation2019; Van Ryzin et al., Citation2016). Moreover, targeting these factors within a broader context of discouraging early alcohol use (as outline above) is even more effective (e.g. Ryan et al., Citation2010; Van Ryzin et al., Citation2016). Particularly parental monitoring (i.e. parents knowing where and with whom their offspring spends free time) is a well-known effective prevention component (Van Ryzin et al., Citation2016). In line with this, most (Coley et al., Citation2008; Eisenberg et al., Citation2008), yet not all (e.g. Hofman & Warnick, Citation2013) studies demonstrate that for instance family dinners are a protective against antisocial behaviour in general. Moreover, media strategies that target parents only in order to promote parental monitoring and family dinners belong to the relatively few evidence-based forms of using media in prevention (Crano et al., Citation2017; Lac & Crano, Citation2009; Metzler et al., Citation2012). Thus, targeting evidence-based risk factors in the prevention of substance use may have contributed to the lower drinking rates among Icelandic youth.
Fifth, although it is not entrenched in its guiding principles (Kristjansson, Mann, et al., Citation2020), the IPM aims at creating the opportunity for supervised leisure activities to youth. Though this may seem obvious, it is not commonly used as an explicit component of prevention interventions. The opportunity for youth to engage in prosocial behaviour, that is most likely to occur in supervised activities, is a protective factor that is likely to be associated with lower alcohol and other substance use in adolescents (Imm et al., Citation2018). On the other hand, involvement in unstructured activities like hanging out and meeting friends after 8 pm and activities that are adult-unsupervised and take place in public, often lack skill-building aims and are less aimed at community building (Weerman et al., Citation2015; Weybright et al., 2016). Unsupervised activities subsequently offer more opportunity to engage in risk behaviours such as alcohol and other substance use (e.g. Weybright et al., Citation2016). Longitudinal research shows that the availability of positive, well supervised and meaningful leisure activities are protective against particularly early alcohol and cannabis use among young people (e.g. Badura et al., Citation2018; Khoddam et al., Citation2018; Weybright et al., Citation2014, Citation2016). However, the participation in (particularly team) sports, by itself (Wichstrom & Wichstrom, Citation2009) can in fact, increase alcohol consumption (Kwan et al., Citation2014) and heavy episodic drinking (Bedendo et al., Citation2013). Strategies that offer alcohol-free programming at for instance colleges seems to be an effective way to lower the alcohol consumption among youth (Layland et al., Citation2019). Thus, encouraging youth to engage in supervised, alcohol-free leisure activities is a promising avenue.
Sixth, the IPM is implemented in the context of national curfew hours. Curfew hours ‘establish a time when children and young people below certain ages must be home’ (Holder, Citation2004). Although these curfew hours are not identified as a guiding principle of the model (Kristjansson, Mann, et al., Citation2020), it reduces the exposure of young people to the environments, situations and crowds that become exponentially more risky the more the night progresses (Brown et al., Citation2008). Among youth, being under adult supervision after a certain hour in the evening is likely to lower the risk of finding oneself in a context where drinking alcohol is normalised/available. Nevertheless, the model developers stress that the intervention goals are set by the local collaboration of partners and do not necessarily include curfew hours as a prerequisite of the model (Kristjansson, Mann, et al., Citation2020).
Although the six identified strengths are evidence based, it remains empirically unclear what the core components of the IPM are. Additionally, the guiding principles of Kristjansson, Mann, et al. (Citation2020) do not include specific intervention components nor do the fact sheets of documents presented on the program website previously mentioned.
The challenges of the Icelandic prevention model
Despite the potentialities observed in the IPM model, some theoretical and practical gaps were identified. Below are listed three axes of challenges that need to be considered when discussing the model's dissemination in alternative scenarios, out of Iceland.
The compelling nature of environmental prevention
The IPM and its increased popularity in the international lay press has rightfully pointed out the importance of two main principles of environmental prevention:
Prevention should not only address individual decision making or skills, but also the automatic, collective and non-conscious determinants of human behaviour, such as incentives, opportunities and social norms (i.e. key characteristics of environmental prevention; Perman-Howe et al., Citation2018).
Crucial prevention interventions are embedded in local strategies at municipal/county level (i.e. managing opportunities and incentives for everyone’s behaviour) preparing the ground for additional developmental (i.e. skills training) programmes targeting individuals, schools or families.
Interventions targeting the environment at a local level tend to focus on modifying the community, that is a set of persons that share the social, cultural, political, and economic processes they’re part of (Holder, Citation2002). For alcohol use, this is mostly done by (1) restricting or reducing the availability of alcohol, (2) mobilizing community citizens, leaders, and institutions, (3) focusing primarily on changing the community environment and (4) implementing multiple components (also e.g. skills-based strategies) (Jansen et al., Citation2016; Perman-Howe et al., Citation2018; Stockings et al., Citation2018; Toomey & Wagenaar, Citation2002). In recent years, the concept has been further developed by proposing that automatic processes, instead of individual responsibility for decision-making and self-control, are key in environmental prevention (EMCDDA, Citation2018). This implies that the environment should be altered as such and that the exposure to risk behaviour opportunities should be lowered or availability of healthy opportunities should be promoted through regulatory, physical and economic measures (see EMCDDA, Citation2018).
The environmental approach has increasingly been applied in the domain of alcohol use, yet not always in the strict environmental approach and probably therefore has mixed results (e.g. Hallgren & Andreasson, Citation2013; Stockings et al., Citation2018). For example, the community-based alcohol intervention as described by Hallgren and Andreasson (Citation2013) demonstrated not effectiveness due to the selection of non-effective intervention strategies by the community (school and parent based strategies). It remains a challenge to combine environmental strategies with those targeting skills and competences at the individual level (developmental approaches), while this seems to be the most promising way forward. Furthermore, it is even a greater challenge to unpack the complex interplay between (interaction[s] of) environmental factors and individual factors influencing alcohol use (i.e., the mediating factors). Currently, there is an urgent need for studies that identify the causal pathways and mechanisms through which environmental strategies exert an effect on individual alcohol use (Shadish et al., Citation2002). This information is a prerequisite to judge the generalisability of evidence (Watts et al., Citation2011) and subsequent transferability of interventions. Clear descriptions of the implemented environmental and individual strategies as well as the intervention context is warranted, yet up to recently (2020 papers of Kristjannson, Mann, et al., 2020) not available for the IPM.
Environmental strategies focus on reducing the visibility and accessibility of alcohol or other substances and aim at changing the perception of normality and acceptance (descriptive and injunctive community norms). The IPM’s five guiding principles (Kristjannson, Mann, et al., 2020) and the ten core steps of implementation (Kristjannson, Mann, et al., 2020) in combination with the IPM’s presumably active ingredients (e.g. lower accessibility to substances, parental monitoring and participation in organized sports; Kristjansson et al., Citation2010) indeed reflect an environmental prevention perspective. Contrarily, developmental approaches aim to develop skills and cognitions in individuals or groups. Environmental interventions in turn aim to modify the context where the behaviour takes place by limiting exposure and opportunity of risky and promoting the availability of healthy behaviours (EMCDDA, Citation2018).
In short, the behavioural change induced by environmental prevention strategies should intend to change affordances and choice architecture by modifying physical, economic and regulatory conditions, with the rationale that social context (norms, beliefs, values, interactions) follows (is secondary to) the changes in economic, physical or regulatory context, in additional to developmental prevention strategies. This environmental approach offers a great opportunity to advance evaluated developmental interventions by supplementing them with environmental measures (EMCDDA, Citation2018). However, it is imperative to invest in rigorous evaluation strategies before promoting the implementation of environmental strategies. We apply this imperative to the example of the IPM below. In line with this rationale, the EMCDDA’s Xchange registry boardFootnote1 recommended additional evaluation studiesFootnote2 before implementing the model in the European context.
The context: a challenge to transferability and external validity
Alcohol policy
In line with the principles of environmental prevention (EMCDDA, Citation2018; Perman-Howe et al., Citation2018), the implementation of the most important components of the IPM (curfew hours and supervised leisure time offers, which have a substantial cost), embedded in a strong national alcohol policy, depend upon changing laws or delegating regulation of power and resources to local authorities. To develop a strong alcohol policy (for example, banning alcohol advertising) together with curfew hours requires significant legislative action, which–even at local level–can take several years in most countries and can hardly be influenced by the intervention developers. An important discussion is that even after a decade of the release of WHO’s Global Strategy to reduce the harmful use of alcohol, most of the countries haven’t made any move to change any of their alcohol policies (Jernigan & Trangenstein, 2020), which suggests that the introduction of IPM in countries other than Iceland may not do enough on the axis of alcohol availability control. Although model developers argue that a strong alcohol policy, as well as other components of the IPM, are not a prerequisite of the model, the marketing of the IPM to other countries or regions can be problematic if one fails to acknowledge that a crucial. possibly sufficient, and basic precondition of the IPM’s claimed success–a strong national alcohol and youth policy–can be found only in a tiny minority of the countries that have been implementing it (Burkhart, Citation2011). In terms of evaluation, local alcohol policy, a major confounder, needs to be clearly disclosed, as the generalisability of any prevention strategy can only be claimed if knowledge is available about the essential features of the context of the intervention and the inner mechanisms of the community (e.g. its traditions, cultural characteristics, power structures; Movsisyan et al., Citation2019; Pawson & Tilley, Citation1997; Watts et al., Citation2011). This information is to be acknowledged in evaluation designs to understand under what circumstances the intervention achieved its impact (Holmila & Warpenius, 2009). Yet, such additional information about the context is currently lacking in the IPM’s evaluation studies, which hinders credible generalizability of the intervention to other contexts.
Availability of resources
Insight into the availability of sufficient resources is a prerequisite for successful and sustainable implementation of any intervention in a new context (Shelton et al., Citation2018). Like many other interventions, the IPM is associated with high implementation costs. The developers charge for survey distribution and analysis (also discussed later), but this only provides insight into risk and protective factors in particular areas/countries. Additional local resources are required to take forward the findings, for example in terms of implementing leisure activities ($430.- per year for one child between 6 and 18 years), developing parenting programs etc. As discussed previously, these are potentially relevant mechanisms to target and most likely contribute to desired change in substance use among youth. Moreover, implementation of effective preventive interventions is cost-saving for health-related costs; in the US for each $invested in the implementation of an effective preventive intervention could save an estimated $18 assuming an average of $220 invested per pupil (Miller et al., Citation2008). Yet, given that only the leisure voucher of the IPM already costs twice as much as the average costs of the US preventive programs (Miller and Hendrie, Citation2008) as well as the huge reduction in funding for youth activities in many countries, it would be unethical to conduct the survey and not have adequate funds in place to address the gaps. Insight into the recourses required to implement the core elements of the IPM in other contexts is warranted, so that the resources can be ensured.
Geographical and social context
Iceland is comparable to some European countries, yet not all and certainly not in terms of geography and social context (OECD, Citation2016). The findings of the IPM should be considered in the context of Iceland as a country different in many aspects from other countries. That is, we know that the context shapes the conceptualization of the intervention by the impact on outcomes as well as how the intervention can be implemented, translated and scaled up (Craig et al., 2018). For example, people aged 15 years and above Iceland and some other countries are comparable in their life satisfaction (Iceland: 9.5, Netherlands: 9.3, Switzerland: 9.6, Denmark/Norway/Finland: >9.6), self-reported experience of good health (Iceland: 8.6, Netherlands: 8.4, Switzerland: 9.0, Ireland: 9.1) and the quality of education (Iceland: 6.9, NL: 7.4; UK: 6.8). Yet, other countries, such as Turkey and Italy differ substantially in all these aspects.
Another important difference is the population density. Previous studies have shown that the higher the population density, the greater the volume and severity of health problems requiring treatment (Rosenberg, 1982), including mental health disorders, such as depression and suicidal thoughts (Werneck & Silva, Citation2020) and drug misuse (Galea et al., Citation2005). Iceland is a country with the lowest population density in Europe and is a fairly secluded island with the lowest number of inhabitants in Europe. In Iceland, 3.3 people live p/km2, whereas for instance in the Netherlands 411 people live p/km2 and 206 people p/km2 in Italy. This affects the social relations and the subsequent perceived quality of support from the social network; which is rated lower in many other countries (Netherlands: 6.5, Estonia: 6.8, Norway: 8.2) compared to Iceland (10) (OECD, Citation2016). A good insight in the differences related to the geographical and social context are imperative for choosing the type of interventions that will be effective in a specific context. For example, increasing social control and support (by parents in particular) is a key feature of the IPM (Sigfusdottir et al., Citation2011). When this is implemented in a context in which social relations are strong, this is more feasible and accepted by the public than in a context where this is less the case at baseline.
The social and geographical differences will be larger if the program is implemented in Latin America. At this moment there is evidence at lay media of a potential dissemination of the program in Chile (Gobierno, 2019) and in Brazil (Ministério, 2019). In both situations, geography, demographics and economy differs deeply from Iceland. For instance, Brazil population is almost 600 times Iceland population, presents a territory 83 times larger and a PIB per capita 3.4 times smallerFootnote3. Chile has a population density 8 times larger than IcelandFootnote4. When considering educational disparities, it’s worth noting that while Iceland is the 25th best country on math scores among 15 y.o students, Chile is 59th and Brazil 70th, among a total of 77 countries (OECD, Citation2018).
Even beyond the aspects mentioned so far, differences in social relations have also contributed to the fact that the above-mentioned bottom-up approach is much more challenging to carry out in the same way in other countries (such as e.g. Chile, Spain or Romania), where intervention development and implementation is still mainly induced by experts and institutional actors. Moreover, the radical differences from the point of view of the economic structure and social inequality of European countries and those of Latin America, certainly limit the extrapolation of community measures (Cornia, 2011). While in Latin American countries an important portion of the population living in conditions of poverty is identified, reflected in the lack of resources to maintain their subsistence, this phenomenon is rarer in European countries (Cornia, 2011). In general, while 20% of the Brazilian population survives on less than US $5.5 a day, only 0.2% of Icelanders live this reality (World Bank, Citation2018). On the other hand, the affordability of alcohol in Brazil in much higher (Sanchez, Citation2017) than in most European countries (Rabinovich et al., Citation2009), which suggests that adolescent’s access is facilitated (Wall & Casswell, Citation2013). It is therefore very important that the content of essential intervention components and the context wherein the intervention is implemented is clearly described, imperative information that is lacking for the IPM, so that interventions can be tailored to cultural differences (Movsisyan et al., Citation2019; Resnicow et al., Citation2000). Such adaptation can increase the effectiveness of an intervention (Nierkens et al., Citation2013).
Declining prevalence of alcohol use across europe
Icelandic researchers indicate that the number of 15–16 year olds who have ever drunk alcohol has decreased from 77% in 1995 when the IPM was introduced, to 35% in 2015 (see EMCDDA & ESPAD, Citation2016). This impressive decrease must be seen in light of secular trends. During the same period, substantial reductions were observed for Ireland, Finland, Norway and Sweden and even in the UK 11–15 year olds reported ‘ever drank’ alcohol fell from 62% (1996) down to 38% (2014) (Office for National Statistics, Citation2019). Although the Icelandic trend indeed appears to be steeper, similar secular trends have been observed in other European countries (De Looze, et al, Citation2015) particularly in Northern Europe (Kraus et al., Citation2018; Pedersen & Von Soest, Citation2015). Moreover, at the European level, the steepest declines were observed for adolescents aged 11–14. In the Netherlands, the life-time prevalence of 12–14 year old youth decreased from 84% in 2003 to 43% in 2015 (De Looze et al., 2019). In addition, in 2010, prevalence rates of weekly drinking and drunkenness among 11 and 13 year olds in Iceland were comparable to several other countries such as Portugal, Germany and the Netherlands (De Witte & Mitchel, 2012). Thus, the reduction in drinking among Icelandic youth is impressive, particularly among 15–16 year olds but needs to be considered in light of a general decline of alcohol use across youth in Europe. It is also worth noting that declines in adolescent risk-taking behaviour observed across Europe during this period were not restricted to alcohol consumption, but also included significant reductions in drug use and youth crime (Chester et al., Citation2015; Farrell et al., Citation2014; Hublet et al., Citation2015; Pickett et al., Citation2013; Smit & Bijleveld, Citation2015) and appear to be correlated with e.g. a general decline in face to face peer contact in the evening (De Looze et al., Citation2019) and inclusion of parents as a target of intervention (e.g. Koning et al., Citation2009).
Different to Europe, another epidemiological scenario is found in Latin America. In Brazil, for instance, according to the 2015 National School Health Survey (PeNSE), 55.5% of Brazilian 9th grade students (14–15 years old) reported that they had tried alcohol at least once on their lifetime and the prevalence of binge drinking was 13.7% for the whole of Brazil, being higher in the urban area (14.2%) when compared to the rural area (10.3%) (Instituto Brasileiro de Geografia e Estatística, 2016). Alcohol consumption in Brazil also has decreased in the past 3 decades, but the prevalence was initially smaller than the ones found in Iceland in the same years (Carlini et al., Citation2010; Sanchez et al., Citation2015). In Chile we found a similar scenario in 2016: 39.5% of students with a mean age of 15.7 y.o (SD = 1.2) reported ever drinking an alcoholic beverage on their lifetime and 87% of them reported easy access to alcohol and no restrictions at the time of alcohol purchase (Alarcón et al., Citation2018).
Considering that the historical trend of decrease of alcohol use among adolescents in different countries can be a potential confounder of IPM effects, it’s essential to consider these scenarios when initiating the transportability of the model to Latin America or other European countries. Knowledge about the mechanisms contributing to the reduction in alcohol use is imperative to understand how the model has achieved its effects and how much of the reduction can be attributable to the IPM and not to other environmental attributes.
Challenges to internal validity: limited hard scientific evidence
The question stated on the website of the Icelandic Prevention model (Planet Youth, https://planetyouth.org) ‘How did Iceland go from being among the highest in substance use of adolescents in Europe to the lowest in 15 years?’ cannot be answered based on the available scientific evidence, which is corroborated by the evaluators when stating that they ‘were unable to establish a statistical linkage between substance use and the primary prevention variables’ (Kristjansson et al., Citation2016). Moreover, the section of their website named ‘publications’ that claims to present more than 100 peer reviewed papers from their team of scientists, does not show randomized controlled trial studies that would permit to evidence a causal association between IPM and the reduction of alcohol use among adolescents. In fact, while the IPM is currently implemented in 32 countries worldwide, there are no published papers that report on the evaluation of the IPM in any country other than Iceland. The only studies posted that direct mention IPM are mainly descriptive (e.g. Hoare et al., Citation2019) or observational and cannot be used to infer causality (Munnangi & Boktor, Citation2020).
As described previously, the decline in alcohol consumption in Iceland over the past 20 years is comparable to the decline observed in several other European countries. This is called a ‘period effect’, which indicates that it is most likely that alcohol use would have declined in Iceland over this period without any intervention. Therefore, this decrease in drinking among youth cannot with certainty be attributed to the model, as it was not factored in the evaluation design. Moreover, though the developers argue that ‘the model has proven easily transferable and can be applied in any community’ (https://planetyouth.org/, retrieved on March 26, 2020), no evidence is provided that supports this claim; neither implementation nor evaluation reports published of the implementations of the Icelandic Prevention Model in other countries are available. Moreover, papers on the effective ingredients of the intervention, a clear description of the intervention components and the relevant contextual factors are currently lacking. The currently published papers focus on the development and implementation of the model in Iceland (Halldorsson et al., Citation2014; Kristjansson, Mann, et al., Citation2020; Kristjansson, Mann, et al., Citation2020; Kristjansson & Sigfúsdóttir, Citation2009; Sigfusdottir et al., Citation2011, Citation2020). Four points of attention related to the evaluation of the model stand out.
The content of the model
A description of the content of the model itself and its targeted mechanisms are crucial to increase insight into what is being done and how the overall effects are achieved (McKenzie, Citation2017). A detailed description of the five guiding principles and the ten procedural steps of the model have only become available recently (Kristjansson, Mann, et al., Citation2020; Kristjansson, Mann, 2020), while the IPM has been widely disseminated during the past years (Kristjansson, Sigfusdottir, et al., Citation2020). Moreover, lack of insight into the effective targeted mechanisms does not allow policy makers and youth professionals to make evidence-based or informed decisions on which strategies in the IPM to pick that may work well in their environment. Curfew hours, stricter access to alcohol outlets, improved opportunities for participation in organized leisure activities, local policy change, or other interventions, may perhaps meet the goals of a local prevention collaborative yet they are not based on a hierarchy of evidence linking IPM components to improvement of outcomes. That is, none of the intervention components of the Icelandic Prevention Model are ‘unmissable elements of the model’ (Kristjansson, Sigfusdottir, et al., Citation2020). Therefore, it is insufficiently known what mechanisms are targeted in each of the intervention components and to which behavioural outcomes in youth they are expected to contribute.
Understanding the targeted mechanisms and mediation effects
As a consequence of the lack of knowledge about the content of the model, it cannot be statistically tested which elements or components contributed to which mechanisms or which components mediate the effect of the program at the outcome, leading to a potential decrease in alcohol use. There are correlational indications from cohort studies in Iceland indicating that three factors may have contributed to the decrease of monthly drinking due to the model’s influence: (1) knowledge of parents on how and with whom young people spend the afternoon and evening, (2) knowledge of parents of who the (parents of) friends of their child are, and (3) a minimum of doing a team sport 4 times a week (Kristjansson et al., Citation2010, Citation2016). This knowledge about possible pathways is promising but as the developers stress that they are not a key asset of the IPM, it remains unclear how to build it.
Evaluation design
There is only one (quasi-experimental) study available that included an experimental and a comparison condition (Kristjansson et al., Citation2010), yet it is unclear how the comparison group was composed and impacted by the IPM. In addition, the fact that five communities were excluded in the intervention group and used as comparison group (due to low implementation rates) implies fidelity and dosage issues that are not accounted for in the currently available studies and reduce internal validity of the study by introducing a large selection bias. Though testing effectiveness of environmental interventions by conducting randomized clinical trials is often not feasible, additional strong designed longitudinal experimental designs are needed to determine cause and effect of these correlations.
Three additional evaluation-related shortcomings should be considered. First, although one of the key components of the model consists of targeting established risk and protective factors at community level, the evaluations do not assess these as community-related outcomes, but instead as outcomes at the individual level. Second, Kristjansson et al. (Citation2016) describe the use of a Community Based Participatory Research (CBPR) design which includes active involvement of community members, organizational representatives, and researchers in all aspects of the research process (Israel et al., Citation1998). However, the model was initially not conceived as such and this approach does not appear to be described or evaluated in the Icelandic studies. The fact that the developers stress that the model is to be considered a process-structure rather than an intervention, should urge to systematically evaluate this process in terms of a community-based or other participatory research designs, such as conducting a process evaluation where e.g. level of involvement, acceptability and satisfaction of stakeholders are described. Third, prevention interventions are likely to yield differential effects across (vulnerable) subgroups (e.g. Spoth et al., Citation2008; Burkhart, 2011), based on risk status and demographics. Yet, none of the available studies evaluate the differential impact of the model on at-risk populations, such as youth that is particularly exposed to risk factors (i.e. high externalising behaviour, impulsiveness, parents with low parental skills or substance use etc.) (Burkhart, 2011; Verdurmen et al., Citation2014), nor are socio-economic baseline difference or attrition rates accounted for in the analysis while these could cause bias in the results (Halldorsson, Citation2014). Fourth, for published research to be used most effectively, the guidelines for accurate and transparent reporting of trial studies should be followed. The consolidated standards of reporting trials (CONSORT) statement (Moher et al., Citation2010) are among the most widely used reporting guidelines which, amongst others, include the intention-to-treat analysis (ITT). In an ITT analysis all participants are included in the analysis according to the intervention to which they were allocated, regardless of whether they received it or adhered fully to the protocol. The latter was the case for some communities in the quasi-experimental trial in Iceland; five communities that were originally elegible for the experimental condition were not included in the analysis because they participated partially in the program (Kristjansson et al., Citation2010). This is particularly relevant as this provides imperative knowledge about noncompliance that is likely to occur when the intervention is used in practice.
Altogether, we conclude that the scientific evidence to match the decline in drinking rates in Iceland to the Icelandic Prevention Model is far from conclusive. Moreover, due to a lack of insight into the content and context of the interventions, we do not really know the active ingredients (components, dosage etc.) and how they relate to potential changes in parenting strategies or participation in sports activities (as suggested by Kristjansson et al., Citation2010). This brings us to the point of our support to an open science framework and how it relates to the widespread implementation of the Icelandic Prevention Model.
The need for transparency and autonomy
One can only make use of the IPM by joining the Icelandic Monitoring Centre, which includes instruments that are different from the most commonly used national instruments, such as in the HBSC study, a well-established international study on the health and well-being of schoolchildren (http://www.hbsc.org/). Though the requirement for monitoring as such can be considered a strength, most countries have their regular data source evaluating trends of alcohol use among adolescents that are completely being disregarded. This impedes comparisons between IPM data and existing knowledge on substance use, risk and protective factors in other countries. Moreover, the use of existing monitoring tools in host sites would contribute to increasing the sustainability of the monitoring and implementation of IPM or any other intervention on the long-term.
Additionally, it has been coined (Holmila & Warpenius, 2009) that scientific objectivity is lowered if the implementers are involved in evaluation research because they are potentially opinionated stakeholders, hoping for successful results. This may result in research bias, as well as a conflict of interest. Subsequently, current proposals to address the ‘replication crisis’ in prevention studies and broader social sciences (e.g. Lösel, Citation2018; Shrout & Rodgers, Citation2018; Tackett et al., Citation2019) argue for increased transparency and openness (open materials, open data and open code) in trials, pre-registration, and review and multisite collaboration (Valentine et al., Citation2011). Nevertheless, the data collected by the centre are owned and analysed by the centre, while the existence of the centre is dependent on the reporting of favourable results. Though centralisation of data can be an advantage in terms of cross-national comparability, the way it is designed in Iceland appears not to be in line with an open science agenda, represented by a lack of transparency and an important withdrawal of the country contractor autonomy. We favor of a structure where the countries implementing IPM are allowed to own and manage the data set and then share the data with the IPM developers. More openness about the interventions, instruments and data contributes to the scientific dissemination of knowledge and constructive knowledge building.
Discussion and conclusion
The environmental approach of the IPM targets the reduction of (the onset of) alcohol and other substance use among youth by means of five guiding principles and ten procedural steps. This environmental approach is promising and innovative in the world. The lack of adequate IPM process and outcome evaluation studies and the evaluation shortcomings that we outlined are closely intertwined with a broader discussion on how to evaluate environmental interventions as well as the theoretical backdrop of intervention models, such as insight into mechanisms of change (mediation) and differential effects of interventions (moderation).
Six axes of strengths were found: bottom up approach, recent and local data driven approach, multicomponent approach, targeted factors (parental monitoring and decreased opportunity to engage in risk behaviours), supervised leisure activities, and curfew hours. In addition, three axes of challenges were described: transferability, external and internal validity. Some of the components of IPM cannot be just transferred from one country to another, since they depend on alcohol and drug policy change, which can limit results in less regulated markets. Yet, as the alcohol policy is not considered as a component of the model, the (moderating) role of alcohol or drug policy in the allegedly effectiveness of the model is not factored in. Most of the challenges turns into ethical concerns especially when the intervention becomes commercial and starts to be sold to countries of different continents, without disclosures of the its potential limitation.
Indeed, it is hard to evaluate the impact of environmental measures such as curfew hours and alcohol policy on individual behaviour. Nevertheless, and at the backdrop of well accepted behavioural change theories, the particular stance that ‘society is the patient’–taken by the IPM developers (Kristjansson, Mann, et al., Citation2020)–cannot in itself legitimise and substantiate prevention interventions. Together with considering targeted changes in the environment it is necessary to target and evaluate differentiated interventions at the individual behavioural level. Traditional evaluation methods (i.e. randomized controlled trials) do predominantly focus on individual behavioural changes and often (though not always) insufficiently consider contextual characteristics, implementation and evaluation contexts. But ideally, intervention designers and evaluators should focus both on individual (differentiated by risk) and environmental measures and interventions and develop evaluation designs that allow to understand both; i.e. combine process and outcome evaluation.
The IPM may have the potential to achieve the reduction of (the onset of) alcohol and other substance use in other countries, but only if national alcohol legislation is factored in as a major moderator and if the local contextual characteristics outlined in this paper as well as context-specific implementation data are registered and evaluated. Additionally, the active ingredients and specific interventions included in the IPM should be made explicit so that the model and its included interventions can continuously be evaluated and subsequently readapted in other contexts.
There is an urgent need for more scientific evidence on how the components of the model influence mechanisms that induce the reduction of (the onset of) substance use among youth in the long run. Only clearly defined components and knowledge about the respective implementation tools will allow to clearly identify the logic model that uncovers how each of the intervention components contributes to the desired outcomes of reducing (the onset of) substance use. While this does not happen, we suggest caution in the hype and high expectation of success when implementing the IPM in contexts other than Iceland. The choice of this model by the different government officials must be informed and must take place after all transferability limitations are explained and discussed with the developers. Any situation that does not involve a clear explanation of the points raised in this study, will be improper. Potentially, more caution should be taken in countries with low community support and large social vulnerability. In conclusion, the Iceland Prevention Model is promising and might be effective in Iceland, but when implementing it in other contexts a critical review of the above mentioned issues is warranted.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Notes
2 Interventions for which concerns about evaluation quality or consistency of outcomes in Europe make it difficult to assess if they are effective or not, even if outcomes seem to be in favour of the intervention, are rated “additional studies recommended”.
References
- Alarcón, A. M., Muñoz, N. S., & Grandjean, B. M. (2018). Consumo de alcohol en escolares de un territorio de la Araucanía-Chile: etnicidad y residencia [Alcohol consumption among high school students from the Araucanía-Chile: ethnicity and residence. Revista chilena de pediatría, 89, 0–461. https://doi.org/10.4067/S0370-41062018005000601
- Badura, P., Madarasova Geckova, A., Sigmundova, D., Sigmund, E., Van Dijk, J., & Reijneveld, S. A. (2018). Can organized leisure-time activities buffer the negative outcomes of unstructured activities for adolescents’ health? International Journal of Public Health, 63(6), 743–751. https://doi.org/10.1007/s00038-018-1125-3
- Bedendo, A., Opaleye, E. S., Andrade, A. L., & Noto, A. R. (2013). Heavy episodic drinking and soccer practice among high school students in Brazil: the contextual aspects of this relationship. BMC Public Health, 20,247. https://doi.org/10.1186/1471-2458-13-247. PMID: 23514566; PMCID: PMC3610150.
- Brown, S. A., McGue, M., Maggs, J., Schulenberg, J., Hingson, R., Swartzwelder, S., Martin, C., Chung, T., Tapert, S. F., Sher, K., Winters, K. C., Lowman, C., & Murphy, S. (2008). A developmental perspective on alcohol and youths 16 to 20 years of age. Pediatrics, 121(Supplement 4), S290–S310. https://doi.org/10.1542/peds.2007-2243D
- Burkhart, G. (2011). Environmental drug prevention in the EU. Why is it so unpopular? Adicciones, 23(2), 87–100. ISSN: 0214-4840. doi:10.20882/adicciones.151
- Carlini, E., Noto, A., & Sanchez, Z. (2010). VI Levantamento Nacional sobre o Consumo de Drogas Psicotrópicas entre Estudantes do Ensino Fundamental e Médio das Redes Pública e Privada de Ensino nas 27 Capitais Brasileiras 2010. Retrieved from https://www.cebrid.com.br/wp-content/uploads/2012/10/VI-Levantamento-Nacional-sobre-o-Consumo-de-Drogas-Psicotrópicas-entre-Estudantes-do-Ensino-Fundamental-e-Médio-das-Redes-Pública-e-Privada-de-Ensino-nas-27-Capitais-Brasileiras.pdf
- Chester, K. L., Callaghan, M., Cosma, A., Donnelly, P., Craig, W., Walsh, S., & Molcho, M. (2015). Cross-national time trends in bullying victimization in 33 countries among children aged 11, 13 and 15 from 2002 to 2010. The European Journal of Public Health, 25 (suppl. 2), 61–64. https://doi.org/10.1093/eurpub/ckv029
- Coley, R. L., Votruba-Drzal, E., & Schindler, H. S. (2008). Trajectories of parenting processes and adolescent substance use: reciprocal effects. Journal of Abnormal Child Psychology, 36(4), 613–625. https://doi-org.proxy.library.uu.nl/10.1007/s10802-007-9205-5 https://doi.org/10.1007/s10802-007-9205-5
- Cornia, G. A. 2011. Economic integration, inequality and growth: Latin America vs. the European economies in transition. DESA Working Paper No. 101 ST/ESA/2011/DWP/101. Retrieved from https://www.un.org/esa/desa/papers/2011/wp101_2011.pdf
- Craig, P., Ruggiero, D., Frohlich, E., & L, K. L. 2018. Taking account of context in population health intervention research: Guidance for producers, users and funders of research. Southampton (UK): NIHR Journals Library; 2018 Apr. Available from: https://www.ncbi.nlm.nih.gov/books/NBK498645/
- Crano, W. D., Alvaro, E. M., Tan, C. N., & Siegel, J. T. (2017). Social mediation of persuasive media in adolescent substance prevention. Psychology of Addictive Behaviors, 31(4), 479–487. https://doi.org/10.1037/adb0000265
- Looze, M. d., Raaijmakers, Q., Bogt, T. t., Bendtsen, P., Farhat, T., Ferreira, M., Godeau, E., Kuntsche, E., Molcho, M., Pfortner, T.-K., Simons-Morton, B., Vieno, A., Vollebergh, W., & Pickett, W. (2015). Decreases in adolescent weekly alcohol use in Europe and North America: Evidence from 28 countries from 2002 to 2010. The European Journal of Public Health, 25(suppl 2), 69–72. https://doi.org/10.1093/eurpub/ckv031
- De Looze, M., van Dorsselaer, S., Stevens, G. W. J. M., Boniel-Nissim, M., Vieno, A., & Van den Eijnden, R. J. J. M. (2019). The decline in adolescent substance use across Europe and North America in the early twenty-first century: A result of the digital revolution? International Journal of Public Health, 64(2), 229–240. https://doi.org/10.1007/s00038-018-1182-7(0123456789().,-volV)(0123456789().,-volV)
- De Witte P. & M.C. Jr. Mitchell (eds.). (2012). Underage drinking: A report on drinking in the second decade of life in Europe & North America. Presses Universitaires de Louvain. Retrieved from: http://books.openedition.org/pucl/3272
- Eisenberg, M. E., Neumark-Sztainer, D., Jayne, R. D., Fulkerson, A., & Story, M. (2008). Family meals and substance use: Is there a long-term protective association? The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 43(2), 151–156. https://doi.org/10.1016/j.jadohealth.2008.01.019
- EMCDDA. (2017). Communities That Care (CTC): A comprehensive prevention approach for communities. https://doi.org/10.2810/972747
- EMCDDA and ESPAD. (2016). ESPAD Report 2015—Results from the European School Survey Project on Alcohol and Other Drugs, EMCDDA–ESPAD joint publications, Publications Office of the European Union, Luxembourg. Retrieved from: https://www.emcdda.europa.eu/publications/joint-publications/emcdda-espad-report_en
- European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). (2018). Environmental substance use prevention interventions in Europe. Technical Report. http://www.emcdda.europa.eu/system/files/publications/7882/Environmental-substance-use-prevention-Interventions-in-Europe.pdf
- European Society for Prevention Research (EUSPR). (2020). The Icelandic model; is the hype justified? Retrieved from: http://euspr.org/position-paper-of-the-european-society-for-prevention-research-on-the-icelandic-model/
- Fagan, A. A., Arthur, M. W., Hanson, K., Briney, J. S., & Hawkins, J. D. (2011). Effects of Communities That Care on the Adoption and Implementation Fidelity of Evidence-Based Prevention Programs in Communities: Results from a Randomized Controlled Trial. Prevention Science: The Official Journal of the Society for Prevention Research, 12(3), 223–234. https://doi.org/10.1007/s11121-011-0226-5
- Farrell, G., Tilley, N., & Tseloni, A. (2014). Why the crime drop? Crime and Justice, 43(1), 421–490. Retrieved from: https://heinonline.org/HOL/P?h=hein.journals/cjrr43&i=426. https://doi.org/10.1086/678081
- Foxcroft, D. R., & Tsertsvadze, A. (2011). Universal school- based prevention programs for alcohol misuse in young people. Cochrane Database of Systematic Reviews, 9. https://doi.org/10.1002/14651858.CD009113
- Galea, S., Rudenstine, S., & Vlahov, D. (2005). Drug use, misuse, and the urban environment. Drug and Alcohol Review, 24(2), 127–136. https://doi.org/10.1080/09595230500102509
- Gobierno, D. C. (2019). President Piñera highlights his administration’s commitment to the fight against drugs. [INTERNET]. Retrieved June 10, 2020, from https://www.gob.cl/en/news/president-pinera-highlights-his-administrations-commitment-fight-against-drugs/
- Griffin, K. W., & Botvin, G. J. (2010). Evidence-based interventions for preventing substance use disorders in adolescents. Child and Adolescent Psychiatric Clinics of North America, 19(3), 505–526. https://doi.org/10.1016/j.chc.2010.03.005
- Halldorsson, V., Thorlindsson, T., & Sigfusdottir, I. D. (2014). Adolescent sport participation and alcohol use: The importance of sport organization and the wider social context. International Review for the Sociology of Sport, 49(3-4), 311–330. https://doi.org/10.1177/1012690213507718
- Hallgren, M., & Andreasson, S. (2013). The Swedish six-community alcohol and drug prevention trial: Effects on youth drinking. Drug and Alcohol Review, 32(5), 504–511. https://doi-org.proxy.library.uu.nl/10.1111/dar.12057. https://doi.org/10.1111/dar.12057
- Hawkins, J. D., Catalano, R. F., & Arthur, M. W. (2002). Promoting science-based prevention in communities. Addictive Behaviors, 27(6), 951–976. https://doi.org/10.1016/S0306-4603(02)00298-8
- Hawkins, J. D., Catalano, R. F., & Miller, J. Y. (1992). Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psychological Bulletin, 112(1), 64–105. https://doi.org/10.1037/0033-2909.112.1.64
- Hoare, E., Thorisdóttir, I. E., Kristjansson, A. L., Sigfusdóttir, I. D., Hayward, J., Allender, S., Strugnell, C., Reavley, N., Patton, G., Berk, M., & Jacka, F. (2019). Lessons from Iceland: Developing scalable and sustainable community approaches for the prevention of mental disorders in young Australians. Mental Health & Prevention, 15, 200166. https://doi.org/10.1016/j.mhp.2019.200166
- Hoffmann, J. P., & Warnick, E. (2013). Do family dinners reduce the risk for early adolescent substance use? A propensity score analysis. Journal of Health and Social Behavior, 54(3), 335–352. https://doi.org/10.1177/0022146513497035
- Holder, H. D. (2000). Community prevention of alcohol problems. Addictive Behaviors, 25(6), 843–859. https://doi.org/10.1016/S0306-4603(00)00121-0
- Holder, H. D. (2002). Prevention of alcohol and drug “abuse” problems at the community level: What research tells us. Substance Use & Misuse, 37(8-10), 901–921. https://doi.org/10.1081/ja-120004158
- Holder, H. D. (2004). Supply side approaches to reducing underage drinking: An assessment of the scientific evidence in reducing underage drinking: A collective responsibility, edited by Bonnie, R.J. & O’Connell, M.E. National Academies Press (US). Retrieved from: https://www.ncbi.nlm.nih.gov/books/NBK37601/
- Holmila, M., & Warpenius, K. (2009). A study on effectiveness of local alcohol policy: Challenges and solutions in the PAKKA project. Drugs: Education Prevention and Policy, 14, 529–541. https://doi.org/10.1080/09687630701392016
- Hublet, A., Bendtsen, P., de Looze, M. E., Fotiou, A., Donnelly, P., Vilhjalmsson, R., Baska, T., Aasvee, K., Franelic, I. P., Nic Gabhainn, S., & ter Bogt, T. F. M. (2015). Trends in the co-occurrence of tobacco and cannabis use in 15-year-olds from 2002 to 2010 in 28 countries of Europe and North America. The European Journal of Public Health, 25(suppl 2), 73–75. https://doi.org/10.1093/eurpub/ckv032
- Imm, P., Chinman, M., Kulesza, M., Hunter, S., & Acosta, J. (2018). Evidence-based practices: Community-based interventions to reduce alcohol use and misuse. In Leukefeld C., Gullotta T. (eds) Adolescent substance abuse. Issues in children’s and families’ lives. Springer Publications. https://doi.org/10.1007/978-3-319-90611-9_14
- Instituto Brasileiro de Geografia e Estatística. (2016). Pesquisa Nacional de Saúde do Escolar. (2015). IBGE. Retrieved from: https://biblioteca.ibge.gov.br/visualizacao/livros/liv97870.pdf
- Israel, B. A., Schulz, A. J., Parker, E. A., & Becker, A. B. (1998). Review of community-based research: assessing partnership approaches to improve public health. Annual Review of Public Health, 19, 173–202. https://doi.org/10.1146/annurev.publhealth.19.1.173
- Jansen, S. C., Haveman-Nies, A., Bos-Oude Groeniger, I., Izeboud, C., de Rover, C., & van ’t Veer, P. (2016). Effectiveness of a Dutch community-based alcohol intervention: Changes in alcohol use of adolescents after 1 and 5 years. Drug and Alcohol Dependence, 159 (1), 125–132. https://doi.org/10.1016/j.drugalcdep.2015.11.032
- Jernigan, D. H., & Trangenstein, P. J. (2020). What’s next for Who’s global strategy to reduce the harmful use of alcohol? Bulletin of the World Health Organization, 98(3), 222–223. ‐doi: 10.2471/BLT.19.24173 doi:10.2471/BLT.19.241737
- Khoddam, R., Cho, J., Jackson, N. J., & Leventhal, A. M. (2018). Diminished alternative reinforcement as a mechanism linking conduct problems and substance use in adolescence: A longitudinal examination Addiction, 113(6), 1139–1148. https://doi.org/10.1111/add.14160
- Kiesner, J., Poulin, F., & Dishion, T. J. (2010). Adolescent substance use with friends: Moderating and mediating effects of parental monitoring and peer activity contexts. Merrill Palmer Q, 56, 529–556. Retrieved from: https://www.jstor.org/stable/23097954 doi:10.1353/mpq.2010.0002
- Koning, I. M., van den Eijnden, R. J. J. M., Verdurmen, J. E. E., Engels, R. C. M. E., & Vollebergh, W. A. M. (2011). Long-term effects of a parents and student intervention on alcohol use in adolescents. American Journal of Preventive Medicine, 40, 541–547.
- Koning, I. M., Vollebergh, W. A. M., Smit, F., Verdurmen, J. E. E., van den Eijnden, R. J. J. M., ter Bogt, T. F. M., Stattin, H., & Engels, R. C. M. E. (2009). Preventing heavy alcohol use in adolescents (PAS): Cluster randomized trial of a parent and student intervention offered separately and simultaneously. Addiction, 104(10), 1669–1678. https://doi.org/10.1111/j.1360-0443.2009.02677.x
- Kraus, L., Kümmler, P., Augustin, R., Pfeiffer, T., & Simon, R. (2004). Key epidemiological indicator: Prevalence of problem drug use. EMCDDA. Retrieved from https://www.emcdda.europa.eu/system/files/publications/321/Guidelines_Prevalence_Revision_280704_b-1_124620.pdf
- Kraus, L., Seitz, N.-N., Piontek, D., Molinaro, S., Siciliano, V., Guttormsson, U., Arpa, S., Monshouwer, K., Leifman, H., Vicente, J., Griffiths, P., Clancy, L., Feijão, F., Florescu, S., Lambrecht, P., Nociar, A., Raitasalo, K., Spilka, S., Vyshinskiy, K., & Hibell, B. (2018). ‘Are the times A-changin’? Trends in adolescent substance use in Europe. Addiction, 113(7), 1317–1332. https://doi-org.proxy.library.uu.nl/10.1111/add.14201 doi:https://doi.org/10.1111/add.14201
- Kristjansson, Á. L., & Sigfúsdóttir, I. D. (2009). The role of parental support, parental monitoring, and time spent with parents in adolescent academic achievement in Iceland: A structural model of gender differences. Scandinavian Journal of Educational Research, 53(5), 481–496. https://doi.org/10.1080/00313830903180786
- Kristjansson, A. L., James, J. E., Allegrante, J. P., Sigfusdottir, I. D., & Helgason, A. R. (2010). Adolescent substance use, parental monitoring, and leisure-time activities: 12-year outcomes of primary prevention in Iceland. Preventive Medicine, 51(2), 168–171. https://doi.org/10.1016/j.ypmed.2010.05.001
- Kristjansson, A. L., Sigfusdottir, I. D., Thorlindsson, T., Mann, M. J., Sigfusson, J., & Allegrante, J. P. (2016). Population trends in smoking, alcohol use and primary prevention variables among adolescents in Iceland, 1997–2014. Addiction, 111(4), 645–652. https://doi.org/10.1111/add.13248
- Kristjansson, A. L., Mann, M. J., Sigfusson, J., Thorisdottir, I. E., Allegrante, J. P., & Sigfusdottir, I. D. (2020). Development and guiding principles of the icelandic model for preventing adolescent substance use. Health Promotion Practice, 21(1), 62–69. https://doi.org/10.1177/1524839919849032
- Kristjansson, A. L., Mann, M. J., Sigfusson, J., Thorisdottir, I. E., Allegrante, J. P., & Sigfusdottir, I. D. (2020). Implementing the icelandic model for preventing adolescent substance use. Health Promotion Practice, 21(1), 70–79. https://doi.org/10.1177/1524839919849033
- Kristjansson, A. L., Sigfusdottir, I. D., & Sigfusson, J. (2020). Response to position paper “The Icelandic model; Is the hype justified?” http://euspr.org/wp-content/uploads/2020/02/Reaction-Planet-Youth-feb-2020-euspr-icelandic-model.pdf
- Kristjansson, A. L., Sigfusdottir, I. D., & Sigfusson, J. (2020). Response to position paper “The Icelandic model; Is the hype justified?” http://euspr.org/wp-content/uploads/2020/02/Reaction-Planet-Youth-feb-2020-euspr-icelandic-model.pdf
- Kwan, M., Bobko, S., Faulkner, G., Donnelly, P., & Cairney, J. (2014). Sport participation and alcohol and illicit drug use in adolescents and young adults: A systematic review of longitudinal studies. Addictive Behaviors, 39, 497–506.
- Lac, A., & Crano, W. D. (2009). Monitoring matters: Meta-analytic review reveals the reliable linkage of parental monitoring with adolescent marijuana use. Perspectives on Psychological Science, 4(6), 578–586. https://doi.org/10.1111/j.1745-6924.2009.01166.x
- Larrison, C. (2000). A comparison of top-down and bottom-up community development interventions in Rural Mexico: Practical and theoretical implications for community development programs.
- Layland, E. K., Calhoun, B. H., Russell, M. A., & Maggs, J. L. (2019). Is alcohol and other substance use reduced when college students attend alcohol-free programs? Evidence from a measurement burst design before and after legal drinking age. Prevention Science: The Official Journal of the Society for Prevention Research, 20(3), 342–352. https://doi.org/10.1007/s11121-018-0877-6
- Lösel, F. (2018). Evidence comes by replication, but needs differentiation: The reproducibility issue in science and its relevance for criminology. Journal of Experimental Criminology, 14(3), 257–278. https://doi.org/10.1007/s11292-017-9297-z
- McConnell, M., Memetovic, J., & Richardson, C. (2014). Coping style and substance use intention and behavior patterns in a cohort of BC adolescents. Addictive Behaviors, 39(10), 1394–1397. https://doi.org/10.1016/j.addbeh.2014.05.018
- McKenzie, N. T. (2017). Planning, implementing & evaluating health promotion programs: A primer (7th ed.). Pearson. ISBN-13: 978-0134219929. ISBN-10: 0134219929.
- Metzler, C. W., Sanders, M. R., Rusby, J. C., & Crowley, R. N. (2012). Using consumer preference information to increase the reach and impact of media-based parenting interventions in a public health approach to parenting support. Behavior Therapy, 43(2), 257–270. https://doi.org/10.1016/j.beth.2011.05.004
- Midgley, G. (2006). Systemic intervention for public health. American Journal of Public Health, 96(3), 466–472. https://doi.org/10.2105/AJPH.2005.067660
- Miller, T., & Hendrie, D. (2008). Substance abuse prevention dollars and cents: A cost-benefit. (SMA) 07-4298. Center for Substance Abuse Prevention, Substance Abuse and Mental Health Services Administration.
- Ministério, D C. (2019). Programa internacional de combate às drogas será implementado no Brasil [International Program of Drug Prevention will be implemented in Brazil]. [INTERNET]. Retrived June 10, 2020, from http://mds.gov.br/area-de-imprensa/noticias/2019/setembro/programa-internacional-de-combate-as-drogas-sera-implementado-no-brasil
- Moher, D., Hopewell, S., Schulz, K. F., Montori, V., Gøtzsche, P. C., Devereaux, P. J., Elbourne, P., Egger, M., & Altman, D. G. (2010). CONSORT 2010 Explanation and Elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ, 340, c869. https://doi.org/10.1136/bmj.c869
- Movsisyan, A., Arnold, L., Evans, R., Hallingberg, B., Moore, G., O’Cathain, A., Pfadenhauer, L. M., Segrott, J., & Rehfuess, E. (2019). Adapting evidence-informed complex population health interventions for new contexts: A systematic review of guidance. Implement Sci, 14(1), 105. https://doi.org/10.1186/s13012-019-0956-5
- Munnangi, S., & Boktor, S. W. (2020). Epidemiology of study design. In StatPearls. Treasure. StatPearls Publishing. Retrieved from https://www.ncbi.nlm.nih.gov/books/NBK470342/
- Netherlands Youth Institute (NJI database). 2020. Database of effective interventions targeting alcohol, smoking and/or drugs. Retrieved from June 04, 2020. https://www.nji.nl/nl/Databank/Databank-Effectieve-Jeugdinterventies/Erkende-interventies?thema=alcohol%2C+roken+en+drugs
- Nierkens, V., Hartman, M. A., Nicolaou, M., Vissenberg, C., Beune, E. J. A. J., Hosper, K., van Valkengoed, I. G., & Stronks, K. (2013). Effectiveness of cultural adaptations of interventions aimed at smoking cessation, diet, and/or physical activity in ethnic minorities. A systematic review. PLoS One, 8(10), e73373. https://doi.org/10.1371/journal.pone.0073373
- OECD. (2016). Health at a glance: Europe 2016: State of Health in the EU Cycle. OECD Publishing. https://doi.org/10.1787/9789264265592-en
- OECD. (2018). PISA 2018 insights and interpretations. Retrieved from https://www.oecd.org/pisa/PISA%202018%20Insights%20and%20Interpretations%20FINAL%20PDF.pdf
- Office for National Statistics. (2019). Smoking, drinking and drug use among young people in England 2018 [NS]. Retrieved from https://digital.nhs.uk/data-and-information/publications/statistical/smoking-drinking-and-drug-use-among-young-people-in-england/2018#
- Paschall, M. J., Grube, J. W., & Kypri, K. (2009). Alcohol control policies and alcohol consumption by youth: A multi-national study. Addiction, 104(11), 1849–1855. https://doi-org.proxy.library.uu.nl/10.1111/j.1360-0443.2009.02698.x https://doi.org/10.1111/j.1360-0443.2009.02698.x
- Pawson, R., & Tilley, N. (1997). Realistic evaluation. Sage.
- Pedersen, W., & Von Soest, T. (2015). Adolescent alcohol use and binge drinking: An 18-year trend study of prevalence and correlates. Alcohol and Alcoholism, 50(2), 219–225. https://doi-org.proxy.library.uu.nl/10.1093/alcalc/agu091 https://doi.org/10.1093/alcalc/agu091
- Perman-Howe, P. R., Davies, E. L., & Foxcroft, D. R. (2018). The classification and organisation of alcohol misuse prevention with a focus on environmental prevention. Current Addiction Reports, 5(1), 87–92. https://doi.org/10.1007/s40429-018-0190-2
- Pickett, W., Molcho, M., Elgar, F. J., Brooks, F., de Looze, M., Rathmann, K., ter Bogt, T. F. M., Nic Gabhainn, S., Sigmundová, D., Gaspar de Matos, M., Craig, W., Walsh, S. D., Harel-Fisch, Y., & Currie, C. (2013). Trends and socioeconomic correlates of adolescent physical fighting in 30 countries. Pediatrics, 131(1), e18–e26. doi:10.1542/peds.2012-1614
- Rabinovich, L., Brutscher, P. B., De Vries, H., Tiessen, J., Clift, J., & Reding, A. (2009). The affordability of alcoholic beverages in the European Union: Understanding the link between alcohol affordability, consumption and harms. RAND Corporation. https://www.rand.org/pubs/technical_reports/TR689.html
- Resnicow, K., Soler, R., Braithwaite, R. L., Ahluwalia, J. S., & Butler, J. (2000). Cultural sensitivity in substance use prevention. Journal of Community Psychology, 28(3), 271–290. https://doi-org.proxy.library.uu.nl/10.1002/(SICI)1520-6629.
- Rosenberg, G. (1982). High population densities in relation to social behavior. Ekistics, 49(296), 12312469.
- Rusby, J. C., Light, J. M., Crowley, R., & Westling, E. (2018). Influence of parent-youth relationship, parental monitoring, and parent substance use on adolescent substance use onset. Journal of Family Psychology, 32(3), 310–320. https://doi.org/10.1037/fam0000350
- Ryan, S. M., Jorm, A. F., & Lubman, D. I. (2010). Parenting factors associated with reduced adolescent alcohol use: A systematic review of longitudinal studies. The Australian and New Zealand Journal of Psychiatry, 44(9), 774–783. https://doi-org.proxy.library.uu.nl/10.1080/00048674.2010.501759 https://doi.org/10.1080/00048674.2010.501759
- Sanchez, Z. M., Prado, M. C. O., Sanudo, A., Carlini, E. A., Nappo, S. A., & Martins, S. S. (2015). Trends in alcohol and tobacco use among Brazilian students: 1989 to 2010. Revista de Saúde Pública, 49(0), 1–79. https://doi.org/10.1590/S0034-8910.2015049005860
- Sanchez, Z. M. (2017). Binge drinking among young Brazilians and the promotion of alcoholic beverages: A public health concern. Epidemiologia e servicos de saude: revista do Sistema Unico de Saude do Brasil, 26(1), 195–198. https://doi.org/10.5123/S1679-49742017000100020
- Santacroce, R. (2018). Il modello islandese di prevenzione per le condotte a rischio in adolescenza: un intervento da imitare? [The Icelandic Model for Preventing risky behaviours among adolescents: Shall we think about this project?]. Epidemiol Prev, 42, 198–199. https://doi.org/10.19191/EP18.3-4.P198.060
- Sawyer, S. M., Afifi, R. A., Bearinger, L. H., Blakemore, S.-J., Dick, B., Ezeh, A. C., & Patton, G. C. (2012). Adolescence: A foundation for future health. Lancet, 379(9826), 1630–1640. https://doi.org/10.1016/S0140-6736(12)60072-5 https://doi.org/10.1016/S0140-6736(12)60072-5
- Schloemer, T., & Schröder-Bäck, P. (2018). Criteria for evaluating transferability of health interventions: A systematic review and thematic synthesis. Implementation Science, 13(1), 88. https://doi.org/10.1186/s13012-018-0751-8
- Shadish, W. R., Cook, T. D., & Campbell, D. T. (2002). Experimental and quasi-experimental designs for generalized causal inference. Mifflin and Company.
- Shelton, R. C., Cooper, B. R., & Stirman, S. W. (2018). The sustainability of evidence-based interventions and practices in public health and health care. Annual Review of Public Health, 39, 55–76. https://doi.org/10.1146/annurev-publhealth-040617-014731
- Shrout, P. E., & Rodgers, J. L. (2018). Psychology, science, and knowledge construction: Broadening perspectives from the replication crisis. Annual Review of Psychology, 69, 487–510. https://doi-org.proxy.library.uu.nl/10.1146/annurev-psych-122216-011845 https://doi.org/10.1146/annurev-psych-122216-011845
- Sigfusdottir, I. D., Kristjansson, A. L., Gudmundsdottir, M. L., & Allegrante, J. P. (2011). Substance use prevention through school and community-based health promotion: A transdisciplinary approach from Iceland. Global Health Promotion, 18(3), 23–26. https://doi.org/10.1177/1757975911412403
- Sigfusdottir, I. D., Soriano, H. E., Mann, M. J., & Kristjansson, A. L. (2020). Prevention is possible: A brief history of the origin and dissemination of the icelandic prevention model. Health Promotion Practice, 21(1), 58–61. https://doi.org/10.1177/1524839919886314
- Sigfúsdóttir, I. D., Thorlindsson, T., Kristjánsson, A. L., Roe, K. M., & Allegrante, J. P. (2009). Substance use prevention for adolescents: The Icelandic Model. Health Promotion International, 24(1), 16–25. https://doi-org.proxy.library.uu.nl/10.1093/heapro/dan038 https://doi.org/10.1093/heapro/dan038
- Smit, P. R., & Bijleveld, C. C. (2015). Juvenile delinquency and juvenile justice trends in Europe. In M.D. Krohn & J. Lane (Eds.) The handbook of juvenile delinquency and juvenile justice (pp. 15–26). John Wiley and Sons.
- Smit, E., Verdurmen, J., Monshouwer, K., & Smit, F. (2008). Family interventions and their effect on adolescent alcohol use in general populations; a meta-analysis of randomized controlled trials. Drug & Alcohol Dependence, 97:195–206.
- Spoth, R. L., Randall, G. L., Trudeau, L., Shin, C., & Redmond, C. (2008). Substance use outcomes 5½ years past baseline for partnership-based, family-school preventive interventions. Drug and Alcohol Dependence, 96(1–2), 57–68. https://doi.org/10.1016/j.drugalcdep.2008.01.023
- Stockings, E., Shakeshaft, A., & Farrell, M. (2018). Community approaches for reducing alcohol-related harms: An overview of intervention strategies, efficacy, and considerations for future research. Current Addiction Reports, 5(2), 274–286. https://doi-org.proxy.library.uu.nl/10.1007/s40429-018-0210-2. https://doi.org/10.1007/s40429-018-0210-2
- Tackett, J. L., Brandes, C. M., King, K. M., & Markon, K. E. (2019). Psychology’s replication crisis and clinical psychological science. Annual Review of Clinical Psychology, 15, 579–604. https://doi-org.proxy.library.uu.nl/10.1146/annurev-clinpsy-050718-095710. https://doi.org/10.1146/annurev-clinpsy-050718-095710
- Toomey, T. L., & Wagenaar, A. C. (2002). Environmental policies to reduce college drinking: Options and research findings. Journal of Studies on Alcohol, Supplement, 14(s14), 193–205. https://doi.org/10.15288/jsas.2002.s14.193
- Valentine, J. C., Biglan, A., Boruch, R. F., Castro, F. G., Collins, L. M., Flay, B. R., Kellam, S., Mościcki, E. K., & Schinke, S. P. (2011). Replication in prevention science. Prevention Science: The Official Journal of the Society for Prevention Research, 12(2), 103–117. https://doi.org/10.1007/s11121-011-0217-6
- Van Ryzin, M. J., Roseth, C. J., Fosco, G. M., Lee, Y., & Chen, C. I. (2016). A component-centered meta-analysis of family-based prevention programs for adolescent substance use. Clinical Psychology Review, 45, 72–80. https://doi.org/10.1016/j.cpr.2016.03.007
- Verdurmen, J. E. E., Koning, I. M., Engels, R. C. M. E., van den Eijnden, R. J. J. M., & Vollebergh, W. A. M. (2014). Risk moderation of a parent and student preventive alcohol intervention by adolescent and family factors: A cluster randomized trial. Preventive Medicine, 60, 88–94. https://doi.org/10.1016/j.ypmed.2013.12.027
- Valente, J. Y., Cogo-Moreira, H., & Sanchez, Z. M. (2019). Predicting latent classes of drug use among adolescents through parental alcohol use and parental style: a longitudinal study. Social Psychiatry and Psychiatric Epidemiology, 54, 455–467. https://doi.org/10.1007/s00127-018-1645-4
- Wall, M., & Casswell, S. (2013). Affordability of alcohol as a key driver of alcohol demand in New Zealand: A co-integration analysis. Addiction, 108(1), 72–79. https://doi.org/10.1111/j.1360-0443.2012.03992.x
- Watts, P., Phillips, G., Petticrew, M., Harden, A., & Renton, A. (2011). The influence of environmental factors on the generalisability of public health research evidence: Physical activity as a worked example. The International Journal of Behavioral Nutrition and Physical Activity, 8, 128. doi:10.1186/1479-5868-8-128
- Weerman, F. M., Bernasco, W., Bruinsma, G. J. N., & Pauwels, L. J. R. (2015). When is spending time with peers related to delinquency? The importance of where, what and with whom. Crime & Delinquency, 61(10), 1386–1416. https://doi.org/10.1177/0011128713478129
- Werneck, A. O., & Silva, D. R. (2020). Population density, depressive symptoms, and suicidal thoughts. Brazilian Journal of Psychiatry, 42(1), 105–106. https://doi.org/10.1590/1516-4446-2019-0541
- Weybright, E. H., Caldwell, L. L., Ram, N., Smith, E. A., & Jacobs, J. (2014). The dynamic association between healthy leisure and substance use in South African adolescents: A state and trait perspective. World Leisure Journal, 56(2), 99–109. https://doi.org/10.1080/16078055.2014.903726
- Weybright, E. H., Caldwell, L. L., Ram, N., Smith, E. A., & Wegner, L. (2016). Trajectories of adolescent substance use development and the influence of healthy leisure: A growth mixture modeling approach. Journal of Adolescence, 49, 158–169. https://doi.org/10.1016/j.adolescence.2016.03.012
- Wichstrom, T., & Wichstrom, L. (2009). Does sport participation during adolescence prevent later alcohol, tobacco, and cannabis use? Addiction, 104, 138–149. https://doi-org.proxy.library.uu.nl/10.1111/j.1360-0443.2008.02422.x doi:10.1111/j.1360-0443.2008.02422.x
- World Bank. (2018). Poverty headcount ratio at $5.50 a day (2011 PPP) (% of population). https://data.worldbank.org/indicator/SI.POV.UMIC
- Xchange database (2020). European database of evidence-based intervention targeting substance use and related behaviors. https://www.emcdda.europa.eu/best-practice/xchange_en
- Young, E. (2017). Iceland knows how to stop teen substance abuse but the rest of the world isn’t listening. The Independent. [INTERNET]. Retrieved from https://www.independent.co.uk/life-style/health-and-families/iceland-knows-how-to-stop-teen-substance-abuse-but-the-rest-of-the-world-isn-t-listening-a7526316.html