
Abstract
Social identities associated with recovery are protective of relapse from addiction. How such identities develop and differentially link to outcomes at different points of the recovery journey and across multiple recovery attempts is relatively unknown. The current study utilised a pre-existing cross-sectional dataset (n = 237 Alcoholics Anonymous (AA) members, 50% male, 49.4% female and 0.6% female-to-male, aged between 19 and 71 years) to explore these issues. Relationships between AA identity, quit efficacy (a proxy for recovery maintenance) and AA meeting attendance (over the last month) were tested. The moderating effects of length of AA attendance during the current recovery episode and first vs. subsequent quit attempts on the identity-efficacy link were also tested. Levels of social identity were stable amongst those in the early in their current recovery through to those who have more experience, but the relationships between identity and efficacy differed. While those early on in their current AA attendance showed a positive relationship between identities and frequency of attending meetings, those with more long-standing attendance reported social identification unrelated to involvement. Our results suggest that social identities may be particularly protective for those who are on their first quit, suggesting recovery formation and transition may be a priority.
Introduction
In the USA, recent figures suggest 19.7 million US citizens aged 12 years or older experience substance abuse issues, including 14.5 million people with alcohol use disorder (AUD; Substance Abuse and Mental Health Services Administration, Citation2018). The relative scale of AUD is similar in many other countries (see Davies et al., Citation2021 for an overview). For instance, in the UK, alcohol and drug addiction costs £36 billion a year from the burden on health-care, welfare and addiction related crime (Centre for Social Justice, Citation2013). This cost does not count the emotional distress, family breakdown and co-morbid illnesses (both physical and psychological) that affect both those using drugs and the people around them (see Laslett et al., Citation2019).
One effective form of treatment in the addiction space is group therapy, either within a formal therapy setting (i.e. in treatment communities or psychotherapeutic groups) or through peer-led organisations such as the recovery Fellowships (such as Alcoholics, Narcotics, Gamblers Anonymous). For alcohol consumption, the Fellowship model (Alcoholics Anonymous; AA) is highly prevalent, with around 80% of people seeking recovery in the US having contact (Dawson et al., Citation2006; Kelly et al., Citation2010) and active membership in groups such as AA can continue for decades (Frings et al., Citation2019). A recent Cochrane Review suggests that AA provides similar outcomes and benefits to other treatment modes, but may be superior in terms of continuous abstinence (Kelly et al., Citation2020). However, the development of psychosocial mechanisms which underpin the success of AA (and other group-based interventions) are relatively poorly understood. One way to understand the operation of these groups is through the lens of social identities (psychological affiliations with social groups Tajfel & Turner, Citation1979). The current paper explores how social identities change over the recovery journey amongst a sample of people actively engaging with AA, using a large and diverse cross-sectional sample.
Social identity and recovery
Recently, social identities associated with recovery have been linked with better recovery related outcomes such as treatment retention, abstinence and confidence in one’s ability to maintain treatment goals such as abstinence and harm reduction (Frings & Albery, Citation2015). In general, higher levels of recovery related identity, or increased differentiation between addiction and recovery related identities, are associated with positive outcomes (Bathish et al., Citation2017; Dingle, Stark, et al., Citation2015; Dingle, Cruwys, et al., Citation2015; Frings & Albery, Citation2017). Alongside AA, these effects have been observed amongst varied populations, including other group based treatments such as SMART (a group based CBT approach), and in both in-patient, out-patient and peer support settings (Buckingham et al., Citation2013; Dingle, Stark, et al., Citation2015; Hutchinson et al., 2018; Wolff et al., Citation2015). The Social Identity Model of Cessation Maintenance (SIMCM; Frings & Albery, Citation2015, Citation2017) argues these effects are present to the extent that social identities provide social support and normative control, increase actual and perceived efficacy, contextualise the meaning of events and behaviours, and guide automatic behavioural tendencies (Frings, Collins, et al., Citation2016; Frings, Melichar et al., Citation2016; Frings et al., Citation2019).
Social identities across time
Despite a wide range of work supporting SIMCM, and the role of identity in addiction recovery more generally, less is known how social identification with groups such as AA change over time – particularly during important transitions in the recovery journey, such as initial engagement with groups, or the period around lapses or relapses (a limited duration or consistent return to drinking behaviours respectively – both common features of the recovery process – Scott et al., Citation2005). Understanding such changes may provide insight into why not all individuals continue to attend group sessions (important as lower attendance is linked with poorer outcomes; Gossop et al., Citation2003; Marshall et al., Citation2018) and why long term outcomes in extended addiction recovery vary between individuals.
Changes in identity over time
The suite of social identities we hold are not fixed. New identities are adopted across our lifespans, sometimes voluntarily (i.e. adopting a new professional and associated occupational identity or retiring) and sometimes not (i.e. becoming a person with significant physical impairment). Such identity transitions (even when positive) are recognised to be psychologically challenging events, associated with both positive and negative experiences and outcomes (Bule & Frings, Citation2016; Gleibs et al., Citation2011; Jones & Jetten, Citation2011). Social identities are themselves dynamic constructs - defined in part by the immediate social world an individual occupies and perceives (Turner, Citation1982). The level of importance a specific identity has for the self, the similarity between the self and other people in the group, and the extent to which group members are seen as similar, also varies between group members and across time (Leach et al., Citation2008). Within the field of addiction recovery, research has explored a variety of temporal social processes such as the benefits of adopting new social connections (Best et al., Citation2016), the transition between seeing oneself as an addict and in recovery (Dingle, Cruwys, et al., Citation2015; Dingle et al., Citation2019) and the development of socially defined norms and beliefs (Frings, Collins, et al., Citation2016).
Although social identities associated with recovery have been shown to be an important part of successful recovery journeys, relatively little research has explored how levels of social identification with recovery groups changes over time (cf. Dingle, Cruwys, et al., Citation2015; Dingle, Stark, et al., Citation2015), and none has focus on changes over decades. This is important as involvement in AA can be relatively brief – perhaps a single meeting – but can also span 40 or more years (Frings et al., Citation2019). Such involvement can also include a move from being ‘treatment naïve’ (i.e. never having attempted to stop) to in recovery, or from a period of relapse back into recovery. This is important, as unsuccessful prior attempts have been shown to influence future outcomes (Chiappetta et al., Citation2014; Martin, Citation1998), but their effects on identity are not known. Changes in levels of social identification, the degree of interaction between group members (for instance, meeting attendance), and the relationships between identity and outcomes (in particular, quit efficacy, an important predictor of relapse see Frings et al., Citation2019) are all open questions which the current study aimed to address.
Social identities in early recovery
It is possible that social identities play a particularly crucial role in early recovery (i.e. the first year, see The Betty Ford Institute Consensus Panel, Citation2007), to the extent that they may be (i) a source of support that is present before other sources (such as experience) are established, (ii) protective against social networks and identities which can increase relapse risk (Beckwith et al., Citation2015; Best et al., Citation2016) and (iii) provide conscious guidance to challenge habitual behaviours (Frings & Albery, Citation2015, Citation2017). However, it may also be possible that those who are on their first recovery attempt may not receive the same beneficial effects of identity as those who are on subsequent attempts. New identities around recovery are seen as an outcome of, amongst other factors, a process of social negotiation (Best et al., Citation2016) and normative influence (Frings & Albery, Citation2015). As these processes unfold, individuals gain different understandings and response options in relation to addiction behaviours (Best et al., Citation2016; Frings & Albery, Citation2021). For instance, social identity with treatment groups contextualises the meaning of lapse and relapse (Frings, Collins, et al., Citation2016). Generally, new social identity formation also involves a period of ’remooring’ to members of existing and new social categories (Deaux & Ethier, Citation1998). The initial first recovery attempt may be a specific period during which protective aspects of identity are not fully defined. It may also be unique in that the individual has no/limited access to direct experience of either being in recovery, lapsing or relapsing, nor opportunity to reflect (in particular upon lapse/relapse) from the point of view of the new identity. In subsequent attempts, a period of reflection is available (between as well as within attempts) with identity formation ongoing. These effects may be compounded as social identities related to recovery may initially be competing with others (perhaps including identities linked with the enactment of the addictive behaviour) with risky behavioural norms and less protective understandings. Thus, in the current study we aimed to explore the possibility that social identity may be particularly important in early vs. later recovery by (i) comparing people who were on a first recovery attempt to those on a repeat attempt and (ii) testing the moderating effect of longer vs. shorter lengths of individuals’ current AA attendance.
Identity or involvement?
A related issue concerns the relative effects of involvement with the group and social identification with it on recovery related outcomes. From some perspectives, taking part in the activities of the group is a form of identity enactment (see e.g. Haslam et al., Citation2005) which in itself is a core social motive (Vignoles, Citation2011). However, both high and low identifiers can engage in greater or lesser levels of involvement, and research has shown they related to unique variances in outcomes (Taylor, McNamara, & Frings, Citation2019).
Within the addiction domain, active mutual aid group involvement has been shown to be related to positive recovery in a number of studies (Hutchison et al., Citation2018; Kelly et al., Citation2010; McKellar et al., Citation2003; Montgomery et al., Citation1995; Tappin et al., Citation2015). Involvement has been classed in these studies as activities such as attending meetings, helping others (including acting as a sponsor), supporting the functioning of the group (for instance, setting up rooms before meetings) or undertaking leadership roles. Whilst it may not be surprising that involvement leads to better outcomes, theoretical models such as SIMCM argue that it is the social identification associated with involvement which may be the important ‘active ingredient’ of recovery group processes. While clear differentiation effects of identity above and beyond contact (which could be argued to be a pre-requisite for involvement) have been observed in studies exploring depression and stress (Sani et al., Citation2012, Citation2015), little research has attempted to test this assertion in the realm of addiction. An initial exploration of this amongst members of AA suggests that while both identity and involvement were related to high efficacy, the effects of involvement were mediated by social identification, but not vice-versa (Taylor et al., Citation2020). Thus, we also aimed to explore the relationship between involvement and both social identity and efficacy.
Summary and predictions
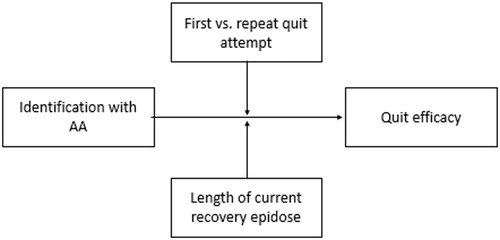
In the current study, we utilised a cross-sectional sample to look at differing levels of involvement and social identification amongst people who actively maintained AA membership and who had been in recovery for different time periods during their current quit. We also tested for a moderating effect of length of recovery episode and first/repeating recovery attempt on the identity - efficacy link observed in previous research. We achieved this by undertaking a secondary analysis of a dataset exploring the role of identity on the perception of life narratives (Frings et al., Citation2019). In line with previous work we predicted that higher levels of AA identity, involvement in AA and greater perceived future quit efficacy would all be positively related. Identity processes associated around first vs repeat quit attempts and across the length of a quit have not been quantitatively explored. However, both are theoretically likely to be important variables which could either attenuate or strengthen identity effects. As such, we predicted a moderating effect of both of these factors on the identity to efficacy relationship but made no specific hypotheses as to the direction of moderation ().
Figure 1. Potential moderation of the identity to efficacy relationship by first vs. repeat quit attempt and length of current recovery episode.
Materials & methods
Data used in the current study were collected as part of a study exploring the links between social identity as an AA member and perceived self-relevance of ‘tales of hope’ (life narratives), perceived quit efficacy and perceived cost of relapse to the self and groups (see below and also Frings et al., Citation2019 for full details).
Participants
Participants in Frings et al., (Citation2019) were recruited using a snowball methodology. An initial call for participants to take part in a short study exploring the psychological underpinnings of AA were placed on two relevant ‘reddit’ forums, on one of the author’s psychology-based blog and via online social networks (Facebook and Twitter). The calls included a request to forward to interested parties. These calls were subsequently reposted to other channels by other people. A sample of 237 members of Alcoholics Anonymous was recruited (operationalised as participants self-selecting on the basis of AA membership, and indicating they identified with the group via the scales below). Of these, 165 were complete cases (for each analysis, data were included from participants who had completed the relevant measures). The mean age of the sample who completed demographic items (n = 170), ranged from 19–71 years (M = 45.40, SD = 13.21). Eighty-five (50%) were male, 84 (49.4%) female and one participant (0.6%) self-reported as female-to-male.
Design
The current study comprises a secondary data analysis utilising a cross-sectional correlational design. The key variables included social AA identity, quit efficacy, level of involvement (operationalised as number of meetings per month), length of current recovery episode and whether the current episode was a first/repeating recovery attempt. Other measures (perceived relevance and perceived utility of a tale of hope, and perceived cost of relapse to self and others) were not considered in the present study, but are detailed in Frings et al., (Citation2019).
Materials
Social identity
Level of AA identity was measured using the multi-component in-group identification scale (Leach et al., Citation2008). This fourteen item scale has items related to solidarity with the group (i.e. ‘I feel a bond with AA’), satisfaction (‘I am glad to be an AA member’), centrality (‘The fact I am an AA member is an important part of my identity’), self-stereotyping (‘I have a lot in common with the average AA member’) and in-group heterogeneity (‘AA members have a lot in common with each other’). All items were recorded on seven-point Likert scales, anchored at 1 (Very strongly disagree) and 7 (Very strongly agree). In the current study, internal reliability for this scale was good (Cronbach’s α = 0.94).
Quit efficacy
Perceived quit efficacy was measured using an established scale (Buckingham et al., Citation2013) consisting of four items (‘I can remain abstinent’,’ I can manage my addiction’, ‘It is unlikely that I will remain alcohol free’ (reverse scored) and ‘I think I can achieve recovery’ using the same 7 point scales as personal relevance. Internal reliability for this variable was low but acceptable (Cronbach’s α = 0.58). Removing one item (I can manage my addiction) improved this marginally to 0.60. A mean score was calculated, with higher scores representing greater efficacy.
Length of current recovery episode AA attendance
Participants were asked ‘How many months have you attended AA during this quit attempt?’
Number of recovery attempts
Participants were asked to record the number of recovery attempts to date with two items. The initial item asked ‘is this your first quit attempt?’. Participants who indicated this was not their first attempt were also asked ‘how many previous quits have you had’?) We chose to dichotomise the response to these items into first vs subsequent attempts as it is reasonable to assume the psychological meaning of moving between 0 and 1 attempts is likely to differ from 1 and 2 (or 32 and 33, etc.), and initial recovery attempts are the focus of interest in the current paper.
Number of meetings
Participants were asked how many meetings they had attended in the last month.
Procedure
Upon being directed to the website, participants gave informed consent, and completed the measures in the order described above, before answering demographic questions. Finally, they were thanked for their time and debriefed.
Ethics statement
The research which the dataset was collected via received ethical approval from London South Bank University School of Applied Sciences. The ethical approval number is ETH1819-0030.
Results
Data analysis strategy
To test (i) relationships between AA identity, involvement in AA and greater perceived future quit efficacy, (ii) the differences between first vs. repeat quit attempts and (iii) moderating effects of first vs. repeat quit attempts and length of current AA attendance on the identity to efficacy relationship, a three-stage approach was adopted. In the first stage, zero order correlations between variables were tested. In the second, levels of outcomes between participants undergoing first vs. repeat quit attempts were tested. Finally, moderation models were constructed to test the relationship between identity and efficacy under differing levels of the moderating factors.
Missing case analysis
Missing case analysis using t-tests did not reveal differences between completed cases vs missing cases in mean age, meeting attendance, length of current AA attendance, and quit efficacy (ps>.198). Chi square analysis of completed cases revealed no difference in the distribution of gender (p=.64, including males and females only) or first quit status (p=.73).
Correlational analysis
Pearson’s zero order correlations revealed that AA identity had a significant positive relationship with both efficacy and meeting attendance (). Efficacy was unrelated to length of current AA attendance. Meeting attendance was not linked to efficacy but was significantly negatively related to length of current recovery episode.
Table 1. Descriptive statistics and relationships between variables (Pearson’s rs).
First vs. repeat attempt differences
Within the sample, levels of quit efficacy did not differ between those undertaking initial recovery attempts (n = 64, M = 5.89, SD = 1.01) and repeat attempts (n=116, M=5.73, SD=1.21), t(178)=0.89, p=.373. Nor did length of current AA attendance (Ms[SDs] = 116.90 [135.96] vs. 88.10 [106.53], t(167)=1.524, p=.129) or number of meetings attended (Ms[SDs] = 12.82 [7.50] vs. 13.30 [9.31], t(37)=0.19, p=.985) differ.
Moderation analysis
To test the potentially moderating effects of length of current AA attendance and initial vs. repeat quit status on the identity/efficacy link, moderation analysis was conducted using the Hayes (Citation2017) process macro (V3.3).
Models were constructed to test the relationship between identity and efficacy with two moderators (length of current AA attendance and initial/repeat recovery status). Five thousand bootstrap samples were taken.
Correlations () suggested no multicollinearity. Multivariate outlier analysis revealed 2 multivariate outliers – excluding these made no difference to the pattern of results or significance, and analysis of the full dataset is reported below. There was a moderate skew on the outcome variable (skew statistic = −0.998, SE = 0.178). Transformations were not applied as the bootstrapping approach adopted is a recognised method of analysing skewed data in parametric models (see Efron, Citation1979; Sainani, Citation2012). An examination of variances associated with each variable revealed some evidence of a lack of homoscedasticity between months of current quit and other variables. Again, no adjustments were made as the bootstrapping approach provides an established mitigation for this (Cribari-Neto & Zarkos, Citation1999).
The overall model was significant predictor of variance in efficacy R2=0.17 F(5, 163)=6.87, p<.001. As can be seen in , identity was positively linked with efficacy. Recovery type (first vs. subsequent) was linked to efficacy with people not on their first quit reporting higher efficacy (in contrast to the t-tests reported above). Current recovery episode length was unrelated to efficacy (in contrast to the correlation reported above). Of the moderation effects, the identity efficacy link was moderated by first/repeat recovery status, but not by length of current AA attendance. Further analysis unpacking this interaction revealed that the identity-efficacy link was present amongst both initial and repeat recovery participants, but the effect was stronger amongst participants who were undertaking their first quit ().
Table 2. Moderating effects of length of current recovery episode length and first/repeat recovery type on the identity efficacy link.
Table 3. Moderation of identity – efficacy link by recovery type.
Discussion
Social identities are increasingly recognised as an important part of the recovery process but how they evolve and differentially affect recovery over time is not well understood. In the current study, we examined relationships between group involvement and social identification amongst people who were members of AA with varying years of being in recovery. We also explored how the effect of length of current AA attendance duration and whether participants were undergoing a first or subsequent recovery attenuated or strengthened the identity – quit efficacy link. It was predicted that positive relationships between AA identity, involvement in AA and greater efficacy would all be observed. Given the extant literature, a moderating effect of both of these factors was predicted, but directional hypotheses were not made.
The findings of the current study suggest that levels of identity were generally stable over time for people who stay in AA. However, levels of involvement (operationalised in the current study by meeting attendance in the last month) dropped off over time – perhaps due to a combination of socialisation processes which encourage intense attendance in early months, but also due to other factors, possibly including changes in the way identities are experienced. In terms of the latter, these findings present an intriguing possibility – namely that during the early phases of identification with a new social category, regular contact with group members is important or highly desirable. However, as time goes by (and, perhaps as the identity is increasingly internalised in a social cognitive sense, see Frings & Albery, Citation2017), the lack of a correlation between involvement and identity suggests that contact with the group becomes less of a prerequisite for maintaining the group identity and associated behaviours and is thus engaged with less often. This account is in line with ideas around automaticity and in particular the idea that social cognitive constructs require significant amounts of ‘training’ or activation to become established but are then slow to decay even without subsequent reinforcement through activation of associated constructs (Lindgren et al., Citation2017). To put this another way, the group acts as a stimulus which creates or activates the social cognitive constructs comprising representations associated with one’s social identity and associated behavioural schemas (Wiers et al., Citation2010). Once established, this identity-related representational set may be activated automatically in the mere presence of a stimulus (Frings & Albery, Citation2015, Citation2017). Perhaps as a result of these processes, our findings also suggest that in our sample it was identity, but not number of meetings attended (a measure of involvement), which was related positively to quit efficacy (a marker of subsequent quit success, see Buckingham et al., Citation2013; Gulliver et al. Citation1995; Miller et al., Citation1996). This is in line with other research suggesting it is identity which is the ‘active ingredient’ of various therapeutic groups, including those around addiction, but also other groups. Support for this assertion has been found in research on support groups for individuals with diverse conditions including Multiple Sclerosis, eating disorders, depression and anxiety amongst others (see e.g. Cruwys et al., Citation2016; Haslam et al., Citation2016; Sani et al., Citation2012, Citation2015; Taylor et al., Citation2020; Wakefield et al., Citation2013).
An additional aim of this paper was to investigate how those who were undertaking their first quit attempt differed from those with one or more previous quit attempts. We also wanted to explore the extent to which the link between identity and efficacy (observed in numerous other studies) changes across people’s current recovery journey. Moderation analysis suggests that the relationship between social identity as a member of AA and quit self-efficacy was moderated by whether or not people were on their initial quit attempt or not. In both cases, a positive relationship was observed between identity and efficacy. However, this effect was greater (around twice as large) in individuals who were on their first quit attempt.
This moderation effect could have been observed for a number of reasons. First of all, work has proposed that social connections with non-using others are a key predictor of quit success, particularly in early recovery (Best et al., Citation2016). It is reasonable to propose that social identities associated with recovery are linked with the formation of such social connections, and may thus have an immediate impact on efficacy. Secondly, identity may also be important in early recovery as people may have fewer other resources (such as knowledge or effective relapse avoidance strategies and experience) to draw upon. As they may simultaneously face greater demands (such as more frequent psychological craving), the effect of one of (relatively fewer) psychological resources may be greater than for those on subsequent attempts. Thirdly, identity may also be related to other important outcome variables such as shaping understanding of what recovery means and what relapse is (willingness to persist and/or increase resilience against failure). Whilst these may not be predictive of early relapse directly, they may well be protective against failing to re-engage with recovery after setbacks (see Frings et al., Citation2019). Similarly, having complex, well-established social identities may present protection in ways not captured in the current study. For instance, longer/repeat quit individuals may benefit from identities in other ways such as via better outcomes when behaviour is guided by more automated processes such as habit (Albery et al., Citation2015; Frings, Melichar, et al., Citation2016; Lindgren et al., Citation2016). However, the current findings suggest that interventions which facilitate social identity development are likely to be beneficial, and these effects may be particularly helpful for those on their first quit attempts.
As well as these open conceptual questions, the current study has a number of methodological limitations. The sample was self-selecting responding to a request for AA members to take part in research. This has two implications for interpretation. First, levels of AA identity may be higher in this sample than in the general population of people who have been/are in contact with AA. Second, it is possible that people in AA for longer periods are more likely to be abstinent than those who have left, and those who may start to drink again may leave AA earlier than those who do not. These dual effects may result in the analysis of long-term members showing higher levels of efficacy than would be observed in a more representative sample of the population. Related to this, our definition of a recovery episode was driven by months attending AA - which could vary from the start of both an individuals’ entire recovery journey, or from the start of a specific recovery episode. However, defining a recovery episode is in itself difficult, as start points can be conceptualised in various ways depending on one’s theoretical and/or lay perspective. For instance, the ‘start’ can be understood as being from the start of a given recovery attempt which can be the same or different to the date of a recent lapse. From other perspectives, that ‘start’ can also include contemplating the possibility of change (i.e. the transtheoretical model, see Prochaska & DiClemente, Citation1983). However, the variance between joining AA during the current quit attempt and a move from contemplation/or preparation to action is likely to be proportionally small against the range of episode lengths observed (weeks or possible months vs up to 50 years), which provides confidence variance associated with this design decision is likely incidental.
Unexpectedly, the internal reliability of the self-efficacy measure in the study was relatively low. This was unexpected given its stable reliability across a variety of other studies, including those involving Fellowships. It may be in part driven by AA’s core assumption that addiction cannot be ‘managed’. Differences between this study and previous work may be reflected in the heterogeneity of the current sample in terms of AA membership length, and/or may reflect changes in how people understand efficacy across the recovery journey. This warrants further investigation. This may also have impacted the relationship between AA meeting attendance and efficacy, to the extent the reliability may have been differentially affected by those with greater or lesser attendance rates. Finally, as we were interested in changes spanning many years, the data were cross-sectional, the measures were taken simultaneously, and the relationships observed correlational. This presents a need for longitudinal work to explore the extent to which the relationships observed in this and other work are causational.
In conclusion, this research presents a novel insight into how social identification with social categories associated with addiction recovery develop. It suggests that, although levels of social identity are relatively stable amongst those in the early stages of their current recovery episode through to those who have more experience, the effects of identity on efficacy may differ over time. Moreover, while those early on in their current recovery show a positive relationship between identities and frequency of attending meetings, those with more long-standing social identities may experience the same level of identity regardless of group involvement. Similar to this, our findings suggest that it is the level of social identification itself rather than the level of involvement associated with it, which is related to higher self-efficacy. Finally, our results suggest that social identities may be particularly protective for those who are on their first recovery attempt suggesting recovery formation and transition may be a treatment priority during this period.
Author contributions
DF and IA conceptualised the study. Analysis was conducted by DF with input from KW. DF, IA and KW completed the drafting of the manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data sharing
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- Albery, I. P., Collins, I., Moss, A. C., Frings, D., & Spada, M. M. (2015). Habit predicts in-the-moment alcohol consumption. Addictive Behaviors, 41, 78–80. https://doi.org/https://doi.org/10.1016/J.ADDBEH.2014.09.025
- Bathish, R., Best, D., Savic, M., Beckwith, M., Mackenzie, J., & Lubman, D. I. (2017). “Is it me or should my friends take the credit?” The role of social networks and social identity in recovery from addiction. Journal of Applied Social Psychology, 47(1), 35–46. https://doi.org/https://doi.org/10.1111/jasp.12420
- Beckwith, M., Best, D., Dingle, G. A., Perryman, C., & Lubman, D. (2015). Predictors of flexibility in social identity among people entering a therapeutic community for substance abuse. Alcoholism Treatment Quarterly, 33(1), 93–104. https://doi.org/https://doi.org/10.1080/07347324.2015.982465
- Best, D., Beckwith, M., Haslam, C., Alexander Haslam, S., Jetten, J., Mawson, E., & Lubman, D. I. (2016). Overcoming alcohol and other drug addiction as a process of social identity transition: the social identity model of recovery (SIMOR). Addiction Research & Theory, 24(2), 111–123. https://doi.org/https://doi.org/10.3109/16066359.2015.1075980
- Buckingham, S. A., Frings, D., & Albery, I. P. (2013). Group membership and social identity in addiction recovery. Psychology of Addictive Behaviors: Journal of the Society of Psychologists in Addictive Behaviors, 27(4), 1132–1140. https://doi.org/https://doi.org/10.1037/a0032480
- Bule, B., & Frings, D. (2016). The role of group membership continuity and multiple memberships on mental well-being amongst post-operative stoma patients. Psycho-oncology, 25(6), 726–728. https://doi.org/https://doi.org/10.1002/pon.4006
- Centre for Social Justice. (2013). No Quick Fix. Exposing the depth of Britain's drug and alcohol problem. The Centre for Social Justice.
- Chiappetta, V., García-Rodríguez, O., Jin, C. J., Secades-Villa, R., & Blanco, C. (2014). Predictors of quit attempts and successful quit attempts among individuals with alcohol use disorders in a nationally representative sample. Drug and Alcohol Dependence, 141, 138–144. https://doi.org/https://doi.org/10.1016/j.drugalcdep.2014.05.019
- Cribari-Neto, F., & Zarkos, S. G. (1999). Bootstrap methods for heteroskedastic regression models: Evidence on estimation and testing. Econometric Reviews, 18(2), 211–228. https://doi.org/https://doi.org/10.1080/07474939908800440
- Cruwys, T., Platow, M. J., Rieger, E., Byrne, D. G., & Haslam, S. A. (2016). The social psychology of disordered eating: The Situated Identity Enactment model. European Review of Social Psychology, 27(1), 160–195. https://doi.org/https://doi.org/10.1080/10463283.2016.1229891
- Davies, E. L., Puljevic, C., Connolly, D., Zhuparris, A., Ferris, J. A., & Winstock, A. R. (2021). The world’s favorite drug: What we have learned about alcohol from over 500,000 respondents to the Global Drug Survey. In D. Frings & I. P. Albery (Eds.), The handbook of alcohol use. Understandings from synapse to society (pp. 17–48). Academic Press.
- Dawson, D. A., Grant, B. F., Stinson, F. S., & Chou, P. S. (2006). Estimating the effect of help-seeking on achieving recovery from alcohol dependence. Addiction (Abingdon, England), 101(6), 824–834. https://doi.org/https://doi.org/10.1111/j.1360-0443.2006.01433.x
- Deaux, K., & Ethier, K. A. (1998). Negotiating Social Identity. In J. Swim & C. Strangor (Eds.), Prejudice. The targets perspective (pp. 301–323). Academic Press.
- Dingle, G. A., Cruwys, T., & Frings, D. (2015). Social identities as pathways into and out of addiction. Frontiers in Psychology, 6, 1795. https://doi.org/https://doi.org/10.3389/fpsyg.2015.01795
- Dingle, G. A., Haslam, C., Best, D., Chan, G., Staiger, P. K., Savic, M., Beckwith, M., Mackenzie, J., Bathish, R., & Lubman, D. I. (2019). Social identity differentiation predicts commitment to sobriety and wellbeing in residents of therapeutic communities. Social Science and Medicine, 237, 112459. https://doi.org/https://doi.org/10.1016/j.socscimed.2019.112459
- Dingle, G. A., Stark, C., Cruwys, T., & Best, D. (2015). Breaking good: Breaking ties with social groups may be good for recovery from substance misuse. British Journal of Social Psychology, 54(2), 236–254. https://doi.org/https://doi.org/10.1111/bjso.12081
- Efron, B. (1979). Bootstrap methods: Another look at the jackknife. Annals of Statistics, 1, 1–26. https://doi.org/https://doi.org/10.1007/978-1-4612-4380-9_41
- Frings, D., & Albery, I. P. (2015). The social identity model of cessation maintenance: Formulation and initial evidence. Addictive Behaviors, 44, 35–42. https://doi.org/https://doi.org/10.1016/j.addbeh.2014.10.023
- Frings, D., & Albery, I. P. (2017). Developing the social identity model of cessation maintenance: theory, evidence and implications. In Sarah Buckingham & David Best (Eds.), Addiction, behavioural change and social identity. The pathway to resilience and recovery (pp. 128–148). Routledge.
- Frings, D., & Albery, I. P. (2021). An identity-based explanatory framework for alcohol use and misuse. In D. Frings & I. P. Albery (Eds.), The handbook of alcohol use: Understandings from synapse to society (pp. 329–345). Academic Press.
- Frings, D., Collins, M., Long, G., Pinto, I. R., & Albery, I. P. (2016). A test of the Social Identity Model of Cessation Maintenance: The content and role of social control. Addictive Behaviors Reports, 3, 77–85. https://doi.org/https://doi.org/10.1016/j.abrep.2016.02.003
- Frings, D., Melichar, L., & Albery, I. P. (2016). Implicit and explicit drinker identities interactively predict in-the-moment alcohol placebo consumption. Addictive Behaviors Reports, 3, 86–91. https://doi.org/https://doi.org/10.1016/j.abrep.2016.04.002
- Frings, D., Wood, K. V., Lionetti, N., & Albery, I. P. (2019). Tales of hope: Social identity and learning lessons from others in Alcoholics Anonymous: A test of the social identity model of cessation maintenance. Addictive Behaviors, 93, 204–211. https://doi.org/https://doi.org/10.1016/j.addbeh.2019.02.004
- Gleibs, I. H., Haslam, C., Jones, J. M., Alexander Haslam, S., McNeill, J., & Connolly, H. (2011). No country for old men? The role of a 'Gentlemen's Club' in promoting social engagement and psychological well-being in residential care. Aging & Mental Health, 15(4), 456–466. https://doi.org/https://doi.org/10.1080/13607863.2010.536137
- Gossop, M., Harris, J., Best, D., Man, L.-H., Manning, V., Marshall, J., & Strang, J. (2003). Is attendance at Alcoholics Anonymous meetings after inpatient treatment related to improved outcomes? A 6-month follow-up study. Alcohol and Alcoholism, 38(5), 421–426. https://doi.org/https://doi.org/10.1093/alcalc/agg104
- Gulliver, S. B., Hughes, J. R., Solomon, L. J., & Dey, A. N. (1995). An investigation of self-efficacy, partner support and daily stresses as predictors of relapse to smoking in self-quitters. Addiction, 90(6), 767–772. https://doi.org/https://doi.org/10.1046/j.1360-0443.1995.9067673.x
- Haslam, S. A., O'Brien, A., Jetten, J., Vormedal, K., & Penna, S. (2005). Taking the strain: Social identity, social support, and the experience of stress. British Journal of Social Psychology, 44, 355–370.
- Haslam, C., Cruwys, T., Haslam, S. A., Dingle, G., & Xue-Ling, M. (2016). Groups 4 Health: Evidence that a social-identity intervention that builds and strengthens social group membership improves mental health. Journal of Affective Disorders, 194, 188–195. https://doi.org/https://doi.org/10.1016/J.JAD.2016.01.010
- Hayes, A. (2017). Introduction to mediation, moderation, and conditional process analysis: A regression‐based approach. The Guildford Press.
- Hutchison, P., Cox, S., & Frings, D. (2018). Helping you helps me: Giving and receiving social support in recovery groups for problem gamblers. Group Dynamics: Theory, Research, and Practice, 22(4), 187–199. https://doi.org/https://doi.org/10.1037/gdn0000090
- Jones, J. M., & Jetten, J. (2011). Recovering from strain and enduring pain. Social Psychological and Personality Science, 2(3), 239–244. https://doi.org/https://doi.org/10.1177/1948550610386806
- Kelly, J. F., Abry, A., Ferri, M., & Humphreys, K. (2020). Alcoholics Anonymous and 12-step facilitation treatments for alcohol use disorder: A distillation of a 2020 Cochrane review for clinicians and policy makers. Alcohol and Alcoholism, 55(6), 641–651. https://doi.org/https://doi.org/10.1093/alcalc/agaa050
- Kelly, J. F., Stout, R. L., Magill, M., Tonigan, J. S., & Pagano, M. E. (2010). Mechanisms of behavior change in alcoholics anonymous: does Alcoholics Anonymous lead to better alcohol use outcomes by reducing depression symptoms? Addiction, 105(4), 626–636. https://doi.org/https://doi.org/10.1111/j.1360-0443.2009.02820.x
- Laslett, A.M. Room, R., Waleewong, O., Stanesby, O., Callinan, S. (Eds). (2019). Harm to others from drinking: patterns in nine societies. World Health Organization.
- Leach, C. W., van Zomeren, M., Zebel, S., Vliek, M. L. W., Pennekamp, S. F., Doosje, B., Ouwerkerk, J. W., & Spears, R. (2008). Group-level self-definition and self-investment: A hierarchical (multicomponent) model of in-group identification. Journal of Personality and Social Psychology, 95(1), 144–165. https://doi.org/https://doi.org/10.1037/0022-3514.95.1.144
- Lindgren, K. P., Gasser, M. L., Werntz, A., Namaky, N., Baldwin, S. A., & Teachman, B. A. (2016). Moderators of implicit and explicit drinking identity in a large US adult sample. Addictive Behaviors, 60, 177–183. https://doi.org/https://doi.org/10.1016/J.ADDBEH.2016.04.022
- Lindgren, K. P., Neighbors, C., Gasser, M. L., Ramirez, J. J., & Cvencek, D. (2017). A review of implicit and explicit substance self-concept as a predictor of alcohol and tobacco use and misuse. The American Journal of Drug and Alcohol Abuse, 43(3), 237–246. https://doi.org/https://doi.org/10.1080/00952990.2016.1229324
- Marshall, S. W., Albery, I. P., & Frings, D. (2018). Who stays in addiction treatment groups? Anxiety and avoidant attachment styles predict treatment retention and relapse. Clinical Psychology & Psychotherapy, 25(4), 525–531. https://doi.org/https://doi.org/10.1002/cpp.2187
- Martin, C. S. (1998). Diagnosis and assessment of alcohol use disorders among adolescents. Alcohol Research and Health, 22, 95–105.
- McKellar, J., Stewart, E., & Humphreys, K. (2003). Alcoholics Anonymous involvement and positive alcohol-related outcomes: Cause, consequence, or just a correlate? A prospective 2-year study of 2,319 alcohol-dependent men. Journal of Consulting and Clinical Psychology, 71(2), 302–308. https://doi.org/https://doi.org/10.1037/0022-006X.71.2.302
- Miller, W. R., Westerberg, V. S., Harris, R. J., & Tonigan, J. S. (1996). What predicts relapse? Prospective testing of antecedent models. Addiction, 91(12s1), 155–172. https://doi.org/https://doi.org/10.1046/j.1360-0443.91.12s1.7.x
- Montgomery, H. A., Miller, W. R., & Tonigan, J. S. (1995). Does Alcoholics Anonymous involvement predict treatment outcome. Journal of Substance Abuse Treatment, 12(4), 241–246. https://doi.org/https://doi.org/10.1016/0740-5472(95)00018-Z
- Prochaska, J. O., & DiClemente, C. C. (1983). Stages and processes of self-change of smoking: Toward an integrative model of change. Journal of Consulting and Clinical Psychology, 51(3), 390–395. https://doi.org/https://doi.org/10.1037/0022-006X.51.3.390
- Sainani, K. L. (2012). Dealing with non-normal data. PM & R: The Journal of Injury, Function, and Rehabilitation, 4(12), 1001–1005. https://doi.org/https://doi.org/10.1016/j.pmrj.2012.10.013
- Sani, F., Herrera, M., Wakefield, J. R. H., Boroch, O., & Gulyas, C. (2012). Comparing social contact and group identification as predictors of mental health. The British Journal of Social Psychology, 51(4), 781–790.
- Sani, F., Madhok, V., Norbury, M., Dugard, P., & Wakefield, J. R. H. (2015). Greater number of group identifications is associated with lower odds of being depressed: Evidence from a Scottish community sample. Social Psychiatry and Psychiatric Epidemiology, 50(9), 1389–1397. https://doi.org/https://doi.org/10.1007/s00127-015-1076-4
- Scott, C. K., Foss, M. A., & Dennis, M. L. (2005). Pathways in the relapse—treatment—recovery cycle over 3 years. Journal of Substance Abuse Treatment, 28(2), S63–S72. https://doi.org/https://doi.org/10.1016/J.JSAT.2004.09.006
- Substance Abuse and Mental Health Services Administration. (2018). Key substance use and mental health indicators in the United States: Results from the 2017 National Survey on Drug Use and Health. Retrieved March 25, 2019, from https://www.samhsa.gov/data/report/2017-nsduh-annual-national-report
- Tajfel, H., & Turner, J. (1979). An integrative theory of intergroup conflict. In W. G. Austin & S. Worchel (Eds.), The social psychology of intergroup relations (pp. 33–47). Brooks/Cole.
- Tappin, D., Bauld, L., Purves, D., Boyd, K., Sinclair, L., MacAskill, S., McKell, J., Friel, B., McConnachie, A., de Caestecker, L., Tannahill, C., Radley, A., & Coleman, T, Cessation in Pregnancy Incentives Trial Team (2015). Financial incentives for smoking cessation in pregnancy: randomised controlled trial. British Medical Journal, 350(jan27 4), h134–h134. https://doi.org/https://doi.org/10.1136/BMJ.H134
- Taylor, I., McNamara, N., & Frings, D. (2020). The ‘doing’ or the ‘being’? Understanding the roles of involvement and social identity in peer-led addiction support groups. Journal of Applied Social Psychology, 50(1), 3–9. https://doi.org/https://doi.org/10.1111/jasp.1263.5
- The Betty Ford Institute Consensus Panel. (2007). What is recovery? A working definition from the Betty Ford Institute. Journal of Substance Abuse Treatment, 33, 221–228. https://doi.org/https://doi.org/10.1016/j.jsat.2007.06.001
- Turner, J. (1982). Towards a cognitive redefinition of the social group. In H. Tajfel (Ed.), Social identity and intergroup relations (pp. 15–40). Cambridge Univeristy Press.
- Vignoles, V.L. (2011). Identity motives. In Seth Schwartz, Koen. Luyckx & Vivian Vignoles (Eds.), Handbook of identity theory and research (pp. 403–432). Springer.
- Wakefield, J. R. H., Bickley, S., & Sani, F. (2013). The effects of identification with a support group on the mental health of people with multiple sclerosis. Journal of Psychosomatic Research, 74(5), 420–426. https://doi.org/https://doi.org/10.1016/J.JPSYCHORES.2013.02.002
- Wiers, R. W., Rinck, M., Kordts, R., Houben, K., & Strack, F. (2010). Retraining automatic action-tendencies to approach alcohol in hazardous drinkers. Addiction, 105(2), 279–287. https://doi.org/https://doi.org/10.1111/j.1360-0443.2009.02775.x
- Wolff, N., von Hippel, C., Brener, L., & von Hippel, W. (2015). Implicit identification with drug and alcohol use predicts retention in residential rehabilitation programs. Psychology of Addictive Behaviors, 29(1), 136–141. https://doi.org/https://doi.org/10.1037/adb0000004