
Abstract
According to the World Health Organization stress in the workplace is becoming a major challenge of employers worldwide. While perceived stress levels can be assessed by questionnaires there is growing evidence that stress-related wear and tear of our body can be measured by the Allostatic Load Index (ALI). In a sample of 12,477 German industrial employees (19.6% female, 18–65 years) self-rated stress was explored by the effort-reward imbalance (ERI) questionnaire. A voluntary health check included biomarkers such as diastolic blood pressure, waist circumference, glycosylated hemoglobin, low-density lipoprotein, and heart rate variability. Based on predefined subclinical cutoff values, a 5-variable ALI was calculated. Differences in ALI according to low (ERI ≤1.0) and high (ERI >1.0) stress levels were tested. The association of ERI and ALI was explored using logistic regression analysis controlling for multiple confounders. Employees perceiving high stress levels showed significant higher ALI scores (p < .001) compared to lower stressed employees. This association was stronger in men and independent of age. ALI was associated with work stress in adjusted models (OR 1.18 ± .08 [95% CI 1.03, 1.36]; p < .05). This study replicates former results in a large sample of industrial employees indicating that work stress is associated with a short form ALI.
Introduction
Psychosocial stress at the workplace is common and the impact on employee health has been extensively investigated during the past decades. Chronic stress at the workplace can lead to major health problems such as depression (Theorell et al., Citation2015), cardiovascular disease (Backé et al., Citation2012), and musculoskeletal disorders (Lundberg, Citation2015) as well as psychosomatic complaints (Ruotsalainen et al., Citation2015).
Different concepts have been developed to demonstrate the root causes of work-related stress. The Effort-Reward-Imbalance Model (ERI) (Siegrist et al., Citation2004) presents extraordinary evidence for the association with major stress-related diseases. The model is characterized by a discrepancy between work-related efforts (e.g. workload, time pressure and interruptions) and rewards (e.g. career perspectives, job security, esteem and salary) with a disparity of high efforts and low rewards indicating the most perceived stress.
The framework of “allostatic load” has been developed by McEwen and Stellar (McEwen & Stellar, Citation1993) to provide a possible explanation for the cumulative biological impact of chronic and repeated stress exposure. The goal of allostasis is to maintain stability within the human body by adapting to psychosocial stressors. To reach this goal different biological variables are released called “primary mediators”, such as neuroendocrine and anti-inflammatory variables as well as a shift in sympathovagal balance. Sub-clinical disturbances may occur such as increased cardiovascular, immunological, and metabolic biomarkers called “secondary outcomes”. The consequence of chronic stress dysregulation is a clinical manifestation of adverse health disturbances known as “tertiary outcomes”. Seeman et al. (Citation1997) operationalized the Allostatic Load Index (ALI) to provide an early indicator for the cumulative “wear and tear” of the body caused by psychosocial burden. Elevated ALI scores have been linked to multiple adverse health conditions such as cardiovascular disease (Sabbah et al., Citation2008) and reduced mental health (McEwen, Citation2003). According to previous work, the index should include at least one variable of neurophysiologic pathways (primary mediator) and one biomarker showing strong predictive power for future diseases (secondary outcome) (Goldman et al., Citation2006; Karlamangla et al., Citation2002; Mauss et al., Citation2015b).
A recent study explored a positive association of work-related stress, operationalized by the effort-reward imbalance model, and the Allostatic Load Index in a sample of 3797 German industrial employees (Mauss et al., Citation2015a). A short form of this index including five variables (diastolic blood pressure, glycosylated hemoglobin, low-density lipoprotein, waist circumference, heart rate variability) showed good results to measure employees at risk for work-related stress. Assuming it is beneficial to use a short form index for allostatic load, there is a scientific need to replicate new study findings to avoid statistical misinterpretation and publication bias, to reduce limitations of the origin study as well as to build up valid and robust scientific evidence (Ferguson & Heene, Citation2012). It is a common approach to replicate previous study results within a bigger study sample to enlarge statistical power (Gelman & Carlin, Citation2014). The aim of the present cross-sectional study was to replicate the results of the mentioned study above using the same 5-variable Allostatic Load Index in a large sample of German employees working in different industries.
Methods
Study population
A total of 19,274 healthy employees at nineteen sites of four German industrial companies drawn from the Mannheim Industrial Cohort Studies (MICS) were eligible to take part in a voluntary on-site health assessment during regular working hours between September 2009 and Mai 2013. The participants included white and blue collar employees of a pharmaceutical, automobile, aeronautic, and electricity company. No incentive except a full personal health report was provided. The cohort spanned all levels of socio-economic status. The participants with missing values on any data of the questionnaire or clinical examination were excluded from the analyses. A total of 12,477 employees (response rate, 64.7%) presented a full data set, including 2446 women and 10,031 men (80.4%). The age range of the sample was 18–65 years (mean age 42.0 ± 10.9 years). The study was approved by the Medical Ethic Committee II of the Mannheim Medical Faculty of Heidelberg University (2010-296E-MA) in accordance with the Declaration of Helsinki. Written informed consent was given by each participant.
Measurements
The participants’ age, gender, medical history for three major diseases (cardiovascular disease, arterial hypertension, diabetes mellitus) as well as current smoking status were assessed by paper and online questionnaires. Work-related stress was measured using a short form of the effort-reward questionnaire (Li et al., Citation2012). The two subscales of effort (3 items, Cronbach’s α 0.76) and reward (7 items, Cronbach’s α 0.80) were scored on a five-point Likert scale (1 = strongly disagree; 5 = strongly agree). Effort-reward ratio was calculated using the sum score of both subscales with a value >1.0 indicating work-related stress (Siegrist, Citation1996).
Clinical measurements assessed waist circumference, body-mass-index (BMI), diastolic and systolic blood pressure, fasting blood samples, as well as heart rate variability (HRV). Waist circumference (centimeters) was measured horizontally around the smallest circumference between the ribs and iliac crest, or at the navel if no natural waistline was present. BMI (weight in kilograms/height in meters2) was assessed with participants dressed in light clothes and without shoes. Blood pressure (mmHg) was analyzed by the mean of two recordings with the participant in a seated position after a standardized five minutes rest period using an automated Critikon Dinamap Portable and Neonatal Vital Signs Monitor (Model 8100). Fasting blood samples were collected between 7 and 9 a.m. and included low-density lipoprotein (LDL), high-density lipoprotein (HDL), triglycerides, fasting plasma glucose (FPG), glycosylated hemoglobin (HbA1c), white blood cells, and C-reactive protein (CRP). All blood samples were immediately transported to a single commercial laboratory (Synlab, Augsburg, Germany) and analyzed within 24 h using standardized laboratory procedures.
Long term heart rate was recorded and participants were asked to return the HR recorder (t6 Suunto Memory Belt, SuuntoVantaa, Finland) after a minimum of 22 hours. The root mean square of successive differences (RMSSD) was determined in beat-to-beat intervals between two successive R-spikes, with increased RMSSD values indicating elevated parasympathetic activity. All HRV data were analyzed by researchers at the Center for Neuropsychological Research (University of Trier, Germany) according to the Task Force Guidelines (Malik et al., Citation1996). Due to artifacts and missing values only day recordings were analyzed for this study. Characteristics of the study sample are reported in .
Table 1. Characteristics of the study sample (n = 12,477).
Calculation of the allostatic load index
According to the nature of our replication study the Allostatic Load Index included the following five variables: diastolic blood pressure, HbA1c, LDL, waist circumference, HRV measured by RMSSD. These variables showed the most significant and strongest correlation of all variables with work-related stress measured by ERI in the origin study justifying the inclusion to the index (Mauss et al., Citation2015a). For example, inflammatory markers such as white blood cells or CRP were not significantly associated with ERI in the origin study. All participants’ values were coded with respect to predefined subclinical cutoffs () based on our previous research and described elsewhere (Mauss et al., Citation2015a). Values exceeding the cutoff were scored as “1” (all variables except HRV, for which lower values indicate higher risk) while those falling within the normal range were scored as “0”. Values were summed to yield an ALI for all five biomarkers with a range of 0–5 and higher scores indicating higher allostatic load.
Statistical analyses
We present descriptive, univariate analysis using means, standard deviations and range where appropriate. To better approximate a normal distribution we applied a logarithmic transformation of HRV and waist circumference for further analyses. Bivariate correlations of all five ALI variables plus additional clinical variables with effort-reward imbalance (ERI >1) were tested using chi2 test for categorical variables and point-bi-serial correlations for continuous variables. Differences in ALI related to low (≤1) and high (>1) effort-reward ratio were tested with the Wilcoxon–Mann–Whitney test.
A logistic regression model tested the relationship of the 5-variable ALI (dependent variable) with ERI (independent variable), adjusting for age, gender, smoking and present diseases, such as arterial hypertension, diabetes mellitus and hypercholesterolemia.
All logistic regression models were adjusted for the nested structure of employees’ data (clustering within study site) using STATA vce (cluster) option. With this option, the standard errors are adjusted for intragroup correlation on the study site level, thus relaxing the usual requirement of the observations (employees) to be independent within groups (study sites). Hence, observations are assumed to be independent across groups (study sites) but not necessarily within groups. Additionally, adjusted models tested gender- and age-related differences of ALI and ERI. For all models allostatic sum scores were divided into two categories with the lower two tertiles as reference category and an upper tertile with values >3. We used Stata 12.1 MP (College Station, TX: StataCorp LP) for all the statistical analysis.
Results
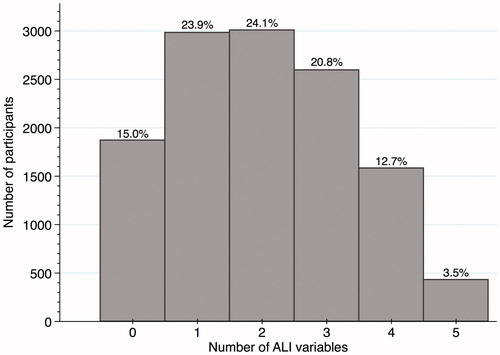
Mean value of the ALI including all five variables was 2.02 ± 1.37 (0–5). The distribution of ALI for all the participants is presented in .
Figure 1. Distribution of Allostatic Load Index (ALI) with absolute and relative frequencies (n = 12,477).
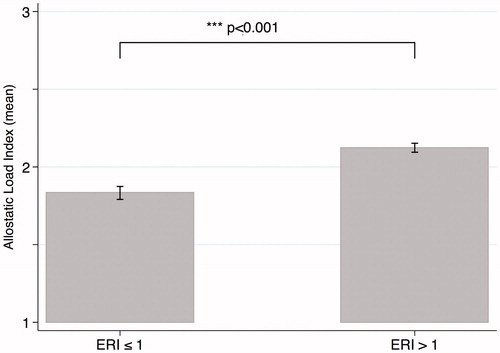
Participants perceiving work stress (n = 8302; 66.5%) had significant higher ALI scores (p = .001) than participants with lower effort-reward ratio (n = 4175; 33.5%) as shown in . This association did not differ between men and women. Men were more likely to report higher perceived stress levels compared to women (effort-reward ratio: men with 1.21 ± 0.46 vs. women with 1.17 ± 0.47, p < .01).
Figure 2. Scores of Allostatic Load Index in low (n = 4175) versus high (n = 8302) effort–reward imbalance (ERI) risk, differences calculated by Wilcoxon–Mann–Whitney test.
Bivariate comparisons of effort-reward imbalance with all 5 ALI variables showed highly significant correlations (p < .001) with coefficients between 0.06 and 0.10 (). Other clinical variables were tested and showed lower correlation coefficients such as systolic lower than diastolic blood pressure, HDL and triglycerides lower than LDL, BMI lower than waist circumference, FPG lower than HbA1c. White blood cells and CRP showed the weakest correlation of all variables with ERI. Additionally, age, gender, and smoking was correlated to work stress (p < .001; data not shown). Participants within the highest tertile of ALI had higher odds (OR 1.18 [95% CI: 1.03, 1.36]; p = .016) of perceived work stress (), compared with those in the lower two tertiles. Stratifying by gender, men showed a higher odds ratio compared to women for the association of ALI with work stress (OR 1.19 [95% CI: 1.03, 1.38]; p = .02 vs. OR 1.08 [95% CI: 0.85, 1.37]; p = .54). Stratified by age cluster, no significant association of ALI with ERI was explored.
Table 2. Bivariate correlation of multiple parameters with effort-reward ratio >1 (effort-reward imbalance), chi2 for categorical variables and point-bi-serial correlation for continuous variables.
Table 3. Logistic regression analysis, Allostatic Load Index (ALI) as dependent variable (defined as upper tertile), effort-reward imbalance (effort-reward ratio >1) as independent variable, adjusted for age, gender, smoking, and present diseases (arterial hypertension, diabetes mellitus, hypercholesterolemia), and ALI stratified by gender and age.
Discussion
Work-related stress was significantly associated with a short form of the Allostatic Load Index in a large sample of German industrial employees. This association was stronger in men than in women and was independent of age. The 5 variables used to calculate the index included diastolic blood pressure, glycosylated hemoglobin, low-density lipoprotein, waist circumference and heart rate variability.
For the purpose of replicability, a comparison of both study samples is useful, the present sample and the sample of the origin study (Mauss et al., Citation2015a). Both samples are based on working populations. Sociodemographic data such as age (41.0 ± 11.4; 15–64 years vs. 42.0 ± 10.9; 18–65 years) and gender (20.7% vs. 19.6% female) showed similar results as well as the proportion of employees perceiving work stress (64.9% vs. 66.5%). While the origin study explored employees of one engineering and manufacturing company, the replication study analyzed employees of four industries such as an automobile, a pharmaceutical, an electricity and an aeronautic company.
Our study has specific strengths. We present a replication of study results in a large sample of 12,477 German industrial employees. To our knowledge, an employee sample of that size has not been explored in ALI research before. The American National Health and Nutrition Examination Survey (NHANES) with comparable sample sizes included all ages of 17–90 years (Beckie, Citation2012). The largest sample size in a working context explored 3887 Polish men of the age of 25–60 years (Lipowicz et al., Citation2014). Therefore, we provide more evidence for the association of allostatic load and work-related stress measured by ERI. Further, we present a short tool to measure the biological wear and tear of employees including only five biomarkers.
In this replication study we could detect the same five variables showing the strongest correlation to work stress as in the origin study. Inflammatory variables such as white blood cells and CRP showed the lowest correlation with work stress giving justification that this pathway is not included in our 5-variable ALI. Previous attempts to build an ALI in working populations with seven (Johansson et al., Citation2007) or eight (Langelaanet al., Citation2007; Näswall et al., Citation2012) variables included no primary mediators. On the other hand, approaches in general populations with four or five variables included biomarkers covering different pathways, but these variables were expensive and difficult to assess such as cortisol, DHEA-S, epinephrine, and norepinephrine (Gersten, Citation2008), or d-dimer, tissue type plasminogen activator antigen, thrombin/antithrombin III complex, von Willebrand factor, and plasminogen activator inhibitor 1 antigen (Känel et al., Citation2003). In order to provide a set of variables that is accepted and used by occupational health practitioners it is essential to include a limited number of biomarkers covering neurophysiologic (e.g. heart rate variability), metabolic (e.g. waist circumference) and cardiovascular (e.g. glycosylated hemoglobin) pathways and that have strong predictive power for future disease events as described earlier. These variables should be easy and reliable to measure within a subclinical range. All that is the fact for biomarkers used in our study. Firstly, a lack of measurement standards for exact timing and thresholds as well as high costs (e.g. cortisol, epinephrine) and secondly, an ALI calculation based on the variable distribution within a sample contradict a daily use for occupational health practitioners. Taking this into account, especially HRV seems to be a cost-effective primary mediator. Based on our previous empirical data we predefined a threshold of 30 ms for all age groups, although age-related thresholds could still be discussed and should be a focus of further explorations.
We found age to be associated with work stress and allostatic load. The age-dependency of ALI has been described before due to the nature of included biomarkers. The NHANES study explored a constantly increasing allostatic load in people aged 20–60 years. Afterwards, the score remained the same up to the age of 90 (Crimmins et al., Citation2003). Juster depicted this as “window of opportunity” giving people a 40 years option for intervention and improvement of psychosocial strain and its health impact (Juster et al., Citation2010).
There seem to be gender-related differences in the association of work stress and ALI. Men in our sample showed higher stress levels and a stronger association with ALI as women. There are gender-based behavioral patterns due to divergent roles and genetic disparities, which have been described before in the context of psychosocial stressors with ALI (Juster et al., Citation2013).
Limitations
First, our results could have been biased by the fact that usually predominantly health-conscious people attend to screenings. Given a participation rate of 65% that effect should be very small but could have led us to an underestimation of possible associations. Nevertheless, participation rate was much higher than 37.8% in the origin study. Offering corporate health-promoting activities, a participation rate of more than 50% is usually perceived as very good. Second, our results cannot be fully generalized due to the recruitment of German, mainly male industrial employees. Nevertheless, some sort of generalizability is applicable due to the fact that at least employees of different industries participated. Third, our cross-sectional study design does not allow any causal conclusion about the direction of observed associations. Forth, we are very much aware, that our sample presented a high proportion of employees showing an effort-reward imbalance (>60%). That could have biased our findings. According to EUROSTAT data, over a period of nine years, 28% of European workers reported exposure to psychosocial risks that affected their mental well-being (Eurostat, Citation2010). As described by the European agency for health and safety at work (EU-OSHA), nearly 80% of European managers express work-related stress to be common in their workplace (Flintrop & Vargas, Citation2014).
Conclusion
Our results indicate that a short form of the Allostatic Load Index is associated with work stress in German industrial employees. This index composed of five variables seems successfully assessing employees at risk for biological wear and tear due to work-related stress. It could be used as an indicator for stress serving the corporate health management and should be validated in longitudinal study settings.
Acknowledgements
We are indebted to HealthVision Ltd., Berlingen Switzerland for providing the data as well as the Center for Neuropsychological Research (University of Trier) for providing HRV-data computations.
Disclosure statement
The authors of this study report no relevant conflict of interest with the subject matter or materials discussed in the manuscript. Until December 2012, Prof Fischer was the major shareholder of Health Vision Ltd, the company that organized the data collection. All authors are responsible for the content and writing of the paper. No writing assistance was utilized in the production of this manuscript.
References
- Backé E, Seidler A, Latza U, Rossnagel K, Schumann B. (2012). The role of psychosocial stress at work for the development of cardiovascular diseases: a systematic review. Int Arch Occup Environ Health 85(1):67–79.
- Beckie TM. (2012). A systematic review of allostatic load, health, and health disparities. Biol Res Nurs 14(4):311–46.
- Crimmins EM, Johnston M, Hayward M, Seeman T. (2003). Age differences in allostatic load: an index of physiological dysregulation. Exp Gerontol 38(7):731–4.
- Eurostat. (2010). Health and safety at work in Europe (1999–2007), A statistical portrait. Luxembourg: Publication Office ot the European Union. p 74.
- Ferguson CJ, Heene M. (2012). A vast graveyard of undead theories: publication bias and psychological science's aversion to the null. Perspect Psychol Sci 7(6):555–61.
- Flintrop J, Vargas O. (2014). Psychosocial risks in Europe, Prevalence and strategies for prevention A joint report from the European Foundation for the improvement of Living and Working Conditions and the European Agency for Safety and Health at Work. Luxembourg: Publications Office of the European Union. p 6.
- Gelman A, Carlin J. (2014). Beyond power calculations: assessing type S (Sign) and type M (Magnitude) errors. Perspect Psychol Sci 9(6):641–51.
- Gersten O. (2008). Neuroendocrine biomarkers, social relations, and the cumulative costs of stress in Taiwan. Soc Sci Med 66(3):507–19.
- Goldman N, Turra CM, Glei DA, Seplaki CL, Lin Y, Weinstein M. (2006). Predicting mortality from clinical and nonclinical biomarkers. J Gerontol A Biol Sci Med Sci 61(10):1070–4.
- Johansson G, Huang Q, Lindfors P. (2007). A life-span perspective on women's careers, health, and well-being. Soc Sci Med 65(4):685–97.
- Juster R, McEwen BS, Lupien SJ. (2010). Allostatic load biomarkers of chronic stress and impact on health and cognition. Neurosci Biobehav Rev 35(1):2–16.
- Juster R, Moskowitz DS, Lavoie J, D'Antono B. (2013). Sex-specific interaction effects of age, occupational status, and workplace stress on psychiatric symptoms and allostatic load among healthy Montreal workers. Stress 16(6):616–29.
- Känel R. v, Dimsdale JE, Patterson TL, Grant I. (2003). Acute procoagulant stress response as a dynamic measure of allostatic load in Alzheimer caregivers. Ann Behav Med 26(1):42–8.
- Karlamangla AS, Singer BH, McEwen BS, Rowe JW, Seeman TE. (2002). Allostatic load as a predictor of functional decline. MacArthur studies of successful aging. J Clin Epidemiol 55(7):696–710.
- Langelaan S, Bakker AB, Schaufeli WB, van Rhenen W, van Doornen LJ. (2007). Is burnout related to allostatic load? Int J Behav Med 14(4):213–21.
- Li J, Loerbroks A, Jarczok MN, Schöllgen I, Bosch JA, Mauss D, Siegrist J, Fischer JE. (2012). Psychometric properties and differential explanation of a short measure of effort-reward imbalance at work: a study of industrial workers in Germany. Am J Ind Med 55(9):808–15.
- Lipowicz A, Szklarska A, Malina RM. (2014). Allostatic load and socioeconomic status in Polish adult men. J Biosoc Sci 46(2):155–67.
- Lundberg U. (2015). Work conditions and back pain problems. Stress Health 31:1–4.
- Malik M, Bigger JT, Camm AJ, Kleiger RE, Malliani A, Moss AJ, Schwartz PJ. (1996). Heart rate variability: standards of measurement, physiological interpretation, and clinical use. European Heart Journal 17:354–81.
- Mauss D, Jarczok MN, Fischer JE. (2015a). A streamlined approach for assessing the Allostatic Load Index in industrial employees. Stress 18(4):475–83.
- Mauss D, Li J, Schmidt B, Angerer P, Jarczok MN. (2015b). Measuring allostatic load in the workforce: a systematic review. Indus Health 53(1):5–20.
- McEwen BS. (2003). Mood disorders and allostatic load. Biol Psychiatry 54(3):200–7.
- McEwen BS, Stellar E. (1993). Stress and the individual. Mechanisms leading to disease. Arch Intern Med 153(18):2093–101.
- Näswall K, Lindfors P, Sverke M. (2012). Job insecurity as a predictor of physiological indicators of health in healthy working women: an extension of previous research. Stress Health 28(3):255–63.
- Ruotsalainen JH, Verbeek JH, Marine A, Serra C. (2015). Preventing occupational stress in healthcare workers. Cochrane Database Syst Rev 4: CD002892.
- Sabbah W, Watt RG, Sheiham A, Tsakos G. (2008). Effects of allostatic load on the social gradient in ischaemic heart disease and periodontal disease: evidence from the Third National Health and Nutrition Examination Survey. J Epidemiol Community Health 62(5):415–20.
- Seeman TE, Singer BH, Rowe JW, Horwitz RI, McEwen BS. (1997). Price of adaptation-allostatic load and its health consequences. MacArthur studies of successful aging. Arch Intern Med 157(19): 2259–68.
- Siegrist J. (1996). Adverse health effects of high-effort/low-reward conditions. J Occup Health Psychol 1(1):27–41.
- Siegrist J, Starke D, Chandola T, Godin I, Marmot M, Niedhammer I, Peter R. (2004). The measurement of effort-reward imbalance at work: European comparisons. Soc Sci Med 58(8):1483–99.
- Theorell T, Hammarstrom A, Aronsson G, Traskman Bendz L, Grape T, Hogstedt C, Marteinsdottir I, et al. (2015). A systematic review including meta-analysis of work environment and depressive symptoms. BMC Public Health 15:738.