
Abstract
Cognitive impairment has frequently been shown in patients who seek medical care for stress-related mental health problems. This study aims to extend the current knowledge of cognitive impairments in these patients by focusing on perceived fatigue and effects of distraction during cognitive testing. Executive function and attention were tested in a group of patients with stress-related exhaustion (n = 25) and compared with healthy controls (n = 25). Perceived fatigue was measured before, during and after the test session, and some of the tests were administered with and without standardized auditory distraction. Executive function and complex attention performance were poorer among the patients compared to controls. Interestingly, their performance was not significantly affected by auditory distraction but, in contrast to the controls, they reported a clear-cut increase in mental tiredness, during and after the test session. Thus, patients with stress-related exhaustion manage to perform during distraction but this was achieved at a great cost. These findings are discussed in terms of a possible tendency to adopt a high-effort approach despite cognitive impairments and the likelihood that such an approach will require increased levels of effort, which can result in increased fatigue. We tentatively conclude that increased fatigue during cognitive tasks is a challenge for patients with stress-related exhaustion and plausibly of major importance when returning to work demanding high cognitive performance.
Introduction
Patients seeking care for stress-related mental health problems often report cognitive dysfunction as a main problem. The relationship between burnout and cognition has been addressed in previous research and several studies suggest a connection with cognitive deficits (Eskildsen, Andersen, Degn Pedersen, Kjaer Vandborg, & Hviid Andersen, Citation2015; Jonsdottir et al., Citation2013; Öhman, Nordin, Bergdahl, Slunga Birgander, & Stigsdotter Neely, Citation2007; Oosterholt, van der Linden, Maes, Verbraak, & Kompier, Citation2012; Rydmark et al., Citation2006; Sandström, Nyström Rhodin, Lundberg, Olsson, & Nyberg, Citation2005; Van Dam, Keijsers, Eling, & Becker, Citation2011; Van der Linden, Keijsers, Eling, & van Schaijk, Citation2005). In particular, inferior performances have been demonstrated for executive functions, attention, and memory (Deligkaris, Panagopoulou, Montgomery, & Masoura, Citation2014). Here, we extend the current knowledge of cognitive problems in patients with stress-related mental health problems, by studying the fatigue related to performing cognitive tasks and the effects of including concurrent disturbing stimuli during testing.
Many patients seeking medical care for stress-related exhaustion are highly educated and thus most probably holding positions that are cognitive demanding (Glise, Ahlborg, & Jonsdottir, Citation2012). The cost of performing cognitive demanding tasks is thus an important issue and plausibly a major challenge for these individuals (Oosterholt, Maes, van der Linden, Verbraak, & Kompier, Citation2014).
Increased sensitivity to disturbing sounds could constitute a problem during stress exposure and exhaustion (Hasson, Theorell, Bergquist, & Canlon, Citation2013; Horner, Citation2003). In clinical practice, the patients often describe it as difficult to concentrate when exposed to disturbing auditory stimuli. Background sounds, such as overhearing people talking are thought to be particularly bothersome. To our knowledge, the present study is the first to include concurrent disturbing human voices during the performance of demanding cognitive tasks.
The primary aims of this study were to explore perceived fatigue and the effects of distraction when performing executive and complex attentional tasks. The main hypothesis is that patients with stress-related exhaustion will report higher levels of fatigue during cognitive test session compared to healthy controls. We also hypothesize that the patients in comparison with controls will be more affected by auditory distractions during their test performance.
Method
Participants
This study consists of 50 participants (25 patients and 25 healthy controls). All patients fulfilled the criteria for Exhaustion disorder (ED) (). These criteria were established by the Swedish National Board of Health and Welfare in 2005 and assigned the F43.8A code of the International Classification of Diseases and Related Health Problems (ICD-10; World Health Organization, Citation1992).
Table 1. Diagnostic criteria for exhaustion disorder according to the National Board of Health and Welfare.
Burnout and ED seem to be closely related in terms of symptoms and it has been shown that most patients who meet the diagnostic criteria for ED also can be defined as burned out (Glise et al., Citation2012; Jonsdottir, Hägg, Glise, & Ekman, Citation2009). One major difference between ED and burnout is that ED is defined by clinical criteria whereas burnout is a psychological construct based on self-reports using different rating scales. The clinical manifestation of patients with stress-related exhaustion is comprehensively reviewed in a recent paper by Grossi, Perski, Osika, and Savic (Citation2015).
The patients in this study were referred to an outpatient stress clinic in the Region Västra Götaland, Sweden, from primary care units or occupational health care centers. The referral criteria were (1) “probable ED” with no apparent somatic disorder or abuse that could explain the exhaustion and (2) a maximum duration of sick leave of 6 months. Consecutive inclusion was applied, i.e. all patients who entered the stress clinic (during August 2010 to January 2011) and eligible to participate in this study were asked to participate, until the intended number of patients was reached. Of the eligible patients, eight were not included in the final sample: one moved to another part of the country, one did not respond to our calls, and six declined participation. The patients not included (n = 8) did not differ from the patients included (n = 25) with regard to level of burnout, depression, and anxiety (data not shown). The diagnostic procedure was conducted by a senior physician at the stress clinic, based on an extended anamnesis and a clinical examination. Co-morbid depression and/or anxiety were allowed, but patients with recurrent depression were not included in this study. Antidepressants were used by 46% of the patients at the time of the study. One patient came from another clinic and data concerning antidepressants and self-reported symptoms of depression and anxiety was missing for this patient.
Twenty-five healthy controls were recruited from three different sources, mainly from an ongoing longitudinal cohort study predominantly including health care workers. Several controls were also recruited from a private company in Gothenburg or among students at the University of Gothenburg in order to recruit controls that matched the patient group. These participants were offered financial compensation for participating. A first screening of eligibility was made by telephone, based on age, level of education, and the exclusion criteria. The exclusion criteria were (1) neurological disease that could affect neuropsychological outcome, (2) current somatic disease causing fatigue, (3) previous or ongoing ED, and (4) anxiety and/or depressive symptoms during the last six months requiring health care. Three individuals were excluded based on these criteria; one met the first and two met the third criterion. One person was not able to visit the clinic during the study period and thus did not participate in the study. At the beginning of the test session, the eligibility was further investigated, using a standardized questionnaire, and another four controls were then excluded; three were found to meet the third exclusion criterion and one met the fourth. The control group was matched to the ED-group by age and sex, and a maximum level of years of education was set for the controls, corresponding with the maximum level observed in the patient group. The study was conducted in accordance with the Declaration of Helsinki and approved by the regional ethical review board in Gothenburg, Sweden. All subjects gave written informed consent to participate in the study.
Measurements
Self-reported burnout and symptoms of depression and anxiety
Self-reported burnout was measured with the Shirom-Melamed Burnout Questionnaire (SMBQ). The questionnaire includes 22 items (graded 1–7) measuring different aspects of burnout syndrome (Lundgren-Nilsson, Jonsdottir, Pallant, & Ahlborg, Citation2012; Melamed, Kushnir, & Shirom, Citation1992). A mean score >4.4 has previously been used as cutoff for clinical burnout (Lundgren-Nilsson et al., Citation2012). Stenlund et al. (Citation2007) reported the mean score of the total scale in patients with burnout to be 5.7 for women and 5.6 for men. Cronbach’s alpha for the SMBQ burnout total score was 0.82. Symptoms of anxiety and depression were measured with the Hospital Anxiety and Depression Scale (HADS), defined as scores ≥8 on anxiety and/or depression (Zigmond & Snaith, Citation1983). Cronbach’s alpha for HADS was 0.84 for anxiety and 0.57 for depression.
Self-reported fatigue and cognitive function
Level of fatigue was measured with the Swedish version of the Fatigue Impact Scale (FIS; Flensner, Ek, & Söderhamn, Citation2005). The FIS consists of 40 items describing how fatigue affects daily life situations. Participants rate the impact and consequences of fatigue in these situations on a five-level scale, ranging from no problem (0) to extreme problem (4). Total range in score is 0–160.
Subjective cognitive function was assessed with a Swedish version of the Prospective and Retrospective Memory Questionnaire (PRMQ; Rönnlund, Mäntylä, & Nilsson, Citation2008) and with the Cognitive Failures Questionnaire (CFQ; Broadbent, Cooper, FitzGerald, & Parkes, Citation1982). The PRMQ consists of 16 items measuring the frequency of memory failures. Answers are given on a five-point Likert-type scale, ranging from never (1) to very often (5). Total range is 16–80. The CFQ consists of 25 items measuring the frequency of cognitive failures in daily life. A five-point Likert-type scale is used for answering, ranging from never (0) to very often (4). Total range is 0–100.
Estimate of general cognitive ability
In order to estimate the general cognitive level, a Swedish version of the National Adult Reading Test (NART; Tallberg, Wenneborg, & Almkvist, Citation2006) was used, measuring the ability to pronounce irregularly spelled words (ISW). This ability relies on implicit memory processes and is thought to be stable during normal aging and after brain damage or disease, and it is positively related to general cognitive level. Tallberg et al. (Citation2006) have shown that the ISW-score in combination with gender and years of education in a regression-based formula improves the estimate of general cognitive ability. This regression model was used in the present study in order to compute predicted WAIS-full scale IQ-score.
Neuropsychological tests
Executive functions
Verbal fluency in a divided attention condition
A modified version of the Controlled Word Association Test (COWAT) was used. COWAT is a test of verbal fluency, where the participants are asked to generate as many words as possible beginning with the letters F, A, and S (Lezak, Howieson, Bigler, & Tranel, Citation2012). The time available for this task is one minute for each letter. The COWAT was modified in that a card-sorting task was administered simultaneously with the main task. For each generated word, the participants were to pick a playing card from a deck of cards and then sort it according to the principle even/uneven into two different piles (the jacks, queens, and kings were removed from the deck, and the aces could correspond to either 1 or 14). This modification was adapted from Öhman et al. (Citation2007). The score obtained in this test was total number of generated words.
Working memory
The 2-back condition subtest from the Test of Attentional Performance Version 2.1 (TAP; Zimmermann & Fimm, Citation2007) was used. A sequence of single digit numbers is presented at the center of a monitor. The digits are presented one by one at three-second intervals. The participants are required to respond when the current digit is the same as the one shown two steps back. The test contains 15 target stimuli and the duration is five minutes. The task is considered a test of working memory and a high degree of attentional control is also required in the test. The number of omissions is the most important parameter of performance, since it is related to lack of control in the flow of information. The number of errors may also indicate lapses of attention. The numbers of omissions and errors were selected for analysis in this study.
Complex attention
A modified version of the Paced Visual Serial Addition Test (PVSAT) was used in this study. PVSAT (Fos, Greve, South, Mathias, & Benefield, Citation2000) is an analog of the Paced Auditory Serial Addition Test (PASAT). In these tests of complex attention, working memory and information processing speed, the participants are presented with a sequence of numbers and asked to add each number to the one immediately preceding it, and to say the answer out loud. In the PVSAT specifically designed for this study, the numbers were presented one by one in the center of a 15 inch PC-laptop screen. The font was Times New Roman with font size 96. Each number was presented for 2 s, and was then immediately replaced by the subsequent number. A series of 61 numbers were presented, which gives a possible maximum score of 60 correct additions.
Standardized distraction (2-back and PVSAT)
Both the 2-back test and the PVSAT were administered twice, the second time a CD-recording with a female and a male voice was played simultaneously with the test administration. The voices read out different numbers (0–9), and the reading of numbers was intermittently interrupted by “Hello!”, “You!”, and “Hello you!” Numbers were chosen because of the potential interference with the main task. The readings were varied by using low and high voices and different intervals. The numbers were read from a standardized protocol and recorded. There was one reading for the 2-back and one for the PVSAT, and the same standardized recordings were used for all test administrations. Before patients and controls were tested, the sound level was tested in the different test rooms, and no differences were found. When the second administration of the 2-back test had been in progress for one minute, the disturbing sound was gradually introduced and then lasted for the remainder of the test. The disturbing noise was started at the same time as the main task in the administration of the PVSAT. A difference score was given for the scores with and without distraction (subtracting one score from the other). The difference scores were computed so that a negative score always meant an inferior performance during distraction.
Basic attention
The three measures of hit reaction time, commission errors, and omissions from the Conners Continuous Performance Test II (CPT-II; Conners, Citation2004) were used for investigating aspects of basic attention. The CPT-II lasts for 14 minutes and measures different components of attention. The participants are required to respond to letters appearing on the monitor, except for the letter “x”. The inter-stimulus intervals are 1, 2, or 4 seconds. The display time is 250 milliseconds. The variable hit reaction time (the mean response time for all target responses) measures general processing speed. The variable commissions measure basic selective attention and inhibition and the variable omissions measure attention.
Sustained attention/performance
The CPT-II also includes measures of the consistency of performance over time. The results from the test (as described above) can be partitioned into six equal blocks and the performance can thus be examined by block, which enables assessment of change over time in the individual responses. The following three measures were included for describing different aspects of variability across time/block: (1) variability of standard error, a measure of “within respondent” variability – the degree of variation in response speed between the different blocks throughout the test, (2) hit reaction time by block, which measures change in reaction time at the initial blocks compared to the final blocks, and (3) standard error by block, a measure of changes in response variability when comparing initial blocks with final blocks.
Mental tiredness during and after the test administration
A self-rating scale of fatigue was specifically designed for this study, measuring the participants’ perceived mental weariness before, during (i.e. in the middle of), and after the testing session. The participants were asked to rate their mental tiredness on a scale consisting of the following seven levels: “No tiredness”, “Mild”, “Moderate”, “Average”, “Severe”, “Very severe”, and “Worst thinkable tiredness”. The scale did not contain numbers, and all the three ratings (before, during, and after) were on the same paper; thus the participants could see their previous ratings. For statistical analyses, the ratings were given numerical values ranging from 1 (“No tiredness”) to 7 (“Worst thinkable tiredness”).
Procedure
Each participant was tested on one occasion by the same psychologist. The administration of the computerized tests included an introductory practice run. The sessions lasted for 1.5–2 hours, including a short break and feedback. Prior to the testing session, the questionnaires FIS, PRMQ, and CFQ were sent to the participants by post, completed at home and brought to the testing session. General cognitive ability was investigated before the testing of executive and attentional functions. The tests and self-ratings of mental tiredness were administered in the following standardized sequence: an initial self-rating of tiredness, modified COWAT, 2-back test, 2-back test with distraction, the second self-rating of tiredness, a short break, CPT-II, PVSAT, PVSAT with distraction, the third self-rating of tiredness. The test session also comprised a test of prospective memory but this measurement was not included in this study.
Statistical analysis
Non-parametric statistics were used due to the small size of the groups and skewed distributions. Between-group comparisons were made with Mann–Whitney’s U-test, and for categorical data Pearson’s Chi-square and Fisher’s exact test were used. Holm–Bonferroni’s correction for multiple comparisons (1979) was used for the analyses of the effects of distraction and of experienced tiredness during testing to counteract the probability of a Type I error. Correction was also made for post hoc subgroup comparison of commission errors in CPT-II. No correction was applied for demographic background data. Effect sizes were given as η2 based on the Chi-square from nonparametric two-sample comparisons, using the formula: Chi-square/N – 1 (Green & Salkind, Citation2008). The interpretations were: 0.01 = small effect, 0.06 = moderate effect, and 0.14 = large effect (Cohen, Citation1988). In all analysis, p < .05 was considered statistically significant. Estimates of population means were made by 95% confidence intervals (CI); bias-corrected bootstrap CI with 5000 resamples were used in order to obtain more robust and accurate estimates. No CI was given for variables with few levels and a narrow interval of the observed scores.
One subject in the ED-group found the 2-back test too difficult, and did not complete the task – neither the standard condition nor the condition with distraction. For the same reasons, another subject in the ED-group did not do the condition with distraction. For data analysis of these two tasks, values of one point below the lowest recorded performance in the ED-group were used (i.e. one error more and one omission more). The patient that found the two tasks difficult also found the PVSAT administration with the distraction-condition too difficult, and did not complete the task. For this subject, a value of one point below the lowest recorded performance in the ED-group was used (i.e. one less correct answer).
Results
Demographics and self-report outcome
The mean score of SMBQ was 5.9 (range 4.7–6.7) for the ED group. Thus, all the patients scored above the cutoff for clinical burnout previously defined by the research group (cutoff >4.4; Lundgren-Nilsson et al., Citation2012). Ninety-two percent of the patients had co-morbid anxiety and/or depression. Patients and controls did not differ with regard to sex, age, or estimate of general cognitive ability (). On the other hand, a significant difference was seen between patients and controls on all the ratings of fatigue and subjective cognitive functioning (p < .001, η2 between 0.52 and 0.75), in that the patients felt more fatigued (FIS) and reported more cognitive problems (PRMQ and CFQ; ).
Table 2. Demographics, general cognitive level, SMBQ, and HADS for patients and controls.
Table 3. Ratings of fatigue and subjective cognitive functioning in patients (n = 25) and controls (n = 25).
Neuropsychological results
Executive functions
There was a significant difference in test performance between groups for the modified COWAT task that measured verbal fluency in a divided attention condition (); the controls generated more words than the patients. In the 2-back working memory test, the patient group showed significantly more omissions than the control group, but no differences for number of errors. This pattern was observed both with and without distraction. For complex attention (PVSAT), no significant difference between groups was seen in the condition without distraction, but with distraction there was a significant difference, in that the control group made more correct additions. For the difference scores that described differences in performance with and without distraction (see ), no significant group differences were obtained for any of the measures (errors and omissions in working memory and correct additions in PVSAT).
Table 4. Neuropsychological test results of executive function and complex attention in patients (n = 25) and controls (n = 25).
Basic attention
The basic attentional performance was described by three measurements of the overall performance in the CPT-II; the mean reaction time, total number of commissions, and total number of omissions. No significant differences between groups were obtained for any of these three measurements ().
Table 5. Neuropsychological test results of basic and sustained attention in the CPT-II in patients (n = 25) and controls (n = 25).
Sustained attention/performance
The potential variability in attentional performance over time (over test blocks) was investigated by three measurements included in the CPT-II. Significant group differences were observed for measurements of the variability of standard error and hit reaction time by block (). These results illustrate that patients showed a higher variation throughout the test in the variability of the response speed than controls and that the change in reaction time (initial blocks vs final blocks) was greater for patients compared to controls.
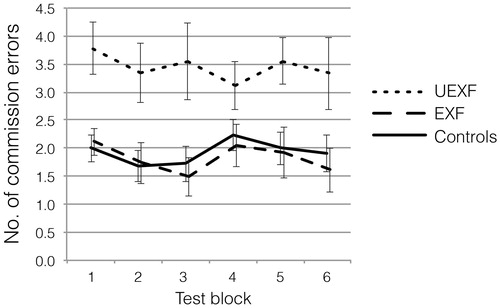
Since a different response pattern by test blocks was indicated for the patients relative to controls, we further explored performance over time. A plot of the hit reaction times of the six consecutive blocks of the CPT-II revealed that the ED group had faster responses at the beginning of the test compared to controls (). In order to investigate the tentative effect of an unexpectedly fast (UEXF) start in the test, the ED group was divided into two subgroups according to the response speed in the first block. One group (n = 9) was classified as UEXF, defined as a response time ≤ the 16th percentile of the control group (a response at least 1 SD faster than the controls). The other group (n = 16) was classified as expected fast (EXF) (a response time > the 16th percentile of the controls). When commissions and omissions in the test were compared between these subgroups, the UEXF group had more commission errors () during the test (Mann–Whitney: z=−2.809, p = .01). No difference was observed for omissions (data not shown).
Figure 1. Mean response time (in milliseconds) with ± SEM for targets in the six consecutive blocks of the CPT-II test for the ED group (n = 25) and controls (n = 25).
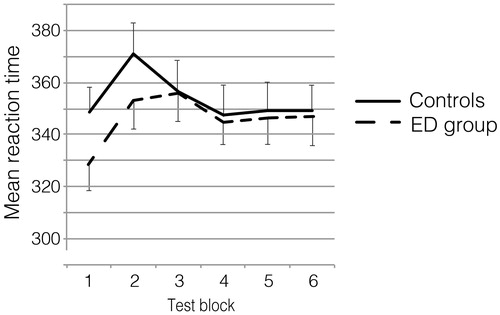
Figure 2. Average number of commission errors (with ± SEM) across six test blocks of the CPT-II test for patients with stress-related exhaustion (Exhaustion Disorder (ED)) and controls (n = 25). The ED group is divided into patients with an unexpected fast response speed at the beginning of the test (UEXF; n = 9) and those with expected fast response speed in the first block (EXF; n = 16). The UEXF-group had more commission errors during the test compared to the other groups.
Mental tiredness during and after the test administration
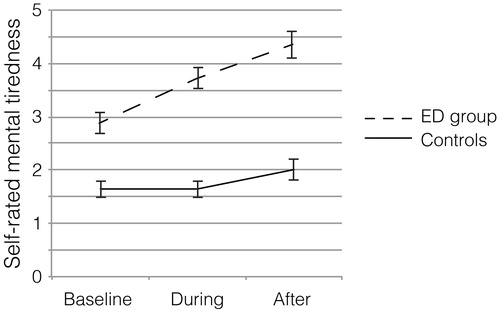
The group difference in experience of tiredness during and after testing was analyzed in terms of change (a change score) from baseline to each measurement point (during and after testing). In contrast to the controls, the patients reported an increase in mental tiredness during the testing with significant group differences in the change score of tiredness; baseline-during testing (Mann–Whitney, z = −3.22, p < .005, η2 = 0.21; M (SD), patients 0.8 (0.9), controls 0.0 (0.9)) and baseline-after testing (z = −3.02, p < .005, η2 = 0.19; M (SD), patients 1.5 (1.2), controls 0.4 (1.2)). These group differences in self-reported tiredness are illustrated in . An additional post hoc analysis between the two subgroups UEXF and EXF described above was made. Ratings of tiredness after testing were categorized as either “low fatigue score” (ratings ≤ average tiredness; n = 13) or “high fatigue score” (ratings > average tiredness; n = 12), and it was found that the UEXF group was more tired compared to the EXF group (Fisher’s exact test, p = .041).
Figure 3. Mean mental tiredness (with ± SEM) reported by patients with stress-related exhaustion (Exhaustion disorder (ED)) (n = 25) and controls (n = 25) before, during and after the administration of the neuropsychological tests. The scale is graded as; 1 = No tiredness, 2 = Mild, 3 = Moderate, 4 = Average, 5 = Severe, and 6 = Very severe. None of the participants rated 7 = Worst thinkable tiredness.
Discussion
The main finding of the study is that individuals with stress-related exhaustion report increased mental tiredness during and after neuropsychological test session. The other main finding is that distraction does not affect cognitive performance which is contrary to our hypothesis. Thus, similar levels of performance in working memory and complex attention were observed with and without distraction. However, the clear-cut observation of increased tiredness concomitantly with unaffected performance during distraction indicates that patients suffering from stress-related exhaustion manage to perform with cognitive load during a restricted period, but such a high level of performance comes at a great cost. This novel finding raises several important questions related to cognitive demands in patients with stress-related mental health problems. One important issue is the seemingly poor adaptation to available mental resources. Van Dam, Keijsers, Eling, and Becker (Citation2015) found that neither perception of fatigue nor a strategic low-effort approach to demanding tasks could explain the level of performance in individuals with burnout. Instead, they observed a typical tendency to adopt a high-effort approach despite cognitive impairments. They proposed that the strive to maintain acceptable or high performance levels despite impairments require increased levels of effort, which result in increased fatigue. The results of our study seem to be in line with this proposal and it is also in line with the clinical experience of the patients, i.e. that individuals with stress-related exhaustion often struggle with a high-effort approach. Our results implicate that perspectives such as behavioral patterns and ability to adjust is as important to consider as the cognitive impairment itself. This is particularly important for individuals returning to work with high cognitive demands. Response style and ability to adjust to available resources may also be related to an increased vulnerability to developing symptoms of exhaustion. This is important since extended studies of preventive measures are needed. Another interesting aspect of our results is offering a plausible explanation why some patients may exhibit marked subjective cognitive complaints in spite of relatively fair results on objective tests. The explanation may be that individuals who adapt to a high-effort approach despite cognitive impairments may manage to maintain acceptable levels of performance but will perceive cognitive problems due to the effort of performing the task. Of particular interest is the somewhat unexpected behavioral pattern of faster response among the patients at the beginning of the task and greater inconsistency in the responses throughout the test. These unexpected rapid responses at the start of the test were also associated with a higher error rate across the entire test. This is interesting because normally a gradual adjustment of performance over time is seen for this type of continuous task in trying to obtain a balance between speed and accuracy (Conners, Citation2004). The current subgroup, with an unexpected fast start, did not reach such an adjustment – they began the task with a high response speed and were unable to find an optimal adjustment as they continued to demonstrate a high level of error. Also, this subgroup experienced the highest level of fatigue after the test session.
In the present study, age, sex, and general cognitive level were well balanced between patients and controls. Even though anxiety and/or depressive symptoms during the last six months requiring health care were exclusion criteria for controls, the lack of measure of symptoms of depression for this group is a limitation. Further, a majority of the patients had symptoms of anxiety and depression, and many had antidepressant medication. In other studies, depression was excluded even in the burnout group. However, our intention was to investigate cognition and fatigue in patients with exhaustion/clinical burnout in a clinical setting, where depressive symptoms are common. This implicates the possibility of the results being influenced by depression but at the same time reflects the actual situation for these patients as they usually have depression. Previous studies show that level of depression does not seem to explain the cognitive impairment in patients with ED (Jonsdottir et al., Citation2013). The findings described in this study were based on small samples and larger studies are needed.
We can cautiously conclude that increased fatigue during cognitively demanding tasks is a challenge for patients with stress-related exhaustion and plausibly a major obstacle when returning to work situations that encompass high cognitive demands. Many patients with stress-related exhaustion seem to strive to perform at high cost and show a poor ability to adapt to the situation. These behavioral patterns are important to pay attention to during rehabilitation in order to ensure sustainable return to work.
Acknowledgements
The authors thank all the patients and controls for participating in this study. The authors also thank Sandra Pettersson, Agneta Lindegård Andersson, and Emina Hadzibajramovic for valuable help with administration and statistics. Special thanks also go to Jerry Larsson, Thorleif Thorlin, and Patrik Säterö for their support and advice in the initial stages of this study. This study was funded by grants from The Healthcare Sub-Committee, Region Västra Götaland (Hälso-och sjukvårdsutskottet), The Anna Ahrenberg Foundation for Scientific and other Purposes, The Local Research and Development Council, Göteborg and Södra Bohuslän, and Wilhelm and Martina Lundgren Foundation.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Broadbent, D.E., Cooper, P.F., FitzGerald, P., & Parkes, K.R. (1982). The Cognitive Failures Questionnaire (CFQ) and its correlates. British Journal of Clinical Psychology, 21, 1–16. doi: 10.1111/j.2044-8260.1982.tb01421.x
- Cohen, J. (1988). Statistical power analysis for the behavioural sciences (2nd ed.). Hillsdale, NJ: LEA.
- Conners, C.K. (2004). Conners’ Continuous Performance Test II for Windows, technical guide and software manual. Toronto: Multi-Health Systems Inc.
- Deligkaris, P., Panagopoulou, E., Montgomery, A.J., & Masoura, E. (2014). Job burnout and cognitive functioning: A systematic review. Work and Stress, 28, 107–123. doi: 10.1080/02678373.2014.909545
- Eskildsen, A., Andersen, L.P., Degn Pedersen, A., Kjaer Vandborg, S., & Hviid Andersen, J. (2015). Work-related stress is associated with impaired neuropsychological test performance: A clinical cross-sectional study. Stress, 18, 198–207. doi: 10.3109/10253890.2015.1004629
- Flensner, G., Ek, A.C., & Söderhamn, O. (2005). Reliability and validity of the Swedish version of the Fatigue Impact Scale (FIS). Scandinavian Journal of Occupational Therapy, 12, 170–180. doi: 10.1080/11038120510031806
- Fos, L.A., Greve, K.W., South, M.B., Mathias, C., & Benefield, H. (2000). Paced Visual Serial Addition Test: An alternative measure of information processing speed. Applied Neuropsychology, 7, 140–146. doi: 10.1207/S15324826AN0703_4
- Glise, K., Ahlborg, G., Jr., & Jonsdottir, I.H. (2012). Course of mental symptoms in patients with stress-related exhaustion: Does sex or age make a difference? BMC Psychiatry, 12, 18. doi: 10.1186/1471-244X-12-18
- Green, S.B., & Salkind, N.J. (2008). Using SPSS for Windows and MacIntosh: Analyzing and understanding data (5th ed.). Upper Saddle River, NJ: Pearson Prentice Hall.
- Grossi, G., Perski, A., Osika, W., & Savic, I. (2015). Stress-related exhaustion disorder – Clinical manifestation of burnout? A review of assessment methods, sleep impairments, cognitive disturbances, and neuro-biological and physiological changes in clinical burnout. Scandinavian Journal of Psychology, 56, 626–636. doi: 10.1111/sjop.12251
- Hasson, D., Theorell, T., Bergquist, J., & Canlon, B. (2013). Acute stress induces hyperacusis in women with high levels of emotional exhaustion. PLoS One, 8, e52945. doi: 10.1371/journal.pone.0052945
- Holm, S. (1979). A simple sequentially rejective multiple test procedure. Scandinavian Journal of Statistics, 6, 65–70. doi: 10.2307/4615733
- Horner, K.C. (2003). The emotional ear in stress. Neuroscience and Biobehavioral Reviews, 27, 437–446. doi: 10.1016/s0149-7634(03)00071-x
- Jonsdottir, I.H., Hägg, D.A., Glise, K., & Ekman, R. (2009). Monocyte chemotactic protein-1 (MCP-1) and growth factors called into question as markers of prolonged psychosocial stress. PLoS One, 4, e7659. doi: 10.1371/journal.pone.0007659
- Jonsdottir, I.H., Nordlund, A., Ellbin, S., Ljung, T., Glise, K., Währborg, P., & Wallin, A. (2013). Cognitive impairment in patients with stress-related exhaustion. Stress (Amsterdam, Netherlands), 16, 181–190. doi: 10.3109/10253890.2012.708950
- Lezak, M.D., Howieson, D.B., Bigler, E.D., & Tranel, D. (2012). Neuropsychological assessment (5th ed.). New York: Oxford University Press.
- Lundgren-Nilsson, Å., Jonsdottir, I.H., Pallant, J., & Ahlborg, G. Jr. (2012). Internal construct validity of the Shirom-Melamed Burnout Questionnaire (SMBQ). BMC Public Health, 12, 1. doi: 10.1186/1471-2458-12-1
- Melamed, S., Kushnir, T., & Shirom, A. (1992). Burnout and risk factors for cardiovascular diseases. Behavioral Medicine (Washington, D.C.), 18, 53–60. doi: 10.1080/08964289.1992.9935172
- Öhman, L., Nordin, S., Bergdahl, J., Slunga Birgander, L., & Stigsdotter Neely, A. (2007). Cognitive function in outpatients with perceived chronic stress. Scandinavian Journal of Work, Environment & Health, 33, 223–232. doi: 10.5271/sjweh.1131
- Oosterholt, B., Maes, J., Van der Linden, D., Verbraak, M., & Kompier, M. (2014). Cognitive performance in both clinical and non-clinical burnout. Stress (Amsterdam, Netherlands), 17, 400–409. doi: 10.3109/10253890.2014.949668
- Oosterholt, B., Van der Linden, D., Maes, J., Verbraak, M., & Kompier, M. (2012). Burned out cognition – Cognitive functioning of burnout patients before and after a period with psychological treatment. Scandinavian Journal of Work, Environment & Health, 38, 358–369. doi: 10.5271/sjweh.3256
- Rönnlund, M., Mäntylä, T., & Nilsson, L.G. (2008). The Prospective and Retrospective Memory Questionnaire (PRMQ): Factorial structure, relations to global subjective memory ratings, and Swedish norms. Scandinavian Journal of Psychology, 49, 11–18. doi: 10.1111/j.1467-9450.2007.00600.x
- Rydmark, I., Wahlberg, K., Ghatan, P.H., Modell, S., Nygren, Å., Ingvar, M., … Heilig, M. (2006). Neuroendocrine, cognitive and structural imaging characteristics of women on longterm sickleave with job stress-induced depression. Biological Psychiatry, 60, 867–873. doi: 10.1016/j.biopsych.2006.04.029
- Sandström, A., Nyström Rhodin, I., Lundberg, M., Olsson, T., & Nyberg, L. (2005). Impaired cognitive performance in patients with chronic burnout syndrome. Biological Psychology, 69, 271–279. doi: 10.1016/j.biopsycho.2004.08.003
- Stenlund, T., Ahlgren, C., Lindahl, B., Burell, G., Knutsson, A., Stegmayr, B., & Slunga Birgander, L. (2007). Patients with burnout in relation to gender and a general population. Scandinavian Journal of Public Health, 35, 516–523. doi: 10.1080/14034940701271874
- Tallberg, I.M., Wenneborg, K., & Almkvist, O. (2006). Reading words with irregular decoding rules: A test of premorbid cognitive function? Scandinavian Journal of Psychology, 47, 531–539. doi: 10.1111/j.1467-9450.2006.00547.x
- Van Dam, A., Keijsers, G., Eling, P., & Becker, E. (2011). Testing whether reduced cognitive performance in burnout can be reversed by a motivational intervention. Work & Stress, 25, 257–271. doi: 10.1080/02678373.2011.613648
- Van Dam, A., Keijsers, G., Eling, P., & Becker, E. (2015). Burnout and impaired cognitive performance: Review of evidence, underlying processes and future directions. In T.N. Winston (Ed.), Handbook on burnout and sleep deprivation (pp. 113–128). New York: Nova Science Publishers Inc.
- Van der Linden, D., Keijsers, G., Eling, P., & van Schaijk, R. (2005). Work stress and attentional difficulties: An initial study on burnout and cognitive failures. Work & Stress, 19, 23–36. doi: 10.1080/02678370500065275
- World Health Organization. (1992). ICD-10 classifications of mental and behavioural disorder: Clinical descriptions and diagnostic guidelines. Geneva: World Health Organization.
- Zigmond, A.S., & Snaith, R.P. (1983). The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica, 67, 361–370. doi: 10.1111/j.1600-0447.1983.tb09716.x
- Zimmermann, P., & Fimm, B. (2007). Test of attentional performance. Herzogenrath: PSYTEST.