
Abstract
The present study examined associations among parent and child reports of youth’s stressful life events (SLEs), perceived stress, and biological measures of stress activity (i.e. cortisol and cardiovascular activity). Examining these aspects of youth stress presents several challenges. Unlike adult studies of individual differences in which information regarding SLEs, perceptions of events, and biological activity are gathered from one individual, assessment of individual differences among children usually involves other informants (e.g. parent). However, parent and child reports of SLEs and the child’s psychological response to such events are often discordant. Moreover, examinations of youth perception of stress are hampered by limitations of child cognitive processes, as well as parents’ limited knowledge of their child’s perception of stress. In a preliminary effort to unscramble the complex effects of youth SLEs and perceived stress in relation to biological response to acute stressors, this study examined 51 boys and girls aged 7–16, with no history of psychopathology or medical concerns. Contrary to hypotheses, findings revealed that compared to actual experiences of stress, perceived stress has greater associations with both cortisol and cardiovascular activity. That is, perceived stress is more biologically salient relative to actual stress. Results also suggest that informant differences may explain some previous inconsistent findings in studies of youth’s stress reactivity. The current findings mirror the adult studies that show appraisal and perception of traumatic and stressful events may be more predictive of negative health and mental health outcomes than the severity of the events. Further studies are needed to understand the impact of youth’s perceptions of stress on their biological stress reactions and later health outcomes such as clinical disorders.
Introduction
Numerous studies show that exposure to stressful life events (SLEs) is associated with biological activity and alterations among children and adolescents (see Teicher, Andersen, Polcari, Anderson, & Navalta, Citation2002; Trickett, Noll, Susman, Shenk, & Putnam, Citation2010). However, few studies have examined whether the perception of stress is similarly associated with biological activity among youth. As defined by Lazarus and Folkman (Citation1984), heightened perceived stress is the impression that an individual’s demands are beyond their abilities. Perceived stress might alter the way in which children appraise an acute stressor, and in turn, that appraisal might influence acute stress reactivity and recovery (Gump & Matthews, Citation1999). For example, greater perceived stress may make some children prone to higher emotional distress (Hampel & Petermann, Citation2006), thereby influencing the interpretation and broader outcomes of life events. Some evidence suggests that perceived stress might mediate the relationship between adolescents’ life events and their depressive symptoms (e.g. Martin, Ford, Dyer-Friedman, Tang, & Huffman, Citation2004). However, cognitive limitations (Bailey & Garralda, Citation1990), and/or the perceived consequences of disclosure of events (e.g. Malloy, Brubacher, & Lamb, Citation2011), might bias children’s reports of experiences and symptoms. Parents might also be subject to biased reporting (De Los Reyes & Kazdin, Citation2005). Therefore, the effect of perceived stress, actual life events, or psychological distress in relation to acute stress activity might vary depending on the informant of the stress level and events, as well as the informant of the distress symptoms.
Children typically reveal a higher incidence of negative life events than their parents (e.g. Bailey & Garralda, Citation1990; Rende & Plomin, Citation1991; Richters & Martinez, Citation1993). Yet, parent ratings of their child’s stress in response to negative life events are notably higher than child ratings of their own stress (Rende & Plomin, Citation1991). Additionally, parent–child agreement on youth’s emotional and behavioral problems is low to moderately correlated (e.g. Achenbach, McConaughy, & Howell, Citation1987; Martin et al., Citation2004; Michels et al., Citation2013). The discrepancy between parent and child reports of emotional states is complex and might be tied to parents’ limited awareness of children’s experiences and different perceptions of life events (Kolko & Kazdin, Citation1993). Another common explanation has been that a youth’s internal state is outside of the parent’s awareness and thus, is difficult to report (Bailey & Garralda, Citation1990). If internal states are difficult to detect, then parent reports and child biomarkers pertinent to stress (e.g. HPA axis secretion of the hormone cortisol) might also be highly discordant. Nonetheless, associations between cortisol activity and internalizing symptoms in children and adolescents often rely on parental reports of child and adolescent internalizing symptoms and life events (e.g. Cicchetti & Natsuaki, Citation2014; Laurent, Gilliam, Wright, & Fisher, Citation2015; Ruttle, Armstrong, Klein, & Essex, Citation2014). However, some studies rely on self-reports of internalizing symptoms (El-Sheikh, Arsiwalla, Hinnant, & Erath, Citation2011; Nelemans et al., Citation2014) and some take a multi-informant approach (Shirtcliff & Essex, Citation2008). Variation in the reporter of events and internalizing symptoms might produce disparate findings even when studies uniformly examine specific cortisol markers (e.g. basal levels, reactivity, awakening response, diurnal patterns) but there is a paucity of relevant research in this area.
Present study
Utilizing a sample of typically developing children and adolescents, the current study examined relationships among parent and child reports of youth’s SLEs, perceived stress, and biological measures of arousal (e.g. cortisol and cardiovascular reactivity). This examination focused on three hypotheses. First, child-reported versus parent-reported SLEs (i.e. objective experience) and perceived stress would be more strongly associated with cortisol and cardiovascular responses to acute stress. Second, regardless of the reporter, SLEs would be more strongly associated with cortisol and cardiovascular activity than perceived stress (i.e. subjective experience). Third, the associations between stress (perceived or objective) and cortisol and cardiovascular activity would be positive, such that high stress would be associated with higher cortisol, heart rate, and blood pressure. Finally, post hoc analyzes explored whether perceived stress might mediate or moderate the association between SLEs and cortisol and cardiovascular activity.
Methods
Recruitment and participants
Participants were 51 healthy children/adolescents (52.9% boys) and their mothers recruited through community postings and direct mailings as part of a larger study of physiological responses to stress over the transition from childhood to adolescence (Stroud et al., Citation2009). Individuals interested in the study were screened by telephone to determine study eligibility. Fluency in spoken and written English was required for all participants and their mothers. Individuals taking prescription medications including oral contraceptives, thyroid medications, steroids, and psychotropic medications were excluded from the study. Participants were also required to be physically healthy (no current acute or chronic physical illness), with no history of diagnosed psychological or behavioral problems. All participants denied smoking, and regular drug or alcohol use.
Participants ranged in age from 7 to 16 (M = 12.41, SD = 2.30), and the racial composition in this sample was 80.4% Caucasian, 7.8% African American, 7.8% Multi-racial, 2.0% Hispanic, and 2.0% Other. Seventy-eight percent of the parents were married and 82% of mothers and 93.5% of fathers were employed. The average family income was $60,000–80,000. Maternal education ranged from completing/tenth grade to completion of a graduate degree. About one-quarter (24%) of mothers had a high school education or less and 40% graduated from college or obtained a graduate degree. Paternal education ranged from completion of middle school to completion of a graduate degree. About one-third (37.8%) of the fathers had a high school education or less and 44.5% graduated college or obtained a graduate degree.
Procedures
Protocols and procedures were reviewed and approved by The Miriam Hospital’s Institutional Review Board. Informed consent was obtained from mothers and assent was obtained from children and adolescents. The study involved two sessions: (1) the questionnaire session and (2) the physiology session. In the first session, participants habituated to the laboratory and physiological monitors while completing a battery of questionnaires including measures of anxiety and behavior problems (see below). The second session, a performance stress session, included a 20–25 min baseline period where participants were asked to read easy (grade K-2) books or watch G-rated movies and television shows, three stressors (lasting 10, 5, and 5 min, respectively), and a one-hour recovery period. During the recovery period participants completed questionnaires and again watched G-rated movies and television shows.
The stressor tasks included speech (5 min preparation, 5-min speech), mental arithmetic (5 min), and mirror tracing (5 min) tasks. The speech and mental arithmetic tasks were modified from the TSST for Children (TSST-C; Buske-Kirschbaum et al., Citation1997); the mirror-tracing task was adapted from Allen and Matthews (Citation1997). The speech task involved a preparation period (5 min, representing anticipation stress) and an academic speech (5 min) in front of a two-person audience who purportedly rated the speaker for quality and accuracy. Speeches focused on academic topics (e.g. history, science, and book report) and were adjusted to the age of the participant. Participants then completed a mental arithmetic task involving serial subtraction under time pressure for 5 min in front of the same two-person audience. Difficulty was adjusted based on participants’ age and performance. If an error was made, participants were asked to start over again from the beginning. The mirror-tracing task also lasted 5 min and involved tracing the figure of a six-sided star while viewing only its mirror image using a mirror star tracing apparatus (Lafayette Instruments, Lafayette, IN, 1987). Mistakes were counted and indicated by a sound and a white light. If errors were made, participants were instructed to start tracing the star again from the beginning.
All sessions began between 14:00 and 17:00 to control for diurnal variation in cortisol. Participants were asked to refrain from consuming food or drink (besides water) for two hours prior to the stress session, abstain exercise for 24 h prior to the session, and to avoid caffeine beginning the evening before the stress session. Seven to nine saliva samples were taken over the baseline, stress, and recovery periods (Stroud et al., Citation2009). Timing of saliva samples was designed to take into account a 20-min delay in cortisol responding (see section “Measures”). Blood pressure and heart rate recordings were taken at 2-min intervals during the baseline and stress induction periods and at 5-min intervals during the recovery period. Self-reported affect was assessed at baseline, during each stress task, and during the recovery period. Following the stress session, participants were extensively debriefed. Debriefing included an explanation with the experimenter as well as positive interactions with the audience members from the performance stress session. Participants and mothers were then compensated for their time.
Measures
Questionnaires
The Coddington Life Events Scale-Child (CLES-C; Coddington, Citation1972, Citation1999) is a validated measure of SLEs experienced during the past year. The CLES-C assesses the frequency of 12-positive and 24-negative life events that are likely to occur in childhood, including two open ended questions about changes that occurred. Negative life events were endorsed as “yes” or “no” and included items such as moving to a new school and death of a parent. For this study, we summed the 24 negative life events that were experienced in the past year. Both child and parent completed the same version of the CLES-C, allowing for comparison across items; however, this measure was only completed by participants age 11 and older. Life experiences (e.g. death of a pet and moving to a new school) were not expected to be highly correlated. Therefore, the internal consistency of the measure is not provided.
The Perceived Stress Scale (PSS; Cohen, Kamarck, & Mermelstein, Citation1983) is a 14-item measure designed to assess one’s perception of stress over the past month. Each item is rated on a 5-point Likert scale with higher ratings indicating higher perceived stress (0 = “never”, 2 = “sometimes”, 4 = “very often”). Both child and parent completed the PSS, with parent ratings reflecting their perception of their child’s stress. Similar to the CLES-C, the PSS was completed with participants age 11 and older. For the current study, the alpha coefficients for parent and child PSS were .89 and .64, respectively.
Given previous findings of increased stress reactivity among children with elevated anxiety symptoms (Rappaport & Katkin, Citation1972), the potential confluence of anxiety was measured by the Revised Children’s Manifest Anxiety Scale (RCMAS; Reynolds & Richmond, Citation1978, Citation2000), a 37-item self-report measure of anxiety for children and adolescents aged 6–19. For the present study, the “yes–no” responses were summed for a total anxiety symptom score. The composite scale yielded α = .82 showing good internal consistency.
Biological measures
Cortisol
Over the course of each stress session, seven to nine saliva samples were collected from each participant. Participants were asked to fill saliva collection vials to a designated line using a straw or by salivating directly into the tube (i.e. passive drool). Following collection, samples were frozen at −80 °C until overnight shipment on dry ice to Salimetrics Laboratories (State College, PA). Cortisol was analyzed in duplicate using a commercially available enzyme immunoassay without modification to the manufacturer’s protocol (Salimetrics, PA). The range of sensitivity was 0.007–3.0 ug/dL, and intra- and inter-assay coefficients of variation less than 5% and 10%, respectively. Salivary cortisol data are expressed in micrograms per deciliter (ug/dL).
Cardiovascular
Heart rate (HR), systolic blood pressure (SBP), and diastolic blood pressure (DBP) were measured using a Dinamap, automated, oscillometric blood pressure monitor (Critikon Inc., Tampa, FL). Participants were fitted with an appropriately sized cuff on their non-dominant arm prior to the start of the baseline period. Readings were collected every 2 min during baseline and stressor periods, and every 5 min during the recovery period. The cuff was removed at the end of the recovery period.
Statistical analysis
Preliminary analyzes and data reduction procedures
Due to variability in the number of saliva samples (7–9) collected during stress sessions, salivary cortisol and cardiovascular measures were reduced to six matched time points (see Stroud et al., Citation2009). Time points were selected to optimize timing for cortisol peaks relative to onset of stressors (20–30 min after onset). For all analyzes, baseline cortisol and cardiovascular measures were defined as the minimum of two baseline samples. Maximum post-stress biological measures were characterized as the maximum value achieved in response to (i.e. following) the stressors. Difference scores (i.e. change or reactivity) were calculated by subtracting the baseline from the maximum value.
For all data analyzes, outliers were defined as data points at or greater than three standard deviations from the mean and at least one standard deviation from the closest data point. Consequently, there was one outlier for each of five biological measures (i.e. baseline cortisol, peak cortisol, baseline BP, peak BP, peak SBP). All outliers were truncated to the nearest data value. There were no outliers for questionnaire measures. Likewise, there was no significant skewness and kurtosis for biological or questionnaire measures.
Primary analyzes
All data analyzes were conducted in IBM SPSS Statistics 23 Software (Armonk, NY). First socio-demographic variables were assessed in relation to psychosocial and biological measures of stress. Next, Pearson correlations were conducted to examine the bivariate associations between anxiety symptoms, perceived stress, SLEs, cortisol, and cardiovascular measures. Lastly, a series of hierarchical regression analyzes were planned to examine whether perceived stress mediated or moderated the association between SLEs and biological measures of stress. In keeping with the recommendations of Baron and Kenny (Citation1986), mediation analysis required that both the predictor and the mediator be significantly associated with the outcome variable and with each other. Significant demographic variables and anxiety symptoms were treated as covariates to examine the unique relationship between SLEs, perceived stress, and biological stress measures, as well as to examine potential differences across reporters (i.e. child and parent). In addition, cross product interaction terms were tested.
Notably, because of the small sample no corrections for multiple comparisons were applied. The study is essentially under powered and thus the estimates are conservative. With alpha at .05, power is estimated conservatively as .80 (80%) with two tested predictors (SLEs and CPS). With five predictors in total (Gender, Income, Anxiety, SLEs, and CPS), the required sample size is 68.
Results
Sample characteristics
An examination of demographics indicated that there were no significant gender, age, or family income differences in relation to SLEs or perceived stress, or in relation to anxiety symptoms. For this non-referred sample, baseline cortisol ranged from .03 to .26 ug/dL and peak cortisol levels ranged from .03 to .71 ug/dL (). Boys had significantly higher baseline and peak cortisol than girls (t(49) = 2.16, p < .05; t(49) = 2.37, p < .05, respectively), and girls had significantly higher cortisol change than boys (t(49) = 2.00, p < .05). Higher family income was significantly associated with higher baseline cortisol (r = .36, p < .01), but not with peak cortisol (r = .19, p = .18) or cortisol change (r = .10, p = .49). Age was not associated with any cortisol measures (r < .26, ns).
Table 1. Descriptive statistics of cortisol and cardiovascular measures and correlations between cardiovascular and cortisol measures.
With regards to cardiovascular measures, boys had higher systolic blood pressure than girls at baseline (t(49) = 2.69, p < .01), but not at peak (t(49) = 1.15, p = .26). There were no other gender differences or family income differences for cardiovascular measures. On the other hand, age was significantly negatively correlated with baseline and peak blood pressure (r = −.50, p < .001; r = −.36, p < .01), and age was positively related to peak systolic blood pressure and systolic change (r = .32, p < .05; r = .31, p < .05, respectively).
As shown in , baseline cardiovascular measures were not significantly associated with baseline cortisol. Similarly, cardiovascular reactivity (i.e. difference scores) was not significantly related to baseline cortisol. However, peak cardiovascular measures were significantly associated with baseline cortisol, with the exception of peak blood pressure (). Cardiovascular measures were also significantly positively related to peak cortisol and cortisol reactivity, with the exception of blood pressure ().
Parent, child-reporter effect
Self-report measures
On the Coddington Life Events Scale, child and parent reports were in agreement that there were no sibling, friend, or parent deaths during the past year. Children and adolescents reported school difficulties, increased arguments between parents, issues of peer acceptance, and increased arguments with parent(s) as the most frequent SLEs experienced in the past year. On the other hand, parents reported school difficulties, increased arguments between parent(s), moving to a new school, and a pet dying as the most prevalent SLEs experienced by their children in the past year (see ).
Table 2. Stressful life events that were endorsed most frequently.
Overall, child reports of SLEs, perceived stress, and symptoms were significantly correlated with each other but were not significantly correlated with parent reports (). Child-reported number of SLEs in the past year and child-perceived stress in the past month was significantly, positively related and both variables were significantly positively associated with anxiety symptoms. Similarly, parent-reported SLEs were positively related to parent-perceived child stress. However, neither of the parent-reported measures of child stress were associated with child-reported SLEs or perceived stress. Parent perception of child stress, but not reports of SLEs, neither parent measure was significantly related to child anxiety symptoms.
Table 3. Descriptives and correlations of child-reported and parent-reported stressful life events, perceived stressor, and child-reported symptoms.
Biological measures
In concert with our hypothesis, child-reports of life events and perceived stress were associated with biological measures to a greater extent than parent-reports. In fact, as indicated in , with the exception of heart rate change, parental reports were not significantly related to child cortisol or cardiovascular activity. On the other hand, as described below, child reports were significantly associated with indices of cortisol, heart rate, and diastolic blood pressure activity.
Table 4. Pearson correlations between life events, perceived stress, and biological measures.
Subjective versus objective stress
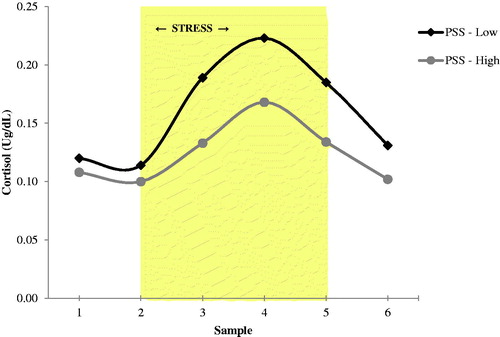
depicts average cortisol response by low and high levels perceived stress across the six samples collected during the stress session. As indicated, regardless of level of perceived stress, the peak stress period on average occurred between the third and fourth samples signaling that the mental arithmetic task or the combination of the speech and mental arithmetic tasks were the most stressful.
Figure 1. Perceived stress in relation to peak cortisol.
However, contrary to hypothesis, objective stress (child-reported SLEs) in the past year was not significantly related to measures of cortisol activity (). Yet, as shown in , subjective stress (child-reported perceived stress) was significantly negatively associated with baseline and peak cortisol, as well as with cortisol change. In other words, as compared to children and adolescents with lower levels of perceived stress, those with higher levels of perceived stress had lower baseline and peak cortisol, and lower changes in cortisol. Notably, the significant association between child reported of perceived stress and baseline cortisol was not maintained when perceived stress was dichotomized (see ).
Similar to the patterns found for cortisol activity, and contrary to hypothesis, actual life experience was not more closely associated with cardiovascular activity than perceived stress. Child-reported SLEs was significantly negatively associated with baseline heart rate and baseline diastolic blood pressure (see ), whereas child-reported perceived stress was significantly negatively related to peak heart rate and baseline diastolic blood pressure. As noted above, parent-reports were only associated with one biological measure. Specifically, parent-reported perception of increased child stress was associated with increased changes in heart rate.
Perceived stress in relation to cortisol activity, adjusted for life events, and demographics
Given the non-significant association between SLEs and biological measures, planned mediation analyzes were not conducted (see Baron & Kenny, Citation1986). However, hierarchical regression analyzes were conducted to examine if the child perception of stress remained negatively associated with cortisol and cardiovascular measures after controlling for relevant demographics, anxiety symptoms, and SLEs. Given the higher level of baseline cortisol found for boys, and for families with higher income, gender and family income were included in the first step of the model. Likewise, given the significant associations between child-reported SLEs and perceived stress with anxiety, anxiety symptoms were also included in the first step of the model. All variables except gender and family income were mean centered. As shown in , the significant association between child-perceived stress and baseline cortisol remained significant after accounting for demographics, anxiety symptoms, and SLEs. Family income also remained significant in the model. Similarly, when the model accounted for demographics, anxiety symptoms, and SLEs, perceived stress remained significantly related to peak cortisol and cortisol change. In fact, the associations were stronger than those found for the bivariate associations. Notably, the association between SLEs and cortisol peak was significant when perceived stress was not included in the model (i.e. Step 2). Perceived stress also remained significantly associated with change in cortisol during the acute stressor. A potential interaction between stressful experiences and perceived stress was examined by adding the mean-centered multiplicative terms to the regression models. As shown (i.e. Step 4), the interactions were significant for peak cortisol and for change in cortisol, such that cortisol activity (i.e. peaks and changes) was lower at high perceived stress and high life stress than at high perceived stress and low life stress. However, examinations of the linear slopes at below and above the means for perceived stress and SLEs did not yield significant findings. Examination of cardiovascular measures found that neither SLEs nor perceived stress remained significant in regression models after controlling for gender, family income, and anxiety. Albeit, with alpha at .05, a sample size of 51, power for the model was .70.
Table 5. Hierarchical regression of child-perceived stress in relation to cortisol.
Discussion
In this study, we examined both SLEs and perceived stress in relation to cortisol and cardiovascular activity in typically developing youth. We also investigated the differential effects of using self- or parent-report in such assessments. This unique assessment of biological activity among typically developing youth yields several findings that have implications for future stress research. Most importantly we found that biological reactivity is most strongly associated with child perception of stress in comparison to actual life events. This and other findings have valuable implications for the interpretation and understanding of existing studies of the experience of stress in youth.
Biological salience of perceived stress versus actual stress
Contrary to the hypothesis that SLEs would be more closely related to biological measures than to children’s perception of stress, we found that perceived stress was more strongly associated with biological measures. Perhaps the normative stressors assessed in this study (e.g. moving to a new school, parental divorce) do not meet threshold to generate the types of biological alterations and stress responses found in studies that assess trauma and severe adversities (e.g. Gordis, Granger, Susman, & Trickett, Citation2006; Jaffee et al., Citation2015; Trickett et al., Citation2010). Alternately, perhaps the duration or chronicity of the past year’s stressors is insufficient to provoke physiological changes. On the other hand, although we expected that for children actual experiences of stress and adversities, would be more biologically (e.g. physically, medically) impactful than perceived stress, these findings indicate that the perception of stress might be more closely tied to biological outcomes than the actual stressful experiences. Research with adults suggests that the appraisal and ongoing perception of stressful events may be one key component of adversity that helps to perpetuate the experience of stress (Gartland, O’connor, Lawton, & Bristow, Citation2014), and this continuation of stress, in turn, could generate biological responses and alterations. Unexpectedly, this cognitive perpetuation of stress seems to apply not only to adults, but also to children and adolescents.
Moreover, the direction of the associations between child-perceived stress and cortisol and cardiovascular activity among this healthy non-referred child and adolescent sample is unexpected. Although several child and adolescent studies have shown attenuation of biological activity to acute stress in relation to histories of severe and pervasive stressors, such as child abuse (Trickett et al., Citation2010), this is the first known study to report a similar pattern of attenuation among a typically developing, primarily a White middle class sample. This finding raises questions regarding the role of normative, everyday stressors on cortisol activity, as well as questions regarding the interpretation of attenuated HPA and autonomic system activity. Applying this complex picture to existing literature suggests that studies examining trauma exposure or other adverse life events in relation to cortisol activity might yield different results by accounting for the perception or appraisal of the potentially stressful or traumatic events in addition to the occurrence or the frequency of the events.
Importance of informants in relation to internal and biological processes
Our findings indicate that research examining physiological activity among children and adolescents should systematically address potential informant effects. As in previous research (e.g. Achenbach et al., Citation1987; Martin et al., Citation2004; Michels et al., Citation2013), we found low concordance between parent-report and self-report, further confirming the need for multiple informants and reemphasizing the value of the child’s perspective. As hypothesized, child and adolescent reports of their stress and stressors were more strongly associated with their biological markers of stress, particularly cortisol activity, than parent’s reports of those same indices. Indeed, internalizing processes that may not be available to parents, such as children’s cognitions, perceptions, or appraisal of events and of stress level, might have the greatest association with biological markers of stress. Thus, relying solely on parental reports of events, stress level, and/or internalizing symptoms might result in Type 2 errors or in inconsistent findings. Notably, even when parental reports were significantly associated with child cardiovascular activity, the direction of the associations was opposite that of the child-reports. Specifically, parents’ perception of higher child stress was associated with higher changes in heart rate and higher peak blood pressure, whereas child perception of higher stress was associated with lower cardiovascular activity.
Interestingly, parents’ perception of their child’s stress was more closely aligned with faster cardiovascular activity (i.e. heart rate and blood pressure) than with cortisol activity. This is consistent with the literature on informant correspondence with internalizing and externalizing symptoms. Cardiovascular activity, which has been most closely linked to externalizing symptoms (see Ortiz and Raine (Citation2004) for a meta-analysis), the symptoms most perceptible to parents, is associated with parents’ perception of stress. Whereas cortisol activity, which is most closely tied to depression and other internalizing symptoms (see Lopez-Duran, Kovacs, and George (Citation2009) for a meta-analysis), was not found to be significantly related to parental reports. This lack of an association suggests that parental reports might better align with biological markers correlated with externalizing and observable behaviors than with biological markers that correlate with internalizing and/or less observable behaviors (e.g. affective disorders). Although recent child stress response research has focused on measuring HPA axis and autonomic activity in tandem (Allwood, Handwerger, Kivlighan, Granger, & Stroud, Citation2011; Bauer, Quas, & Boyce, Citation2002), weighting and interpreting this multi-system information may also require the use of multiple informants.
Limitations and future directions
Despite the potential contributions of this study, the findings must be regarded as preliminary and interpreted in the context of several limitations. First, this is a small sample of healthy, typically developing children and adolescents and their mothers. Thus, the findings should be replicated with a larger sample and parental reports should be gathered from both mothers and fathers. Achenbach et al.’s (Citation1987) meta-analytical study found no differences in parent–child concordance of emotional/behavioral problems when fathers were the informant versus mothers, however, fathers’ reports of child’s stressful life experiences and their perception of their child’s stress may differ from mothers’ reports of these same phenomena. Moreover, the association between fathers’ reports and children’s biological stress activity is unknown and should be examined due to potential differences in the parent–child relationship.
In addition, the sample size, analyzes are limited to basic examinations and cannot investigate the possibility of more complex associations, such as three-way interaction effects, or the potential impact of parental concerns (e.g. parental depression) on parent ratings, or potential effects of pubertal stage. Note that self-reported Tanner stage was gathered for a subsample of the participants (n = 22). Correlation analyzes showed no significant relationship between the self-reported Tanner stage and the biological measures, perhaps because fewer than half the sample provided the information. Also, note that the stressful events and perceived stress measures were completed by those 11 and older.
Conclusion
In conclusion, our preliminary findings suggest that children’s and adults’ perceptions of child stress “gets under the skin” to differentially impact their biological functioning. Our findings suggest that perceived stress is more biologically salient relative to actual stress. Efforts to cope under conditions of perceived stress might lead to attenuated cortisol and cardiovascular activity. Alternatively, perceptions of high stress might render efforts to induce stressful conditions in laboratory paradigms less effective. These possibilities should be investigated further, with replication studies utilizing both a longitudinal approach and multiple informants.
Disclosure statement
The authors have no financial, consulting, or personal relationships to disclose.
Additional information
Funding
References
- Achenbach, T.M., McConaughy, S.H., & Howell, C.T. (1987). Child/adolescent behavioral and emotional problems: Implications of cross-informant correlations for situational specificity. Psychological Bulletin, 101, 213.
- Allen, M.T., & Matthews, K.A. (1997). Hemodynamic responses to laboratory stressors in children and adolescents: the influences of age, race, and gender. Psychophysiol, 34, 329–339.
- Allwood, M.A., Handwerger, K., Kivlighan, K.T., Granger, D.A., & Stroud, L.R. (2011). Direct and moderating links of salivary alpha-amylase and cortisol stress-reactivity to youth behavioral and emotional adjustment. Biological Psychology, 88, 57–64.
- Bailey, D., & Garralda, M.E. (1990). Life events: children's reports. Social Psychiatry and Psychiatric Epidemiology, 25, 283–288.
- Baron, R.M., & Kenny, D.A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51, 1173.
- Bauer, A.M., Quas, J.A., & Boyce, W.T. (2002). Associations between physiological reactivity and children’s behavior: advantages of a multisystem approach. Journal of Developmental and Behavioral Pediatrics, 23, 102–113.
- Buske-Kirschbaum, A., Jobst, S., Wustmans, A., Kirschbaum, C., Rauh, W., & Hellhammer, D. (1997). Attenuated free cortisol response to psychosocial stress in children with atopic dermatitis. Psychosomatic Medicine, 59, 419–426.
- Cicchetti, D., & Natsuaki, M.N. (2014). Multilevel developmental perspectives toward understanding internalizing psychopathology: current research and future directions. Development and Psychopathology, 26, 1189–1190.
- Coddington, R.D. (1972). The significance of life events as etiologic factors in the diseases of children. I. A survey of professionals. Journal of Psychosomatic Research, 16, 7–18.
- Coddington, R.D. (1999). Coddington life events scales (CLES) technical manual. Toronto: Multi-Health Systems.
- Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385–396.
- De Los Reyes, A., & Kazdin, A.E. (2005). Informant discrepancies in the assessment of childhood psychopathology: a critical review, theoretical framework, and recommendations for further study. Psychological Bulletin, 131, 483–509.
- El-Sheikh, M., Arsiwalla, D.D., Hinnant, J.B., & Erath, S.A. (2011). Children's internalizing symptoms: The role of interactions between cortisol and respiratory sinus arrhythmia. Physiology and Behavior, 103, 225–232.
- Gartland, N., O’connor, D.B., Lawton, R., & Bristow, M. (2014). Exploring day-to-day dynamics of daily stressor appraisals, physical symptoms and the cortisol awakening response. Psychoneuroendocrinology, 50, 130–138.
- Gordis, E.B., Granger, D.A., Susman, E.J., & Trickett, P.K. (2006). Asymmetry between salivary cortisol and α-amylase reactivity to stress: relation to aggressive behavior in adolescents. Psychoneuroendocrinology, 31, 976–987.
- Gump, B.B., & Matthews, K.A. (1999). Do background stressors influence reactivity to and recovery from acute stressors? Journal of Applied Social Psychology, 29, 469–494.
- Hampel, P., & Petermann, F. (2006). Perceived stress, coping, and adjustment in adolescents. The Journal of Adolescent Health, 38, 409–415.
- Jaffee, S.R., McFarquhar, T., Stevens, S., Ouellet‐Morin, I., Melhuish, E., & Belsky, J. (2015). Interactive effects of early and recent exposure to stressful contexts on cortisol reactivity in middle childhood. Journal of Child Psychology and Psychiatry, 56, 138–146.
- Kolko, D.J., & Kazdin, A.E. (1993). Emotional/behavioral problems in clinic and nonclinic children: Correspondence among child, parent and teacher reports. Journal of Child Psychology and Psychiatry, 34, 991–1006.
- Laurent, H.K., Gilliam, K.S., Wright, D.B., & Fisher, P.A. (2015). Child anxiety symptoms related to longitudinal cortisol trajectories and acute stress responses: evidence of developmental stress sensitization. Journal of Abnormal Psychology, 124, 68–79.
- Lazarus, R.S., & Folkman, S. (1984). Stress, appraisal, and coping. New York (NY): Springer Publishing Company.
- Lopez-Duran, N.L., Kovacs, M., & George, C.J. (2009). Hypothalamic–pituitary–adrenal axis dysregulation in depressed children and adolescents: a meta-analysis. Psychoneuroendocrinology, 34, 1272–1283.
- Malloy, L.C., Brubacher, S.P., & Lamb, M.E. (2011). Expected consequences of disclosure revealed in investigative interviews with suspected victims of child sexual abuse. Applied Developmental Science, 15, 8–19.
- Martin, J.L., Ford, C.B., Dyer-Friedman, J., Tang, J., & Huffman, L.C. (2004). Patterns of agreement between parent and child ratings of emotional and behavioral problems in an outpatient clinical setting: When children endorse more problems. Journal of Developmental and Behavioral Pediatrics, 25, 150–155.
- Michels, N., Vanaelst, B., Stoppie, E., Huybrechts, I., Bammann, K., Henauw, S., & Sioen, I. (2013). Parental and children's report of emotional problems: agreement, explanatory factors and event‐emotion correlation. Child and Adolescent Mental Health, 18, 180–186.
- Nelemans, S.A., Hale, W.W., III, Branje, S.J., van Lier, P.A., Jansen, L.M., Platje, E., … Meeus, W.H. (2014). Persistent heightened cortisol awakening response and adolescent internalizing symptoms: a 3-year longitudinal community study. Journal of Abnormal Child Psychology, 42, 767–777.
- Ortiz, J., & Raine, A. (2004). Heart rate level and antisocial behavior in children and adolescents: a meta-analysis. Journal of the American Academy of Child and Adolescent Psychiatry, 43, 154–162.
- Rappaport, H., & Katkin, E.S. (1972). Relationships among manifest anxiety, response to stress, and the perception of autonomic activity. Journal of Consulting and Clinical Psychology, 38, 219–224.
- Rende, R.D., & Plomin, R. (1991). Child and parent perceptions of the upsettingness of major life events. Journal of Child Psychology and Psychiatry, 32, 627–633.
- Reynolds, C.R., & Richmond, B.O. (1978). What I think and feel: a revised measure of children's manifest anxiety. Journal of Abnormal Child Psychology, 6, 271–280.
- Reynolds, C.R., & Richmond, B.O. (2000). Revised Children's Manifest Anxiety Scale. RCMAS manual. Los Angeles: Western Psychological Services.
- Richters, J.E., & Martinez, P.E. (1993). Violent communities, family choices, and children's chances: an algorithm for improving the odds. Development and Psychopathology, 5, 609–627.
- Ruttle, P.L., Armstrong, J.M., Klein, M.H., & Essex, M.J. (2014). Adolescent internalizing symptoms and negative life events: the sensitizing effects of earlier life stress and cortisol. Development and Psychopathology, 26, 1411–1422.
- Shirtcliff, E.A., & Essex, M.J. (2008). Concurrent and longitudinal associations of basal and diurnal cortisol with mental health symptoms in early adolescence. Developmental Psychobiology, 50, 690–703.
- Stroud, L.R., Foster, E., Papandonatos, G.D., Handwerger, K., Granger, D.A., Kivlighan, K.T., & Niaura, R. (2009). Stress response and the adolescent transition: performance versus peer rejection stressors. Development and Psychopathology, 21, 47–68.
- Teicher, M.H., Andersen, S.L., Polcari, A., Anderson, C.M., & Navalta, C.P. (2002). Developmental neurobiology of childhood stress and trauma. The Psychiatric Clinics of North America, 25, 397–426.
- Trickett, P.K., Noll, J.G., Susman, E.J., Shenk, C.E., & Putnam, F.W. (2010). Attenuation of cortisol across development for victims of sexual abuse. Development and Psychopathology, 22, 165–175.