
Abstract
There has been a long-standing interest in better understanding how social factors contribute to racial disparities in health, including birth outcomes. A recent emphasis in this context has been on identifying the effects of stress exposure and protective factors experienced over the entire lifetime. Yet despite repeated calls for a life course approach to research on this topic, very few studies have actually assessed how stressors and protective factors occurring over women’s lives relate to birth outcomes. We discuss this issue here by describing how challenges in the measurement of lifetime stress exposure and protective factors have prevented researchers from developing an empirically-based life course perspective on health. First, we summarize prevailing views on racial inequality and birth outcomes; second, we discuss measurement challenges that exist in this context; and finally, we describe both new tools and needed tools for assessing lifetime stress exposure and suggest opportunities for integrating information on stress exposure and psychosocial protective factors. We conclude that more studies are needed that integrate information about lifetime stress exposures and the protective factors that promote resilience against such exposures to inform policy and practice recommendations to reduce racial disparities in birth outcomes.
In 1983, the infant mortality rate for blacks was 2.1 times greater than the infant mortality rate for whites in the United States. Thirty years later, the magnitude of this gap had not changed: the infant mortality rate was 5.0% for whites and 11.2% for blacks (a 2.2-fold difference; Federal Interagency Forum on Child and Family Statistics, Citation2015). Relatedly, in 2014, black women gave birth to low birth weight infants at almost double the rate of white women (13.4% versus 6.9%) and had 1.5 times the preterm birth rate of white women (13.4% versus 8.9%; Martin, Hamilton, Osterman, et al., Citation2017). Inequality in income, education, or other demographic characteristics does not fully account for the black–white disparity in birth outcomes. In fact, the black–white infant mortality disparity is greater among women with a college degree or more compared to women with less education (United States Department of Health and Human Services, Citation2017).
These high rates of preterm birth, low birth weight, and infant mortality, which we collectively refer to here as poor birth outcomes, have significant costs. For example, coping with poor birth outcomes takes a social and emotional toll on family members (Lasiuk, Comeau, & Newburn-Cook, Citation2013). Preterm babies are also more likely to have neurodevelopmental disabilities (Jarjour, Citation2015), and up to two thirds will require special education services during their school age years (Hornby & Woodward, Citation2009). Longitudinal studies suggest that adults who were born preterm are also at increased risk for disabilities in adulthood (Moster, Lie & Markestad, Citation2008). Similarly, studies following low birth weight infants into adulthood have documented long-term neurodevelopmental impairments and persisting deficits in academic achievement (Hack et al., Citation2002). According to a National Institute of Medicine (Citation2007) report, the medical and education costs associated with preterm birth averaged $51,000 more per infant born prematurely compared to a baby born at term, totaling over $26 billion in 2005. Given the persistence, complexity, and high cost of the racial disparity in birth outcomes, many researchers have pursued its explanations.
The importance of understanding how inequities in stress over the life course may contribute to racial disparities in birth outcomes has been recognized since at least 2003, when Lu and Halfon (Citation2003) described the issue. Their recommendation to utilize a life course perspective was based on well-founded theory and suggestive empirical evidence. Since then, Lu and Halfon’s article has been cited over 500 times, and repeated calls have been made for the life course perspective in birth outcomes research, policy, and practice (Halfon, Larson, Lu, Tullis, & Russ, Citation2014; Rohan et al., Citation2014). Despite these calls, however, we still have very few empirical studies examining how lifetime stress exposure and related psychosocial protective factors interact to shape birth outcomes. The paucity of such research is largely because scientists have lacked the tools necessary to measure stress exposure and related protective factors over the life course.
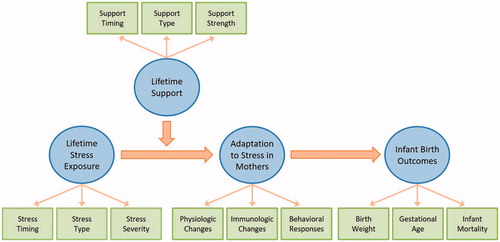
We address this issue here by discussing conceptual and measurement issues related to life course and birth outcomes research. First, we summarize the major theoretical tenants of the life course perspective for understanding racial inequality in birth outcomes, with the main factors depicted in . Second, we describe challenges that exist for gathering data based on the life course perspective. Finally, we suggest possible solutions to these challenges by examining new survey tools and recommending directions for the development of other survey tools that could provide the data needed for evidence-based policy and practice recommendations. Our hope is that by addressing the measurement challenges to testing the theoretical model, we will spur additional thinking and research on these topics, which is critical for identifying stress-related social, psychological, and biological processes that unfold over the lifespan and interact to shape birth outcomes and human health in general.
Figure 1. The theoretical model is based on the work of Lu and Halfon (Citation2003). The present paper focuses on the measurement challenges in evaluating the theoretical model.
Life course perspective
Theoretical approach
Understanding the effect of race on the life course requires a primer in social theory. Historians have documented how racial categories in the United States were developed to justify the inequitable distribution of material and psychological rewards in the colonial era (Zinn, Citation1980). This history’s legacy is wide-ranging. For example, racial residential segregation allows whites access to more resources such as wealth (e.g. through housing values), neighborhood resources (e.g. full scale grocers), access to desirable jobs, the best public education, and distance from environmental hazards (Reskin, Citation2012). The system of racial inequality also structures access to social rewards, such as fair interpersonal treatment, positive portrayal in the media, and the experience of being evaluated on one’s actions rather than one’s racial group membership (Bonilla-Silva, Citation1997). In this paper, we focus on differences between Blacks and Whites, but disparities in birth outcomes exist between other groups in the United States as well, making the theoretical and measurement challenges discussed below widely applicable.
In 2003, Lu and Halfon (Citation2003) described how racially-structured inequity in both exposure to stressors and access to protective factors over a lifetime could lead to unequal birth outcomes through cumulative exposure and early programing. More evidence about how these pathways may operate has been collected since their paper was published. Mechanistically speaking, stress alters the activity of the hypothalamic–pituitary–adrenal (HPA) axis, sympathetic-adrenal-medullary (SAM) axis, and immune system in ways that in turn affect health (for reviews, see Boyce & Ellis, Citation2005; Graham, Christian, & Kiecolt-Glaser, Citation2006; Lupien, McEwen, Gunnar, & Heim, Citation2009; Miller, Chen, & Parker, Citation2011; Slavich, Citation2016). For example, stress triggers the release of cortisol (from the HPA axis) and epinephrine and norepinephrine (from the SAM axis), which interact with receptors on immune cells to regulate levels of cellular inflammatory activity throughout the body (Slavich & Irwin, Citation2014). Over time, however, this response can cause increased epinephrine and norepinephrine sensitivity, and reduced glucocorticoid sensitivity (Cohen et al., Citation2012; Silverman & Sternberg, Citation2012), which promotes chronic, low-grade inflammation that leads to oxidative stress and increased risk for inflammation-related disease over time (McEwen, Citation1998; Miller et al., Citation2011). Stress can also cause long-term changes in how these systems are regulated by, for example, inducing alterations in the leukocyte basal transcriptome (Slavich & Cole, Citation2013), physical structure and functional activity of brain regions that regulate the HPA and SAM axis (McEwen, Eiland, Hunter, & Miller, Citation2012), and regulation of neural-immune pathways that govern systemic inflammation (Irwin & Cole, Citation2011; Slavich, Citation2015).
Other scholars have described additional, non-biological pathways that may lead to unequal health outcomes, such as negative health behaviors that individuals engage in when coping with stress (Kramer & Hogue, Citation2009). When combined with social theory and the biological models, these formulations begin to provide a rich theoretical framework for understanding how differences in stress exposure and psychosocial resources may affect health over the lifespan. However, very few studies have actually tested predictions derived from these models and, consequently, only a very small empirical literature exists describing how different stressors occurring over the life course accumulate to affect birth outcomes. We also know relatively little about the psychosocial factors that might moderate the negative effects that such exposures have on health.
Empirical research on birth outcomes
The studies that have been conducted thus far have been informative. Early in the development of the life course perspective on health, for example, Geronimus (Citation1992) showed that Black and White women have different patterns of birth outcomes over their reproductive lives. She also demonstrated that Black women experience higher rates of factors that are associated with stress and poor birth outcomes, including high blood pressure (Geronimus, Andersen, & Bound, Citation1991). More recent studies provided additional support for the life course perspective in other areas of health, showing that adverse childhood experiences negatively affect adult health (e.g. allostatic load, health behaviors, cardiovascular disease) and are more common among Blacks and Latinos than among whites (Felitti et al., Citation1998; Shonkoff, Garner, The Committee on Psychological Aspects of Child and Family Health, Committee on Early Childhood, Adoption, and Dependent Care and Second on Developmental and Behavioral Pediatrics, Citation2012). Yet, a recent review of population-based studies found only three studies linking pre-pregnancy stress and birth outcomes, with the longest preconception period being only 6 months (Witt, Litzelman, Cheng, Wakeel, & Barker, Citation2014). A short-preconception period is a common challenge in research on stress exposure and health. For example, CDC’s Pregnancy Risk Assessment Monitoring System asks about stressful life events, but only for the 12 months prior to the birth of the focal child, which is at odds with the theoretical perspectives on lifetime stress exposure and health described above. In fact, we are aware of very few birth outcome studies that have examined lifetime stress exposure.
Among the studies that have been done, Witt et al. (Citation2015) used the large Early Childhood Longitudinal Study, Birth Cohort (n= 9300 in their subsample) to examine the interaction of current neighborhood disadvantage and stressors related to relationships, such as the death of a family member, divorce, and fertility problems, at any time before conception. They found that more preconception stress was associated with greater likelihood of a very low birth weight infant. Additionally, these effects were strongest for mothers living in the most disadvantaged neighborhoods. A study by Collins, Wambach, David, and Rankin (Citation2009) used linked Illinois birth records (N > 300 K) to estimate lifetime exposure to poverty for recent mothers based on the mothers’ residence at the time of their infants’ birth and at the time of their own births. They found that Black women were more likely to have lived in poor neighborhoods at both times and, in addition, that living in neighborhoods in the lowest income tertile was associated with a greater risk for low birth weight for Black women relative to White women. None of these studies included comprehensive measures of stress, timing of stress, or assessed physiological markers of stress. Yet, taken together, the findings highlight the utility of adopting a life course perspective on health and provide initial evidence that stressful circumstances can affect pregnancy outcomes, even if only measured using a short list of stressors.
These existing studies of stress and birth outcomes underscore the potentially deleterious consequences of stress, but not everyone who is exposed to major life stressors experiences poor health. To better understand social factors that might structure differences in stress-related health outcomes, researchers have studied a variety of psychosocial processes that might buffer the impact of stress on health. Probably the most widely studied dynamic involves positive social relationships (Cohen & Williamson, Citation1988). Both emotional support (e.g. someone to listen to one's problems) and instrumental support (e.g. free childcare) have been associated with positive health outcomes (Thoits, Citation2011). It is difficult to disentangle the effects of social support from the potential for social ties to help women avoid stressors in the first place (Thoits, Citation2011). Nonetheless, as Lu and Halfon (Citation2003) explained, the considerable evidence that social support improves health makes the construct central to models of how life course factors affect health. Indeed, a few studies have linked a warm parenting relationship during childhood with improved adult health on a wide range of measures (e.g. Russek & Schwartz, Citation1997). Similarly, a recent study found that perceptions of being loved and cared for as a child is associated with reduced allostatic load among adults (Slopen, Chen, Priest, Albert, & Williams, Citation2016). And yet, to our knowledge, no studies have examined how lifetime social support or other protective psychosocial factors influence birth outcomes.
Measurement challenges and recommendations
To improve our understanding of the life course perspective on health, we need more empirical studies that can provide additional specificity on the strength and nature of the relationships between lifetime stress exposures, protective factors, and birth outcomes. To help advance this initiative, we make some methodological recommendations below and describe how existing measures could be applied to assist in this effort.
Lifetime stress exposure
Lifetime social environment can be measured using panel studies in which individuals are interviewed repeatedly over time or in cross-sectional studies where individuals are asked to recall their exposure to different stressors over the life course. Panel studies are ideal, but require substantial time and money. We thus recommend beginning with a cross-sectional approach to obtain initial data quickly. The validity of the retrospective approach has been questioned by investigators who are concerned with recall bias, but research has shown that major life stressors can be reliably recalled for decades, especially when the stress assessment questions are detailed and the stressors probed are moderate-to-severe in nature (e.g. Dohrenwend, Citation2006; Kessler & Wethington, Citation1991).
Research on stress has identified several aspects of the stress experience that are important to assess. First, because stressors are not experienced in the same way across different individuals, it is important to measure not just stress exposure, but also perceptions of the severity of those exposures, because perceived stress is known to predict negative health behaviors and poor health outcomes (Cohen & Willis, Citation1985). In fact, given evidence showing that appraisals of situations and a person’s perceived ability to cope strongly influence the degree to which individuals find situations to be stressful (Lazarus & Folkman, Citation1984; Lebois, Hertzog, Slavich, Feldman Barrett, & Barsalou, Citation2016), the best tests of the life course theory of stress and birth outcomes may ultimately focus on women’s perceptions of the different stressors they have experienced. Second, numerous studies have shown that stressors occurring early in life may exert stronger effects on health by influencing individuals’ physiologic “set point” or reactivity to stressors, and by influencing sleep quality, diet, and related health behaviors. Consequently, it is also important to assess the specific timing of when each major life stressor occurred during life course. Finally, stressors can occur in several different life domains (e.g. relationships, work, housing, finances) and may possess different social–psychological characteristics (e.g. interpersonal loss, physical danger, humiliation) that may have different effects on health. It is also important, therefore, to assess stressors’ life domain and core social–psychological characteristics (Slavich, Citation2016).
Assessing these different aspects of lifetime stress exposure has historically been difficult because no tools have existed for systematically measuring stress exposure occurring over the life course. However, Slavich addressed this issue by developing the Stress and Adversity Inventory (STRAIN), which is the first online system for assessing the severity, frequency, timing, and duration of 55 different types of acute life events and chronic difficulties that individuals could have experienced since childhood. Based on this information, the system produces 115 summary scores and life charts that describe a person’s exposure to different types of stressors that are known to affect health. The STRAIN has excellent test–retest reliability (rs = .904–.919; Slavich & Shields, Citation2017) and predictive validity in relation to several different health outcomes, including metabolic function (Kurtzman et al., Citation2012), fatigue and depression (Bower, Crosswell, & Slavich, Citation2014; Dooley, Slavich, Moreno, & Bower, Citationin press), and mental and physical health (Shields, Moons, & Slavich, Citation2017; Toussaint, Shields, Dorn, & Slavich, Citation2016). As the STRAIN produces summary scores across 12 different life domains (e.g. work, marital/partner, financial, etc.) and five social–psychological characteristics (e.g. interpersonal loss, physical danger), future research using the STRAIN or similar instruments could evaluate whether birth outcomes differ as a function of specific type, timing, or perceived severity of stressor exposure.
Researchers seeking to understand racial disparities in birth outcomes could employ systems like the STRAIN, but should also pay particular attention to stressors that are known to be distributed or experienced differently across races. Examples include everyday racial discrimination, exposure to the criminal justice system, and neighborhood stress. Researchers have already developed validated measures of everyday discrimination, for example, that could be adapted to a life course perspective (Williams & Mohammed, Citation2008). In addition, neighborhood stress data could be constructed by asking women where they have lived over their lives, linking the addresses to publicly available data on poverty or crime, and determining whether the timing of these factors is associated birth outcomes. By developing measures of lifetime stress that capture the particular difficulties created by the structural sources of racial inequality, researchers would be better equipped to answer questions about whether and how racial disparities in lifetime stress exposure, severity, and time lead to racial disparities in birth outcomes.
Protective factors
In terms of protective factors, we are not aware of any comprehensive measures assessing the presence of protective factors across the life course. The development of such measures will require methodological testing, but can be accelerated by adapting existing measures to a life course perspective. The Midlife in the United States study offers one example of how existing measures can be adapted. This study utilized a subset of the Childhood Trauma Questionnaire (Bernstein & Fink, Citation1998) to assess childhood support by asking seven questions about feeling loved and having an adult to provide care (Slopen et al., Citation2016). This measure does not capture strength of the support, variation in support over the life course, or the wide range of sources of support, but it does provide a foundation from which expanded measures can be created.
The development of new measures can be guided by instruments that have been well-tested, such as Berkman and Syme’s Social Network Index (Citation1979). Items ask respondents about their frequency of attendance religious services and whether they have someone they can trust to provide good advice. Like other social support measures, the index assesses both the frequency and quality of social contact. Social relationship quality may be very important in this context, because social relationships can provide support but also be a source of stress (Thoits, Citation2011). New measures would have to be tested to evaluate the instrument’s psychometric properties and respondents’ reliability of recall.
Several protective factors other than social integration may also be important to assess, including optimism, religious faith, hobbies, and exercise. Instruments exist for obtaining current assessments of these factors, and we believe that lifetime measures could be developed based on these instruments. The development of such measures would be extremely beneficial, and future research should thus develop and test the validity and reliability of such measures to improve research on birth outcomes from a life course perspective. Multidimensional measures of lifetime support would allow researchers to assess the extent to which various types of support improve birth outcomes, whether the perceived strength of the support influences outcomes, and whether the timing of the support matters.
Integrating measures of stress exposure and protective factors
Measuring stress exposure and protective factors separately is a challenge, but the greatest challenge – and thus opportunity for future research – will be to match the timing of stressors with the presence of protective factors over the life course. The availability of social support and other protective factors is most critical when an individual is undergoing high levels of stress. One strategy for integrating these two sources of information would be to create general timing categories (e.g. childhood, adolescence, young adulthood, adulthood) and then catalog the presence of both stress exposure and protective factors in each category in order to test the buffering effect of the protective factors on health. A second, more nuanced approach would involve building a life chart of major life stressors and then working with individuals to plot the presence of various protective factors over time.
Protective factors can be immensely helpful when a major life stressor occurs, but the presence of factors such as good social support can also lessen the likelihood of particular stressors occurring (e.g. a person gives you good advice, which helps you avoid a bad financial investment; Thoits, Citation2011). Consequently, the positive effect that protective factors have on health may be underestimated if buffering effects are evaluated only during stressful periods. In addition, researchers could compare the influence of protective factors among individuals with similar individual and neighborhood social conditions in order to elucidate the extent to which various protective factors minimize exposure to particular stressors. Regardless of the specific strategy used, we believe these integrative approaches highlight the need to collect data on both stress exposure and protective factors over the entire life course, as opposed to just during certain time periods.
Ultimately, matching stress exposure and protective factor data over the life course could greatly advance research on the psychosocial determinants of health outcomes, leading in turn to better interventions. At the same time, acquiring high resolution data on both stressor exposure and protective factors is time consuming. Future research should thus evaluate the relative utility of these approaches while attempting to balance the need for highly detailed timing information with the respondent burden that is associated with obtaining such information. It is only with such data that we can assess whether support over the life course protects against the potentially negative health effects of stress experiences.
Conclusions
The United States has a large Black–White gap in infant prematurity, low birth weight, and mortality. A substantial body of research suggests that these outcomes are strongly shaped by the social–environmental context and health of the mother. Consequently, there is a pressing need to better understand how stress exposure and psychosocial resources like social support affect birth outcomes, in addition to other sources of human morbidity and mortality, and whether these factors explain the Black–White inequity in birth outcomes. In this context, theorists have widely recognized the importance of adopting a life course perspective for understanding these effects. However, despite repeated calls for additional studies on the topic, the potential of life course research for advancing our understanding of racial disparities in birth outcomes has not been realized. We argue that the lack of empirical studies on the topic is due in large part to challenges that have been associated with measuring individuals’ stress exposure and protective factors across the life course.
Recent developments in stress measurement, including the STRAIN for assessing lifetime stress exposure, have enabled investigators to characterize disparities in the specific types and amount of life stress that individuals experience over the life course. Similar systems could be developed to measure protective factors as well. The development of such tools is critical for advancing the study of psychosocial and environmental factors affecting birth outcomes specifically, as well as human health more generally. Such initiatives are also important for providing a balanced perspective on human health – one that integrates across several levels of analysis, including neural, physiologic, and genetic, while paying attention to social factors that are known to structure health disparities.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Berkman, L.F., & Syme, L. (1979). Social networks, host resistance, and mortality: A nine-year follow-up study of Alameda county residents. American Journal of Epidemiology, 109, 186–204. doi: https://doi.org/10.1093/oxfordjournals.aje.a112674
- Bernstein, D., & Fink, L. (1998). Manual for the Childhood Trauma Questionnaire. New York: The Psychological Corporation.
- Bonilla-Silva, E. (1997). Rethinking racism: Toward a structural interpretation. American Sociological Review, 62, 465–480. doi: 10.2307/2657316
- Bower, J.E., Crosswell, A.D., & Slavich, G.M. (2014). Childhood adversity and cumulative life stress: Risk factors for cancer-related fatigue. Clinical Psychological Science, 2, 108–115. doi: 10.1177/2167702613496243
- Boyce, W.T., & Ellis, B.J. (2005). Biological sensitivity to context: I. An evolutionary-developmental theory of the origins and functions of stress reactivity. Development and Psychopathology, 17, 271–301. doi: 10.1017/S0954579405050145
- Cohen, S., & Williamson, G. (1988). Perceived stress in a probability sample of the United States. In S. Spacapan & S. Oskamp (Eds.), The social psychology of health: The Claremont symposium on applied social psychology (pp. 31–67). Thousand Oaks, CA: Sage Publications.
- Cohen, S., & Willis, T.A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98, 310–357. doi: 10.1037//0033-2909.98.2.310
- Cohen, S., Janicki-Deverts, D., Doyle, W.J., Miller, G.E., Frank, E., Rabin, B.S., & Turner, R.B. (2012). Chronic stress, glucocorticoid receptor resistance, inflammation, and disease risk. Proceedings of the National Academy of Sciences of the United States of America, 109, 5995–5999. doi: 10.1073/pnas.1118355109
- Collins, J.W., Wambach, J., David, R.J., & Rankin, K.M. (2009). Women’s lifelong exposure to neighborhood poverty and low birth weight: A population-based study. Maternal and Child Health Journal, 13, 326–333. doi: 10.1007/s10995-008-0354-0
- Dohrenwend, B.P. (2006). Inventorying stressful life events as risk factors for psychopathology: Toward resolution of the problem of intracategory variability. Psychological Bulletin, 132, 477–495. doi: 10.1037/0033-2909.132.3.477
- Dooley, L.N., Slavich, G.M., Moreno, P.I., & Bower, J.E. (in press). Strength through adversity: Moderate lifetime stress exposure is associated with psychological resilience in breast cancer survivors. Stress and Health, doi: 10.1002/smi.2739
- Federal Interagency Forum on Child and Family Statistics. (2015). America’s children: Key national indicators of well-being. Washington, DC: U.S. Government Printing Office. Retrieved from https://www.childstats.gov/pdf/ac2015/ac_15.pdf
- Felitti, V.J., Anda, R.F., Nordenberg, D., Williamson, D.F., Spitz, A.M., Edwards, V., … Marks, J.S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine, 14, 245–258. doi: 10.1016/S0749-3797(98)00017-8
- Geronimus, A.T. (1992). The weathering hypothesis and the health of African-American women and infants: Evidence and speculations. Ethnicity and Disease, 2, 207–221.
- Geronimus, A.T., Andersen, H.F., & Bound, J. (1991). Differences in hypertension prevalence among U.S. black and white women of childbearing age. Public Health Reports, 106, 393–399.
- Graham, J.E., Christian, L.M., & Kiecolt-Glaser, J.K. (2006). Stress, age, and immune function: Toward a lifespan approach. Journal of Behavioral Medicine, 29, 389–400. doi: 10.1007/s10865-006-9057-4
- Hack, M., Flannery, D.J., Schluchter, M., Cartar, L., Borawski, E., & Klein, N. (2002). Outcomes in young adulthood for very-low-birth-weight infants. The New England Journal of Medicine, 346, 149–157. doi: 10.1056/NEJMoa010856
- Halfon, N., Larson, K., Lu, M., Tullis, E., & Russ, S. (2014). Lifecourse health development: Past, present and future. Maternal and Child Health Journal, 18, 344–365. doi: 10.1007/s10995-013-1346-2
- Hornby, G., & Woodward, L.J. (2009). Educational needs of school-aged children born very and extremely preterm: A review. Educational Psychology Review, 21, 247–266. doi:10.1007/s10648-009-9109-8
- Institute of Medicine, Committee on Understanding Premature Birth and Assuring Healthy Outcomes. (2007). Societal costs of preterm birth. In R.E. Behrman & A. Stith Butler (Eds.), Preterm birth: Causes, consequences, and prevention (pp. 398–428). Washington, DC: The National Academies Press.
- Irwin, M.R., & Cole, S.W. (2011). Reciprocal regulation of the neural and innate immune systems. Nature Reviews Immunology, 11, 625–632. doi: 10.1038/nri3042
- Jarjour, I.T. (2015). Neurodevelopmental outcome after extreme prematurity: A review of the literature. Pediatric Neurology, 52, 143–152. doi: 10.1016/j.pediatrneurol.2014.10.027
- Kessler, R.C., & Wethington, E. (1991). The reliability of life event reports in a community survey. Psychological Medicine, 21, 723–738. doi: https://doi.org/10.1017/s0033291700022364
- Kramer, M.R., & Hogue, C.R. (2009). What causes racial disparities in very preterm birth? A biosocial perspective. Epidemiologic Reviews, 31, 84–98. doi: 10.1093/ajerev/mxp003
- Kurtzman, L., O'donovan, A., Koslov, K., Arenander, J., Epel, E.S., & Slavich, G.M. (2012). Sweating the big stuff: Dispositional pessimism exacerbates the deleterious effects of life stress on metabolic health. European Journal of Psychotraumatology, 3. doi: 10.3402/ejpt.v3i0.19401
- Lasiuk, G.C., Comeau, T., & Newburn-Cook, C. (2013). Unexpected: An interpretive description of parental traumas’ associated with preterm birth. BMC Pregnancy and Childbirth, 13, S13. doi: 10.1186/1471-2393-13-S1-S13
- Lazarus, R.S., & Folkman, S. (1984). Stress, appraisal, and coping. New York, NY: Springer.
- Lebois, L.A.M., Hertzog, C., Slavich, G.M., Feldman Barrett, L., & Barsalou, L.W. (2016). Establishing the situated features associated with perceived stress. Acta Psychologica, 169, 119–132. doi: 10.1016/j.actpsy.2016.05.012
- Lee, H., McCormick, T., Hicken, M.T., & Wildeman, C. (2015). Racial inequalities in connectedness to imprisoned individuals in the United States. Du Bois Review: Social Science Research on Race, 12, 269–282. doi: 10.1017/S1742058X15000065
- Lu, M.C., & Halfon, N. (2003). Racial and ethnic disparities in birth outcomes: A life-course perspective. Maternal and Child Health Journal, 7, 13–30. doi: 10.1023/A:1022537516969
- Lupien, S.J., McEwen, B.S., Gunnar, M.R., & Heim, C. (2009). Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nature Reviews Neuroscience, 10, 434–445. doi: 10.1038/nrn2639
- Martin, J.A., Hamilton, B.E., Osterman, M.J., Driscoll, A.K., & Matthews, T.J.. (2017). Births: Final data for 2015. National vital statistics report (Vol. 66, no. 1). Hyattsville, MD: National Center for Health Statistics.
- McEwen, B.S. (1998). Stress, adaptation, and disease. Allostasis and allostatic load. Annals of the New York Academy of Sciences, 840, 33–44. doi: 10.1111/j.1749-6632.1998.tb09546.x
- McEwen, B.S., Eiland, L., Hunter, R.G., & Miller, M.M. (2012). Stress and anxiety: Structural plasticity and epigenetic regulation as a consequence of stress. Neuropharmacology, 62, 3–12. doi: 10.1016/j.neuropharm.2011.07.014
- Miller, G.E., Chen, E., & Parker, K.J. (2011). Psychological stress in childhood and susceptibility to the chronic diseases of aging: Moving towards a model of behavioral and biological mechanisms. Psychological Bulletin, 137, 959–997. doi: 10.1037/a0024768
- Moster, D., Lie, R.T., & Markestad, T. (2008). Long-term medical and social consequences of preterm birth. The New England Journal of Medicine, 359, 262–273. doi: 10.1056/NEJMoa0706475
- Reskin, B. (2012). The race discrimination system. Annual Review of Sociology, 38, 17–35. doi: 10.1146/annurev-soc-071811-145508
- Rohan, A.M., Onheiber, P.M., Hale, L.J., Kruse, T.L., Jones, M.J., Gillespie, K.H., … Katcher, M.L. (2014). Turning the ship: Making the shift to a life-course framework. Maternal and Child Health Journal, 18, 423–430. doi: 10.1007/s10995-013-1225-x
- Russek, L.G., & Schwartz, G.E. (1997). Feeling of parental caring predict health status in midlife: A 35-year follow-up of the Harvard Mastery of Stress Study. Journal of Behavioral Medicine, 20, 1–13. doi: 10.1023/A:1025525428213
- Shields, G.S., Moons, W.G., & Slavich, G.M. (2017). Better executive function under stress mitigates the effects of recent life stress exposure on health in young adults. Stress, 20, 75–85. doi: 10.1080/10253890.2017.1286322
- Shonkoff, J.P., Garner, A.S., & The Committee on Psychological Aspects of Child and Family Health, Committee on Early Childhood, Adoption, and Dependent Care and Second on Developmental and Behavioral Pediatrics. (2012). The lifelong effects of early childhood adversity and toxic stress. Pediatrics, 129, e232–e246.s. doi: 10.1542/peds.2011-2663
- Silverman, M.N., & Sternberg, E.M. (2012). Glucocorticoid regulation of inflammation and its functional correlates: From HPA axis to glucocorticoid receptor dysfunction. Annals of the New York Academy of Sciences, 1261, 55–63. doi: 10.1111/j.1749-6632.2012.06633.x
- Slavich, G.M. (2015). Understanding inflammation, its regulation, and relevance for health: A top scientific and public priority. Brain, Behavior, and Immunity, 45, 13–14. doi: 10.1016/j.bbi.2014.10.012
- Slavich, G.M. (2016). Life stress and health: A review of conceptual issues and recent findings. Teaching of Psychology (Columbia, MO), 43, 346–355. doi: 10.1177/0098628316662768
- Slavich, G.M., & Cole, S.W. (2013). The emerging field of human social genomics. Clinical Psychological Science, 1, 331–348. doi: 10.1177/2167702613478594
- Slavich, G.M., & Irwin, M.R. (2014). From stress to inflammation and major depressive disorder: A social signal transduction theory of depression. Psychological Bulletin, 140, 774–815. doi: 10.1037/a0035302
- Slavich, G.M., & Shields, G.S. (2017). Assessing lifetime stress exposure using the Stress and Adversity Inventory for Adults (Adult STRAIN): An overview and initial validation. Psychosomatic Medicine, in press.
- Slopen, N., Chen, Y., Priest, N., Albert, M.A., & Williams, D.R. (2016). Emotional and instrumental support during childhood and biological dysregulation in midlife. Preventive Medicine, 84, 90–96. doi: 10.1016/j.ypmed.2015.12.003
- Thoits, P.A. (2011). Mechanisms linking social ties and support to physical and mental health. Journal of Health and Social Behavior, 52, 145–161. doi: 10.1177/0022146510395592
- Toussaint, L., Shields, G.S., Dorn, G., & Slavich, G.M. (2016). Effects of lifetime stress exposure on mental and physical health in young adulthood: How stress degrades and forgiveness protects health. Journal of Health Psychology, 21, 1004–1014. doi: 10.1177/1359105314544132
- United States Department of Health and Human Services (US DHHS), Centers of Disease Control and Prevention (CDC), National Center for Health Statistics (NCHS), Division of Vital Statistics (DVS) (2017). Linked Birth/Infant Death Records 2007–2013, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program, on CDC WONDER On-line Database. Retrieved from http://wonder.cdc.gov/lbd-current.html
- Williams, D.R., & Mohammed, S.A. (2008). Discrimination and racial disparities in health: Evidence and needed research. Journal of Behavioral Medicine, 32, 20–47. doi: 10.1007/s10865-008-9185-0
- Witt, W.P., Litzelman, K., Cheng, E.R., Wakeel, F., & Barker, E.S. (2014). Measuring stress before and during pregnancy: A review of population-based studies of obstetric out comes. Maternal and Child Health Journal, 18, 52–63. doi: 10.1007/s10995-013-1233-x
- Witt, W.P., Park, H., Wisk, L.E., Cheng, E.R., Mandell, K., Chatterjee, D., & Zarak, D. (2015). Neighborhood disadvantage, preconception stressful life events, and infant birth weight. American Journal of Public Health, 105, 1044–1052. doi: 10.2105/AJPH.2015.302566
- Zinn, H. (1980). A people’s history of the United States. New York, NY: The New Press.