
Abstract
The objective of this study was to assess basal autonomic nervous system (ANS) activity as a pathway linking subjective social status to health in a high-demand work environment. It was hypothesized that officers with a lower status experienced more chronic stress (higher basal ANS activity) and that chronic stress was related to more health problems. Fifty-six male and female Swiss police officers self-reported on subjective social status (country, community, friends, police) and their health (depression, post-traumatic stress, physical symptoms) and collected 12 saliva samples over two days for basal α-amylase activation (sAA) assessment. Multilevel regression analyses revealed that subjective social status in the police and physical symptoms explained a significant part of the variance in diurnal sAA activity patterns. The current findings support the idea that more narrowly defined subjective social status may be more closely linked to biological stress mechanisms. Additionally, sAA activity was specifically related to physical, but not mental health problems. These results suggest that subjective social status referencing one’s work environment may be a promising early indicator of health-relevant changes in stress-related physiological systems.
Introduction
Law enforcement is an occupation characterized by the need to balance daily exposure to violent and volatile situations, an increasing public demand for security and probity and a heavy administrative workload in a rigid organizational structure (Collins & Gibbs, Citation2003; Gershon, Barocas, Canton, Li, & Vlahov, Citation2009; McCarty, Zhao, & Garland, Citation2007; Violanti & Marshall, Citation1983). These demands represent stressors, suggesting that daily routine police work is a risk factor for chronic stress (Dantzer, Citation1987). Since chronic stress has consistently been associated with negative health outcomes, it is not surprising that police officers are at a high risk of stress-related physical (e.g. hypertension, heart disease, pain, etc.) and mental health problems (Aamodt, Citation2008; Arter, Citation2008; Austin-Ketch et al., Citation2012), including PTSD and depression (Alkus & Padesky, Citation1983; Lilly, Pole, Best, Metzler, & Marmar, Citation2009; Meffert et al., Citation2008; Violanti et al., Citation2007).
Past research has identified low subjective social status (SSS) as a risk factor for elevated stress (Adler, Epel, Castellazzo, & Ickovics, Citation2000) and health problems (Habersaat, Geiger, Abdellaoui, & Wolf, Citation2015; Singh-Manoux, Marmot, & Adler, Citation2005). SSS is typically defined as one’s perceived position relative to the self-defined groups ‘country’ and ‘community’ (MacArthur ladders: Adler et al., Citation2000). However, more recent work has examined modified versions of this instrument showing that SSS related to social groups defined more proximally (e.g. colleagues) were more strongly related to health-relevant outcomes, specifically subjective well-being, than status among more distal social groups (e.g. country; Anderson, Kraus, Galinsky, & Keltner, Citation2012).
Law enforcement not only is a high-stress occupation with increased health risks (Austin-Ketch et al., Citation2012; Collins & Gibbs, Citation2003; Dantzer, Citation1987; Gershon et al., Citation2009), but the police force is a highly hierarchical and cohesive organization with members showing strong self-identification with their role. As such, an officer’s perceived social standing within the police force may be a particularly interesting indicator of health, as perceiving higher status in the police does not protect against being exposed to the same risk factors as officers who perceive their status to be low. Recent work has supported this idea (Habersaat et al., Citation2015), raising the question regarding the mechanisms underlying the link between SSS and health in this particular population.
Stress has been consistently discussed as an important mediator between low subjective social status and negative health outcomes (Adler et al., Citation2000). Specifically, exposure to chronic stress has been shown to be associated with dysfunctions of the autonomic nervous system (ANS) (Strahler, Berndt, Kirschbaum, & Rohleder, Citation2010; Vigil, Geary, Granger, & Flinn, Citation2010; JM Wolf, Nicholls, & Chen, Citation2008), which in turn have been linked to negative health outcomes, including depression and post-traumatic stress (Charkoudian & Rabbitts, Citation2009; Mahfoud et al., Citation2011; Schwartz & De Ferrari, Citation2011; Stetler & Miller, Citation2011; Wessa, Rohleder, Kirschbaum, & Flor, Citation2006; OT Wolf, Citation2008). While previous studies confirmed links between status in the police and ANS indicators in the context of exposure to an acute laboratory stressor (Akinola & Mendes, Citation2013) and between status in the police, perceived stress and sleep quality (Charles et al., Citation2011), we are not aware of any study examining ANS functioning as an important link between SSS and chronic stress-related health outcomes in the high-risk population of police officers.
One reason for the scarcity of studies is that ANS assessment typically implies equipment and processing-intensive procedures in a laboratory setting (e.g. electrocardiogram) or invasive and restrictive procedures (e.g. repeated blood sampling). However, recently, salivary α-amylase (sAA) has emerged as a noninvasive and ambulatory marker of ANS activity (Nater & Rohleder, Citation2009). Subsequent studies supported the role of basal sAA activity as a health marker, such that a higher basal sAA activity was associated with traumatic situations (Vigil et al., Citation2010), depression symptoms (Ishitobi et al., Citation2010) and hypertension (Strahler, Kirschbaum, & Rohleder, Citation2011). Likewise, altered sAA levels at awakening were related with posttraumatic stress (Thoma, Joksimovic, Kirschbaum, Wolf, & Rohleder, Citation2012). Together, these studies suggest that a higher basal sAA is related to more negative health outcomes. However, to date, studies simultaneously capturing the various circadian components of basal sAA activity and identifying potential differential links to mental and physical health are still missing, both in the general population as well as in a law enforcement context.
The current study aimed at assessing basal sAA activity to test ANS functioning as a pathway linking subjective social status and health outcomes (i.e. stress-related physical symptoms, depression and post-traumatic stress symptoms) in a chronically stressed and high-risk population. In more detail, the aims were (1) to characterize basal sAA activity patterns in a group of Swiss police officers; (2) to identify the role of SSS relative to both distal (e.g. country) and proximal groups (e.g., police) as a potential determinant of basal sAA activity dysfunctions; and lastly, (3) to replicate previously described links between health outcomes and basal sAA activity.
Method
Participants
A total of 101 participants were recruited from a state police department in Switzerland. All participants were French-speaking Swiss nationals. Officers who were taking medication that could interfere with saliva collection or affect the ANS, such as medication for hypertension and diabetes type II (n = 7) were excluded from participation. Among those eligible, 12 participants dropped out before the end of the study (attrition rate = 88%) and 14 were excluded due to failure to return questionnaires or due to multiple missing data. After exploratory analyzes on sAA, 10 participants were identified as outliers (either positive or negative) or did not comply with saliva collection procedures and were excluded. Finally, multivariate analyzes identified two additional outliers who were also removed from analyses. The final sample was therefore composed of 56 police officers. Importantly, participants included and excluded were comparable in terms of socio-demographic factors ().
Table 1. Sociodemographic data of included and excluded participants.
The study was approved by the Ethics Commission for Studies in Humans in Lausanne, Switzerland, the Institutional Review Board at Brandeis University, police administration, as well as police labor unions. Participants provided a written informed consent. Data were identified with participant numbers only and consent forms containing the participants’ signature were stored separately from the data. None of the data collected were shared with the police administration or anyone else besides study personnel. Participation was not compensated.
Procedure
Police officers were recruited through the office of psychological services of the state police via emails and flyers displayed throughout the police department. Interested officers scheduled their study participation on the department’s intranet. Data collection took place over the course of one month (July 2014) in the police department, during duty time, in the administrative floor in a private and confidential area. During the first one-on-one appointment, the objectives and procedures of the study were explained, any questions or concerns addressed and written consent collected. Participants then underwent a 20-min interview collecting socio-demographic information as well as information concerning medication use, health, smoking, substances use, and physical symptoms. Subsequently, participants were asked to complete a set of questionnaires assessing symptoms of post-traumatic stress and depression and subjective social status. Participants then received 12 Salivettes® (Sarstedt, Rommelsdorf, Germany) for saliva samples collection over the course of two days (6 samples per day, at least 2 days after the last nightshift), a booklet of instructions for saliva sampling and a diary to report exact time of saliva collection as well as specific events occurring during the day (e.g. exercise, stress, smoking). In case of current antibiotic or analgesic medication intake, saliva sampling was postponed until after recovery. The participants were instructed to keep saliva samples in the fridge until handing them back to the research team (Habersaat et al., Citation2015).
Measures
Sociodemographic measures
The MacArthur Scales of Subjective Social Status (SSS; Adler et al., Citation2000) consist of two ladder measures assessing participants’ perceived position in the social hierarchy. Participants place an ‘X’ on the ladder rung from 1 to 10 where they feel they stand, with higher rungs representing higher status. One ladder asks participants to rate their status relative to the country as a whole, with those at the top of the ladder being those with the most money, best jobs and most education. In the other ladder, participants rate themselves compared to their community, defined as whatever is most meaningful to them. The current study added two additional ladders asking participants to rate their perceived social status compared to the police as a whole and compared to their friends using language from the community ladder. In previous research, SSS has been shown to predict health outcomes independent of socioeconomic status (Adler et al., Citation2000; Singh-Manoux, Adler, & Marmot, Citation2003) and to have adequate test-retest reliability at six-month follow-up (ρ = .62, p < .01; Operario, Adler, & Williams, Citation2004).
Health measures
The Cohen–Hoberman Inventory of Physical Symptoms (CHIPS; Cohen, Kamarck, & Mermelstein, Citation1983) is a list of 33 common physical symptoms (e.g. back pain, headache). Each item is rated on how much each symptom bothered the individual during the past two weeks on a 0 (‘not at all’) to 4 (‘extremely’) scale. A total score is computed by summing items, with scores ranging from 0 to 132. The inventory is reliable (in the present study Cronbach’s α = .83) and positively correlated with use of health facilities in the following seven weeks (Cohen et al., Citation1983).
The Mississippi Scale – Police version (MIS; Lilly et al., Citation2009) is a validated adaptation (in the present study Cronbach’s α = .82) of the Mississippi Scale for Combat-Related Posttraumatic Stress Disorder (Keane, Caddell, & Taylor, Citation1988). Respondents rated 35 items describing PTSD-related symptoms such as ‘If someone pushes me too far, I am likely to become violent’, on a Likert-type scale from 1 (not at all true) to 5 (extremely true). Items are summed to compute a cumulative PTSD symptom severity score.
The Beck Depression Inventory – Short Form (BDI-SF; Beck, Steer, & Brown, Citation1996) is a 13-item version of the Beck Depression Inventory questionnaire measuring severity of depression symptoms according to DSM-IV criteria for depression. Participants rate symptoms on a 0 (absent) to 3 (very often) scale of intensity. Sum scores range from 0 to 39, with higher scores indicating more severe depressive symptoms. Scores of ten and higher indicate high depression (sensitivity = 100% and specificity = 83.1%; Furlanetto, Mendlowicz, & Bueno, Citation2005). The present study used the validated French version (Bourque & Beaudette, Citation1982), for which test–retest procedure indicated adequate stability over a 4-month period and internal consistency was high (Cronbach’s α = .90). In the present study, the reliability was acceptable (Cronbach’s α = .68).
Salivary α-amylase
Alpha-amylase concentrations in saliva were determined as indicators of ANS functioning. For that, saliva was collected by asking participants to place a dental cotton roll provided in a plastic container (Salivettes®, Sarstedt AG, Germany) into their mouth and moving it in a circular pattern for 2 minutes to ensure collection of saliva from all glands (Decaro, Citation2008; Rohleder & Nater, Citation2009). Each participant collected saliva samples during 2 days (6 samples per day: directly after awakening, 15 and 30 min after awakening, just before mealtime at midday, just before mealtime in the evening and before going to bed) (Pruessner et al., Citation1997). Each exact time of saliva collection was reported in a diary. Participants were instructed not to eat, drink beverages with sugar or providing energy (e.g. coffee: Bishop, Walker, Scanlon, Richards, & Rgers, Citation2006), smoke or brush teeth at least one hour prior to saliva collection.
Saliva samples were sent by express airmail to the Laboratory for Biological Health Psychology of the Brandeis University (Waltham, MA). Alpha-amylase has been shown to be stable at room temperature for at least a period of for 96 h (Granger et al., Citation2006) and was shown to be flow-rate independent (Granger et al., Citation2006; Vining, McGinley, & Symons, Citation1983). Upon arrival, saliva was extracted by centrifugation at 2000 rpm for 5 min, transferred into deep-well plates and stored at −30 °C until assayed (Kahn, Rubinow, Davis, Kling, & Post, Citation1988; Vining et al., Citation1983). Salivary α-amylase activity was measured according to the procedure described by Rohleder, Wolf, Maldonado, and Kirschbaum (Citation2006). In short, duplicates of 20 µl of standards and diluted saliva (1:625) were incubated with 50 µl of substrate reagent (Roche Diagnostics, Mannheim, Germany) in a water bath at 47 °C for 3 min. Optical density was measured at 405 nm. After a second incubation (5 min at 47 °C) and measurements, increases in absorbance were calculated and transformed to α-amylase concentrations (U/ml) using a linear regression calculated for each micro-plate (inter- and intra-assay variation <10%).
Ancillary variables
Information on age, gender, body mass index (BMI, kg/m2), smoking status, marital status, number of children, years of police service and police divisions (Community, Emergency and Criminal) were collected. Specifically, BMI, smoking status and police divisions were considered as potential confounding variables in target analyses, as they may influence sAA activity or had been shown to influence health outcomes in previous investigations on this sample (Habersaat et al., Citation2015). Furthermore, controlling for police division allowed for addressing systematic differences in shiftwork schedules.
Analytical plan
First, socio-demographic characteristics of included and excluded participants were compared using χ2 tests for categorical or nominal variables and Student’s t-tests for continuous variables (). Next, distribution of α-amylase levels as well as SSS and health variables () were assessed and outliers were identified. In order to test for possible confounders, all variables of interest were compared across gender using Mann–Whitney U-tests. A GLM repeated measures was used to compare ratings on the four SSS ladders. The associations between sAA diurnal activity and subjective social status (in the community, in the country, among friends and in the police) as well as between sAA diurnal activity and health variables (physical symptoms, depression and posttraumatic stress symptoms) were investigated with hierarchical multilevel regression analyes (HLM 7, SSI Inc., Skokie, IL). Smoking status (0 = no; 1 = yes), BMI and police division (community, emergency and criminal, coded as two dummy variables) were controlled.
Table 2. Descriptive information of self-reported status and health (individual/level 2 variables).
Two 2-level (uncentred factors) models were computed separately in order to avoid type-II error due to the moderate sample size. For both models, level 1 (occasion level measurement) included sAA activity measurements, saliva collection times (in minutes relative to the first assessment) and day, and level 2 (individual level) introduced control variables (i.e. BMI, police division, smoking). The first model tested the link between SSS and sAA:
Level 1: sAA = β00 + β01*(time) + β02*(day) + E
Level 2: β0j = β00 + β01*(BMI) + β02*(smoke) + β03*(police division dummy 1) + β04*(police division dummy 2) + β05*(SSS Country) + β06*(SSS Community) + β07*(SSS Friends) + β08*(SSS Police) + R0
A similarly constructed second model tested the link between sAA and health symptoms (physical symptoms: CHIPS; depressive symptoms: BDI; PTSD symptoms: MIS).
Level 1: sAA = β00 + β01*(time) + β02*(day) + E
Level 2: β0j = β00 + β01*(BMI) + β02*(smoke) + β03*(police division dummy 1) + β04*(police division dummy 2) + β05*(physical symptoms) + β06*(depression symptoms) + β07*(PTSD symptoms) + R0
Residuals distributions were screened and two outliers identified in this step were removed and analyses were rerun (see participant section above; final sample: n = 56).
Results
Descriptive analysis
Descriptive information on SSS measures as well as health indicators are summarized in . No significant differences were found between men and women in terms of SSS, physical, depression and post-traumatic stress symptoms (all p’s > .16; except second sAA sample on day 2: p = .033). Means for SSS relative to country, community and friends were all over the theoretical mean (>5), while subjective status relative to the police was below the theoretical mean (<5). A GLM assessing all four SSS ladders as repeated measures confirmed that ratings across the ladders were significantly different (F(3) = 32.51; p < .001; ɳ2p = .37), with SSS in the police rated significantly lower (all p’s < .001) and SSS among friends rated significantly higher (all p’s < .005) than the three other SSS ladder ratings.
In terms of health outcomes, police officers reported low depression, but moderate to high post-traumatic stress and physical symptoms (no mean over the clinical range). In line with this mental health pattern, PTSD symptoms were negatively (significantly and at a trend level) associated with all four status indices (−.23 ≤ r ≤ −.44, all p’s ≤ .089; ), while depressive symptoms were only linked to SSS in the community (r= −.33, p=.014; all other SSS ladders: r’s ≤ −.16, p’s ≥ .10). Again, only lower status in the community was at the trend level associated with more physical symptoms (r= −.24, p = .076; all other SSS ladders: r’s ≤ −.22, p’s ≥ .10).
Table 3. Saliva α-amylase activity (U/ml) and collection times (hrs) over two days.
Salivary α-amylase activity levels were very consistent across the two assessment days (.39 ≤ r ≤ .74, all p’s ≤ .003) and showed the expected pattern of decreasing levels over the first hour after wake-up, subsequently high levels for the remainder of the day, and slight decreases towards bedtime ().
Multilevel regressions
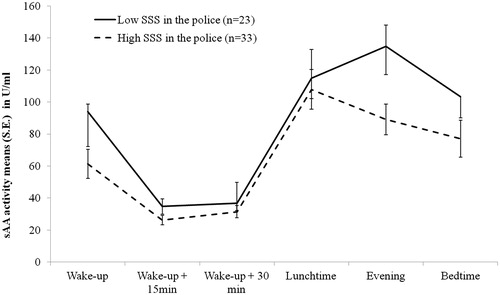
To address the study aims, first, multilevel regression was used to investigate potential differential links between SSS measures and basal sAA activity (see equation in analytical plan section). Results revealed that specifically SSS in the police explained a significant portion of sAA activity variance (β08 = −7.89; p = .044, Cohen’s d = .28, confidence interval (CI) at 95%: −14.15–1.63; ). In more detail, individuals with lower SSS in the police began their day with a higher sAA level followed by a steep decrease and higher levels during the second part of the day, compared to individuals with higher SSS in the police.
Figure 1. Illustration of alpha-amylase activity by time according to high versus low subjective social status (SSS) in the police.
To test for associations between basal sAA activity and health outcomes, a second model was computed including physical (CHIPS), depressive (BDI) and PTSD symptoms (MIS) in the second level. Results revealed that physical symptoms only (β05 = 2.26; p = .021, Cohen’s d = .31, CI at 95%: 0.66–3.83) explained a significant portion of the variance in sAA activity () such that individuals with a higher CHIPS score, that is, more physical symptoms, had higher sAA levels throughout the day compared to individuals with lower CHIPS scores.
Figure 2. Illustration of alpha-amylase activity by time according to high versus low levels of physical problems (CHIPS).
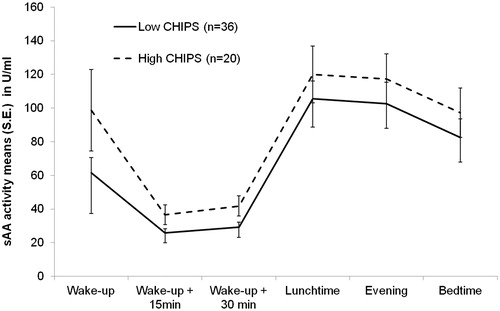
Both and are illustrations of the multilevel analysis findings. SSS in the police and CHIPS scores were binned according to their means in low versus high groups. Alpha-amylase scores were averaged over the two days without taking the exact time of collection into account. BMI, Police Divisions and Smoking Status were not controlled in those figures. Therefore, both figures are only illustrations and do not represent the exact output of the multilevel analyzes.
Discussion
The current study set out to investigate the health relevance of SSS relative to different social groups in police officers with a focus on basal sAA activity as a chronic stress indicator. Overall, subjective social status ratings relative to nonwork social groups increased with proximity, while status ratings in the police were lowest. However, only status among the police was differentially linked to sAA activity patterns, with police officers reporting lower status showing higher sAA activity throughout the day. Overall elevated sAA activity levels were furthermore associated with more physical health symptoms.
Status ratings are differentially linked to salivaryalpha-amylase activity
First, our findings support the idea that SSS ratings vary considerably depending on the reference group. More specifically, in the current study population of Swiss police officers, status ratings increased with proximity, that is, from status in the country to status in the community to the highest ratings being for status among friends. This pattern, however, did not hold true for status ratings among the police. Here, officers reported even lower standing than compared to the entire population of the country. Interestingly, status ratings relative to the country have consistently been reported to most closely reflect actual socioeconomic status (Ghaed & Gallo, Citation2007). Thus, it is possible that, in a very hierarchical structure in which roles are clearly defined, differences between subjective and objective social statuses are reduced, such that officers with a perceived lower status actually have a lower position in the police hierarchy. Importantly, position in the police hierarchy determines work environment and type of tasks. For example, officers with a lower position in the police hierarchy are usually working in the field, while officers with a higher status tend to do more administrative work. As a consequence, stressors police officers are exposed to may vary considerably (Brown & Campbell, Citation1990). Previous research further points to associated differences in physiological stress responses, with higher SSS in the police being related to more adaptive regulatory strategies in stressful situations (Akinola & Mendes, Citation2013). The current findings suggest that status among the police, and thus, type of stressors experienced may also differentially influence basal sAA activity. It could be speculated that unpredictable and frequent stressors associated with lower position tasks may lead to more chronic activation of stress systems, which over time is reflected in elevated basal sAA activity during the day observed among officers reporting lower subjective status in the police compared to those officers reporting higher status.
Interestingly, this appears to be specific to status ratings among the police, as no associations were found between sAA activity and subjective social status ratings related to country, community, or friends. Perhaps social status among the police not only encompasses some components of objective socioeconomic status, but given the highly cohesive social work environment, police status may also capture some of the more salient aspects of an individual’s status in their community and friends as well. Others have suggested that status among close social groups with whom one has frequent face-to-face contact have the potential to be most relevant for health (Anderson et al. (Citation2012). As such, the likelihood for social status to impact stress-related physiological processes may have been the highest for status ratings concerning the police as reference group. To test for such integration of multiple references, future studies may include qualitative reports of information individuals think about when defining their reference groups.
Diurnal salivary alpha-amylase activity is differentially linked to health outcomes
Next, we assessed the health relevance of differences in diurnal sAA activity patterns and observed a significant link between diurnal sAA activity and physical symptoms. More specifically, police officers with a higher level of physical symptoms showed systematically higher sAA levels compared to police officers with a lower level of physical symptoms. This finding replicates previous reports of associations between ANS indices (higher resting heart rate) and physical problems, including cardiovascular disease, coronary heart disease and cancer (Greenland et al., Citation1999) as well as somatic complaints (McFarlane, Atchison, Rafalowicz, & Papay, Citation1994). In contrast, no associations were observed between diurnal sAA activity and psychological symptoms, despite earlier findings of positive relationships between basal sAA activity and depressive symptoms as well as post-traumatic stress symptoms (Ishitobi et al., Citation2010; Vigil et al., Citation2010). One reason for these contrasting findings may be that police officers in the current study reported generally low levels of depressive symptoms and a heterogeneous pattern of post-traumatic stress symptoms. It may be that dysfunctions in basal sAA activity only become apparent at clinically relevant symptom severity. To test this hypothesis, future studies should include police officers suffering from diagnosed mental disorders.
Limitations
This study has multiple strengths such as a homogeneous sample of police officers exposed to the same work environment, objective stress measures and is the first study to consider SSS as having an impact on health-relevant stress mechanisms. However, findings of the current study have to be considered in light of several limitations. First, participants taking medication impacting sAA activity levels were excluded from the present analyses. However, excluded and included participants were comparable in terms of sociodemographic variables, and diurnal sAA activity profiles were nevertheless linked specifically with physical symptoms. Second, although a sample size above 50 is considered sufficient to conduct multilevel regression analyses (Hox, Citation2002), Van der Leeden and Busing (Citation1994) recommended an overall number of observations of 900 (according to level and data points). Our sample encompassed 672 observations (56*12) and had a small effect size (Cohen’s d 0.28–0.31), suggesting low power. As a consequence, the current results should be considered preliminary. Third, the cross-sectional design did not allow for a causal interpretation of the results. For example, physical symptoms may influence ANS functioning or ANS dysfunctions may result in physical symptoms, although previous literature suggests the latter (Greenland et al., Citation1999). A fourth limitation is the possibility of a selection bias, such that only very stressed police officers had an interest to take part in the study. On the other hand, highly stressed officers may also have felt that they did not have enough time to take part in the study, thus potentially balancing out the former issue. Similarly, it is possible that participants who were excluded from the analyses were higher in symptoms than those included. Fifth, given the nature of the occupation, it was not possible to control all aspects of data collection. Particularly differences in time of day questionnaire data were collected could have affected, for example, perception or reporting of health symptoms. Although we adhered to recommendations for controlling potential sAA confounds (physical effort, situational stress), sAA levels can be influenced by a multitude of factors. Therefore, we cannot exclude that factors other that those controlled in the current study may have introduced noise to the sAA measures. Finally, despite assurance of confidentiality regarding participation and anonymity of the data collected, as well as the encouragement of the police management, the study took place in the police department building, which may have discouraged some officers from participating.
Conclusions
Taken together, results of the current study suggest that subjective social status referencing one’s work environment may be a promising early indicator of health-relevant changes in stress-related physiological systems. These changes presented as generally elevated diurnal salivary α-amylase activity, that is, potential ANS dysfunction. Future studies will have to determine to what extent the proposed processes are solidified in the context of physical diseases and whether similar associations will be found for clinically relevant levels of mental health symptoms.
Acknowledgements
The authors wish to thank the representatives of the police unions, as well as the police management (psychological office, human resources and top management) who promoted and supported this study. We are grateful to all police officers who took the time to participate in the study and gave us this valuable information. The authors would also like to thank Professor Andre Kuhn at the Swiss-French Center for Research in Criminology, University of Neuchâtel, Switzerland, Professor Serge Guimond at the Laboratory for Social Psychology, University Blaise Pascal, France, as well as Professor Raymund Schwan at the University of Lorraine, France, for their valuable support during the course of this study. The study was approved by the Ethics Commission in the State of Vaud, Switzerland, and Brandeis University IRB.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Aamodt, M.G. (2008). Reducing misconceptions and false beliefs in police and criminal psychology. Criminal Justice and Behavior, 35, 1231–1240. doi: 10.1177/0093854808321527
- Adler, N.E., Epel, E.S., Castellazzo, G., & Ickovics, J.R. (2000). Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy, White women. Health Psychology, 19, 586. doi: 10.1037/0278-6133.19.6.586
- Akinola, M., & Mendes, W.B. (2013). It's good to be the king neurobiological benefits of higher social standing. Social Psychological and Personality Science, 4, 43–51. doi: 10.1177/1948550613485604
- Alkus, S., & Padesky, C. (1983). Special problems of police officers: stress-related issues and interventions. Counseling Psychologist, 11, 55–64. doi: 10.1177/0011000083112010
- Anderson, C., Kraus, M.W., Galinsky, A.D., & Keltner, D. (2012). The local-ladder effect social status and subjective well-being. Psychological Science, 23, 764–771. doi: 10.1177/0956797611434537
- Arter, M.L. (2008). Stress and deviance in policing. Deviant Behavior, 29, 43–69. doi: 10.1080/01639620701457774
- Austin-Ketch, T.L., Violanti, J.M., Fekedulegn, D., Andrew, M.E., Burchfield, C.M., & Hartley, T.A. (2012). Addictions and the criminal justice system, what happens on the other side? Post-traumatic stress symptoms and cortisol measures in a police cohort. Journal of Addictions Nursing, 23, 22–29. doi: 10.3109/10884602.2011.645255
- Beck, A.T., Steer, R.A., & Brown, G.K. (1996). Beck depression inventory-II. San Antonio, Texas: Psychological Corporation.
- Bishop, N.C., Walker, G.J., Scanlon, G.A., Richards, S., & Rgers, E. (2006). Salivary IgA responses to prolonged intensive exercice following caffeine ingestion. Medicine and Science in Sports and Exercise, 38, 513–519. doi: 10.1249/01.mss.0000187412.47477.ee
- Bourque, P., & Beaudette, D. (1982). Psychometric study of the Beck Depression Inventory used on a sample of French-speaking university students. Canadian Journal of Behavioral Science, 14, 211–218. doi: 10.1037/h0081254
- Brown, J.M., & Campbell, E.A. (1990). Sources of occupational stress in the police. Work and Stress, 4, 305–318. doi: 10.1080/02678379008256993
- Charkoudian, N., & Rabbitts, J.A. (2009). Sympathetic neural mechanisms in human cardiovascular health and disease. Mayo Clinic Proceedings, 84, 822–830. doi: 10.4065/84.9.822
- Charles, L.E., Slaven, J.E., Mnatsakanova, A., Ma, C., Violanti, J.M., Fekedulegn, D., … Burchfiel, C.M. (2011). Association of perceived stress with sleep duration and sleep quality in police officers. International Journal of Emergency Mental Health, 13, 229.
- Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385–396. doi: 10.2307/2136404
- Collins, P.A., & Gibbs, A.C.C. (2003). Stress in police officiers: A study on the origins, prevalence and severity of stress-related symptoms within a county police force. Occupational Medicine, 53, 256–264. doi: 10.1093/occmed/kqg061
- Dantzer, M.L. (1987). Police-related stress: A critique for future research. Journal of Police and Criminal Psychology, 3, 43–48. doi: 10.1007/BF02806523
- Decaro, J.A. (2008). Methodological considerations in the use of salivary alpha-amylase as a stress marker in field research. American Journal of Human Biology, 20, 617–619. doi: 10.1002/ajhb.20795
- Furlanetto, L.M., Mendlowicz, M.V., & Bueno, J.R. (2005). The validity of the Beck Depression Inventory-Short Form as a screening and diagnostic instrument for moderate and severe depression in medical inpatients. Journal of Affective Disorders, 86, 87–91. doi: 10.1016/j.jad.2004.12.011
- Gershon, R.R.M., Barocas, B., Canton, A.N., Li, X., & Vlahov, D. (2009). Mental, physical, and behavioral outcomes associated with perceived work stress in police officers. Criminal Justice and Behavior, 36, 275–289. doi: 10.1177/0093854808330015
- Ghaed, S.G., & Gallo, L.C. (2007). Subjective social status, objective socioeconomic status, and cardiovascular risk in women. Health Psychology, 26, 668. doi: 10.1037/0278-6133.26.6.668
- Granger, D.A., Kivlighan, K.T., Blair, C., El-Sheikh, M., Mize, J., Lisonbee, J.A., … Schwartz, E.B. (2006). Integrating the measurement of salivary α-amylase into studies of child health, development, and social relationships. Journal of Social and Personal Relationships, 23, 267–290. doi: 10.1177/0265407506062479
- Greenland, P., Daviglus, M.L., Dyer, A.R., Liu, K., Huang, C.F., Goldberger, J.J., & Stamler, J. (1999). Resting heart rate is a risk factor for cardiovascular and noncardiovascular mortality: The Chicago Heart Association Detection Project in Industry. American Journal of Epidemiology, 149, 853–862. doi: 10.1093/oxfordjournals.aje.a009901
- Habersaat, S.A., Geiger, A.M., Abdellaoui, S., & Wolf, J.M. (2015). Health in police officers: Role of risk factor clusters and police divisions. Social Science and Medicine, 143, 213–222. doi: 10.1016/j.socscimed.2015.08.04
- Hox, J. (2002). Multilevel analysis: Techniques and applications. Mahwah, New Jersey: Lawrence Erlbaum.
- Ishitobi, Y., Akiyoshi, J., Tanaka, Y., Ando, T., Okamoto, S., Kanehisa, M., … Tsuru, J. (2010). Elevated salivary α-amylase and cortisol levels in unremitted and remitted depressed patients. International Journal of Psychiatry in Clinical Practice, 14, 268–273. doi: 10.3109/13651501.2010.500737
- Kahn, J.P., Rubinow, D.R., Davis, C.L., Kling, M., & Post, R.M. (1988). Salivary cortisol: A practical method for evaluation of adrenal function. Biological Psychiatry, 23, 335–349. doi: 10.1016/0006-3223(88)90284-3
- Keane, T.M., Caddell, J.M., & Taylor, K.L. (1988). Mississippi scale for combat-related posttraumatic stress disorder: Three studies in reliability and validity. Journal of Consulting and Clinical Psychology, 56, 85–90. doi: 10.1037/0022-006X.56.1.85
- Lilly, M.M., Pole, N., Best, S.R., Metzler, T., & Marmar, C.R. (2009). Gender and PTSD: What can we learn from female police officers?. Journal of Anxiety Disorders, 23, 767–774. doi: 10.1016/j.janxdis.2009.02.015
- Mahfoud, F., Schlaich, M., Kindermann, I., Ukena, C., Cremers, B., Brandt, M.C., … Sobotka, P.A. (2011). Effect of renal sympathetic denervation on glucose metabolism in patients with resistant hypertension: A pilot study. Circulation, 123, 1940–1946. doi: 10.1161/CIRCULATIONAHA.110.991869
- McCarty, W.P., Zhao, J.S., & Garland, B.E. (2007). Occupational stress and burnout between male and female police officers: Are there any gender differences?. Policing: An International Journal of Police Strategies & Management, 30, 672–691. doi: 10.1108/13639510710833938
- McFarlane, A.C., Atchison, M., Rafalowicz, E., & Papay, P. (1994). Physical symptoms in post-traumatic stress disorder. Journal of Psychosomatic Research, 38, 715–726. doi: 10.1016/0022-3999(94)90024-8
- Meffert, S.M., Metzler, T., Henn-Haase, C., McCaslin, S.E., Inslicht, S.S., Chemtob, C., … Marmar, C.R. (2008). A prospective study of trait anger and PTSD symptoms in police. Journal of Traumatic Stress, 21, 410–416. doi: 10.1002/jts.20350
- Nater, U.M., & Rohleder, N. (2009). Salivary alpha-amylase as a non-invasive biomarker for the sympathetic nervous system. Psychoneuroendocrinology, 34, 486–496. doi: 10.1016/j.psyneuen.2009.01.014
- Operario, D., Adler, N.E., & Williams, D.R. (2004). Subjective social status: Reliability and predictive utility for global health. Psychology and Health, 19, 237–246. doi: 10.1080/08870440310001638098
- Pruessner, J.C., Wolf, O.T., Hellhammer, D.H., Buske-Kirschbaum, A., von Auer, K., Jobst, S., … Kirschbaum, C. (1997). Free cortisol levels after awakening: A reliable biological marker for the assessment of adrenocortical activity. Life Sciences, 61, 2539–2549. doi: 10.1016/S0024-3205(97)01008-4
- Rohleder, N., & Nater, U.M. (2009). Determinants of salivary alpha-amylase in humans and methodological considerations. Psychoneuroendocrinology, 34, 469–485. doi: 10.1016/j.psyneuen.2008.12.004
- Rohleder, N., Wolf, J.M., Maldonado, E.F., & Kirschbaum, C. (2006). The psychosocial stress-induced increase in salivary alpha-amylase is independant of saliva flow rate. Psychophysiology, 43, 645–652. doi: 10.1111/j.1469-8986.2006.00457.x
- Schwartz, P.J., & De Ferrari, G.M. (2011). Sympathetic–parasympathetic interaction in health and disease: abnormalities and relevance in heart failure. Heart Failure Reviews, 16, 101–107. doi: 10.1007/s10741-010-9179-1
- Singh-Manoux, A., Adler, N.E., & Marmot, M.G. (2003). Subjective social status: its determinants and its association with measures of ill-health in the Whitehall II study. Social Science and Medicine, 56, 1321–1333. doi: 10.1016/S0277-9536(02)00131-4
- Singh-Manoux, A., Marmot, M.G., & Adler, N.E. (2005). Does subjective social status predict health and change in health status better than objective status?. Psychosomatic Medicine, 67, 855–861. doi: 10.1097/01.psy.0000188434.52941.a0
- Stetler, C., & Miller, G.E. (2011). Depression and hypothalamic-pituitary-adrenal activation: a quantitative summary of four decades of research. Psychosomatic Medicine, 73, 114–126. doi: 10.1097/PSY.0b013e31820ad12b
- Strahler, J., Berndt, C., Kirschbaum, C., & Rohleder, N. (2010). Aging diurnal rhythms and chronic stress: Distinct alteration of diurnal rhythmicity of salivary α-amylase and cortisol. Biological Psychology, 84, 248–256. doi: 10.1016/j.biopsycho.2010.01.019
- Strahler, J., Kirschbaum, C., & Rohleder, N. (2011). Association of blood pressure and antihypertensive drugs with diurnal alpha-amylase activity. International Journal of Psychophysiology, 81, 31–37. doi: 10.1016/j.ijpsycho.2011.04.002
- Thoma, M.V., Joksimovic, L., Kirschbaum, C., Wolf, J.M., & Rohleder, N. (2012). Altered salivary alpha-amylase awakening response in Bosnian War refugees with posttraumatic stress disorder. Psychoneuroendocrinology, 37, 810–817. doi: 10.1016/j.psyneuen.2011.09.013
- Van der Leeden, R., & Busing, F.M. (1994). First iteration versus final IGLS/RIGLS estimators in two-level models: A Monte Carlo study with ML3. Department of Psychology, University of Leiden.
- Vigil, J.M., Geary, D.C., Granger, D.A., & Flinn, M.V. (2010). Sex differences in salivary cortisol, alpha‐amylase, and psychological functioning following Hurricane Katrina. Child Development, 81, 1228–1240. doi: 10.1111/j.1467-8624.2010.01464.x
- Vining, R.F., McGinley, R.A., & Symons, R.G. (1983). Hormones in saliva: mode of entry and consequent implications for clinical interpretation. Clinical Chemistry, 29, 1752–1756.
- Violanti, J.M., Andrew, M., Burchfiel, C.M., Hartley, T.A., Charles, L.E., & Miller, D.B. (2007). Post-traumatic stress symptoms and cortisol patterns among police officers. Policing: An International Journal of Police Strategies & Management, 30, 189–202. doi: 10.1108/13639510710753207
- Violanti, J.M., & Marshall, J.R. (1983). The police stress process. Journal of Police Science and Administration, 11, 389–394.
- Wessa, M., Rohleder, N., Kirschbaum, C., & Flor, H. (2006). Altered cortisol awakening response in posttraumatic stress disorder. Psychoneuroendocrinology, 31, 209–215. doi: 10.1016/j.psyneuen.2005.06.010
- Wolf, J.M., Nicholls, E., & Chen, E. (2008). Chronic stress, salivary cortisol, and α-amylase in children with asthma and healthy children. Biological Psychology, 78, 20–28. doi: 10.1016/j.biopsycho.2007.12.004
- Wolf, O.T. (2008). The influence of stress hormones on emotional memory: Relevance for psychopathology. Acta Psychologica, 127, 513–531. doi: 10.1016/j.actpsy.2007.08.002