
Abstract
Stress can impair T cell-mediated immunity. To determine if infants with high stress responses had deficits in T-cell mediated immunity, we examined the association of pain-induced cortisol responsiveness with thymic function and vaccine responses in infants. This study was performed among 306 (male = 153 and female = 153) participants of a randomized, controlled trial examining the effect of neonatal vitamin A supplementation on immune function in Bangladesh (NCT01583972). Salivary cortisol was measured before and 20 min after a needle stick (vaccination) at 6 weeks of age. The thymic index (TI) was determined by ultrasonography at 1, 6, 10 and 15 weeks. T-cell receptor excision circle and blood T-cell concentrations were measured at 6 and 15 weeks. Responses to Bacillus Calmette–Guérin (BCG), tetanus toxoid, hepatitis B virus and oral poliovirus vaccination were assayed at 6 and 15 weeks. Cortisol responsiveness was negatively associated with TI at all ages (p < .01) in boys only, was negatively associated with naïve helper T-cell concentrations in both sexes at both 6 (p = .0035) and 15 weeks (p = .0083), and was negatively associated with the delayed-type hypersensitivity (DTH) skin test response to BCG vaccination at 15 weeks (p = .034) in both sexes. Infants with a higher cortisol response to pain have differences in the T-cell compartment and a lower DTH response to vaccination. Sex differences in the immune system were seen as early as 6 weeks of age in these healthy infants.
Introduction
Cortisol, a glucocorticoid hormone, affects the health and functioning of multiple organ systems, including the immune system, and is one of the mediators of stress-induced immune-suppression (Webster Marketon & Glaser, Citation2008). Such immune-suppression affects both the innate and adaptive components of the immune system. The thymus, a key component of adaptive immunity, is particularly affected by cortisol, which causes apoptotic death of thymocytes (Cohen, Citation1992; Nieto, Gonzalez, Gambon, Diaz-Espada, & Lopez-Rivas, Citation1992). This apoptosis presumably accounts for the negative association seen between elevated cortisol and lower thymic output of naïve T-cells (measured by analysis of T-cell receptor excision circles [TREC] in blood) in adults (Benjamin et al., Citation2016) and between elevated cortisol and smaller thymus size in very-low birthweight infants (de Felice et al., Citation2008) suggesting a constant, negative effect of elevated cortisol on thymic function across the lifespan. Unlike thymocytes, peripheral-blood T-cells are resistant to cortisol-induced apoptosis (Nieto et al., Citation1992) but cortisol infusion transiently decreases concentrations of both naïve and memory T-cells by causing redistribution to tissue sites such as lymph nodes (Dimitrov et al., Citation2009).
The thymus is essential for adaptive immunity because it is the source of naïve T-cells (Majumdar and Nandi, Citation2018). Decreased thymic function in early infancy, when output of naïve T-cells is at its peak (den Braber et al., Citation2012), can decrease the ability of the immune system to recognize novel antigens later in life due a decrease in diversity of the T-cell repertoire. This decreased diversity presumably accounts for the lower vaccine response seen in young adults who underwent thymectomies at a median age of 11 months (Prelog et al., Citation2008). These young adults also had fewer naïve T-cells and the deficit in vaccine responsive was greatest in those whose thymectomies occurred under 6 months of age. Genetic defects in thymic function (e.g. DiGeorge syndrome) are also associated with smaller thymus size, decreased thymic output and increased risk of death from infections, presumably due to impaired adaptive immunity (Sauce and Appay, Citation2011). Studies of euthymic new-borns in Guinea Bissau at high risk of malaria and other infections has shown that a smaller thymus at birth is associated with an increased risk of death from infectious diseases during the first 2 years of life (Aaby et al., Citation2002). In a separate study in the same setting a twofold larger thymus measured at 6 months of age was associated with a 70% lower risk of death over the next 30 months (Garly et al., Citation2008). Similarly, a smaller thymus during infancy was associated with an increased risk of death from infectious diseases through 5 years of age in Bangladesh, where the overall risk of death was lower than in Guinea Bissau (Moore et al., Citation2014). Thus variation in thymus size early in infancy, driven by environmental factors that may include stress, has adverse effects on immune function and overall health later in life, as has been recently reviewed (Moore, Collinson, Tamba N'Gom, Aspinall, & Prentice, Citation2006).
In this study, we tested the hypothesis that infants with higher stress responses would have impaired T-cell-mediated immunity, based on the premise outlined above. Specifically, we determined if higher pain-induced (via a needle-stick for vaccination) cortisol responsiveness was associated with thymus size, peripheral blood naïve and memory T lymphocyte and TREC concentrations, as well as with responses to T-cell-dependent vaccines, in Bangladeshi infants between birth and 15 weeks of age. The study was conducted with infants recruited into a randomized, controlled trial examining the effect of vitamin A supplementation to new-born infants on vaccine responsiveness and thymic function in Dhaka, Bangladesh.
Materials and methods
Study design
This study was an observational study nested within a block-randomized double-blind placebo-controlled clinical trial [ClinicalTrials.gov identifier: NCT01583972], conducted on healthy infants in Bangladesh, as outlined in the Figure S1. The study was approved by the Research Review Committee (RRC) and the Ethical Review Committee (ERC) of the International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b). Written consents were obtained from the parents or legal guardian of the study participants. The detail of the inclusion–exclusion criteria, study design, laboratory methodology, and baseline characteristics of the study participant have been described earlier (Ahmad, Raqib, Qadri, & Stephensen, Citation2014).
Study subjects and sample collection
The study subjects were enrolled at the Maternal and Child Health Training Institute (MCHTI). The study was conducted at International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) and MCHTI in collaboration with the USDA Western Human Nutrition Research Center located at the University of California, Davis, CA, USA. The detail of the parent study design and baseline data have been described earlier (Ahmad et al., Citation2014). In brief, a total of 306 infants were enrolled in the parent study (male = 153) for 50,000 IU vitamin A supplementation within 48 h of birth. All the infants received standard vaccines according to Bangladesh Ministry of Health’s guidelines. Vaccine administration and sample collection are described in Figure S1. Collected saliva and blood samples were stored in an ice chest with a gel pack and then transported to the Immunobiology, Nutrition and Toxicology (INT) Laboratory at icddr,b within 3–4 h of collection for analyzing, processing and storing at –80 °C. We could not collect saliva for cortisol measurement from all 306 infants because of a lack of availability of the saliva collection kits during two periods of the study, each about 1 month in duration, during the months June, July and August of enrollment period January 2012 to May 2013. A total of 229 pre-vaccine cortisol and 231 post vaccine cortisol samples were collected. Thus, in this paper, we are presenting data from 229 infants (male = 107). Two study participants withdrew from the study at 10 w and, thus, no follow-up data were available from those two after 10 w. All anthropometric and laboratory data were securely stored on using the RedCap database (Harris et al., Citation2009) provided by the UC Davis Clinical and Translational Sciences Center.
Salivary cortisol analysis
Infant saliva was collected by a Salimetrics infant's saliva collection kit (Salimetrics, Carlsbad, CA, USA) before and 20 min after a single intramuscular immunization with pentavalent vaccine at 6 weeks of age to determine cortisol responsiveness. Pre-vaccine saliva was collected between 9:39 am and 1:34 pm with a median of 11:34 am. During saliva collection, the infant’s behavior (asleep, awake, awake and crying), saliva collection time, body temperature, anthropometry, breastfeeding status and other health-related information were recorded. After completion of the enrollment, the salivary concentration was determined by enzyme immunoassay (EIA) kit (Salimetrics) as per the manufacturer’s instruction. Appropriate low and high-quality standards were measured with every EIA plate assay. The intra-assay coefficient of variation (CV) was 4.25% and inter-assay CV was 4.30%. We successfully collected saliva and measured pre- and post-vaccine salivary cortisol from 229 infants’ (male = 107). Venipuncture blood collection occurred during the same visit and the sequence of blood collection and vaccination varied due to scheduling issues beyond the control of the study. Pre-saliva collection occurred before blood collection in 66 infants. All other saliva collections occurred from 1 to 184 min after blood collection. Post-vaccine saliva collection occurred 23.4 ± 0.47 min after the vaccination. Based on the time between blood collection and pre-vaccine saliva collection, infants were divided into four time groups; G1 = obtained saliva collection before blood collection (n = 66), G2 = obtained saliva collection 1–30 min after blood collection (n = 67), G3 = obtained saliva collection 31–60 min after blood collection (n = 80), G4 = more than 60 min after blood collection (n = 16) to evaluate the effect of the venipuncture on salivary cortisol.
Thymus size
Thymus size was measured by ultrasound at 1, 6, 10 and 15 weeks of age. Thymic index (TI) was obtained by multiplying the transverse diameter and the sagittal area of the largest lobe (Hasselbalch, Nielsen, Jeppesen, Pedersen, & Karkov, Citation1996).
Blood cells counts
Naïve T cell counts in per µL of peripheral blood at 6 and 15 weeks were determined by commercially available Multitest four-color reagent kits (CD45RA-FITC/CD45RO-PE/CD3-PerCP/CD4-APC) with Trucount Tubes (BD Biosciences, San Jose, CA, USA) on flow cytometer FACSCalibur (BD Biosciences). Flow data were analyzed by FlowJo software (FlowJo, LLC., Ashland, OR, USA). The gating strategy for memory and naïve T-cells assay is shown in Figure S5. TREC copy number was per million PBMCs was determined by sybergreen based qPCR method (Raqib et al., Citation2007). Additionally, complete blood count was performed by hematology analyzer Sysmex XT1800i (Sysmex, IL, Lincolnshire, USA). Details of these methods have been described previously (Ahmad et al., Citation2014).
Vaccine responses
To determine vaccine specific memory T-cell (CD45RO+) response we cultured 1 × 106/mL isolated PBMC in the presence of 5.0 μg/mL of purified protein derivative (PPD) of tuberculin (NIBSC, Potters Bar, UK), 7.5 μg/mL of rHBsAg subtype ADW (Fitzgerald, Acton, MA, USA), 5.0 Lf/mL of tetanus toxoid (NIBSC) and 10% of inactivated trivalent polio vaccine (IPOL, Sanofi Pasteur S.A., Lyon, France). The superantigen staphylococcus enterotoxin B (SEB; 0.25 μg/mL; Sigma Chemicals, St. Louis, MO, USA) and phosphate-buffered saline (PBS) were used as positive and negative controls, respectively. On the 6th day of culture, the cells were harvested for staining with CD3, CD4 and CD45RO markers and analyzed by FACSAria-III (BD Biosciences). Flow data were analyzed by FlowJo software (FlowJo, LLC.). The gating strategy for the T-cell stimulation index assay is shown in Figure S6. The proliferation index was calculated by dividing the ratio of antigen-stimulated memory T-cells to total T-cells by the ratio of control memory T-cells to total T-cells. To determine active secretion of antibodies from PBMC in response to in vivo vaccination, we used ALS (antibodies from lymphocyte secretions) assay method. In brief, 1 × 107 isolated PBMC was cultured with standard Russ-10 and 10% heat-inactivated FBS for 48 h. Commercially available kits were used to determine anti-TT IgG (Binding Site, San Diego, CA, USA), anti-HBsAg IgG (Alpha Diagnostic, San Antonio, TX, USA) and anti-Polio IgG (IBL international, NC, USA) antibodies in culture media according to manufacturers’ instruction. Tuberculin skin tests response to Bacillus Calmette–Guérin (BCG) immunization was assessed at 15 weeks, by using the intradermal injection of PPD. Induration area was determined by the formula “0.8X tuberculin skin tests long diameter (TSTLD) X tuberculin skin tests short diameter (TSTSD).” TSTLD ≥10 mm was considered as a positive response to categorize the PPD skin test response. Details of this method have been described earlier (Ahmad et al., Citation2014).
Nutritional status
Breastfeeding was characterized by using World Health Organization criteria (WHO/UNICEF, Citation2008) with some modifications. “Breastfeeding + non–human milk” and “Breast-feeding + solid or semi-solid food” were combined to category “Other,” which provided us with three categories of breastfeeding status, exclusively breastfeed, predominant breastfeed and other. Other nutritional status was measured by widely used instruments following standard procedures as was described in our previous publication (Huda et al., Citation2014).
Gestational age
Gestational age was calculated from ultrasound data or from the date of the first day of the mother's last menstrual period as was described earlier (Ahmad et al., Citation2014).
Statistical analysis
Paired t test was performed to determine the difference between pre- and post-vaccine cortisol. Student’s t test was performed to compare between sex and supplemental groups. Two-way ANOVA was used to compare pre- and post-vaccine cortisol concentration among time groups based on the time between the blood draw and saliva collection. Associations between cortisol responsiveness and thymic index or blood cell counts were determined by multiple regression modeling. Pre-vaccine cortisol concentration was used as a confounding factor to control the effect of known (venipuncture blood collection) and unknown baseline stress on cortisol responsiveness. Additionally, the analysis we statistically controlled for the following possible confounding factors: infant’s behavior during saliva collection, salivary collection time, sex, mode of delivery, birthweight, length for age Z-score, weight for length Z-score and breastfeeding status. A p value of ≤.05 was considered statistically significant for all analyses. Data are presented as means ± SD unless otherwise indicated. Statistical analysis was performed using R version 3.4.2. Graphs were produced by GraphPad Prism (La Jolla, CA, USA).
Results
Characteristics of the study population
The age range of the mothers participating in this study was 18–37 years. Most of the participating mother had some elementary or secondary education (3–17 years) with <5% having no education. More than half of the infants were delivered by C-section (), 6.11% were born preterm (<37 weeks of gestation) and 27.04% were born with a low birth-weight (<2500 g). Most infants were exclusively breastfeeding at 6 weeks of age with the rate progressively decreasing with age (). The prevalence of wasting (weight-for-length below “–2” Z-scores) was between 4.80% and 7.42% during the study while the prevalence of stunting (length-for-age below “–2” Z-scores) was between 17.5% and 11.9% ().
Table 1. Characteristics of the participants.
Post-vaccine salivary cortisol was higher than pre-vaccine salivary cortisol
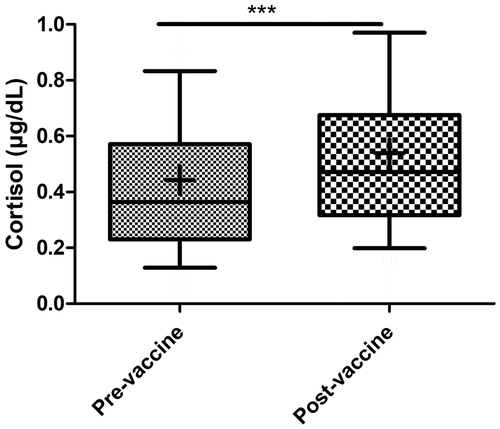
The post-vaccine cortisol concentration increased significantly (t = –15.029, DF = 227, p < .001) above the pre-vaccine concentration (), as expected, and this increase was seen regardless of the timing of the vaccination relative to blood collection at the same visit (Figure S2(A)). Group 2 had significantly higher pre-vaccine cortisol concentration than group 1 (p < .001) and group 4 (p = .0020). However, post-vaccine cortisol concentration did not differ by timing groups (Figure S2(B)).
Figure 1. Post-vaccine salivary cortisol was significantly higher than pre-vaccine cortisol (n = 229). Comparison was calculated by independent two group t-test. Box =25th–75th percentile, whiskers =10th–90th percentile, + = mean, horizontal bar = median, *** = p < .001.
Vitamin A supplementation had no effect on cortisol responsiveness
Cortisol responses were 0.143 ± 0.45 and 0.0541 ± 0.358, respectively, for vitamin A and placebo groups. The cortisol responsiveness did not differ between vitamin A and placebo groups when compared by t test (t = –0.76264, DF = 224.93, p = .45), nor was a treatment effect seen (p = .21) after adjusting for covariates including pre-vaccine cortisol, infant’s behavior during saliva collection, saliva collection time, sex, mode of delivery and nutritional status ().
Cortisol responsiveness was negatively associated with thymus size in boys only
The association of cortisol responsiveness with thymus size was evaluated using multiple regression analysis with adjustment for covariates infant’s behavior during saliva collection, pre-vaccine cortisol, saliva collection time, sex, mode of delivery, birthweight, length for age Z-score, weight for length Z-score and breastfeeding status. In this analysis, a significant interaction was seen for cortisol responsiveness and sex (p < .05) at all study visits, thus results are reported separately for males and females. The cortisol responsiveness was negatively associated with thymus size at all time points, but the association was seen only in boys (). Male infants with cortisol responsiveness in the highest quartile consistently had a 35.4%–37.7% lower predicted TI at all-time points compared to the lowest quartile for cortisol responsiveness, standardizing for exclusive breastfeeding, vaginal delivery, infants asleep during saliva collection, and the median saliva collected time (11:34 am) (Figure S3).
Table 2. Associations between thymic indices and 6 week vaccination-induced cortisol responsiveness (ΔCortisol) in infants determined by multivariate regression modeling.
Cortisol responsiveness was negatively associated with peripheral blood T-cell concentrations
Consistent with the results for TI, the concentration of total naïve T-cells (CD3+CD45RA+) at 6 weeks (β (SE) = –2225 (819), p = .0072) and of naïve helper T-cells (CD3+CD4+CD45RA+) at both 6 weeks (β (SE) = –1671 (565), p = .0035) and 15 w (β (SE) = –1800 (675), p = .0085) were negatively associated with the cortisol responsiveness, though no sex interaction was seen (). The associations remained significant even after adjusting with corresponding thymic indices (data not shown; though the absolute value of β-coefficients decreased by 3%–25%) suggesting an independent effect of cortisol responsiveness on peripheral blood T-cells not mediated through an effect on thymus size. The predicted naïve CD4+ T-cell concentrations in infants with cortisol responsiveness in the highest quartile were 23.1% and 22.8% lower compared to lowest quartile at 6 w and 15 weeks, respectively, representing differences of 609 and 640 cells/μL blood (Figure S4; standardized for vaginal-delivered, exclusively breastfeed, infants who were asleep during saliva collection, with saliva collected at 11:34 am [median saliva collection time]). Similar differences were seen for total CD4+ T-cells (, Figure S4) but not for total memory and CD4+ memory T-cells ().
Table 3. Associations between T cell concentrations and TREC concentrations (per million PBMC) and 6 weeks vaccination-induced cortisol responsiveness in infants determined by multivariate regression modeling.
Cortisol responsiveness was negatively associated with PPD skin test
Infants received vaccines at birth, 6, 10 and 14 weeks of age (Figure S1). Three types of vaccine responses were analyzed: (1) T-cell proliferation; (2) antibody response and (3) the delayed-type hypersensitivity (DTH) response to PPD antigen as an index of the response to BCG immunization. None of the proliferation responses showed a statistically significant association with salivary cortisol (). However, the odds ratio of having a positive PPD skin test at 15 weeks of age was lower (β (SE) = –5.31 (2.51), p = .034) with a higher cortisol response () and infants had a 23.7% lower predicted probability of having a positive PPD skin test if they were in the highest versus lowest quartile of cortisol responsiveness (). In addition, the PPD skin test area analyzed as a continuous variable was also negatively associated with cortisol responsiveness (; p = .049).
Figure 2. Predicted probability of observing positive PPD skin test at 15 weeks by cortisol responsiveness quartiles in normally delivered exclusively breastfeed infants having median baseline cortisol, cortisol collection time, HAZ and WHZ scores. Bar represents 95% CI. Mean and CI were predicted from the regression model described in the .
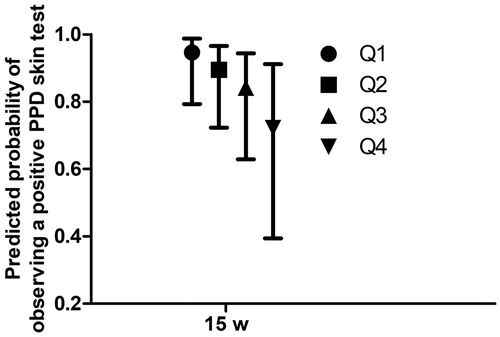
Table 4. Associations between vaccine responses and 6-week vaccination-induced cortisol responsiveness in infants.
Discussion
In the present study, we assessed cortisol responsiveness by measuring pre- and post-vaccine salivary cortisol at 6 weeks of age and characterized associations with the T-cell compartment of the immune system, and with T-cell mediated vaccine responses. The salivary cortisol levels from infants in the present study () were very similar to those recently reported (Albers, Beijers, Riksen-Walraven, Sweep, & de Weerth, Citation2015) for infants at 14 weeks of age, who had morning salivary cortisol concentrations of 0.27 ± 0.18 and 0.31 ± 0.23 µg/dL at home and a child care facility, respectively. Thus the data from our study is consistent with recent literature.
A principal finding of our study was that thymus size between 1 and 15 weeks of age was consistently smaller in boys (but not in girls) with higher cortisol responsiveness, suggesting a negative effect of elevated cortisol on thymic function in boys. To the best of our knowledge, this is the first report showing associations between thymus size and challenge-induced cortisol responsiveness in healthy infants, and it is not clear why this effect would be seen only in boys. The cortisol response does not seem to differ between male and female infants (unlike adults), though data are sparse, as recently reviewed (Rao and Androulakis, Citation2017). Work on prenatal stress indicates that male and female infants respond differently with regard to emotional development (Braithwaite, Murphy, Ramchandani, & Hill, Citation2017), suggesting that sex differences might be seen in other systems as well. One possibility in the thymus, based on data from mice, is that testosterone can act in the thymus to produce cortisol which then acts locally to cause thymocyte apoptosis (Chen, Qiao, Tuckermann, Okret, & Jondal, Citation2010). Since infants in our study are in the period of “mini-puberty,” when estrogen and testosterone differ between the sexes (Lamminmaki, Hines, Kuiri-Hanninen, Kilpelainen, Dunkel, & Sankilampi, Citation2012), it is possible that the additive effect of stress-induced and testosterone-induced cortisol combine to a decrease in thymus size in boys that is not seen in girls. Though we have measured cortisol responsiveness at just a single time point, 6 weeks of age, the inverse association between cortisol responsiveness and thymus size from 1 to 15 weeks of age suggests that high responsiveness at 6 weeks may be representative of cortisol responsiveness throughout early infancy.
Consistent with the observations on thymus size, we also found that peripheral blood levels of naïve T-cells were also negatively associated with the cortisol responsiveness, though TREC levels were not. The association with naïve T-cells was not sex-specific. The association remains significant even after adjusting for thymus size which suggests a direct effect of cortisol responsiveness on peripheral-blood naïve T-cells independent of an effect on the thymus. It is possible that this association could result from a redistribution of T-cells away from the blood but this redistribution effect is also seen for memory T cells (Dimitrov et al., Citation2009), which we did not observe in the present study. Other studies also report stress-related reductions in peripheral blood levels of naïve T-cells, which could be related either to thymic function or redistribution. For example, one study found that reductions of urinary cortisol resulting from a stress-management intervention were associated with increases of naïve T-cell levels in blood (Antoni et al., Citation2005) and other studies have reported decreased helper T-cells in peripheral blood during exam stress (Glaser et al., Citation1985; Kiecolt-Glaser et al., Citation1986).
The DTH skin test response to PPD antigen, which involves the development of T cell-mediated induration (Siegrist, Citation2013), was negatively associated with cortisol responsiveness, though our ex vivo measures of T-cell responsiveness were not. It is possible that the in vivo DTH response is more directly affected by plasma cortisol than are T-cell responses measured over a period of 6 d in media containing only 10% autologous plasma. Lower DTH responses have previously been associated with elevated stress. A study involving preterm infants reported that those with high morning cortisol had lower DTH skin-test responses to a variety of recall antigens (Buske-Kirschbaum et al., Citation2007). It is true that other studies have reported effects on ex vivo T cell responses as well. A study in non-human primates found decreased T-lymphocyte proliferation during peer-separation stress (Friedman, Coe, & Ershler, Citation1991) while similar results were seen for T-cell proliferative responses to Epstein-Barr virus antigen as a result of exam stress in students (Glaser et al., Citation1993). Lower Hepatitis B (HBV) vaccine-specific T-cell proliferation and antibody responses were also seen in healthy adults reporting higher stress (Glaser et al., Citation1992). However, none of these studies evaluated cortisol responsiveness, which may be influenced by factors, such as prior stress (Herman et al., Citation2016), that alter cortisol responsiveness and also impact immune function.
Our study had several strengths, including its relatively large sample size (n = 229), the examination of multiple aspects of adaptive immunity, the direct observation of immunizations by study personnel, and the unique population of healthy infants. A weakness of our study was the timing of the pre-vaccine saliva collection, which was not consistently coordinated with the venepuncture blood collection, though adequate statistical adjustment was made for this additional variable.
In summary, our findings show a sex-specific association of elevated stress-induced cortisol with smaller thymus size, though other negative associations of cortisol with CD4 T-cell concentrations and the DTH response to BCG vaccination were observed in both boys and girls. Demonstration of sex differences in immune function, including response to vaccination, is not new (Garly et al., Citation2004). Differential stress responses between boys and girls may provide mechanistic explanations for other sex-specific differences in immune function; this phenomenon warrants further study.
Supplementary Figure 6
Download JPEG Image (2.4 MB){kind=link}
Supplementary Figure 5
Download JPEG Image (1.3 MB){kind=link}
Supplementary Figure 4
Download JPEG Image (538 KB){kind=link}
Supplementary Figure 3
Download JPEG Image (341.8 KB){kind=link}
Supplementary Figure 2
Download JPEG Image (909.4 KB){kind=link}
Supplemental Tables 1-5
Download MS Word (40.3 KB)Supplementary Figure 1
Download TIFF Image (1.8 MB)Acknowledgements
We also thankfully acknowledge all the study participants. The parent study was supported by the World Health Organization via a Bill and Melinda Gates Foundation grant and Thrasher Research Fund. We respectfully acknowledge Janet M. Peerson, Senior Statistician, WHNRC for her selfless guiding on statistical analysis. We also give thanks to all the research staff, data entry staff, hospital nurses, and physicians at the collaborating clinic MCHTI.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
Related Research Data
References
- Aaby, P., Marx, C., Trautner, S., Rudaa, D., Hasselbalch, H., Jensen, H., & Lisse, I. (2002). Thymus size at birth is associated with infant mortality: a community study from Guinea-Bissau. Acta Paediatrica (Oslo, Norway: 1992), 91, 698–703. doi:10.1111/j.1651-2227.2002.tb03305.x
- Ahmad, S.M., Raqib, R., Qadri, F., & Stephensen, C.B. (2014). The effect of newborn vitamin A supplementation on infant immune functions: trial design, interventions, and baseline data. Contemporary Clinical Trials, 39, 269–279. doi:10.1016/j.cct.2014.09.004
- Albers, E.M., Beijers, R., Riksen-Walraven, J.M., Sweep, F.C.D., & de Weerth, C. (2015). Cortisol levels of infants in center care across the first year of life: links with quality of care and infant temperament. Stress, 19, 8–17. doi:10.3109/10253890.2015.1089230
- Antoni, M.H., Cruess, D.G., Klimas, N., Carrico, A.W., Maher, K., Cruess, S., … Schneiderman, N. (2005). Increases in a marker of immune system reconstitution are predated by decreases in 24-h urinary cortisol output and depressed mood during a 10-week stress management intervention in symptomatic HIV-infected men. Journal of Psychosomatic Research, 58, 3–13. doi:10.1016/j.jpsychores.2004.05.010
- Benjamin, C.L., Stowe, R.P., St John, L., Sams, C.F., Mehta, S.K., Crucian, B.E., … Komanduri, K.V. (2016). Decreases in thymopoiesis of astronauts returning from space flight. JCI Insight, 1, e88787. doi:10.1172/jci.insight.88787
- Braithwaite, E.C., Murphy, S.E., Ramchandani, P.G., & Hill, J. (2017). Associations between biological markers of prenatal stress and infant negative emotionality are specific to sex. Psychoneuroendocrinology, 86, 1–7. doi:10.1016/j.psyneuen.2017.09.004
- Buske-Kirschbaum, A., Krieger, S., Wilkes, C., Rauh, W., Weiss, S., & Hellhammer, D.H. (2007). Hypothalamic-pituitary-adrenal axis function and the cellular immune response in former preterm children. Journal of Clinical Endocrinology and Metabolism, 92, 3429–3435. doi:10.1210/jc.2006-2223
- Chen, Y., Qiao, S., Tuckermann, J., Okret, S., & Jondal, M. (2010). Thymus-derived glucocorticoids mediate androgen effects on thymocyte homeostasis. FASEB Journal, 24, 5043–5051. doi:10.1096/fj.10-168724
- Cohen, J.J. (1992). Glucocorticoid-induced apoptosis in the thymus. Seminars in Immunology, 4, 363–369. https://www.ncbi.nlm.nih.gov/pubmed/1286164
- de Felice, C., Toti, P., Musaro, M., Peruzzi, L., Paffetti, P., Pasqui, L., … Latini, G. (2008). Early activation of the hypothalamic-pituitary-adrenal-axis in very-low-birth-weight infants with small thymus at birth. Journal of Maternal-Fetal and Neonatal Medicine, 21, 251–254. doi:10.1080/14767050801927871
- den Braber, I., Mugwagwa, T., Vrisekoop, N., Westera, L., Mogling, R., de Boer, A.B., … Tesselaar, K. (2012). Maintenance of peripheral naive T cells is sustained by thymus output in mice but not humans. Immunity, 36, 288–297. doi:10.1016/j.immuni.2012.02.006
- Dimitrov, S., Benedict, C., Heutling, D., Westermann, J., Born, J., & Lange, T. (2009). Cortisol and epinephrine control opposing circadian rhythms in T cell subsets. Blood, 113, 5134–5143. doi:10.1182/blood-2008-11-190769
- Friedman, E.M., Coe, C.L., & Ershler, W.B. (1991). Time-dependent effects of peer separation on lymphocyte proliferation responses in juvenile squirrel monkeys. Developmental Psychobiology, 24, 159–173. doi:10.1002/dev.420240303
- Garly, M.L., Jensen, H., Martins, C.L., Bale, C., Balde, M.A., Lisse, I.M., & Aaby, P. (2004). Hepatitis B vaccination associated with higher female than male mortality in Guinea-Bissau: an observational study. Pediatric Infectious Disease Journal, 23(12), 1086–1092. http://www.ncbi.nlm.nih.gov/pubmed/15626943
- Garly, M.L., Trautner, S.L., Marx, C., Danebod, K., Nielsen, J., Ravn, H., … Lisse, I.M. (2008). Thymus size at 6 months of age and subsequent child mortality. Journal of Pediatrics, 153, e683–e688. doi:10.1016/j.jpeds.2008.04.069
- Glaser, R., Kiecolt-Glaser, J.K., Bonneau, R.H., Malarkey, W., Kennedy, S., & Hughes, J. (1992). Stress-induced modulation of the immune response to recombinant hepatitis B vaccine. Psychosomatic Medicine, 54, 22–29. doi:10.1097/00006842-199201000-00005
- Glaser, R., Kiecolt-Glaser, J.K., Stout, J.C., Tarr, K.L., Speicher, C.E., & Holliday, J.E. (1985). Stress-related impairments in cellular immunity. Psychiatry Research, 16, 233–239. doi:10.1016/0165-1781(85)90111-8
- Glaser, R., Pearson, G.R., Bonneau, R.H., Esterling, B.A., Atkinson, C., & Kiecolt-Glaser, J.K. (1993). Stress and the memory T-cell response to the Epstein–Barr virus in healthy medical students. Health Psychology: Official Journal of the Division of Health Psychology, American Psychological Association, 12, 435–442. doi:10.1037/0278-6133.12.6.435
- Harris, P.A., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., & Conde, J.G. (2009). Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 42, 377–381. doi:10.1016/j.jbi.2008.08.010
- Hasselbalch, H., Nielsen, M.B., Jeppesen, D., Pedersen, J.F., & Karkov, J. (1996). Sonographic measurement of the thymus in infants. European Radiology, 6, 700–703. http://www.ncbi.nlm.nih.gov/pubmed/8934137
- Herman, J., P., McKlveen, J., M., Ghosal, S., Kopp, B., Wulsin, A., Makinson, R., … Myers, B. (2016). Regulation of the hypothalamic‐pituitary‐adrenocortical stress response. Comprehensive Physiology, 6, 603–621. doi: 10.1002/cphy.c150015
- Huda, M.N., Lewis, Z., Kalanetra, K.M., Rashid, M., Ahmad, S.M., Raqib, R., … Stephensen, C.B. (2014). Stool microbiota and vaccine responses of infants. Pediatrics, 134, e362–e372. doi:10.1542/peds.2013-3937
- Kiecolt-Glaser, J.K., Glaser, R., Strain, E.C., Stout, J.C., Tarr, K.L., Holliday, J.E., & Speicher, C.E. (1986). Modulation of cellular immunity in medical students. Journal of Behavioral Medicine, 9, 5–21. doi:10.1007/BF00844640
- Lamminmaki, A., Hines, M., Kuiri-Hanninen, T., Kilpelainen, L., Dunkel, L., & Sankilampi, U. (2012). Testosterone measured in infancy predicts subsequent sex-typed behavior in boys and in girls. Hormones and Behavior, 61, 611–616. doi:10.1016/j.yhbeh.2012.02.013
- Majumdar, S., & Nandi, D. (2018). Thymic Atrophy: Experimental Studies and Therapeutic Interventions. Scandinavian Journal of Immunology, 87, 4–14. doi:10.1111/sji.12618
- Moore, S.E., Collinson, A.C., Tamba N'Gom, P., Aspinall, R., & Prentice, A.M. (2006). Early immunological development and mortality from infectious disease in later life. Proceedings of the Nutrition Society, 65, 311–318. doi:10.1079/PNS2006503
- Moore, S.E., Fulford, A.J., Wagatsuma, Y., Persson, L.A., Arifeen, S.E., & Prentice, A.M. (2014). Thymus development and infant and child mortality in rural Bangladesh. International Journal of Epidemiology, 43, 216–223. doi:10.1093/ije/dyt232
- Nieto, M.A., Gonzalez, A., Gambon, F., Diaz-Espada, F., & Lopez-Rivas, A. (1992). Apoptosis in human thymocytes after treatment with glucocorticoids. Clinical and Experimental Immunology, 88, 341–344. https://www.ncbi.nlm.nih.gov/pubmed/1572099
- Prelog, M., Wilk, C., Keller, M., Karall, T., Orth, D., Geiger, R., … Wuerzner, R. (2008). Diminished response to tick-borne encephalitis vaccination in thymectomized children. Vaccine, 26, 595–600. doi:10.1016/j.vaccine.2007.11.074
- Rao, R.T., & Androulakis, I.P. (2017). Modeling the sex differences and interindividual variability in the activity of the hypothalamic-pituitary-adrenal axis. Endocrinology, 158, 4017–4037. doi:10.1210/en.2017-00544
- Raqib, R., Alam, D.S., Sarker, P., Ahmad, S.M., Ara, G., Yunus, M., … Fuchs, G. (2007). Low birth weight is associated with altered immune function in rural Bangladeshi children: a birth cohort study. The American Journal of Clinical Nutrition, 85, 845–852. doi:10.1093/ajcn/85.3.845
- Sauce, D., & Appay, V. (2011). Altered thymic activity in early life: how does it affect the immune system in young adults? Current Opinion in Immunology, 23, 543–548. doi:10.1016/j.coi.2011.05.001
- Siegrist, C.-A. (2013). Vaccine immunology-Plotkin, Stanley A. In W. A. Orenstein & P. A. Offit (Eds.), Vaccines (Sixth Edition) (pp. 14–32). London: W.B. Saunders.
- Webster Marketon, J.I., & Glaser, R. (2008). Stress hormones and immune function. Cells Immunology, 252, 16–26. doi:10.1016/j.cellimm.2007.09.006
- WHO/UNICEF (2008). Indicators for Assessing Infant and Young Child Practices. Geneva, Switzerland: World Health Organization.