
Abstract
Everyday life psychosocial stressors contribute to poor health and disease vulnerabilty. Means alternative to pharmacotherapy that are able to foster stress resilience are more and more under the magnifying glass of biomedical research. The aim of this study was to test stress resilience fostering properties of the self-administration of a cosmetic product enriched with essential oils. On day 0, fourty women, 25-50 years old, self-administered both the enriched cosmetic product (ECP) and a placebo one (PCP). Then, women were randomized for daily self-administration (from day 1 to 28) of either ECP (n = 20) or PCP (n = 20). On day 29, subjects underwent a psychosocial stress test (PST). Autonomic (heart rate and its variability) and neuroendocrine (salivary cortisol) parameters were assessed both on day 0 and 29. All subjects filled a number of psychological questionnaires in order to quantify anxiety, perceived stress, and mood profile, and were videorecorded during PST for non-verbal behavior evaluation. A single application of ECP produced an acute potentiation of cardiac parasympathetic modulation, which was not observed when placebo was used. Prolonged self-administration of ECP induced: (i) a dampening of the cortisol rise produced by PST, (ii) a reduction of state anxiety, (iii) a favorable change in mood profile, and (iv) a reduction of non-verbal behavior patterns that signal anxiety, motivational conflict and avoidance. In conclusion, this study suggests that the self-administration of a cosmetic cream enriched with essential oils should be considered as a stress resilience fostering strategy due to its favorable physiological, neuroendocrine and psychological effects.
Introduction
Everyday life psychosocial challenges may negatively impact health and well-being, contributing to the onset and progression of psychological disorders and psychosomatic dysfunctions (Cummings et al., Citation2016; McEwen, Citation1998; Sgoifo et al., Citation2001). Pharmacological treatments addressing GABA-ergic, serotonergic and noradrenergic neurotransmission can moderate our stress response, but they usually bring about addiction/tolerance and a number of other uncomfortable side effects. Therefore, it is relevant to identify alternative stress relief strategies that are devoid of these unwanted drawbacks. In addition, the effects of such alternative interventions should be objectively quantified by means of reliable psychobiological parameters (Finch et al., Citation2019; Pattini et al., Citation2019; Pico-Alfonso et al., Citation2007).
Along this line, a number of non pharmacological stress management approaches have been studied lately, including noninvasive brain stimulation(Carnevali et al., Citation2020), eye movement desensitization and reprocessing (EMDR) therapy (Elofsson, von Schèele, Theorell & Söndergaard, 2008), yoga (Chu et al., Citation2017), mindfulness (Balconi et al., Citation2019), contact with nature (Hunter et al., Citation2019), art making (Haiblum-Itskovitch et al., Citation2018), and aromatherapy (Huang & Capdevila, 2017). On this last regard, a variety of volatile oils have been shown to produce potent neurobiological effects. Olfactory stimuli are directly conveyed to the limbic system and hypothalamus via the olfactory bulb. Hence, unlike other sensory inputs, they directly trigger emotions and associated autonomic/nueorendocrine responses. Given that odors have an impact on behavior, mood and physiology they may represent a valuable tool to tone down acute and long-term consequences of stressful stimuli (Haze et al., Citation2002; Kiecolt-Glaser et al., Citation2008).
Indeed, a few studies pointed out the stress-relief properties of aromatherapy practice. For instance, inhalation of fragrances has been used to counteract autonomic dysfunction associated with obesity, hypertension and other cardiovascular diseases (Goes et al., Citation2012; Niijima & Nagai, 2003; Peng et al., Citation2009; Shen et al., Citation2005; Shiina et al., Citation2008). Haze et al. reported that rose oil caused a decrease in plasma adrenaline concentrations, and concluded that essential oil inhalation may be used to modulate sympathetic hyperactivity (Haze et al., Citation2002).
Several studies have investigated the clinical benefits of aromatherapy by means of heart rate variability (HRV) measurements and demonstrated significant changes of autonomic nervous system modulation after inhalation of essential oils, including lavender (Chien et al., Citation2012; Kuroda et al., Citation2005; Matsumoto et al., Citation2013; Saeki, Citation2000), jasmine (Kuroda et al., Citation2005) and bergamot (Chang & Shen, Citation2011; Liu et al., Citation2013; Watanabe et al., Citation2015). Overall, these changes consisted mostly in the potentiation of cardiac parasympathetic input, alongside with mood state and sleep improvement.
Interestingly, the beneficial effects of essential oils can be achieved also by applying a mixture of essences (e.g., lavender and bergamot) on the abdomen skin (Hongratanaworakit, Citation2011), with obvious advantages in terms of administration easiness. The study showed that transdermal absorption of blended essential oil provided a synergistic effect on autonomic parameters and emotional responses. Specifically, compared with placebo, blended essential oil caused significant decreases of heart rate and systolic and diastolic blood pressure, suggesting a decrease of autonomic arousal. At the emotional level, subjects belonging to the blended essential oil group rated themselves as “more calm” and “more relaxed” than subjects in the control group (Hongratanaworakit, Citation2011).
The idea behind the present study, therefore, was to test the acute and persistent stress resilience fostering properties of a cosmetic routine based on the self-administration of a face cosmetic product (cream + lotion) with a pleasurable texture, enriched with four essential oils, and applied with a mindful massage. To this purpose, noninvasive quantitative measurements of the activity and reactivity of the autonomic nervous system (heart rate variability parameters) and the hypothalamic-pituitary-adrenocortical axis (salivary cortisol levels) were performed. In addition, behavioral and psychometric data were also collected, by means of an ethological analysis of nonverbal behavior and a number of appropriate questionnaires.
Aiming to propose alternative means that possibly foster stress resilience and improve mental and physical helath, a natural functional aroma was used, a blend of four substances (Juniperus phoenicea gum extract, Copaifera officinalis resin, Aniba rosaeodora wood oil and Juniperus virginiana oil) that are used in aromatherapy and bear a variety of documented beneficial effects, ranging from anti-inflammatory and anti-oxidant to hypotensive, neuroprotective and anxiolytic (de Siqueira et al., Citation2014; Ennajar et al., Citation2009; Guimarães-Santos et al., Citation2012; Leandro et al., Citation2012; Zhang & Yao, Citation2018).
Methods
Subjects
Forty healthy female participants were recruited by the use of flyers. Exclusion criteria included: younger than 25 and older than 50 years old; current or past neurological, psychiatric, and cardiac disorders; cognitive impairment; substance or alcohol abuse or dependence; recent (last 12 months) traumatic events such as a death in the family, serious accident, job loss or divorce; caregiving (last 12 months) a family member with serious pathology or disability; current psychotropic or contraceptive drug use. The study conformed to the Declaration of Helsinki, and the protocol (N. 46700) was approved by Parma Ethical Committee, Italy. All volunteers gave written informed consent for their participation. ClinicalTrials.gov identification code is NCT04127279.
Procedure
A randomized, placebo-controlled, single-blind design was used. Participants were first invited to the lab to complete a set of socio-demographic, lifestyle, and psychometric questionnaires (see section “Psychometric assessment” for details). On the same day (day -2), they were instructed by a specialized operator for a specific mode of self-administration of the cosmetic product, which involved a 3-minute mindful massage.
Recording session 1 (day 0)
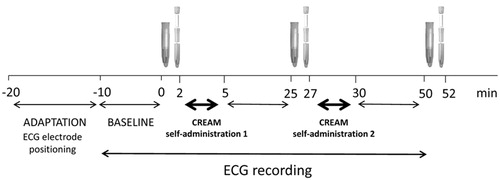
Two days later, participants returned to the lab. They were preventively recommended to refrain from caffeine, alcohol, and nicotine consumption, as well as strenuous exercise for at least 2 hours prior to the experimental session, as these variables may have transient effects on cardiovascular/neuroendocrine measurements (Laborde et al., Citation2017). depicts the sequence of events included in the first recording session of the study protocol. Upon arrival to the lab, participants were fitted with a BT16Plus device (Francesco Marazza Hardware & Software, Monza, IT), which allows real time acquisition of ECG signals (sampling frequency: 250 Hz) in freely-moving subjects. Subsequently, they were allowed to settle down for 10 min while sitting on a comfortable chair. Continuous ECG recordings were performed during the following phases: baseline (10 min, from min –10 to 0), after cosmetic product self-administration 1 (from min 5 to 25), after cosmetic product self-administration 2 (from min 30 to 50). Each subject self-administered both a placebo cosmetic product (PCP) and the one enriched with essential oils (ECP) following a randomized order, in order to avoid effect interferences. Moreover, subjects were not aware of the type of product they were making use of (see section “Cosmetic routine” for details). Saliva samples were collected from each participant using oral swabs and swab storage tubes (Salimetrics, UK), in baseline conditions (from min 0 to 2), after cream self-administration 1 (from min 25 to 27), and after cream self-administration 2 (from min 50 to 52) ().
Figure 1. Outline of recording session 1 (day 0).
Four week self-administration (day 1 to 28)
At the end of recording session 1, participants were randomly assigned to two groups. One group (ECP, “enriched cosmetic product,” n = 20) received the face cosmetic product enriched with essential oils; the other one (PCP, n = 20) received the placebo one, devoid of essential oils. Again, subjects were not aware of the type of product they were making use of. They were asked to self-administer it at home, twice a day, in the morning and at bed time for 4 consecutive weeks (28 days), starting the day after recording session 1.
Recording session 2 (day 29)
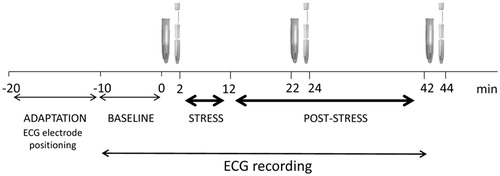
On day 29, participants returned to the lab and were submitted to a psychosocial stress test (PST), following a previously adopted procedure (Pico-Alfonso et al., Citation2007) that was based on an adapted version of the Trier Social Stress Test (Kirschbaum et al., Citation1993) (see section “Psychosocial stress test” for details). Again, participants were preventively asked to refrain from caffeine, alcohol, and nicotine consumption, as well as strenuous exercise for at least 2 hours prior to the recording session. depicts the sequence of events included in the second recording session of the study protocol. Upon their arrival to the lab, participants were fitted with the BT16Plus device (BT16Plus Acquisition System, Francesco Marazza, IT) and were allowed to settle down for 10 min while sitting on a comfortable chair in front of two familiar experimenters. Continuous ECG recordings were performed during the following phases: baseline (10 min, from min –10 to 0), stress (from min 2 to 12), and post-stress (from min 12 to 42). Saliva samples were collected from each participant in baseline conditions (from min 0 to 2), 10 min after the end of the stress test (from min 22 to 24), and at the end of the recovery phase (from min 42 to 44) ().
Figure 2. Outline of recording session 2 (day 29).
Psychosocial stress test (PST)
During the stress interview phase (SI, first 5 min of the PST), participants were asked to answer a series of questions about how they behave and feel in different social contexts (e.g., “What are the social situations that make you most uneasy?”). Subsequently, they were asked to complete a 5-min mental arithmetic task (AT) by counting aloud backwards from 2083 by 13’s. The SI and AT were administered by an unfamiliar male interviewer, with a small unfamiliar audience (2 people) sitting behind the participants, thus contributing to heighten the socially evaluative character of the stress context. During both tasks, the interviewer applied pressure by instructing participants to “please continue” or “go faster” when they paused. The interviewer also corrected participant math responses, invited them to restart from 2083 after an incorrect response, and encouraged them to “try to do better.”
Upon completion of the stress period, the unfamiliar interviewer and audience left the room, and participants remained seated and quiet in the presence of the two familiar experimenters for the following 30-min post-stress phase
The behavior of the participants during the stress interview was videotaped with a camera positioned in front of them (). Finally, before and after the PST participants completed the state version of the STAI (Spielberger et al., Citation1983). The PST took place between 14:30 and 16:30 h, in a quiet room at a comfortable temperature (21 ± 2 °C).
Cosmetic routine
All subjects self-administered both cosmetic products (enriched and placebo) on day 0, in a randomized temporal order. From day 1 to day 28, half of them self-administered (at home, twice a day, at wake-up and bed time) the enriched cosmetic product (ECP), the other half the placebo cream (PCP).
ECP natural functional aroma was a 100% blend of Juniperus phoenicea gum extract, Copaifera officinalis resin, Aniba rosaeodora wood oil and Juniperus virginiana oil. The two cosmetic products were applied with a mindful massage (see https://www.youtube.com/watch?v=Mup9zgP1U14 for details). PCP was devoid of aroma and active ingredients.
Psychometric assessment
The severity of trait anxiety was measured using the trait version of the State-Trait Anxiety Inventory (STAI-Y) (Spielberger et al., Citation1983), which is a 4-point Likert scale consisting of 20 items assessing how the patient feels, independent from the status and circumstances (e.g., “I feel secure,” I feel troubled”). The lowest score that can be obtained is 20 and the highest is 80: higher scores indicate higher anxiety levels. The validity of this scale has been repeatedly confirmed, with reliability coefficients ranging from 0.71 to 0.86 and internal consistency and homogeneity coefficients between 0.83 and 0.87 (Spielberger et al., Citation1983). This questionnaire was adminsitered on day -2. State anxiety was measured using the state version of the STAI, which asks how respondents feel “right now” using 4-point Likert scale items that measure subjective feelings of apprehension, tension, nervousness, worry, and activation/arousal of the autonomic nervous system. The reliability coefficient is 0.62. This questionnaire was adminstered twice on day 29, just before and just after the PST.
The Perceived Stress Scale (PSS) is the most widely used psychological instrument for measuring the perception of stress. It is a measure of the degree to which situations in one’s life are appraised as stressful. Items were designed to tap how unpredictable, uncontrollable, and overloaded respondents find their lives. The 10 questions that compose this test are related to feelings and thoughts experienced during the last month. In each case, respondents are asked how often they felt a certain way. The questionnaire was administered on day -2 and day 29. Scores ranging from 14–26 are considered “moderate perceived stress,” those ranging from 27–40 are considered “high perceived stress” (Cohen et al., Citation1983).
The Profile of Mood States (POMS) is a a wide-spread instrument to measure psychological well-being (McNair, Lorr & Droppleman, 1971). It is a rating scale that measures 6 distinct mood states, namely tension-anxiety (TA), depression-dejection (DD), anger-hostility (AH), fatigue-inertia (FI), confusion-bewilderment (CB), and vigor-activity (VA). Subjects were asked to report the intensity of these six different dimensions of mood as they felt them during the last week. An overall score of mood profile (POMS score) can be drawn by summing the scores obtained in each of the five “negative” factors and subtracting the single positive factor (VA). The questionnaire was administred on day –2 and day 29.
Ethological analysis
Non-verbal behavior during the stress interview phase of the PST was analyzed by means of the Ethological Coding System for Interviews (ECSI) by a trained observer. The ECSI is a modified version of Grant’s ethogram (Grant, Citation1968; Troisi, Citation1999) and is designed to measure 37 different patterns of non-verbal behaviors, which are grouped in eight macro categories that reflect the subject’s intention to communicate a certain mood or intention and show different aspects of individual’s psychosocial attitude (Dixon & Fisch, 1998). Before the beginning of the study, the observer was trained until she reached an adequate level of inter-observer reliability. Assessment of inter-observer reliability was based on a sample of 30 interviews not including those with the subjects of this study. Recording method was one-zero sampling. The recording session was divided into successive 15-second sample intervals. The instant of time at the end of each sample interval, referred to as the “sample point,” was identified by a beeper. On the instant of each sample point, the observer recorded whether or not the behavior pattern had occurred during the preceding sample interval. The score of each behavior for each subject was expressed as the proportion of all sample intervals during which that behavior occurred (see Troisi, Citation1999, for details). One-zero scores are highly correlated with both frequency and duration measures of the same behavior, which means that they give a composite measure of “amount” of behavior. Using a short sample interval (e.g., 15 seconds), the scores obtained using one-zero sampling and continuous recording are highly correlated (Troisi, Citation1999). Briefly, the following categories were considered: (1) eye contact, which expresses involvement and attention, (2) affiliation, a positive attitude that promotes social interaction; (3) submission, whose purpose is to maintain non hostile social interaction; (4) flight, which includes all the non-verbal patterns of behavior aimed at avoiding social stimuli that are perceived as harmful or stressful, (5) assertion, which includes all the facial expressions and hand movements indicating a low level of aggressiveness, (6) gesture, which is a reliable index of global psychomotor activity and includes all the hand movements that illustrate and reinforce the contents of a speech, (7) displacement, which includes all the movements that are focused on one’s own body or addressed to manipulate external objects, and (8) relaxation, which indicates a low level of emotional arousal.
Heart rate and heart rate variability data
ECG signals were converted to digital, transferred to a laptop computer via Bluetooth technology, pre-processed in a Matlab environment, and analyzed by means of Chart5 software (ADInstruments, Sydney, Australia). Initially, each raw ECG signal was manually inspected to ensure that all R-waves were correctly detected. For each recording period, ECGs were split in 5-min epochs. For each epoch, we then calculated HR (bpm) and quantified two frequency-domain indexes of HRV, namely the power of the high frequency band (HF; 0.15–0.4 Hz) in normalized units (nu), and the low frequency (LF; 0.04–0.15 Hz) to high frequency ratio (LF/HF). The HFnu carries information about the relative contribution of cardiac vagal influence when breathing rates are between nine cycles per minute (0.15 Hz) and up to 24 cycles per minute (0.40 Hz) (Laborde et al., Citation2017). Therefore, respiratory rate was controlled online via a respiratory belt connected to the BT16Plus device (Francesco Marazza Hardware & Software, Monza, IT) to ascertain that participants were breathing “normally” throughout all the phases of PST.
The LF/HF ratio estimates the fractional distribution of power and is taken as a measure of cardiac sympathovagal balance, where lower values indicate a larger vagal predominance (Montano et al., Citation1994).
Salivary cortisol level determinations
Immediately after collection, saliva samples were frozen at −20 °C until analysis. Salivary cortisol levels were determined by enzyme linked immunosorbent assay (ELISA). Samples were thawed, brought to room temperature and centrifuged (1500 g × 10 min), resulting in a clear supernatant of low-viscosity. Cortisol levels were assayed in duplicates following kit instructions with a 96-well plate enzyme-linked immunosorbent assay (High Sensitivity Salivary Cortisol Enzyme Immunoassay Kit: Salimetrics LLC, State College, PA), using Infinite F50 plate reader and Magellan software (TecanGroup Ltd, Männedorf, Switzerland). To avoid inter-assay variability all samples from the same participant were assayed in the same batch. The inter-assay and intra-assay coefficients of variability were 9.4% and 8.3%, respectively. Salivary cortisol levels during the various experimental phases of the two laboratory sessions (day 0 and day 29) were calculated as absolute values.
Statistical analyses
All statistical analyses were performed using SPSS 25 software package (SPSS Inc., Chicago, IL, USA). Statistical significance was set at p < .05. Socio-demographic, anthropometric and lifestyle factors were compared between the two groups using independent t-tests and Chi-square tests, as appropriate. STAI-T scores were compared between the two groups using independent t-tests.
PSS and POMS score comparisons were performed by means of two-way ANOVAs for repeated measures, with “group” as between-subject factor (two levels: ECP and PCP) and “time” as within-subject factor (two levels: day -2 and 29).
To test for the acute effects of ECP and PCP on baseline physiological parameters, one-way ANOVAs for repeated measures, with “condition” as within-subject factor (three levels: baseline, ECP, PCP), were applied for: (i) HR and HRV data, (ii) cortisol levels.
To test for the effects of the stressor (PST, day 29) on the physiological parameters of the two women groups, two-way ANOVAs for repeated measures were used, with “group” as between-subject factor (two levels: ECP and PCP) and “recording epoch” as within-subject factor (nine levels: bas, s1 and s2, r1 to r6).
To test for the long-term effects of ECP on baseline physiological parameters, two-way ANOVAs for repeated measures, with “group” as between-subject factor (two levels: ECP and PCP) and “time” as within-subject factor (two levels: day 0 and day 29) were applied for: (i) HR and HRV data, (ii) cortisol levels.
Follow-up analyses were conducted using Student’s t-tests, with a Bonferroni correction for multiple comparisons.
Flowchart
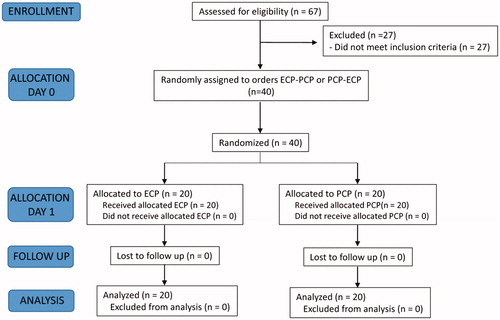
The flowchart of the study procedures is depicted in .
Figure 3. Flowchart of the study procedures.
Results
Anthropometric, lifestyle and psychological data at the beginning of the study
ECP and PCP women were well matched regarding anthropometric and lifestyle characteristics, as well as preliminary psychometric (trait anxiety) profile, as depicted in .
Table 1. Antropometric, lifestyle and psychometric characteristics of ECP (enriched cosmetic product) and PCP (placebo cosmetic product) women at the beginning of the study.
Enriched cosmetic product effects on perceived stress (PSS), state anxiety (STAI-S) and mood states (POMS)
Four-week, twice × day, self-administration of the cosmetic product induced a significant reduction of perceived stress scores in both experimental groups (two-way ANOVA, significant effect of time, F = 14.2, p < .01, ηp2= 0.27), with no difference between the two treatments (PCPday-2 = 18.4 ± 1.4 vs. PCPday29 = 16.1 ± 1.4; ECPday-2 = 18.5 ± 11.2 vs. ECPday29 = 15.4 ± 1.3).
Two‐way ANOVA applied to state‐anxiety scores yielded a significant effect of time (F = 5.1, p < .05, ηp2 = 0.12) and a time × treatment interaction (F = 6.6, p < .05, ηp2 = 0.15). On day 29, state anxiety levels were significantly lower at the end of the psychosocial stress test (post-PST) compared to pre‐PST levels in ECP women (postPST = 33.1 ± 1.6 vs. prePST = 39.0 ± 2.5, p < .01, ηp2 = 0.23), but not in PCP counterparts (postPST = 34.1 ± 1.4 vs. prePST = 36.3 ± 1.9, p > 0.05, ηp2 = 0.01).
POMS data for ECP and PCP women, expressed as difference values between day29 and day-2 scores, are summarized in . T values pointed to significant differences for DD (t = 2.0, p < .05), AH (t = 2.4, p < .05), FI (t = 2.6, p < .05) and CB (t = 3.1, p < .01) delta scores between ECP and PCP women, suggesting a reduction in depression, anger, fatigue and confusion (together with a mild reduction in tension, t = 1.9, p = 0.068) in ECP women, which was not seen in PCP counterparts. T value for overall POMS delta score also indicated a significant difference between ECP and PCP subjects.
Table 2. Partial and overall POMS (Profile of Mood States) scores for ECP (enriched cosmetic product) and PCP (placebo cosmetic product) women, expressed as difference values between day29 and day-2 scores.
Enriched cosmetic routine effects on non-verbal behavior during the psychosocial stress test
The analysis of non-verbal behavior during the stress interview phase of the PST yelded the results summarized in .
Figure 4. Scores of non verbal behavior categories exhibited during the SI (stress interview) phase of the PST (psychosocial stress test) by PCP (placebo cosmetic product) and ECP (enriched cosmetic product) women. EC: eye contact; AF: affiliation; SUB: submission; FLIG: flight; ASS: assertion; DISP: displacement; RELAX: relaxation; GEST: gesture. *p < .05 and §p < .01 vs. placebo.
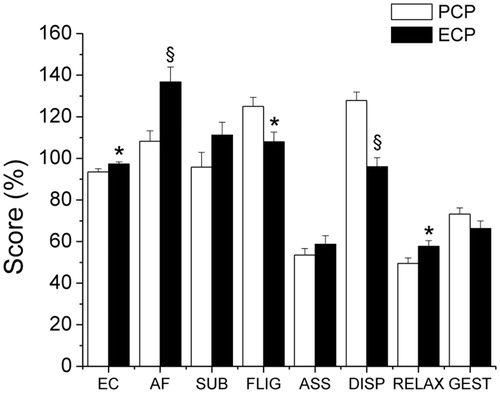
Women self-administering for four weeks (twice × day) the enriched cream (ECP) exhibited significant score differences as compared to control women (PCP) for the following behavioral categories: eye contact (EC, t = 2.1, p < .05, d = 0.66), affiliation (AF, t = 3.3, p < .01, d = 1.04) flight (FLIG, t = 2.7, p < .05, d = 0.85), displacement (DISP, t = 5.3, p < .01, d = 1.68) and relaxation (RELAX, t = 2.2, p < .05, d = 0.69).
Heart rate, heart rate variability and cortisol on recording session 1
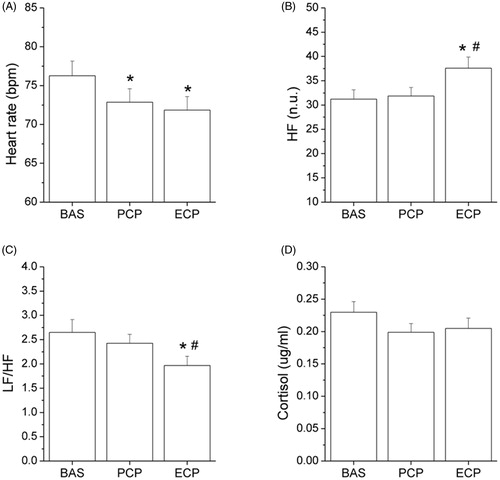
Heart rate, heart rate variability, and saliva cortisol values obtained during recording session 1 (namely, just before and just after the first self-administration of the two creams, acute effect) are reported in . One-way ANOVA yielded a significant effect of condition for HR (F = 41.2, p < .01, ηp2 = 0.52), HFnu (F = 17.2, p < .01, ηp2 = 0.31) and LF/HF (F = 9.7, p < .01, ηp2 = 0.20). The two cosmetic products produced similar, significant bradycardic effects (ECP vs. baseline: p < .01, ηp2 = 0.65; PCP vs. baseline: p < .01, ηp2 = 0.65) (panel A). However, only ECP produced a significant change in HFnu (ECP vs. baseline: p < .01, ηp2 = 0.43; ECP vs. PCP: p < .01, ηp2 = 0.43; panel B) and in LF/HF (ECP vs. baseline: p < .01, ηp2 = 0.36; ECP vs. PCP: p < .01;ηp2 = 0.36; panel C). The two cosmetic products produced only minor effects (non significant reductions) on saliva cortisol levels (panel D).
Figure 5. Heart rate, heart rate variability (HFnu and LF/HF), and saliva cortisol values obtained before and after the first self-administration of the two cosmetic products (recording session 1, day 0). HF(n.u.): high frequency band power in normalized units; LF: low frequency band power. *p < .05 vs. baseline; #p < .05 vs. placebo.
Heart rate, heart rate variability and cortisol on recording session 2
Heart rate, heart rate variability, and saliva cortisol values obtained during recording session 2 (namely, just before, during and just after the psychosocial stress test) are reported in . Two-way ANOVA for repeated measures yelded significant effects of time for HR (F = 79.3, p < .01, ηp2 = 0.68), HFnu (F = 8.3, p < .01, ηp2 = 0.19), and LF/HF (F = 6.6, p < .01, ηp2 = 0.19). Specifically, HR was significantly higher in both groups compared to the respective baseline values during the psychosocial stress test (p < .01 for both groups) (panel A). Moreover, HFnu was significantly lower and LF/HF significantly higher in both groups compared to the respective baseline values during the psychosocial stress test and the first 5 min of the recovery period (HFnu: p < .01 for ECP, p < .05 for PCP; LF/HF: p < .01 for both groups) (panels B and C).
Figure 6. Heart rate, heart rate variability (HFnu and LF/HF), and saliva cortisol values obtained before, during and after the psychosocial stress test (PST, recording session 2, day 29), from ECP (enriched cosmetic product) and PCP (placebo cosmetic product) women. HF(n.u.): high frequency band power in normalized units; LF: low frequency band power; bas: baseline, mean value of the two 5-min recording epochs in resting conditions; s1 and s2: first (stress interview) and second (arithmetic task) phases of the PST; r1–r6: consecutive 5-min recording epochs of the post-stress (recovery) phase. *p < .05 vs. baseline; #p < .05 vs. placebo.
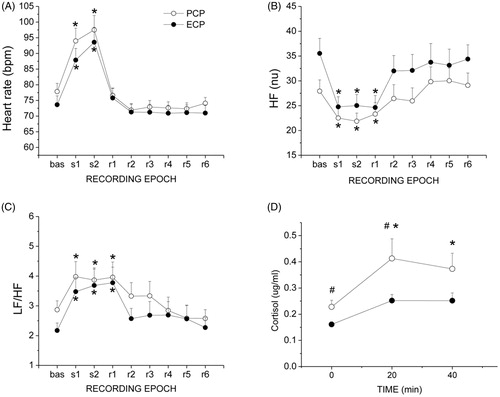
Significant effects of both group (F = 3.7, p < .05, ηp2 = 0.11) and time (F = 11.6, p < .01, ηp2 = 0.25) were found only for cortisol values. PCP group values of cortisol were significantly higher compared to baseline at min 20 (p < .05, ηp2 = 0.29) and 40 (p < .05, ηp2 = 0.29) (panel D). On the contrary, ECP group values of cortisol were not increased by the stressor, neither at min 20 nor at min 40. At min 0 and 20, ECP group cortisol levels were significantly lower compared to PCP corresponding levels (min 0: p < .05, ηp2 = 0.08; min 20: p < .05, ηp2 = 0.10)(panel D).
Comparison of baseline delta values before and after 4-week self-administration of the cream for HR, HFnu, LF/HF and cortisol did not yeld any significant difference between ECP and PCP women ().
Table 3. Changes in baseline values for heart rate (HR), high frequency band power (HFnu), LF/HF ratio, and cortisol levels, following 4-week self-administration of the placebo (PCP) or enriched (ECP) cosmetic product.
Discussion
The present study showed that a single application of a cosmetic routine - based on the self-administration of a cosmetic product with a pleasurable texture, enriched with four essential oils and applied with a mindful massage - produced an acute potentiation of cardiac parasympathetic modulation, which was not observed when a placebo cosmetic product was used. Prolonged self-administration of this same routine (twice a day per 4 consecutive weeks) induced: (i) a dampening of the typical cortisol rise produced by a brief psychosocial challenge, (ii) a reduction of perceived state anxiety, (iii) a favorable change in mood profile, and (iv) a reduction of non-verbal behavior patterns that signal anxiety, motivational conflict and avoidance, as well as a potentiation of those that indicate affiliation and relaxation.
The acute effects here reported are in line with previous studies documenting the favorable impact of aromatherapy (applied either topically, orally or by inhalation) on a number of autonomic function parameters (Chang & Shen, Citation2011; Hongratanaworakit, Citation2011). However, to the best of our knowledge, this is the first study documenting the physiological effects of the administration of an aromatherapeutic cosmetic product to the face skin (transdermal absorption).
The observed acute increase of parasympathetic modulation at the level of the heart – as signaled by increased HF index scores - bears important prevention and treatment implications, in view of the broadly acknowledged evidence that decreased HRV is a risk factor for all-cause morbidity and mortality (Norman et al., Citation2012; Tsuji et al., Citation1994) Indeed, several physiologic systems that are important for stress, health, and disease have been linked to vagal function and HRV, including glucose regulation pathways, HPA axis function, and a number of allostatic systems (Thayer & Lane, Citation2009). In other words, enhanced vagal tone is an indicator of cardiac health, representing behavioral and physiological flexibility of an organism, as well as its ability to adapt in response to stress. Substantial vagal tone reduction is a marker of decreased behavioral, physiological and stress response flexibility (Porges, Citation1995). The present study suggests that a cosmetic routine that blends aromatherapy with mindful massage, through its capacity to acutely regulate HRV and potentiate the vagal component of autonomic neural regulation, might possibly represent an interesting tool for preventing or reversing stress-related psychosomatic and psychological dysfunctions. Needless to say that the potential usefulness of this stress relief approach is further supported by its application easiness.
The other intriguing outcome of the present study is the impact of the enriched cosmetic routine on adrenocortical stress responsivity. Resting salivary cortisol levels were not modified by prolonged application of the enriched product. However, salivary cortisol concentrations indicated that repeated applications of the cosmetic protocol produced a remarkable reduction of the activation of the HPA axis that typically follows a brief psychosocial challenge. Considering the role of stress as a risk factor for psychiatric/psychosomatic disease, it is not surprising that cortisol stress reactivity has frequently been investigated both in patients and healthy individuals. Together with the sympathoadrenal system (producing adrenaline) that fuels fight-or-flight responses, the hypothalamic-pituitary-adrenal (HPA) axis forms the main effector of mammalian neuroendocrine stress response. Under threat, limbic and cortical regions (e.g., amygdala, hippocampus, prefrontal cortex) convey signals through multi-synaptic pathways to the paraventricular nucleus of the hypothalamus. There, corticotropin releasing hormone (CRH) release is stimulated, which in turn stimulates the anterior portion of the pituitary gland causing the release of adrenocorticotropic hormone (ACTH). Once in the general circulation, ACTH stimulates cells in the adrenal gland cortex that produce cortisol (Ulrich-Lai & Herman, 2009). Cortisol produces broad effects in the body and brain, mobilizing energy for prolonged action, helping to store memories for meaningful events, and inhibiting the activity of the immune system. These and other actions support our capability to cope with stressors, which is adaptive in the short-term. However, when the system is repeatedly activated due to chronic stressors, excessive “wear and tear” is placed on the organism (McEwen, Citation2008). In other words, the general idea is that sustained elevations of HPA axis outflow might represent a mechanism through which prolonged stress exerts its pathogenic effects. Indeed, prolonged, excessive activation of the HPA axis may lead to functional/structural changes in specific brain regions (e.g., BDNF downregulation in the hippocampus) and may subsequently result in the development of stress-related disorders (Mc Ewen, Citation2004). Thus, individuals who are buffered from excessive elevations in stress hormones are likely going to enjoy better health in the long run.
As far as the psychological/behavioral effects of this study are concerned, prolonged (4 weeks) twice daily self-administration of the enriched cosmetic routine produced a significant, favorable change of mood profile (overall POMS test score). In particular, depression-dejection, anger-hostility, fatigue-inertia, and confusion-bewilderment scores were all largely reduced as compared to pretreatment evaluation, and were remarkably lower as compared to control women corresponding values. Vigor-activity score, on the other hand, was significantly increased by prolonged enriched product application, an effect that was not found in women self-administering the placebo one.
Similarly, the enriched cosmetic routine produced a reduced score of perceived anxiety (STAI test) following the laboratory stressor as compared to pre-stressor value. These effects were not observed in those women that made use of the placebo cream. This result resembles that obtained by means of dorsolateral prefrontal cortex transcranial direct current stimulation applied during the same laboratory stress condition, supporting the general idea that the activity of this brain area is critically involved in the neurocircuitry that regulates stress-related anxiety (Carnevali et al., Citation2020).
The results of perceived stress self-evaluation, as obtained via the perceived stress scale (PSS), did not suggest a specific stress relief effect of 4-week, twice × day, self-administration of the enriched cosmetic routine. Indeed, placebo treatment produced similar reductions of perceived stress scores. This evidence might be explained by considering that pretreatment values of perceived stress were already quite low in the whole study population (group means close to the lower value of the range 14–26, corresponding to “moderate perceived stress”) (Cohen et al., Citation1983).
Interestingly, women making use of the enriched cosmetic product exhibited (during the interview phase of the psychosocial stress test) a significantly smaller amount of behavioral patterns that signal flight and displacement, which may reflect their reduced levels of avoidance behavior and anxiety (Troisi, Citation1999). In addition, these women were also characterized by a larger frequency of eye contact and affiliative behaviors as compared to placebo counterparts. Such prosocial behaviors are believed to reflect an attempt to maintain a non-hostile interaction with and to elicit empathy in the interviewer (Pattini et al., Citation2019). Finally, prolonged enriched cosmetic product self-administration also favored relaxation during the psychosocial stress test, as signaled by larger scores of this behavioral category when compared to placebo using women.
It must be acknowledged, however, that no significant linear correlations were found between non-verbal behavior and physiological responses to the PST, which is in contrast with a previous study documenting, for instance, a positive relationship between submissive behavior scores and the magnitude of autonomic and cortisol responses to a psychosocial stress test in healthy university students (Sgoifo et al., Citation2003).
Limitations
This exploratory study was performed on a relatively small sample of healthy female participants and, therefore, one has to be cautious about generalizing its results and suggesting tentative applications to general or patient populations. Future work with larger samples is needed to test whether the present results generalize to men or to a population with a higher variation in age and health. Moreover, a striking and consistent feature of HPA axis responses to acute psychosocial stress is their remarkable inter-individual variability. Altough the two groups were homogeneous for a number of anthropometric, lifestyle and psychological characteristics at the time of the testing, we cannot rule out the possibility that other factors contributed to the observed variation in cortisol stress reactivity (Zänkert et al., Citation2019). Furthermore, since blinding perception may have changed during the study, it would be important to ascertain whether the documented changes might be ascribable to changes in attributed self-relevance and efficacy of the self-administred cosmetic product. Indeed, participants blinding was not checked at the end of the experiment, although it has to be emphasized that women assigned to both treatments were told that they were self-administering a cosmetic product with possible stress relief properties. Also, we did not check for compliance with prolonged (4 weeks), twice-daily self-administration. Lastly, given that the control cream did not contain any aroma or active ingredients, the putative cause for the beneficial impact of the cosmetic cream (only the smell or the oils themselves regardless of smell) cannot be isolated.
One might also argue that the HRV parameters used to assess cardiac symapthovagal balance were calculated only in the frequency domain. Although complex techniques have been developed based on nonlinear dynamics and chaos theory that are able to evaluate in greater detail the intrinsic complexity of HRV, these sophisticated tools are mathematically complicated, they require more powerful computing, and they are still under development and evaluation (Sgoifo et al., Citation2015).
Conclusions
Everyday life psychosocial stressors contribute to poor health and disease vulnerabilty. Alternative means that are able to foster stress resilience and protect from stress-related mental and physical dysfunctions are more and more under the magnifying glass of biomedical research. In particular, evidence is accumulating on the beneficial impact of aromatherapy on psychophysiological stress responsivity. The present study suggests that a beauty routine based on the self-administration of a cosmetic product with a pleasurable texture, enriched with essential oils and applied with a mindful massage should be considered as a stress resilience fostering strategy with acute and long lasting physiological, neuroendocrine and psychological effects.
Acknowledgements
This work was financially supported by Davines s. p.a. (Parma – Italy). Davines s.p.a. also devised and produced the cosmetics used in this study.
Disclosure Statement
As corresponding author of this paper, in accordance with Taylor & Francis policy and ethical obligations as a researcher, I am reporting that I received funding for this study from Davines s. p.a. (Parma, Italy).
Additional information
Funding
Notes on contributors
A. Sgoifo
Andrea Sgoifo and Luca Carnevali conceived and designed the experiments.
Andrea Sgoifo, Luca Carnevali, Elena Pattini and Angelica Carandina performed the experiments and analyzed the data.
G. Tanzi
Giulia Tanzi, Carlotta Del Canale, Paolo Goi, Mauro Fornari, Barbara Gavazzoli, Luisa Poisa, Davide Manzoni, and Davide Bollati revised the article critically for importantintellectualcontent.
M. B. De Felici del Giudice
Maria Beatrice de Felici del Giudice and Beatrice De Carne devised cosmetic product preparation.
References
- Balconi, M., Fronda, G., & Crivelli, D. (2019). Effects of technology-mediated mindfulness practice on stress: Psychophysiological and self-report measures. Stress, 22(2), 200–209. doi:10.1080/10253890.2018.1531845
- Carnevali, L., Pattini, E., Sgoifo, A., & Ottaviani, C. (2020). Effects of prefrontal transcranial direct current stimulation on autonomic and neuroendocrine responses to psychosocial stress in healthy humans. Stress, 23(1), 26–36. doi:10.1080/10253890.2019.1625884
- Chang, K. M., & Shen, C. W. (2011). Aromatherapy benefits autonomic nervous system regulation for elementary school faculty in Taiwan. Evidence-Based Complementary and Alternative Medicine, 2011, 1–7. doi:10.1155/2011/946537
- Chien, L. W., Cheng, S. L., & Liu, C. F. (2012). The effect of lavender aromatherapy on autonomic nervous system in midlife women with insomnia. Evidence-Based Complementary and Alternative Medicine, 2012, 1–8. doi:10.1155/2012/740813
- Chu, I. H., Wu, W. L., Lin, I. M., Chang, Y. K., Lin, Y. J., & Yang, P. C. (2017). Effects of yoga on heart rate variability and depressive symptoms in women: a randomized controlled trial. The Journal of Alternative and Complementary Medicine, 23(4), 310–316. doi:10.1089/acm.2016.0135
- Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396. doi:10.2307/2136404
- Cummings, D. M., Kirian, K., Howard, G., Howard, V., Yuan, Y., Muntner, P., Kissela, B., Redmond, N., Judd, S. E., & Safford, M. M. (2016). Consequences of comorbidity of elevated stress and/or depressive symptoms and incident cardiovascular outcomes in diabetes: results from the reasons for Geographic And Racial Differences in Stroke (REGARDS) Study. Diabetes Care, 39(1), 101–109. doi:10.2337/dc15-1174
- de Siqueira, R. J., Rodrigues, K. M., da Silva, M. T., Correia Junior, C. A., Duarte, G. P., Magalhães, P. J., dos Santos, A. A., Maia, J. G., da Cunha, P. J., & Lahlou, S. (2014). Linalool-rich rosewood oil induces vago-vagal bradycardic and depressor reflex in rats. Phytotherapy Research, 28(1), 42–48. doi:10.1002/ptr.4953
- Dixon, A. K., & Fisch, H. U. (1998). Animal models and ethological strategies for early drug-testing in humans. Neuroscience & Biobehavioral Reviews, 23(2), 345–358. doi:10.1016/S0149-7634(98)00036-0
- Elofsson, U. O., von Schèele, B., Theorell, T., & Söndergaard, H. P. (2008). Physiological correlates of eye movement desensitization and reprocessing. Journal of Anxiety Disorders, 22(4), 622–634. doi:10.1016/j.janxdis.2007.05.012
- Ennajar, M., Bouajila, J., Lebrihi, A., Mathieu, F., Abderraba, M., Raies, A., & Romdhane, M. (2009). Chemical composition and antimicrobial and antioxidant activities of essential oils and various extracts of Juniperusphoenicea L. (Cupressacees). Journal of Food Science., 74, 364–371. doi:10.1111/j.1750-3841.2009.01277.x
- Finch, L. E., Cummings, J. R., & Tomiyama, A. J. (2019). Cookie or clementine? Psychophysiological stress reactivity and recovery after eating healthy and unhealthy comfort foods. Psychoneuroendocrinology, 107, 26–36. doi:10.1016/j.psyneuen.2019.04.022
- Goes, T. C., Antunes, F. D., Alves, P. B., & Teixeira-Silva, F. (2012). Effect of sweet orange aroma on experimental anxiety in humans. The Journal of Alternative and Complementary Medicine, 18(8), 798–801. doi:10.1089/acm.2011.0551
- Grant, E. C. (1968). An ethological description of nonverbal behaviour during interviews. British Journal of Medical Psychology, 41(2), 177–184. doi:10.1111/j.2044-8341.1968.tb02022.x
- Guimarães-Santos, A., Santos, D. S., Santos, I. R., Lima, R. R., Pereira, A., de Moura, L. S., Carvalho, R. N., Lameira, O., & Gomes-Leal, W. ( (2012). 2012). Copaiba oil-resin treatment is neuroprotective and reduces neutrophil recruitment and microglia activation after motor cortex excitotoxic injury. Evidence-Based Complementary and Alternative Medicine, 2012, 1–9. doi:10.1155/2012/918174
- Haiblum-Itskovitch, S., Czamanski-Cohen, J., & Galili, G. (2018). Emotional response and changes in heart rate variability following art-making with three different art materials. Frontiers in Psychology, 9, 968. doi:10.3389/fpsyg.2018.00968
- Haze, S., Sakai, K., & Gozu, Y. (2002). Effects of fragrance inhalation on sympathetic activity in normal adults. The Japanese Journal of Pharmacology, 90(3), 247–253. doi:10.1254/jjp.90.247
- Hongratanaworakit, T. (2011). Aroma-therapeutic effects of massage blended essential oils on humans. Natural Product Communications, 6(8), 1199–1204. doi: 10.1177/1934578X1100600838.
- Huang, L., & Capdevila, L. (2017). Aromatherapy improves work performance through balancing the autonomic nervous system. The Journal of Alternative and Complementary Medicine, 23(3), 214–221. doi:10.1089/acm.2016.0061
- Hunter, M. R., Gillespie, B. W., & Chen, S. Y. (2019). Urban nature experiences reduce stress in the context of daily life based on salivary biomarkers. Frontiers in Psychology, 10, 722. doi:10.3389/fpsyg.2019.00722
- Kiecolt-Glaser, J. K., Graham, J. E., Malarkey, W. B., Porter, K., Lemeshow, S., & Glaser, R. (2008). Olfactory influences on mood and autonomic, endocrine, and immune function. Psychoneuroendocrinology, 33(3), 328–339. doi:10.1016/j.psyneuen.2007.11.015
- Kirschbaum, C., Pirke, K. M., & Hellhammer, D. H. (1993). The ‘trier social stress test’–a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology, 28(1-2), 76–81. doi:10.1159/000119004
- Kuroda, K., Inoue, N., Ito, Y., Kubota, K., Sugimoto, A., Kakuda, T., & Fushiki, T. (2005). Sedative effects of the jasmine tea odor and (R)-(–)-linalool, one of its major odor components, on autonomic nerve activity and mood states. European Journal of Applied Physiology, 95(2–3), 107–114. doi:10.1007/s00421-005-1402-8
- Laborde, S., Mosley, E., & Thayer, J. F. (2017). Heart rate variability and cardiac vagal tone in psychophysiological research - recommendations for experiment planning, data analysis, and data reporting. Frontiers in Psychology, 8, 213. doi:10.3389/fpsyg.2017.00213
- Leandro, L. M., Vargas, F., de, S., Barbosa, P. C., Neves, J. K., da Silva, J. A., & da Veiga-Junior, V. F. (2012). Chemistry and biological activities of terpenoids from copaiba (Copaifera spp.) oleoresins. Molecules, 17(4), 3866–3889. doi:10.3390/molecules17043866
- Liu, S. H., Lin, T. H., & Chang, K. M. (2013). The physical effects of aromatherapy in alleviating work-related stress on elementary school teachers in Taiwan. Evidence-Based Complementary and Alternative Medicine, 2013, 1–7. doi:10.1155/2013/853809
- Matsumoto, T., Asakura, H., & Hayashi, T. (2013). Does lavender aromatherapy alleviate premenstrual emotional symptoms? A randomized crossover trial. BioPsychoSocial Medicine, 7(1), 12. doi:10.1186/1751-0759-7-12
- Mc Ewen, B. S. (2004). Protection and damage from acute and chronic stress: allostasis and allostatic overload and relevance to the pathophysiology of psychiatric disorders. Ann. N. Y. Acad. Sci, 1032, 1–7. doi:10.1196/annals.1314.001
- McEwen, B. S. (1998). Protective and damaging effects of stress mediators. New England Journal of Medicine, 338(3), 171–179. doi:10.1056/NEJM1998011533803074
- McEwen, B. S. (2008). Central effects of stress hormones in health and disease: Understanding the protective and damaging effects of stress and stress mediators. European Journal of Pharmacology., 583(2-3), 174–185. doi:10.1016/j.ejphar.2007.11.071
- McNair, D. M., Lorr, M., & Droppleman, L. F. (1971). Manual for the Profile of Mood States. Educational and Industrial Testing Services.
- Montano, N., Ruscone, T. G., Porta, A., Lombardi, F., Pagani, M., & Malliani, A. (1994). Power spectrum analysis of heart rate variability to assess the changes in sympathovagal balance during graded orthostatic tilt. Circulation, 90(4), 1826–1831. doi:10.1161/01.CIR.90.4.1826
- Niijima, A., & Nagai, K. (2003). Effect of olfactory stimulation with flavor of grapefruit oil and lemon oil on the activity of sympathetic branch in white adipose tissue of the epididymis. Experimental Biology and Medicine, 228(10), 1190–1192. doi:10.1177/153537020322801014
- Norman, G. J., Karelina, K., Berntson, G. G., Morris, J. S., Zhang, N., & Devries, A. C. (2012). Heart rate variability predicts cell death and inflammatory responses to global cerebral ischemia. Frontiers in Physiology, 3, 131doi:10.3389/fphys.2012.00131
- Pattini, E., Carnevali, L., Troisi, A., Matrella, G., Rollo, D., Fornari, M., & Sgoifo, A. (2019). Psychological characteristics and physiological reactivity to acute stress in mothers of children with. Stress and Health, 35(4), 421–431. doi:10.1002/smi.2870
- Peng, S. M., Koo, M., & Yu, Z. R. (2009). Effects of music and essential oil inhalation on cardiac autonomic balance in healthy individuals. The Journal of Alternative and Complementary Medicine, 15(1), 53–57. doi:10.1089/acm.2008.0243
- Pico-Alfonso, M. A., Mastorci, F., Ceresini, G., Ceda, G. P., Manghi, M., Pino, O., Troisi, A., & Sgoifo, A. (2007). Acute psychosocial challenge and cardiac autonomic response in women: the role of estrogens, corticosteroids, and behavioral coping styles. Psychoneuroendocrinology, 32(5), 451–463. doi:10.1016/j.psyneuen.2007.02.009
- Porges, S. W. (1995). Cardiac vagal tone: a physiological index of stress. Neuroscience & Biobehavioral Reviews., 19(2), 225–233. doi:10.1016/0149-7634(94)00066-A
- Saeki, Y. (2000). The effect of foot-bath with or without the essential oil of lavender on the autonomic nervous system: a randomized trial. Complementary Therapies in Medicine, 8(1), 2–7. doi:10.1016/S0962-4562(00)80011-9
- Sgoifo, A., Braglia, F., Costoli, T., Musso, E., Meerlo, P., Ceresini, G., & Troisi, A. (2003). Cardiac autonomic reactivity and salivary cortisol in men and women exposed to social stressors: relationship with individual ethological profile. Neuroscience & Biobehavioral Reviews, 27(1-2), 179–188. doi:10.1016/S0149-7634(03)00019-8
- Sgoifo, A., Carnevali, L., Pico-Alfonso, M. A., & Amore, M. (2015). Autonomic dysfunction and heart rate variability in depression. Stress, 18(3), 343–352. doi:10.3109/10253890.2015.1045868
- Sgoifo, A., Koolhaas, J., Alleva, E., Musso, E., & Parmigiani, S. (2001). Social stress. acute and long-term effects on physiology and behavior. Physiology & Behavior, 73(3), 253–254. doi:10.1016/S0031-9384(01)00544-3
- Shen, J., Niijima, A., Tanida, M., Horii, Y., Maeda, K., & Nagai, K. (2005). Olfactory stimulation with scent of grapefruit oil affects autonomic nerves, lipolysis and appetite in rats. Neuroscience Letters, 380(3), 289–294. doi:10.1016/j.neulet.2005.04.010
- Shiina, Y., Funabashi, N., Lee, K., Toyoda, T., Sekine, T., Honjo, S., Hasegawa, R., Kawata, T., Wakatsuki, Y., Hayashi, S., Murakami, S., Koike, K., Daimon, M., & Komuro, I. (2008). Relaxation effects of lavender aromatherapy improve coronary flow velocity reserve in healthy men evaluated by transthoracic Doppler echocardiography. International Journal of Cardiology, 129(2), 193–197. doi:10.1016/j.ijcard.2007.06.064
- Spielberger, C. D., Gorsuch, R. L., Lushene, R., Vagg, P. R., & Jacobs, G. A. (1983). Manual for the State-Trait inventory. Consulting Psychologist Press.
- Thayer, J. F., & Lane, R. D. (2009). Claude Bernard and the heart-brain connection: further elaboration of a model of neurovisceral integration. Neuroscience & Biobehavioral Reviews, 33(2), 81–88. doi:10.1016/j.neubiorev.2008.08.004
- Troisi, A. (1999). Ethological research in clinical psychiatry: The study of nonverbal behavior during interviews. Neuroscience & Biobehavioral Reviews, 23(7), 905–913. doi:10.1016/S0149-7634(99)00024-X
- Tsuji, H., Venditti, F. J., Manders, E. S., Evans, J. C., Larson, M. G., Feldman, C. L., & Levy, D. (1994). Reduced heart rate variability and mortality risk in an elderly cohort. The framingham heart study. Circulation, 90(2), 878–983. doi:10.1161/01.CIR.90.2.878
- Ulrich-Lai, Y. M., & Herman, J. P. (2009). Neural regulation of endocrine and autonomic stress responses. Nature Reviews Neuroscience, 10(6), 397–409. doi:10.1038/nrn2647
- Watanabe, E., Kuchta, K., Kimura, M., Rauwald, H. W., Kamei, T., & Imanishi, J. (2015). Effects of bergamot (Citrus bergamia (Risso) Wright &Arn.) essential oil aromatherapy on mood states, parasympathetic nervous system activity, and salivary cortisol levels in 41 healthy females. Complementary Medicine Research, 22(1), 43–49. doi:10.1159/000380989
- Zänkert, S., Bellingrath, S., Wüst, S., & Kudielka, B. M. (2019). HPA axis responses to psychological challenge linking stress and disease: what do we know on sources of intra- and interindividual variability? Psychoneuroendocrinology, 105, 86–97. doi:10.1016/j.psyneuen.2018.10.027
- Zhang, K., & Yao, L. (2018). The anxiolytic effect of Juniperusvirginiana L. essential oil and determination of its active constituents. PhysiolBehav, 189, 50–58. doi:10.1016/j.physbeh.2018.01.004