
Abstract
Research has identified a variety of strategies people use to cope with stress and that the adaptiveness of various strategies depends on the context in which they are used. However, important questions remain about the role of physiological stress response systems in supporting, influencing, or changing from coping strategies. This study works toward addressing this gap by examining associations between skin conductance level (SCL) and habitual use of coping strategies. It was hypothesized that more use of problem-focused strategies would be associated with SCL trajectories that were more stable and decreased less steeply, with the opposite trend hypothesized for more use of emotion-focused strategies. Participants were 188 college students (78% female) who reported their use of 14 coping strategies. SCL was recorded during recall of a negative family memory from childhood for five minutes. Trajectories of SCL during the recall were estimated with multilevel modeling. Greater self-distraction, planning, active coping, use of emotional support, and coping flexibility were related to trajectories of SCL that decreased less steeply and were more stable. Problem-focused coping and coping flexibility are, therefore, related to reduced SCL reactivity and promoting these skills may benefit mental health.
Stress is well-known to contribute to poor health outcomes (Cohen et al., Citation2007; Esch et al., Citation2002). However, people can manage stress utilizing different coping strategies (Billings & Moos, Citation1981). These coping strategies can be categorized in ways such as problem-focused and emotion-focused (Lazarus & Folkman, Citation1984), and their adaptiveness depends on context (Cheng et al., Citation2014). Understanding the adaptiveness of coping strategies is critical for intervening in stress-related health problems but requires increased study of associations between coping strategies and physiological stress responses. Few studies have examined relations between coping and sympathetic nervous system (SNS) responding to stress, but these studies show relations and indicate a need for additional research (Tomaka et al., Citation1993; Suzuki et al., Citation2003). This study works toward addressing this need by evaluating associations between self-reported, habitual use of coping strategies (“coping tendencies”) and college students’ skin conductance levels (SCLs) during recall of negative family memories.
The SNS provides physiological resources supporting fight-or-flight responses to threatening situations (Boucsein, Citation1992). Because these responses cost energy and cause wear and tear (McEwen, Citation1998), the ideal SNS response to stress innervates only relevant target organs for the minimum necessary magnitude for the minimum necessary duration (Lacey, Citation1967). Polyvagal Theory (Porges, Citation2007, Citation2021) poses a similar idea; an adaptive stress response is one that maximizes the tradeoff between homeostatic efficacy and resource consumption. Such an adaptive stress response would take the form of more stable stress response trajectories, such as less steep increases or decreases. Thus, trajectories of target organ innervation during a condition should be the focus of research, rather than averaging activity levels across the condition, and more directly test the theoretical propositions of adaptive stress responses (Keller & El Sheikh, Citation2011). Importantly, the SNS has projections for nearly every organ system. These organ systems are not all innervated equally at a given moment and assessments of SNS activity via different target organs (heart, pupils, and sweat glands) are not interchangeable.
This study focuses on SNS innervation of the eccrine sweat glands. These glands are innervated solely by the SNS and are present in high quantities on the palm (Wilke et al., Citation2007). Their innervation can easily be quantified by how well the surface of the skin conducts electricity, a measure known as SCL. Many studies have averaged SCL during a baseline period or the course of a laboratory task for data analysis. Using this approach, greater SCL stress response is associated with child internalizing symptoms and lower SCL responding is related to child externalizing behaviors (El-Sheikh et al., Citation2007), aggression (Posthumus et al., Citation2009), and sleep difficulties (El‐Sheikh & Ariswalla, 2011). Moreover, previous research demonstrates that lower levels of anxiety, delinquency, and aggression, are associated with more stable response trajectories of SCL (i.e. less sharp increases or decreases and flatter trajectories; Keller & El Sheikh, Citation2011). Thus, individual differences in SCL responding, both between-task and within-task, are related to risk for mental health problems, making the sweat glands a valuable target organ for study. An important next step for research is to determine how SCL may be related to psychological coping, as such relations may help explain why SCL appears to play a role in mental health.
Coping can be best understood as one’s ability to respond adaptively to stress (Lazarus & Folkman, Citation1984). Two main categories of coping strategies are problem-focused and emotion-focused. Problem-focused coping attempts to directly resolve the stressful situation, whereas emotion-focused coping attempts to combat the negative emotions resulting from the situation. The style of coping being used is not necessarily the same across places, contexts, or stressors (Lazarus, Citation1966; Pearlin & Schooler, Citation1978). However, a measurement of how frequently a person uses a coping strategy across contexts allows researchers to examine a person’s coping tendencies. Generally, the use of coping during the transition from childhood to adolescence is mostly stable (Eschenbeck et al., Citation2018; Richardson et al., Citation2021), a trend that is comparable for adulthood (Wang & Hall, Citation2021). Beyond individual coping strategies, coping flexibility is the degree to which individuals can change their coping strategies to fit different situations (Cheng et al., Citation2014), or end an ineffective strategy and use an alternate strategy (Kato, Citation2012). A meta-analysis of 90 studies supports the benefits of coping flexibility for psychological well-being (Cheng et al., Citation2014). These benefits hold when coping flexibility is measured using either a means-based approach (i.e. the average of the frequency of each strategy use) or a count-based approach (i.e. counting the number of strategies a person uses; Heffer & Willoughby, Citation2017).
It is an open scientific question whether coping tendencies or coping flexibility are associated with SCL. However, there is some research on this topic utilizing other psychophysiological indices of stress. In response to a difficult puzzle task, participants with higher coping flexibility had significantly lower blood pressure responses (determined by SNS; Kato, Citation2017). Participants with higher coping effectiveness secreted less salivary alpha amylase, a salivary biomarker of stress indexing the autonomic nervous system generally, during a stressful speaking paradigm (Ajibewa et al., Citation2021). Similar results have been found with salivary cortisol, a marker of hypothalamic–pituitary–adrenal axis activity: Zapater-Fajarí et al. (Citation2021) demonstrated that active, but not passive coping, contributed to individual differences in cortisol responses during a stressful public speaking paradigm. There has also been some research on coping behavior during a stressor and simultaneous SCL. Participants in a passive observation condition displayed decreasing SCL, whereas those in an active problem-solving condition displayed increasing SCL (Sosnowski et al., Citation1991). During a stressful arithmetic task, avoidant coping in response to a potential punishment for poor performance was associated with an increase in SCL (Suzuki et al., Citation2003). Interestingly, these results may not generalize to other physiological systems, as Schäfer et al. (2020) found no differences in heart rate variability between coping and control groups during a stressful task.
Associations between coping and SCL are likely because the prefrontal cortex (PFC) and the amygdala regulate both psychological coping and SCL. For example, increased activity of the ventromedial PFC and decreased amygdala activity is associated with higher engagement in active and avoidant coping tendencies, and lower SCL (Laine et al., Citation2009; Rauch et al., Citation2007; Sinha et al., Citation2016; Wood et al., Citation2014; Zhang et al., Citation2014). Conversely, decreased activity in the PFC and increased activity in the amygdala are associated with higher engagement in emotion-focused and vigilant coping tendencies and higher SCL.
This study
This study models trajectories of SCL during a negative autobiographical recall interview (i.e. a recollection of a childhood negative family memory). Modeling trajectories is a fairly novel approach to quantifying and analyzing SCL trajectories, rather than comparing single estimates of task means versus baseline. In addition to the previous strengths of modeling trajectories mentioned earlier, such that estimating trajectories is more in line with how the SNS operates and theoretical propositions of adaptive stress responses, it also addresses practical concerns with using task means. Notably, trajectories may be substantively different even when the mean SCL during the task is the same. For example, the single estimate mean difference for two groups could be zero if one group had a trajectory with slope x = 1 and the other group had a trajectory with slope x= −1). In a similar manner, the negative autobiographical task departs from the typical stressful task paradigm, though it has been established to be as effective at eliciting stress as other tasks (e.g. viewing violent or shocking film clips; Martin, Citation1990). Modern research continues to use this task to elicit stress (e.g., Barry et al., Citation2021).
Beyond simply modeling trajectories of SCL during the negative interview, this study examines whether coping tendencies and coping flexibility are associated with these trajectories. Establishing these associations would help draw out the implications of central nervous system coordination of stress response for human behavior and health. Specifically, this study has three main aims: (1) Determine the mean shape of the SCL trajectory and whether there are individual differences in trajectories during negative memory recall. It is hypothesized that average trajectories will initially increase, reach a peak, and then decrease. This would correspond to an automatic initial stress response followed by the conscious downregulation of this response (Nagai et al., Citation2004; Patterson et al., Citation2002). (2) Examine associations between emotion-focused and problem-focused coping tendencies and trajectories of SCL during memory recall. It is hypothesized that greater use of emotion-focused (more passive in nature) coping tendencies, in comparison to less use, will be related to higher and more fluctuating SCL trajectories. Conversely, those with greater use of problem-focused (more active in nature) coping tendencies, rather than lower use, will have lower and less changing SCL trajectories. This would correspond to brain imaging research of coping and SCL (e.g. Laine et al., Citation2009; Rauch et al., Citation2007). Coping tendencies that do not fit into either category are not examined. (3) Determine possible associations between coping flexibility and SCL trajectories. Because higher coping flexibility is related to better psychological adjustment (Cheng et al., 2014), it is hypothesized that higher coping flexibility will be related to lower and less increasing SCL trajectories.
Materials and method
Participants
Participants are 188 college students (Mage =19.01, SD = 1.24) drawn from a larger study (N= 377) who participated for course credit. For the larger study, participants needed to be at least 18 years old and fluent in English. For this study, participants also needed to have valid SCL data (n= 189 of the larger study did not participate in SCL data collection or did not have valid data due to recording errors). Due to the larger study goals, some participants were individually invited to participate if they indicated their parent was an alcoholic on a screening measure (33% of the 188 students). Other participants viewed the description of the study in the online research participation system and self-selected into the study (67%). Also, for the sample of 188 students, participants were 86.8% white, 78.4% female, and 70.4% of participants identified themselves as coming from a middle-class or upper-middle-class household, with 22.6% identifying themselves as coming from a low-income household, and 7.0% coming from a high-income household. The only difference between the sample from the larger study and the sample included in the present analyses was that there was a greater percentage of participants who self-selected rather than received an invitation in the analysis sample, χ2(1)=23.1, p<.001. See the “Covariates” section below for more information. The final sample size utilized was considerably larger than recommended for our analysis method (N= 50; Maas & Hox, Citation2005), and is either equivalent to (Keller & El Sheikh, Citation2011) or larger than similar research cited (Schäfer et al., Citation2020).
Procedure
All procedures were approved by the university’s internal review board (approval number 13-0616-F4S). Written informed consent was obtained prior to participation in any part of the study. The participants attended a single laboratory visit. They completed questionnaires described below. Baseline assessment of SCL was recorded for three minutes while participants sat quietly. Next, participants were asked to recall one of their worst family memories from childhood, describe the details of the event, their feelings, and the impact of the event on their current lives for 5 min. Participants were asked not to discuss child abuse due to a review board restriction. Experimenters were instructed to end the interview if participants requested or if participants exhibited significant distress, however, this did not occur for any participant. This task is highly effective at inducing negative mood and is appraised as stressful (Martin, Citation1990). Moreover, this stressor, in comparison to a problem-based stressor (e.g. mirror-tracing), may better demonstrate associations between a person’s use of coping tendencies and trajectories of SCL during a personally relevant stressor in a way that is more ecologically valid than a simple laboratory task. Study materials may be obtained through correspondence with the first author.
Measures
Coping tendencies
The Brief Cope (BCOPE; Carver, Citation1997) consists of 28 questions, so that two questions each measure the use of 14 different coping tendencies, using a four-point Likert style scale ranging from one (“I haven’t been doing this at all”) to four (“I’ve been doing this a lot”). A total score for each tendency is obtained by summing the scores for each pair of questions. The emotion-focused strategies were: emotional support, positive reframing, acceptance, denial, and religion. Each strategy’s Cronbach’s α was: 0.88, 0.86, 0.78, 0.86, and 0.92, respectively. The problem-focused strategies were: active coping, planning, instrumental support, and self-distraction. Each problem-focused strategy’s Cronbach’s α was: 0.83, 0.92, 0.94, and 0.75, respectively. The “other” group included: venting, substance use, behavioral disengagement, self-blame, and humor. These are used only for the computation of a coping flexibility measure, as described below. Their corresponding internal reliabilities were: 0.52, 0.93, 0.77, 0.87, and 0.93. The venting subscale was the only measure with α < 0.70. However, this measure was not used as an individual variable associated with SCL trajectories as it is in the “other” group.
Coping flexibility
Following the approach of Heffer and Willoughby (Citation2017), a count-based approach to quantifying coping flexibility was used. This method may be preferred in comparison to a means-based approach as a means-based approach may obfuscate distinct coping patterns due to identical means (Heffer & Willoughby, Citation2017). For the count-based approach, scores on the BCOPE subscales were recoded as 0 (usually not using a given strategy at all) or 1 (any other score than not using a given strategy at all). Coping flexibility was then computed by summing across all 14 recoded tendencies, for a possible range from zero to 14, with higher scores indicating greater coping flexibility.
SCL collection and measurement
Two Ag-AgCl electrodes were placed on the non-dominant palm one inch apart. A continuous sinusoidal voltage was used in order to avoid bias from the electrodes. An eight-slot BioNex mainframe received and amplified signals via a three-channel bio-potential and galvanic skin conductance amplifier module (MindWare Technologies Ltd., Westerville, OH). Participants’ SCL (expressed in micro-Siemens) was measured throughout the entirety of the baseline and the negative memory recollection. Software from Mindware Technologies Ltd. (BioLab version 3.2.2) was used to record the data. Following data collection, software from the same company (Electrodermal Activity Analysis; EDA version 3.0.25) was used to compute and export the SCL data from participants for each task. During this process, data were assessed for completeness and validity. Data were deemed unusable if there were problems with the source signal (e.g. due to damaged electrodes; this results in a pattern of non-linear skin conductance during the epoch with extremely low values). Data were also assessed for artifacts that may influence SCL level (e.g. coughing or sneezing during the task). Artifacts were removed for 13 participants. Following this preliminary check, averages were pulled from the program for 30-s epochs during the 5-min negative interview task (total of 10 epochs). The average level of SCL for the baseline period was also computed for use as a covariate in analyses.
Covariates
Previous research has highlighted differences in the use of coping strategies depending on racial/ethnic identity (Bjorck et al., Citation2001) and participant SES (Botchkovar et al., Citation2013). Therefore, participant self-reported race (non-white = 0, white = 1) and self-reported subjective SES (0 = very poor, 1 = poor, 2 = middle class, 3 = upper middle class, and 4 = wealthy) are analyzed as covariates. Previous research also indicates the importance of subjective emotional intensity during a physiological assessment of stress (Hellhammer & Schubert, Citation2012). During the interview, participants were asked an open-ended question about which emotion they were presently feeling and were to rate it on a scale from one to 10. This score is analyzed as a covariate. Finally, participant age in years, sex (female = 1, male = 0), and whether participants can be classified as a child of an alcoholic (COA; COA = 1, non-COA = 0) are also analyzed as covariates. The COA status variable was included because this was a focus of the larger study and the criterion used to extend invitations to some students to participate.
Data analysis plan
Analyses were multilevel models (MLMs) of SCL during the memory recall using SAS version 9.4 (SAS Institute Inc., 2015, Cary, NC). All statistical tests for this study used a p value of .05 to indicate statistical significance. Prior to MLM, preliminary analyses proceeded in four steps. First, the covariates were assessed for potential inclusion in models. Second, cases exhibiting a significant Mahalanobis distance were examined closely as possible outliers (De Maesschalck et al., Citation2000). Third, the amount of missing data for each variable was computed to determine whether multiple imputations were needed. Finally, multivariate normality was assessed by examining the normality of SCL, coping tendencies, and coping flexibility. See the Preliminary Analyses section below for results of these procedures.
Level one of the MLMs (within-person model) modeled SCL as a function of time. Level two (between-person level) included coping tendencies and covariates as “predictors” of these effects of time. Note that the word “predictors” reflects the model parameterization but that the study design does not permit causal inferences. Initial unconditional models (no “predictors” of trajectories) were fit to determine the appropriate model of the trajectories (flat line, straight line with slope, quadratic curve) using a hierarchical approach and compared improvement in model fit with a chi-square test. Next, covariates were added. To preserve model parsimony, covariates were only retained for final models if they were significantly associated with trajectories.
Final models added the mean-centered, continuous score for a single coping variable as a predictor. As there are 10 coping variables, this resulted in 10 models fit. Significant associations between coping variables and growth terms were coping x time interactions. For significant interactions, trajectories of SCL were plotted for +1 and −1 SD from the mean value of the coping variable.
Results
Preliminary analyses
Bivariate correlations between study variables and covariates indicated that there were no associations between study variables and participant age, emotion during the interview, or COA status. These covariates are not considered further. Race, sex, subjective SES, and baseline SCL were correlated with study variables and are considered in MLMs. These results are not detailed in the text. Next, the amount of missing data was low enough to forego multiple imputation: coping tendencies (n= 7, 3.7%), baseline SCL (n= 22, 11.7%), race (n= 6, 3.2%), sex (n= 3, 1.6%), and SES (n= 2, 1.1%), and no SCL data were missing for the interview. Instead, the expectation-maximization algorithm (Moon, Citation1996) was used to impute missing continuous data. The Mahalanobis distance flagged 21 cases as potential multivariate outliers. They were excluded from analyses, as these cases tended to be nontraditional students or those who struggled with substance abuse (final N= 167). Finally, the SCL variables were consistently and severely skewed. Therefore, the recommended approach of maximum likelihood with robust standard errors was used (Huber, Citation1967; see also Harden, Citation2009; Maas & Hox, Citation2005).
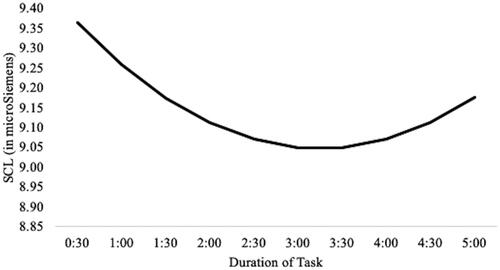
Descriptive statistics and intercorrelations between study variables, after imputation and outlier removal, are shown in . The very high correlations between the measures of SCL are consistent with autoregressive measures taken 30 s apart. On average, SCL means over the course of the interview tended to start high, decreased until reaching a low point about halfway through the interview, and began increasing for the remainder of the interview. All SCL means during the interview (the lowest mean was for epochs five and six, M= 9.03) were over 55% greater than the baseline SCL mean (M= 5.82). A paired-sample t-test revealed that this mean difference was significant, t(166) = 17.225, p<.001. Thus, the interview was significantly more stressful to participants, as indexed by significant increases in SCL across all epochs.
Table 1. Means, standard deviations, and correlations among variables.
Trajectories of SCL
See . The first model in the taxonomy was the unconditional means model, in which trajectories were flat lines (described only by an intercept). This model serves as a baseline model and establishes that the majority of SCL variance was at the between-person level, ICC = 0.96. Next, time was added to the level one model so that trajectories could take the form of straight lines with non-zero slopes. This significantly improved the model, χ2(4)=285.30, p<.001. The third model added the square of time, denoted as time2 for the remainder of the manuscript, so that trajectories could take the form of quadratic curves, and this was an additional improvement in model fit, χ2(4)=32.10, p<.001. Adding the cube of time, denoted as time3, to the model, so that trajectories could take the form of more complex cubic curves, did not significantly improve the model, χ2(2)= 1.20, p=.878.
Table 2. Results from unconditional multilevel models of SCL.
Therefore, the quadratic growth model (model UCG2 in ) is the preferred model. On average, SCL initial status was 9.36 mS, declined by 0.12 mS per epoch, p=.003, and increased toward the end of the task, fixed effect of time2 (i.e. time squared) = 0.01, p=.006. In this manner, the average trajectory resembled a “u” shaped pattern and is shown in . There was also significant variability across participants in the initial starting point, effect of time, and effect of time2, suggesting that this pattern does not adequately represent all participants, and that additional factors may explain these differences in the average trajectory.
Figure 1. Mean trajectory of SCL during the interview.
Covariates associated with trajectories of SCL
Baseline SCL was associated with SCL initial status, B= 1.09, p<.001, but was not related to the effects of time or time2. This model significantly improved the fit of the unconditional model with time2, χ2(1)=148.20, p<.001, and baseline SCL is retained in all additional models. No other examined covariates were related to SCL trajectories or improved model fit. These results are not depicted in a table. Given the results, participants with higher baseline SCL started with higher SCL at the beginning of the interview.
Emotion-Focused coping tendencies and trajectories of SCL
See for results of all five emotion-focused coping models. Adding emotional support and acceptance significantly improved model fit, χ2(3)=17.00, p<.001 for emotional support and χ2(3)=11.60, p=.009 for acceptance. However, there were no significant associations between acceptance and SCL trajectories. This model is not discussed further. There was a significant association between emotional support and the effect of time, B= 0.05, p=.022. In , trajectories of SCL are plotted for persons +1 SD (higher) and −1 SD (lower) from the mean of emotional support. At higher emotional support, SCL trajectories were stable and flat across the interview. At lower emotional support, SCL trajectories decreased across the interview.
Figure 2. Trajectories of SCL for participants higher (+1SD) and lower (–1SD) in coping variables.
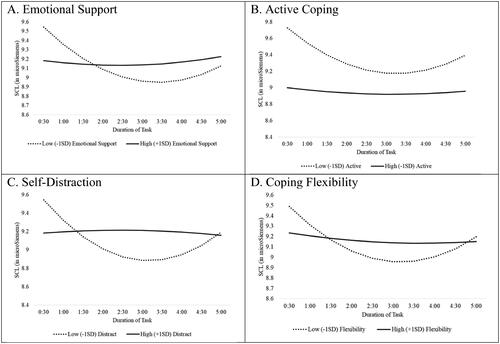
Table 3. Emotion-focused coping tendencies and trajectories of SCL.
Problem-focused coping tendencies and trajectories of SCL
See for all four problem-focused coping models. All four problem-focused coping variables significantly improved model fit compared to the model with only baseline SCL as a covariate, but significant associations with SCL trajectories were observed for three (active, planning, and self-distraction) and are described here. Models for active coping and planning are nearly identical. The model with active coping improved model fit, χ2(3)=18.00, p<.001, as did the model with planning, χ2(3)=16.40, p<.001. Both coping variables were positively related to the effect of time, B = 0.05 and 0.04, respectively, ps<.05, and negatively related to the effect of time2, B= −0.005 and − 0.004, respectively, ps<.05. Because the associations are so similar, they are plotted only for active coping. In , SCL trajectories are plotted for persons +1 SD (higher) and −1 SD (lower) from the mean on active coping. At higher active coping, SCL is overall lower and generally unchanging during the interview. At lower active coping, SCL is higher overall and exhibits more rapid declines that reach a low point around 3:00, transitioning into increases in SCL starting at 3:30.
Table 4. Problem-focused coping tendency, coping flexibility, and SCL trajectories.
The model with self-distraction improved model fit, χ2(3)=40.00, p<.001, and had similar but somewhat greater B coefficients than for active coping and planning. Self-distraction was positively related to the effect of time, B = 0.08, p<.001, and negatively related to the effect of time2, B= −0.007, p<.05. At higher self-distraction, SCL follows a generally flat trajectory, although there are very slight increases for the first half followed by very slight decreases during the second half of the interview. At lower self-distraction, SCL more rapidly declined and reached a low point around 3:00, then transitioned into increasing SCL. These patterns are depicted in .
Coping flexibility and trajectories of SCL
See for results of the coping flexibility model. The coping flexibility model significantly improved model fit, χ2(3) =16.10, p=.001. Coping flexibility was significantly related to the effects of time, B= 0.03, p=.036, and time2, B= −0.003, p=.024. At higher coping flexibility, SCL trajectories are more stable and only exhibit very slight declines that transition to very slight increases. At lower coping flexibility, SCL more rapidly declines and reaches a low point around 3:00, then begins to increase. These patterns are depicted in .
Given that the majority of coping tendencies related to SCL were problem-focused, a post-hoc analysis was conducted with all problem-focused tendencies excluded from the coping flexibility measure. This analysis determined whether associations between coping flexibility and SCL trajectories were a reflection of using more problem-focused strategies rather than coping strategies more generally. Results from the post hoc analysis yielded similar results to the original model. It was also an improvement in model fit, χ2(3)=17.0, p<.001. Furthermore, associations with the effects of time and time2 were almost identical, B= 0.04, p=.028, and −0.004, p=.020, respectively.
Discussion
This study modeled trajectories of SCL during recall of a negative family event among college students and examined associations between these trajectories and psychological coping tendencies and flexibility. The mean trajectory of SCL was a u-shaped curve that decreased for the first 3 min and then increased for the final 2 min (see ). For emotion-focused coping tendencies, the only use of emotional support was significantly related to (flatter) SCL trajectories. For problem-focused coping tendencies, active coping, planning, and self-distraction were each associated with flatter SCL trajectories. Coping flexibility was also associated with flatter trajectories of SCL, even when confined to emotion-focused and other types of coping strategies. depicts each of these findings. These findings are novel for the examination of general coping tendencies in relation to SNS innervation of a specific target organ during a particular situation.
The hypothesis that the average SCL trajectory would follow an upside-down u-shaped curve was not supported. The average trajectory of SCL showed the opposite pattern, indicating that the SNS did not, on average, innervate the eccrine sweat glands in preparation for fight-or-flight responding. Mean decreases in SCL are observed during some tasks, such as a mirror-tracing task (El-Sheikh et al., Citation2010); the increases in SCL following the 3-min mark observed in this study may indicate recovery. Rather than fight-or-flight responses, decreases in SCL may represent engagement responses (Porges, Citation2007). Lower SNS innervation of various target organs promotes calm and allows physiological resources to be devoted to attending to social cues, adjusting behavior to meet social expectations, and negotiating complex relationships with others. The decreases in SCL at the beginning of the interview may therefore permit recall and sharing of a negative autobiographical memory with the experimenter. Measurement of autonomic innervation of other target organs is needed to further investigate this possibility.
Associations between coping tendencies and SCL trajectories were somewhat inconsistent with expectations. The single observed association for emotion-focused coping did not follow the expected pattern of sharper declines in SCL with greater use of emotional support. However, the problem-focused coping tendencies of active coping, planning, and self-distraction were related to SCL trajectories that decreased less steeply during the task. For active coping and planning, SCL trajectories were also lower overall. These findings are consistent with hypotheses, which were derived from research on the shared neurobiology (PFC and amygdala) of the SNS and coping (Sinha et al., Citation2016; Zhang et al., Citation2014). However, the consistent pattern of findings suggests a further explanation. In all cases, persons reporting greater use of coping strategies have a more stable trajectory, whereas those low in coping follow a u-shaped trajectory.
As u-shaped SCL trajectories may indicate an engagement response; those higher in coping tendencies may require less engagement. SNS responding can become habituated (Zimmer, Citation2006). The engagement response is strongest upon the presentation of a novel stimulus and weakens following repeated exposures. Coping may serve to habituate persons to the recall and sharing of negative autobiographical events. For example, persons who engage in greater coping may have discussed the event multiple times with others (e.g. emotional support coping) or have repeatedly distracted themselves from the event (self-distraction coping), reducing the novelty of recalling the event. Unfortunately, we are not aware of any research on SCL trajectories following repeated exposures to stressors rather than perceptual stimuli. Experimental research manipulating novelty and habituation to a stressor would be extremely valuable for understanding whether the orienting response is occurring and is related to coping abilities.
Higher coping flexibility was also related to SCL trajectories that decreased less sharply during the task, although the overall levels were not less than those with lower coping flexibility. This is the first study, to our knowledge, to examine coping flexibility and SCL, despite some research showing relations between coping flexibility and other physiological responses (Kato, Citation2017). Current results also align with previous research showing that coping flexibility is related to adaptive functioning, as less pronounced autonomic reactivity would be more adaptive (Cheng et al., Citation2014; Heffer & Willoughby, Citation2017). Similar to specific coping tendencies, coping flexibility may habituate people to the recall of negative memories, requiring less physiological resources to engage with the experimenter. Interestingly, coping flexibility was associated with SCL trajectories even after removing most of the individual coping strategies that were associated with SCL trajectories from the measure. These findings suggest that coping flexibility is an important factor in SCL reactivity above and beyond engagement in individual strategies.
Study findings have implications for mental health. Differences in SCL reactivity are associated with internalizing and externalizing behaviors (El-Sheikh et al., Citation2007) and aggression (Posthumus et al., Citation2009). Furthermore, stable SCL trajectories during the recall of negative memories may have implications for posttraumatic stress disorder (PTSD). Increased SCL in the recent aftermath of a traumatic event increases the likelihood of PTSD diagnosis over the long term (Hinrichs et al., Citation2019), and PTSD is related to greater SCL reactivity during a trauma interview (Hinrichs et al., Citation2017). Therefore, higher coping flexibility or more use of problem-focused coping strategies may protect against PTSD.
Limitations and future directions
First, it should be noted that the sample was mostly female, white, and rated their family SES as middle or upper-middle-class. Findings should not be generalized to other populations. Given differences in coping tendencies across race (Bjorck et al., Citation2001), future research should explore associations between coping and SCL trajectories in more diverse populations. Second, this study was cross-sectional. Results equally support the influence of coping on SCL trajectories and the influence of SCL trajectories on coping. This study is only a first step; additional research must determine whether coping strategies are related to changes in SCL trajectories over time. Third, this study did not examine coping strategies used during the interview, or perceived efficacy of coping. Such examination would shed additional light on whether past coping may have obviated the need for additional coping during the interview.
Despite these limitations, this study provides valuable insight into changes in SCL during the recall of negative memories among healthy young adults, and how these changes are related to coping tendencies and coping flexibility. Rather than fight-or-flight responding, SCL patterns were consistent with psychological engagement. Finally, individual differences in these changes exist such that less SCL change occurs among persons higher in problem-focused coping tendencies and coping flexibility.
Disclosure statement
The authors report no conflict of interest.
Data availability statement
Study Materials, Such As The Consent Document Or The Autobiographical Task Instructions, And/Or Study Data, May Be Obtained Through Correspondence With The First Author.
References
- Ajibewa, T. A., Adams, T. A., Gill, A. K., Mazin, L. E., Gerras, J. E., & Hasson, R. E. (2021). Stress coping strategies and stress reactivity in adolescents with overweight/obesity. Stress and Health: Journal of the International Society for the Investigation of Stress, 37(2), 243–254. https://doi.org/10.1002/smi.2987
- Barry, T. J., Sewart, A. R., Adam, E. K., Zinbarg, R. E., Mineka, S., & Craske, M. G. (2021). The longitudinal association between individual differences in recall of positive specific autobiographical memories and daily cortisol. Biological Psychology, 162, 108086. https://doi.org/10.1016/j.biopsycho.2021.108086
- Billings, A. G., & Moos, R. H. (1981). The role of coping responses and social resources in attenuating the stress of life events. Journal of Behavioral Medicine, 4(2), 139–157. https://doi.org/10.1007/BF00844267
- Bjorck, J. P., Cuthbertson, W., Thurman, J. W., & Lee, Y. S. (2001). Ethnicity, coping, and distress among Korean Americans, Filipino Americans, and Caucasian Americans. The Journal of Social Psychology, 141(4), 421–442. https://doi.org/10.1080/00224540109600563
- Botchkovar, E. V., Tittle, C. R., & Antonaccio, O. (2013). Strain, coping, and socioeconomic status: Coping histories and present choices. Journal of Quantitative Criminology, 29(2), 217–250. https://doi.org/10.1007/s10940-012-9177-7
- Boucsein, W. (1992). Electrodermal indices of emotion and stress, chapter 3. Electrodermal activity (pp. 369–391). Springer US.
- Carver, C. S. (1997). You want to measure coping but your protocol’s too long: Consider the brief COPE. International Journal of Behavioral Medicine, 4(1), 92–100. https://doi.org/10.1207/s15327558ijbm0401_6
- Cheng, C., Lau, H. P. B., & Chan, M. P. S. (2014). Coping flexibility and psychological adjustment to stressful life changes: A meta-analytic review. Psychological Bulletin, 140(6), 1582–1607. https://doi.org/10.1037/a0037913
- Cohen, S., Janicki-Deverts, D., & Miller, G. E. (2007). Psychological stress and disease. JAMA, 298(14), 1685–1687. https://doi.org/10.1001/jama.298.14.1685
- De Maesschalck, R., Jouan-Rimbaud, D., & Massart, D. L. (2000). The mahalanobis distance. Chemometrics and Intelligent Laboratory Systems, 50(1), 1–18. https://doi.org/10.1016/S0169-7439(99)00047-7
- Esch, T., Stefano, G. B., Fricchione, G. L., & Benson, H. (2002). Stress in cardiovascular diseases. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research, 8(5), RA93–RA101.
- Eschenbeck, H., Schmid, S., Schröder, I., Wasserfall, N., & Kohlmann, C. W. (2018). Development of coping strategies from childhood to adolescence: Cross-sectional and longitudinal trends. European Journal of Health Psychology, 25(1), 18–30. https://doi.org/10.1027/2512-8442/a000005
- El-Sheikh, M., Keiley, M., & Hinnant, J. B. (2010). Developmental trajectories of skin conductance level in middle childhood: Sex, race, and externalizing behavior problems as predictors of growth. Biological Psychology, 83(2), 116–124. https://doi.org/10.1016/j.biopsycho.2009.11.009
- El-Sheikh, M., Keller, P. S., & Erath, S. A. (2007). Marital conflict and risk for child maladjustment over time: Skin conductance level reactivity as a vulnerability factor. Journal of Abnormal Child Psychology, 35(5), 715–727. https://doi.org/10.1007/s10802-007-9127-2
- El‐Sheikh, M., & Ariswalla, D. D. (2011). Children’s sleep, skin conductance level and mental health. Journal of Sleep Research, 20(2), 326–337. https://doi.org/10.1111/j.1365-2869.2010.00880.x
- Harden, J. J. (2009). A comparison of methods for estimating linear and generalized linear models with multilevel data [Paper presentation] 26th Annual Meeting of the Society for Political Methodology, New Haven, CT.
- Heffer, T., & Willoughby, T. (2017). A count of coping strategies: A longitudinal study investigating an alternative method to understanding coping and adjustment. PLoS One, 12(10), e0186057. https://doi.org/10.1371/journal.pone.0186057
- Hellhammer, J., & Schubert, M. (2012). The physiological response to Trier Social Stress Test relates to subjective measures of stress during but not before or after the test. Psychoneuroendocrinology, 37(1), 119–124. https://doi.org/10.1016/j.psyneuen.2011.05.012
- Hinrichs, R., Michopoulos, V., Winters, S., Rothbaum, A. O., Rothbaum, B. O., Ressler, K. J., & Jovanovic, T. (2017). Mobile assessment of heightened skin conductance in posttraumatic stress disorder. Depression and Anxiety, 34(6), 502–507. https://doi.org/10.1002/da.22610
- Hinrichs, R., van Rooij, S. J. H., Michopoulos, V., Schultebraucks, K., Winters, S., Maples-Keller, J., Rothbaum, A. O., Stevens, J. S., Galatzer-Levy, I., Rothbaum, B. O., Ressler, K. J., & Jovanovic, T. (2019). Increased skin conductance response in the immediate aftermath of trauma predicts PTSD risk. Chronic Stress, 3, 247054701984444. https://doi.org/10.1177/2470547019844441
- Huber, P. J. (1967). The behavior of maximum likelihood estimates under nonstandard conditions. Proceedings of the Fifth Berkeley Symposium on Mathematical Statistics and Probability (Vol. 1, pp. 221–233). University of California Press.
- Kato, T. (2012). Development of the coping flexibility scale: Evidence for the coping flexibility hypothesis. Journal of Counseling Psychology, 59(2), 262–273. https://doi.org/10.1037/a0027770
- Kato, T. (2017). Effects of coping flexibility on cardiovascular reactivity to task difficulty. Journal of Psychosomatic Research, 95, 1–6. https://doi.org/10.1016/j.jpsychores.2017.02.001
- Keller, P. S., & El Sheikh, M. (2011). Latent change score modeling of psychophysiological data: An empirical instantiation using electrodermal responding. Psychophysiology, 48(11), 1578–1587. https://doi.org/10.1111/j.1469-8986.2011.01225.x
- Lacey, J. I. (1967). Somatic response patterning and stress: Some revisions of activation theory. Psychological stress: Issues in research (pp. 14–37). Appleton-Century-Crofts.
- Laine, C. M., Spitler, K. M., Mosher, C. P., & Gothard, K. M. (2009). Behavioral triggers of skin conductance responses and their neural correlates in the primate amygdala. Journal of Neurophysiology, 101(4), 1749–1754. https://doi.org/10.1152/jn.91110.2008
- Lazarus, R. S. (1966). Psychological stress and the coping process. McGraw-Hill.
- Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. Springer Publishing Company.
- Maas, C. J., & Hox, J. J. (2005). Sufficient sample sizes for multilevel modeling. Methodology, 1(3), 86–92. https://doi.org/10.1027/1614-2241.1.3.86
- Martin, M. (1990). On the induction of mood. Clinical Psychology Review, 10(6), 669–697. https://doi.org/10.1016/0272-7358(90)90075-L
- McEwen, B. S. (1998). Stress, adaptation, and disease. Allostasis and allostatic load. Annals of the New York Academy of Sciences, 840(1), 33–44. https://doi.org/10.1111/j.1749-6632.1998.tb09546.x
- Moon, T. K. (1996). The expectation-maximization algorithm. IEEE Signal Processing Magazine, 13(6), 47–60. https://doi.org/10.1109/79.543975
- Nagai, Y., Critchley, H. D., Featherstone, E., Trimble, M. R., & Dolan, R. J. (2004). Activity in ventromedial prefrontal cortex covaries with sympathetic skin conductance level: A physiological account of a “default mode” of brain function. NeuroImage, 22(1), 243–251. https://doi.org/10.1016/j.neuroimage.2004.01.019
- Patterson, I. I., J. C., Ungerleider, L. G., & Bandettini, P. A. (2002). Task-independent functional brain activity correlation with skin conductance changes: An fMRI study. NeuroImage, 17(4), 1797–1806. https://doi.org/10.1006/nimg.2002.1306
- Pearlin, L. I., & Schooler, C. (1978). The structure of coping. Journal of Health and Social Behavior, 19(1), 2–21. https://doi.org/10.2307/2136319
- Porges, S. W. (2007). The polyvagal perspective. Biological Psychology, 74(2), 116–143. https://doi.org/10.1016/j.biopsycho.2006.06.009
- Porges, S. W. (2021). Polyvagal theory: A biobehavioral journey to sociality. Comprehensive Psychoneuroendocrinology, 7, 100069. https://doi.org/10.1016/j.cpnec.2021.100069
- Posthumus, J. A., Böcker, K. B. E., Raaijmakers, M. A. J., Van Engeland, H., & Matthys, W. (2009). Heart rate and skin conductance in four-year-old children with aggressive behavior. Biological Psychology, 82(2), 164–168. https://doi.org/10.1016/j.biopsycho.2009.07.003
- Rauch, A. V., Ohrmann, P., Bauer, J., Kugel, H., Engelien, A., Arolt, V., Heindel, W., & Suslow, T. (2007). Cognitive coping style modulates neural responses to emotional faces in healthy humans: A 3-T FMRI study. Cerebral Cortex, 17(11), 2526–2535. https://doi.org/10.1093/cercor/bhl158
- Richardson, C. E., Magson, N. R., Fardouly, J., Oar, E. L., Forbes, M. K., Johnco, C. J., & Rapee, R. M. (2021). Longitudinal associations between coping strategies and psychopathology in pre-adolescence. Journal of Youth and Adolescence, 50(6), 1189–1204. https://doi.org/10.1007/s10964-020-01330-x
- Schäfer, A., Pels, F., & Kleinert, J. (2020). Effects of different coping strategies on the psychological and physiological stress reaction: An experimental study. European Journal of Health Psychology, 27(3), 109–123. https://doi.org/10.1027/2512-8442/a000056
- Sinha, R., Lacadie, C. M., Constable, R. T., & Seo, D. (2016). Dynamic neural activity during stress signals resilient coping. Proceedings of the National Academy of Sciences, 113(31), 8837–8842. https://doi.org/10.1073/pnas.1600965113
- Sosnowski, T., Nurzynska, M., & Polec, M. (1991). Active-passive coping and skin conductance and heart rate changes . Psychophysiology, 28(6), 665–672. https://doi.org/10.1111/j.1469-8986.1991.tb01011.x
- Suzuki, S. I., Kumano, H., & Sakano, Y. (2003). Effects of effort and distress coping processes on psychophysiological and psychological stress responses. International Journal of Psychophysiology: Official Journal of the International Organization of Psychophysiology, 47(2), 117–128. https://doi.org/10.1016/s0167-8760(02)00120-4
- Tomaka, J., Blascovich, J., Kelsey, R. M., & Leitten, C. L. (1993). Subjective, physiological, and behavioral effects of threat and challenge appraisal. Journal of Personality and Social Psychology, 65(2), 248–260. https://doi.org/10.1037/0022-3514.65.2.248
- Wang, H., & Hall, N. C. (2021). Exploring relations between teacher emotions, coping strategies, and intentions to quit: A longitudinal analysis. Journal of School Psychology, 86, 64–77. https://doi.org/10.1016/j.jsp.2021.03.005
- Wilke, K., Martin, A., Terstegen, L., & Biel, S. S. (2007). A short history of sweat gland biology. International Journal of Cosmetic Science, 29(3), 169–179. https://doi.org/10.1111/j.1467-2494.2007.00387.x
- Wood, K. H., Ver Hoef, L. W., & Knight, D. C. (2014). The amygdala mediates the emotional modulation of threat-elicited skin conductance response. Emotion, 14(4), 693–700. https://doi.org/10.1037/a0036636
- Zapater-Fajarí, M., Crespo-Sanmiguel, I., Pulopulos, M. M., Hidalgo, V., & Salvador, A. (2021). Resilience and psychobiological response to stress in older people: The mediating role of coping strategies. Frontiers in Aging Neuroscience, 13, 632141. https://doi.org/10.3389/fnagi.2021.632141
- Zimmer, H. (2006). Habituation of the orienting response as reflected by the skin conductance response and by endogenous event-related brain potentials. International Journal of Psychophysiology, 60(1), 44–58. https://doi.org/10.1016/j.ijpsycho.2005.05.003
- Zhang, S., Hu, S., Chao, H. H., Ide, J. S., Luo, X., Farr, O. M., & Li, C. S. R. (2014). Ventromedial prefrontal cortex and the regulation of physiological arousal. Social Cognitive and Affective Neuroscience, 9(7), 900–908. https://doi.org/10.1093/scan/nst064