
1. Introduction
According to the recommendations of HAS in 2014, the learning curve of surgeons can no longer be the same as in the past when they were trained on the patient: ‘never the first time on the patient’. The pedagogical models of practical learning in surgery are historically: animals, synthetic organs, virtual reality and bodies given to science used in a static (embalmed) mode. These models are not enough to learn all the technical steps required to perform a surgical procedure. In simulation-based training, one of the essential elements is realism of the environment and fidelity of simulation. It is therefore necessary to recreate an operating room ‘as in real life’, which requires having a simulated patient, similar to the anesthetized patient installed on an operating table as in hospitals.
2. Methods
Since 2013, we have developed a mechatronic system (called P4P ‘Pulse for Practice’) designed to be connected to a human body resulting from donation of the body to science and is acquiring the know-how to simulate ventilation and circulation on this human body, according to specifications defined by practitioners. As soon as bodies arrive in the center, they are prepared for this purpose. This involves draining the native blood from the body, and replacing it with a viscous liquid, by placing cannulas in the carotid and femoral vessels and using an injection pump. Cannulas are also introduced into the satellite veins of these arteries. Native human blood, which coagulates, is replaced by a liquid with the same mechanical properties, but without the coagulation effect (clots). An endotracheal tube is inserted into the trachea or a tracheostomy is performed to ventilate the lungs. The upper and lower limbs, as well as the cephalic end, are excluded through proximal ligatures at the venous and arterial levels so that only the trunk is re-vascularized. After 2 to 3 hours of preparation, the body is frozen at −20 °C with vascular cannulas and tracheostomy, without any preservative chemicals and thawed 3 days before using the model ().
Figure 1. Body preparation and connection diagram with the P4P system.
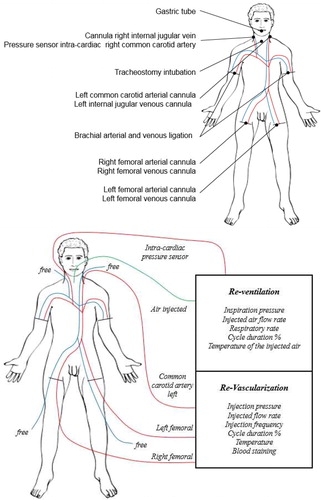
During a surgical simulation session, the bodies are installed and covered with drapes as in an operating room. The mechatronic system is then connected to the body via arterial cannulas for a pulsatile infusion of simulated blood and the tracheostomy tube for ventilation. The system allows to control the simulated physiological functions on the body. The arterial network can then be put under pulsed pressure, while controlling the pulsations rate, blood pressure and systole/diastole ratio. Simulated blood recolors and warms the viscera and drains into the venous system. The cannulas in the satellite veins of the previous arteries may be clamped (closed circuit ensuring a pulsatile vascular column without consumption of false blood) or not (open circuit of simulated blood elimination). Similarly, the lungs are re-ventilated by the tracheostomy cannula while controlling the respiratory rate, air pressure in the lungs and the inspiration/exhalation/ratio. The blood avatar is injected at a temperature of 37 °C. It increases the degree of realism by heating and re-coloring the organs. An intra-cardiac pressure sensor is used to control the system in order to have an intra-cardiac pressure in the heart of 140 mmHg, via a servo algorithm.
The mechatronic system is composed of industrial components that are themselves controlled by a two PLCs allowing surgeons to get started quickly and easily. The graphical interface has been specially designed to be intuitive ().
Figure 2. P4P System (Right: P4P Control and left: P4P Power).
To quantify the degree of realism of the re-perfused model, the Poitiers body donation center made available 8 bodies associated with this mechatronic system. Eight videoscopy adrenalectomies were performed. Each operation was performed by 3 learners and supervised by an instructor surgeon. At the end of each surgical simulation, a questionnaire concerning the degree of realism of the surgical simulation session was anonymously completed by the learners and without communication between them.
3. Results and discussion
The model has an overall degree of realism of 83% (). The main criticisms leveled by the learners were the color of the blood (which has improved since then) and the apprehension of working on corpses.
Table 1. Assessment of learners satisfaction, based on the Kirkpatrick method.
4. Conclusions
Currently, this dynamic model of the human body resulting from donation of body to science reperfused and re-ventilated is the most realistic surgical simulation tool possible because it perfectly imitates an anesthetized patient in the operating room. This tool has also been used in other surgical specialties (abdominal or thoracic) and its use has been validated by professionals who have evaluated it (multi-organ harvesting, digestive surgery, urology, gynecology, thoracic and cardiovascular surgery, etc.). Overall, 300 surgeons were trained using this technology at ABS Lab in Poitiers. This model has become an essential teaching device for simulation-based training in complex surgical procedures or exceptional surgical techniques that can be only learned by simulation (Damage Control Surgery of wounded by war weapons, victims of terrorists attacks).
Improvements to the model are underway to increase the degree of realism (simulated blood), and to adapt it for all surgical or interventional medicine specialties (cardiology, radiology, etc.) by allowing revascularization of the cephalic end for neurosurgeons and ENTs or limbs for orthopedists or plastic surgeons. Simedys distribute this tool.
Acknowledgements
L'Ecole Francophone de Prélèvement Multi-Organe, Ecole de chirurgie du Val de Grace, Société Française de Chirurgie Thoracique et Cardio-Vasculaire
References
- Carey JN, Minneti M, Leland HA, Demetriades B, Talving P. 2015. Perfused fresh cadavers: method for application to surgical simulation. Am J Surg. 210(1):179–187.
- Delpech PO, Danion J, Oriot D, Richer JP, Breque C, Faure JP. 2017. SimLife a new model of simulation using a pulsated revascularized and reventilated cadaver for surgical education. J Visc Surg. 154(1):15–20.
- Faure JP, Breque C, Danion J, Delpech PO, Oriot D, Richer JP. 2017. SIM Life: a new surgical simulation device using a human perfused cadaver. Surg Radiol Anat. 39(2):211–217.
- Kirkpatrick DL, Kirkpatrick JD. 2006. Evaluating training programs: the four levels. 3rd ed. San Francisco, CA: Berrett Koehler Publishers.