
1. Introduction
Temporomandibular joint replacement (TMJR) is the last resort in the management of end-stage TMJ disorders or diseases. There is a clear consensus about the indications for TMJR and a recent increase of the studies concerning the clinical outcomes (Johnson et al. Citation2017). The functional recovering, after the surgery, is usually assessed by the maximal incisal opening, but few studies have investigated other functional aspects (Wojczynska et al. Citation2019). Our goal is to analyse the 3 D kinematic analysis of the mandible combined with electromyography (EMG) of the masticatory muscles to study the functional abilities before and after total TMJR. This paper focuses on the evolution of the muscular activities before and after the surgery, for two patients followed during one year and compared with an asymptomatic group.
2. Methods
The protocol was validated by an ethical committee and all the subjects gave their consent to participate.
2.1. Patients
Two 62-years-old women (patient P1 and P2) underwent a TMJR on the right side. They participated in five kinematic and EMG measurements, one before and four after the surgery up to 12 months of follow-up. They filled at each step a quality-of-life (QoL) questionnaire rating eight items: pain, diet, conversation, activities of daily life, mood, anxiety, QoL linked to the health, and the general QoL.
2.2. Reference asymptomatic group
The reference group encompassed nine asymptomatic women (44 ± 9 years old). Inclusion criteria were a type1 dental occlusion, and the absence of previous TMJ disorders, clicking joint, cephalalgia and tinnitus.
2.3. Electromyographic study
After warming exercises, the subjects were asked to rest, then to bite on dental cotton at their maximum, and finally to turn their head at the maximal axial rotation. The EMG activity of the left and right anterior temporalis (T), masseters (M) and sternocleidomastoïd muscles (SCM) was recorded during each exercise and post-treated following the protocol described by Owashi Vallejo et al. (2017). Briefly, raw signals were high-pass filtered (with an additional filter for the SCM muscles to reduce ECG artefacts), rectified and smoothed. The rest-activity and the maximal voluntary contraction (MVC) were computed as the RMS values on a 10 s interval and 3 s interval respectively. To assess the fatigue appearing during a long-time hold maximal contraction, the mean power frequencies (MPF) were estimated using Welch’s method. Each exercise was repeated three times and averaged values were then computed. Specific attention was paid to ensure the repeated positioning of the electrodes.
3. Results and discussion
3.1. Asymptomatic behaviour
During the rest, the EMG activity was low (< 4.5 µV) and reproducible (standard deviation < 1 µV) for all the muscles. During the maximal bite, the MVC ranged between 128 µV and 450 µV for the T muscles and between 65 µV and 395 µV for the M muscles. On average, the MVC of the T muscles was higher than for the M (MVC Right T = 277 ± 38 µV, MVC Left T = 285 ± 113 µV, MVC Right M = 212 ± 97 µV, MVC Left M = 231 ± 86 µV). Seven subjects underwent a fatigue process, assessed as the decrease of the MPF higher than 3 Hz for at least two T and M muscles. The SCM muscles were systematically activated during maximal bite to sustain the mandible.
For the maximal axial rotation of the head, the MVC of the SCM muscles ranged between 25 and 243 µV (averaged values: MVC Right SCM = 89 ± 50 µV, MVC Left SCM = 112 ± 79 µV), showing a large dispersion between the subjects. The ipsilateral muscle was systematically activated while turning the head in a side to control the movement. Then, its activity decreased when the head achieved the axial maximal rotation (period of MVC of the contralateral SCM).
3.2. Clinical outcomes and QoL for the patients
Before the surgery, the pain was extreme for the two patients, rated as a “not controlled pain”. The QoL score was rated as “poor” and the score combining the entire item was moderate (). After the surgery, the two patients did not suffer at the joints. Patient P2 suffered from cephalalgia and neck pain during the whole period. The QoL regularly increased during the follow-up for both patients, showed by a decrease in the scores. The 6-months follow-up is missing for P2.
Table 1. Patients’ rating of pain and Quality of Life (QoL) before and after the surgery.
3.3. Evolution of the EMG activities for the patients
Before the surgery, the EMG activities during the rest were higher than the asymptomatic values for all the muscles. This is probably due to the stress generated by extreme pain. By considering the suffering (right) side, the rest-activities were higher, and the MVC activities smaller, than for the contralateral side. The MVC values during biting were significantly smaller than for the asymptomatic women, and fatigue was not observed. This may be due to a voluntary limitation by fear to suffer. Contrary to the asymptomatic pattern, the SCM muscles did not activate during the bite.
One month after the surgery, the rest-activities tended to decrease. The MVC activities of the Right T increased (). The Right M and the Right SCM were not active, which could be explained by edema, present from the ear to the neck. The MVC activities tended to increase for the other muscles. The SCM muscles contracted during the bite.
Figure 1. Maximal voluntary contractions before and after total TMJ replacement. In green: asymptomatic range (mean ± 1 standard deviation), in blue: patient P1, in red: patient P2.
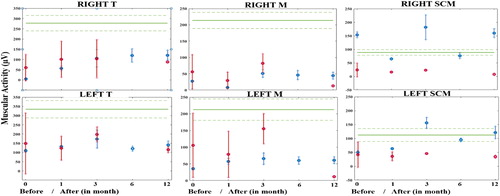
Three months after the surgery, the MVC activities increased for all the muscles but the dispersion was high. The variability of the muscular activities started to decrease for all the muscles from six months of follow-up.
One year after the surgery, for patient P1, the muscular activities during rest were similar to the asymptomatic ones. The MVC activities increased or stabilized. The values were in the asymptomatic range for the SCM muscles but much smaller than the asymptomatic values for the T and M muscles. Patient P2 decreased significantly the MVC activities for the T and M muscles between three months and twelve months of follow-up. It was clearly observed that the patient did not want to hardly bite on the cotton. Discussions revealed difficulties linked to a lack of intraoral feeling as well as the stress of suffering. All the MVC activities were smaller than the asymptomatic values.
4. Conclusions
Our study showed the functional recovering after total alloplastic TMJR through the analysis of the EMG activity of the masticatory muscles. The observed increase of the MVC with the time of follow-up was consistent with the subjective rating of the daily life abilities. One year after the surgery, the muscular activities remained however much smaller than the asymptomatic values for the T and M muscles.
References
- Johnson NR, Roberts MJ, Doi SA, Batstone MD. 2017. Total temporomandibular joint replacement prostheses: a systematic review and bias-adjusted meta-analysis. Int J Oral Maxillofac Surg. 46(1):86–92.
- Owashi Vallejo KP, Sapin – de Brosses E, Bonnet A-S. 2017. Electromyography of the masticatory muscles during biting. Comput Methods Biomech Biomed Eng. 20(sup1):155–156.
- Wojczynska A, Gallo LM, Bredell M, Leiggener CS. 2019. Alterations of mandibular movement patterns after total joint replacement: a case series of long-term outcomes in patient with total alloplastic temporomandibular joint reconstructions. Int J Oral Maxillofac Surg. 48(2):225–232.