
1. Introduction
Surgical procedures for spinal fusion with instrumentation are validated and widely practiced. As the aging population is increasing, pedicle screws anchorage is a problem in osteoporotic degenerative spines.
Biomechanical studies (Liu et al. Citation2016; Kueny et al. Citation2014) of osteoporotic spine instrumentation on anatomical parts have been carried out, using screws with a reinforced anchor as cemented or expandable screws. Comparative biomechanical analysis (Yu et al. Citation2010) of the reinforced anchored screws has been published. It concerned the lumbar, thoracolumbar and lumbar-sacral spine, with tensile-rotation-flexionbending forces measurement in pure moment: a type of force that is applied to the lumbar spine. However, the loading on the thoracic screws in osteoporotic patients is related to trunk anteflexion and thoracic kyphosis, resulting in the axial pull-out mechanism.
The aim of the study is to compare the anchoring of two different screws: standard size cemented thoracic screw versus large diameter thoracic screw optimized by scanning pedicle measurement. We reproduced the pure tensile force using a hydraulic traction machine, applied to the osteosynthesis of the upper (T3-T4) and lower (T9-T10) thoracic spine.
2. Methods
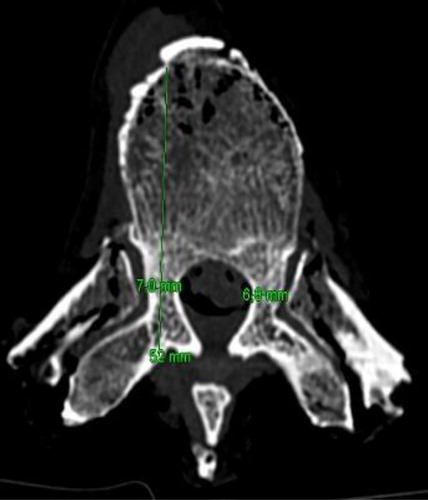
Twenty-four fresh frozen thoracic vertebrae T3, T4, T9 and T10 taken from degenerative spines were scanned to measure the maximal diameter of the pedicles and the length of the vertebral body with pedicle ().
Figure 1. Measure of the maximal diameter of the pedicles and the length of the vertebral body with pedicle (mm).
Each vertebra had a pedicle standard screw on homolateral pedicule (4.5 mm in upper thoracic and 5.5 mm in lower thoracic) using the “Straight Forward” method with cementation. The contralateral pedicle large diameter screw was optimized with prior scanning measurement ().
Figure 2. TDM view with a right cemented screw and a left large diameter pedicle screw.

The screws used were Safeorthopaedics Cypress Fenestrated Polyaxial Screw and the PMMA used was high viscosity PMMA Safeorthopaedics.
The force required to remove thoracic pedicle screws using pure axial traction was tested by a TINIUS OLSEN (10 kN) hydraulic traction machine coupled to a 3 D stereo vision system (DETAC, Institut Pprime, Poitiers, France) (). The values of these pull-out forces obtained were collected and integrated into a matched statistical analysis to compare the two types of improved screw anchoring.
Figure 3. Illustration of the pull-out test bench.

3. Results and discussion
We compared a “Large diameter optimized screw” group with a “Cemented screw” group each containing 24 pull-out tests ().
Table 1. Pull-out test results of cemented vs optimized large diameter screw (N = 24).
For the T3 vertebrae, the average pure axial tensile force required to pull out the large diameter screws was 507 Newtons (N) while it was 393 N for the cemented screws. For T4 vertebrae, the average force required to pull out large diameter screws was 395 N compared to 388 N for cemented screws.
For the T9 vertebrae, the average force required to pull out large diameter screws was 490 N compared to 415 N for cemented screws (p = 0.59). Same for T10 vertebrae with an average force required to pull out 520 N with large diameter screws compared to 417 N for cemented ones.
For each of these levels studied, there was no significant difference between the two groups. It should be noted that four cemented screws (16%) of the 24 cemented screws tested, caused destruction of the pedicle when the screw was removed, while no large diameter screws damaged the shape of the pedicle.
4. Conclusions
This study showed that the two modes of instrumentation with reinforced anchorage were similar in terms of mechanical resistance. The interest of this study is to allow the surgeon to use an optimized large diameter screw when the catheterization of the pedicle is safe, without bone intrusion, or to use a standard diameter screw with cementing in the opposite case.
The significant rate of pedicle destruction during axial tearing of cemented screws may be a limitation in case of revision surgery in elderly osteoporotic patients. The planning and optimization of the diameter of the thoracic spine screws provide mechanical strength non inferior to conventional size cemented screws.
References
- Kueny RA, Kolb JP, Lehmann W, Püschel K, Morlock MM, Huber G. 2014. Influence of the screw augmentation technique and a diameter increase on pedicle screw fixation in the osteoporotic spine: pullout versus fatigue testing. Eur Spine J. 23(10):2196–2202.
- Liu D, Zhang B, Xie Q, Kang X, Zhou J, Wang C, Lei W, Zheng W. 2016. Biomechanical comparison of pedicle screw augmented with different volumes of polymethylmethacrylate in osteoporotic and severely osteoporotic cadaveric lumbar vertebrae: an experimental study. Spine J. 16(9):1124–1132.
- Yu B-S, Zhuang X-M, Zheng Z-M, Zhang J-F, Li ZM, Lu WW. 2010. Biomechanical Comparison of 4 Fixation Techniques of Sacral Pedicle Screw in Osteoporotic Condition. Clin Spine Surg. 23:404.