
1. Introduction
Postel, Moore I, or Schatzker IV P (Kfuri & Schatzker Citation2018) fracture is a tibial eminence sparing fracture that affects the posteromedial tibial plateau. It is a rare type of fracture accounting for 5% of all tibial plateau fractures. Knowing that these fractures are at a high risk of displacement (Cuéllar et al. Citation2015), conservative treatment is at risk of failure, besides to the risk of potential consequences such as flexure contracture and early osteoarthritis. Reduction and stabilization of this fracture using two or three anteromedial lag screws has already been demonstrated (Morin et al. Citation2016). At the same time, the endobutton technique is gaining wide reputation for its success and efficacy in ligaments reconstruction surgeries and its biomechanical properties are of interest. The main objective of this work is to compare the resistance forces of the endobutton and the screw techniques in Moore I plateau fractures, by measuring the maximal load that can be exerted on the fracture fragment and can be tolerated before the montage fails. The secondary objectives of the study are to compare the reduction of fractures as well as the displacement of the fragments at maximal load.
2. Methods
2.1. Subjects
We conducted the study on 14 cadaveric knees from 7 different bodies aged 78 to 88 years. Knees belonged to 3 women, 4 men. The two knees of each body were assigned to the two different groups.
2.2. Preparation and fracture simulation
To reproduce the Schatzker IV P fracture, we used a validated model of osteotomy (Cuéllar et al. Citation2015), allowing to create a posteromedial fragment of 20 mm thickness, at 30° in the posterior plane of the tibial plateau in the axial plane, and 75° in the sagittal plane.
2.3. Reduction technique
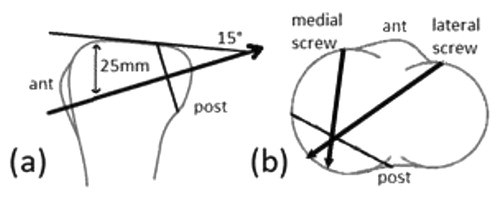
For the endobutton group, drilling was made using a 4.5 mm drill, with an anteromedial point of entry, 5 mm medial to the patellar ligament, and 25 mm distal to the tibial plateau, at a 15° angle of to the tibial plateau. (). The posterior part of the closed loop double endobutton was pulled to the posteromedial surface by a guide loop of suture then we reduced the fracture using the sliding knot of the anterior endobutton. For the screws group, reduction was performed using anteromedial and anterolateral approaches. 2x 6.5 mm holes were made to introduce 2 Low PT profile cancellous screws ().
Figure 1. The different techniques of reduction: a) endobutton; b) screws.
2.4. Data collection and statistical analysis
The samples were studied by CT scan for the evaluation of the reduction and the articular step-off was measured. For the biomechanical properties, we used a compression machine, connected to a medial half total knee arthroplasty to apply an axial compression on the reduced fragment. The loading was recorded by a loadsensor (10 kN), and the displacement by stereoscopic mark tracking method. The statistical analysis was performed using a bilateral paired Wilcoxon Mann Whitney test with the help of R software.
3. Results and discussion
3.1. Primary objective
The results concerning the maximal load tolerance of both techniques are shown in . The maximum load for the endobutton group was 1556.57 N compared to 894.07 N for the screws, the average difference was 662.50 N, IC95 [245.04; 1079.96], P = 0.007.
Table 1. Results concerning the maximal load, all data are measured in Newton (N).
3.2. Secondary objectives
The average displacement at maximal load was 0.39 mm for the endobutton group, against 1.1172 mm for the screws group IC95 [-1.92; 0.49], P = 0.20. For the assessment of the step-off after reduction, the average was 0.37 mm for the endobutton, and 0.50 mm for the screws IC95 [-0.57; 0.32], P = 0.51.
3.3. Discussion
Results show that the endobutton fixation is appear to be superior to lag screwing in terms of resistance to axial compression. This suggests a lower risk of complications. Moreover, the results showed a lower displacement under stress and a better fracture reduction, but these results were non-significant.
This endobutton technique is not commonly used in the management of fractures. However in one study done by Robinson et al., the endobutton technique showed good functional and radiological outcomes with a low prevalence of complications in the fixation of displaced fractures of the lateral end of the clavicle in younger patients. Applying this technique to Moore
I fractures seems feasible and safe; The anteromedial application of the endobutton seems possible using the safe spots described by Ilizarov in the anterior approach of the proximal tibia for the placement of external fixators (Nayagam Citation2007). Moreover both the parapatellar anteromedial and anterolateral approaches can allow us to closely achieve the perpendicularity of the reduction with respect to the fracture line which is essential as described by the AO principles, yet we preferred the anteromedial approach, in order to decrease the length of the endobutton, thus decreasing the elongation/lengthening tension expected under the same load, therefore a better stability. Our study includes some limitations: the average age of the tested knees was 83.3, while the Postel fracture occurs mainly in young patients (Morin et al. Citation2016), however this limitation is inseparable from cadaveric studies and a limited number of subjects.
4. Conclusions
The endobutton reduction of Moore I tibial plateau fracture is superior to the screw fixation in terms of tolerance to loading forces, besides to a better fracture reduction and lower secondary displacement. This is an innovative technique, as the endobutton has never been used in the treatment of such fracture, and combined with arthroscopic guidance, it can be effective.
References
- Cuéllar VG, Martinez D, Immerman I, Oh C, Walker PS, Egol KA. 2015. A biomechanical study of posteromedial tibial plateau fracture stability: do they all require fixation? J Orthop Trauma. 29(7):325–330.
- Kfuri M, Schatzker J. 2018. Revisiting the Schatzker classification of tibial plateau fractures. Injury. 49(12):2252–2263.
- Morin V, Pailhé R, Sharma A, Rouchy R-C, Cognault J, Rubens-Duval B, Saragaglia D. 2016. Moore I postero-medial articular tibial fracture in alpine skiers: surgical management and return to sports activity. Injury. 47(6):1282–1287.
- Nayagam S. 2007. Safe corridors in external fixation: the lower leg (tibia, fibula, hindfoot and forefoot). Strategies Trauma Limb Reconstr. 2(2-3):105–110.
- Robinson CM, Akhtar MA, Jenkins PJ, Sharpe T, Ray A, Olabi B. 2010. Open reduction and endobutton fixation of displaced fractures of the lateral end of the clavicle in younger patients. J Bone Joint Surg Br. 92(6):811–816.