
1. Introduction
Fascia is a fibrous connective tissue present all over the body. This study focuses on the deep fascia that is overlying muscles of the outer thigh. Indeed, fascia lata is involved in various pathologies, such as iliotibial band syndrome, inflammatory lesions, traumatic injuries etc. (Huang et al. Citation2013). This fascia has a sheathing effect on muscles and a stabiliser effect on the knee and hip joints during movements (Eng et al. Citation2014); however, these sheathing and stabiliser effects have not been quantified yet.
Skin is connected to the muscle via fascia and adipose tissues. It also plays a role of sheath on underlying tissues. Thus, body movements cause the stretching of all these tissues.
To unserstand what are the involed mechanical phenomena in these tissues and how they interact, the objective of this study is to look at superfical strain fields of the skin and deep fascia of the thigh during knee flexion extension movements.
2. Methods
2.1. Specimen preparation
One fresh post-mortem female subject (71 y.o) from the Department of Anatomy of the University of Rockefeller (DUAR), Lyon, was instrumented to measure the relative movement of bones during knee flexion-extension. Rigid tripods of markers were screwed in the pelvis, in both femurs and in both tibias. Tripods in the femur were implanted in the medial condyle so that they do not interfere with the lateral and anterior areas of the thigh where soft tissue strains were measured. Palpation of anatomical points was performed with a rigid tripod to define the standard anatomical frames of the lower limb bones.
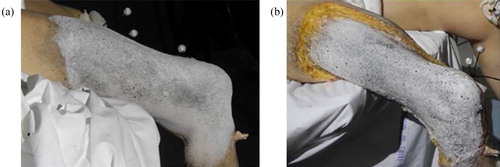
In order to measure superficial strain state of the thigh skin and deep fascia during knee flexion, a random dots (speckle) pattern was needed. Speckle pattern was done on the surface of the skin using a background of white make up and by spraying black paint (). The body was then placed at ambient temperature, lying on this back with buttocks at the edge of the table so that both legs could hang and allow full knee flexion. After skin and adipose tissue removal, the same method was applied on the deep fascia.
Figure 1. Speckle pattern on the right thigh: (a) skin, (b) fascia. Tripods of markers are partly visible.
2.2. Motion analysis
The recording of tripods’ locations was performed with an OptiTrack system. Eight cameras with infrared LEDs were installed around the subject for better visibility and markers tracking. The frame rate was 100 Hz.
2.3. Digital image processing
The stereo correlation set-up requires a pair of low noise, temporally stable cameras that are rigidly mounted in relation to each other during system calibration and subsequent data capture. The cameras used for these tests were GO-5000-USB from JAI’s Go Series with objective KOWA LM12HC where lenses are 12.5 mm. The frame rate was 50 Hz.
Cameras were placed in order to look at the lateral and anterior sides of the thigh to obtain the needed field of view. Care was taken to match cameras centres. After cameras’ setting, calibration was carried out using a calibration grid adapted to the size of the field of view. Data were processed with VIC-3D software. Motion analysis and stereo correlation acquisitions were synchronized using a common trigger box sending a rising edge square signal to both systems.
2.4. Test conductions
Several leg movements were recorded for varying hip angles: 0°, 45° and 90°. The knee extension - flexion range of motion was from 0° to 140° (full flexion). These movements were chosen in order to cover the possible positions of the leg during daily life activities and stretching. Movements were repeated twice during one acquisition and were similar when looking first at the thigh skin and then at the deep fascia.
3. Results and discussion
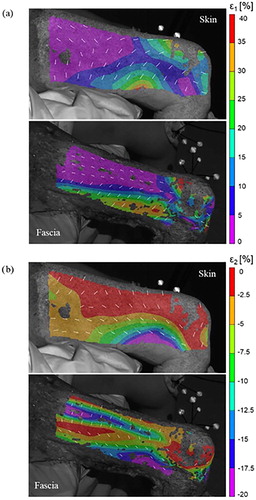
The image with a hip angle of 0° and knee extension was considered as reference image for strain analysis. Preliminary results () show the distribution of the major ε1 and minor ε2 principal strains for a flexion of the knee close to 90°, when hip was at 0°. The knee area stretched a lot due to knee flexion, and strain was not computed on many points in this area. On the thigh skin, the principal strains directions are homogeneous on the distal half part of the thigh showing tension lines around the knee. It differs on the proximal half part of the thigh, maybe because of the table leading to non-free boundary conditions. Regarding the fascia, principal strain directions differ above the iliotibial tract (ITT) and on the area of ITT. On the ITT area, principal strains observed are larger and form an angle with the longitudinal direction of the thigh although ITT has main collagen fibres orientations in the longitudinal direction of the thigh (Otsuka et al. Citation2018).
Figure 2. Principal strain fields for a hip angle of 0° and a knee angle close to 90°: (a) major ε1 strain, (b) minor ε2 strain. White arrows show the direction of the principal strains.
Several limitations were found in this study. Holes on strain maps appear because of tissues’ brightness and fluid loss when stretching them, inducing less accuracy in strain measurements. Secondly, movement of the leg was manually controlled and may differ from one test to another. Finally, tests were performed in a passive state and thus muscles contribution was not considered. Therefore, further controlled tests are required on a higher number of subjects.
4. Conclusions
To our knowledge, this study is the first considering the effect of changing hip and knee angles on skin and deep fascia surfacic strain fields. Strain field is heterogeneous for both skin and fascia surfaces, which is related to their anisotropy properties and fibres distributions. When major strain shows the area was fully stretched, minor strain demonstrates where thigh was compressed. Therefore, further work is needed to compare principal strain directions and fibre orientation in order to better understand the mechanical role of these tissues.
References
- Eng CM, Pancheri FQ, Lieberman DE, Biewener AA, Dorfmann L. 2014. Directional differences in the biaxial material properties of fascia lata and the implications for fascia function. Ann Biomed Eng. 42(6):1224–1237.
- Huang BK, Campos JC, Michael Peschka PG, Pretterklieber ML, Skaf AY, Chung CB, Pathria MN. 2013. Injury of the gluteal aponeurotic fascia and proximal iliotibial Band: anatomy, pathologic conditions, and MR imaging. RadioGraphics. 33(5):1437– 1433.
- Otsuka S, Yakura T, Ohmichi Y, Ohmichi M, Naito M, Nakano T, Kawakami Y. 2018. Site specificity of mechanical and structural properties of human fascia lata and their gender differences: a cadaveric study. J Biomech. 77:69–75.