
1. Introduction
Trunk range of motion (ROM) could be divided into two anatomical parts: the movements of the thorax and the lumbar spine. The trunk mobility is largely described with gait, but few studies are interested in the posture and amplitude of the movement itself, while they are of real interest for future applications for patients (scoliosis, low back pain, upper back pain, Parkinson …). Existing literature on vertebral ROM is focused on the lumbar spine in healthy subjects and in subjects with low back pain (Negrini et al., Citation2016) and not on the thoracic and lumbar spine. Difficulties associated with the explorations of all movements (flexion, extension, lateral blending, and rotations) in a single series of acquisition could be noticed. Optoelectronic system appears as a gold standard to measure the ranges of motion noninvasively. It has been validated in cervical range of motion (Song et al., Citation2018), and it is used like reference in lumbar range of motion (O’Sullivan et al., Citation2012). The objective of this study is to collect trunk ROM data in the asymptomatic population, according to decomposition into three segments in trunk: high thorax (HT), low thorax (LT) and lumbar spine (LS). The ROM of each segment for each movement will be studied.
2. Methods
2.1. Subject characteristics
The recruiting concerns major healthy subjects. Exclusion criteria were: back pain within the last 3 months, pregnancy in the last 12 months, all anomalies of spine. If subject endured a trauma last 12 months, which can affect his static or dynamic posture, he was excluded of this study. All subjects receive an information notice and signed a consent form at beginning of study.
2.2. Protocol and marker positioning
The Codamotion system (Charnwood Dynamics Ltd) is used. It’s an optoelectronic system using three cameras in a tower, transmitters and actives sensors. The sensors are positioned on the skin. The ODIN001 software is used for data acquisition and the Matlab software is used for data processing. Twelves sensors were positioned on the thorny processes of C7, T4, T12, S1 vertebrae, on the maximum curvature of kyphosis and lordosis, on iliacs and on scapulae.
2.3. Data post-processing and statistics analysis
A Matlab script (Mathworks, VILLE, PAYS) has been developed for the post-processing of the data. Visibility of each marker is computed on the whole acquisition. Missing data are completed as average value between the last and next visible point. The maximum ROM are defined as the angle between the initial position (defined as the first second of the acquisition) and the maximum angle of the trunk (average of the three maximal values). Global ROM are defined for C7-S1 segment. The kyphosis angle (C7-maxK-T12) and lordosis angle (T12-maxL-S1) in initial position were computed using fitting circles by three sensors locations. Vertebral levels are interpolated between anatomical sensor location (C7, T4, T12, and S1). Segmental ROMs are defined for: the high thorax (C7-T4 sensors), the low thorax (T4T12) and the lumbar segment (T12-S1). The contribution of each segment to the global ROM is quantified through their own displacement in time (). The pelvis movement is calculated as the mean displacement of iliacs sensors during test.
Figure 1. Lateral bending. A) Sensors displacement during movement acquisition. B) Vertebral extrapolation based on sensor locations.
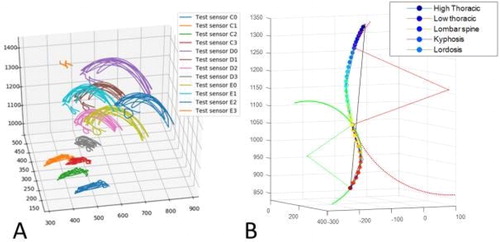
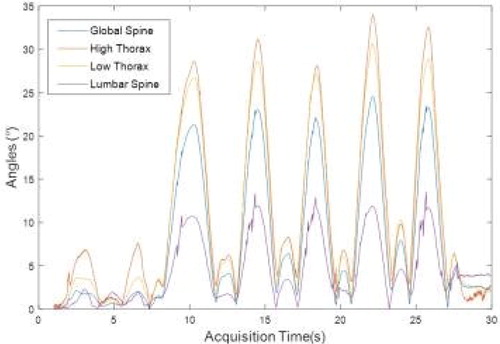
Figure 2. Global and segmental ROM during movement acquisition.
3. Results and discussion
15 healthy participants (age: 28.9 ± 7.7y., body mass index: 22.9 ± 3.5, 7 women) were included with an average weekly sportive activity of 4.1±.4.5h. Missing markers for visibility during acquisition is reported in and is under 20% for rotations and lateral bendings. Quality of the flexion data was not sufficient to compute global and segmental ROM. Such results were then excluded from the rest of the analysis.
Table 1. Missing data and ROM for flexion, rotations and lateral bending for the whole segment (C7-S1), the high thorax (HT), the low thorax (LT) and the lumbar spine (LS).
Global and segmental ROM average on the population is reported in and example of a curve can be found in .
To be noticed that the segmental ROM are found higher than the global ROM highlighting different contribution and motions of each segments: while the high and low thorax motions were found higher for rotation and lateral bending, the contribution of the lumbar spine seems limited in stand up posture.
References lumbar values for rotations were found between 8.4°±3.9° and 2.3°±5.8° (Vicon and Electrogoniometer) (Tojima et al. Citation2013). Similarly, reference values for lateral bending of the lumbar segment were found between 16.3° and 23.7°, and between 31.9° and 35.0° for the thorax (Tojima et al. Citation2013).
Pelvis movements highly depended of the considered task and ranged from 3.8 cm (lateral bending) to 10.3 cm (contralateral for the rotation) in average depending of the side and of the task.
Kyphosis and lordosis were analysed in static posture, resulting respectively in average values of 34.3°±8.0° for and 42.1°±16.8°. The variabilities between intraindividual measurements were respectively of 9.2° and 20.8°. Variations of the kyphosis values found in the literature (D’Amico et al. Citation2017) highlight the different methods use for such measurements based on skin sensors (T4–T12: 31.9°±7.65°(14.2°–51.6°); 45.85°±3.64°(27.24–64.46°)). Lordosis seems to depend of gender (Males: 25.65°±9.38° (4.0°–53.0°); T12-L5 Females: 39.45°±8.97° (16.9°–60.0°).
4. Conclusions
Those preliminary results show that the high variability of the measurements in the literature which depends of the protocol and acquisition system used. It is highlighted that the motion of the pelvis is non negligible and that the segmental analysis is interesting to describe the contribution of each part of the spine towards the definition of strategy of motion by individual. Further studies are needed to improve and test the reproducibility of such protocol.
Acknowledgements
We thank Aurélien Lamolle, Max Py and Maxime Llari for their support and expertise.
References
- D’Amico M, Kinel E, Roncoletta P. 2017. Normative 3D optoelectronic stereo-photogrammetric posture and spine morphology data in young healthy adult population. Plos One. 12(6):e0179619.
- Negrini S, Piovanelli B, Amici C, Cappellini V, Bovi G, Ferrarin M, Zaina F, Borboni A. 2016. Trunk motion analysis: a systematic review from a clinical and methodological perspective. Eur J Phys Rehabil Med. 52(4):583–592.
- O’Sullivan K, O’Sullivan L, Campbell A, O’Sullivan P, Dankaerts W. 2012. Towards monitoring lumbopelvic posture in real-life situations. Man Ther. 17 (1):77–83.
- Song H, Zhai X, Gao Z, Lu T, Tian Q, Li H, He X. 2018. Reliability and validity of a coda motion 3D analysis system for measuring cervical range of motion in healthy subjects. J Electromyogr Kinesiol. 38:56–66.
- Tojima M, Ogata N, Yozu A, Sumitani M, Haga N. 2013. Novel 3D motion analysis method for measuring the lumbar spine range of motion: repeatability and reliability compared with an electrogoniometer. Spine. 38 (21):E1327–1333.