
1. Introduction
Gait is the main mean of movement for Man, therefore an abnormality or deficiency related to it can be disabling. This deficiency is generally caused by a muscular dysfunction or some neurological pathologies such as strokes or Charcot-Marie-Tooth Disease. One of the most commonly used treatment of such problems is the Ankle Foot Orthosis (AFO) (Sawicki and Ferris Citation2009). Passive dynamic AFOs (PD-AFOs) are a category of AFOs that uses design features, such as stiffness, to improve gait performance through storage and elastic energy return (Faustini et al. Citation2008; Benabid et al. Citation2012). The aim of this study is to demonstrate the beneficial effect of an AFO on Vertical Ground reaction forces (VGRFs) impulse during gait for patients suffering from dorsiflexion deficits. To achieve our goal a Wintrack® force platform was used to provide components of VGRFs during gait.
2. Methods
In this study seven patients (53.57 ± 16.17 years old, 1.80 ± 0.07 m height, and 89 ± 15.06 kg body mass) with different pathologies (Stroke, Axonal neuropathy, head trauma and Charcot-Marie-Tooth Disease) were recruited. The recruitment of the participants occurred from January 2019 to February 2019, in the University Hospital Centre (Sebastopol, Reims- France). The inclusion criteria were as follows: adult individuals of both sexes, suffering of deficit during gait. as for the exclusion criteria: individuals with risk of fall. All participants were informed about the aim and objectives of the study and agreed to participate through a written consent form.
The system used in this study is: a foot pressure sensitive walkway dedicated to static, posturogaphic and gait analysis with total freedom in stance and motion acquisition (Wintrack® Medicapteur) (), with a size of: 1610 × 652 mm and a thickness of 9 mm. Which has 12 288 Resistive HD sensors. The AFO (MecaFlex®) () was then adapted and installed on the affected lower limb(s). The patients were instrumented on the affected limb(s) (two on the Right, Two on the Left and Three on both limbs).
Figure 1. Wintrack® Medicapteur force platform used in the study.
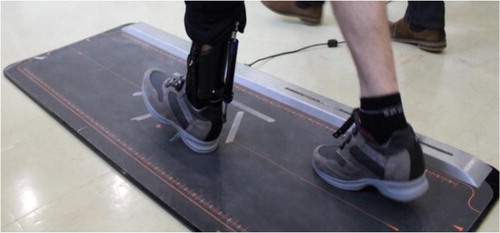
Figure 2. The PD-AFO. The AFO composed of two main parts: The calf part & the Spring cylinder and the orthopedic shoe.

This PD-AFO has two main parts: a calf part which is made from carbon fiber sheet equipped with spring cylinder with adjustable stiffness and an orthopedic shoe. The two parts are connected with a ball joint to ensure a total mobility of the ankle. Lateral straps are used to prevent excessive valgus/varus movement during gait.
A nine-meter walkway with the force platform installed in the middle of it was used to evaluate gait. Patients perform three times the trial of six passages (3 × 6) for each trial back and forth across the platform in a self-selected speed, both with and without the PD-AFO, passages with completed gait cycle are retained to be computed. Pressure and spatiotemporal data are acquired from each trial and then the Vertical Ground Reaction Force (VGRF) impulse were computed using the time integral of the VGRFs for the whole foot for two steps: left and right.
To evaluate the efficiently of the used PD-AFO we compare the VGRF for the affected and instrumented limbs to the non-affected and non-instrumented ones.
A nonparametric Wilcoxon signed-rank test was performed to compare numerical data for two populations: with versus without the PD-AFO. The level of significance has been set to 0.05 (*).
3. Results and discussion
All trial results for the seven patients were treated, computed to get the VGRF impulse, averaged and statistically tested. The average values for each patient with vs without for the affected and instrumented limb are summarized in ().
Table 1. VGRF Impulse for all the patients.
A significant difference (*) was observed for the subjects for the affected and instrumented lower limb (p = 0.05) and a less significant improvement for the non-affected and non-instrumented lower limb (p = 0.06) in the VGRF impulse. Such results demonstrate the beneficial effect and the positive impact of the assistance brought by the spring cylinder pushing the leg forward during the initial swing phase. Helping the patient to propel himself forward easier giving him better propulsion and more fluid gesture. This results showed that the PD-AFO has a positive impact on the VGRF impulse during gait and not only on the spatiotemporal parameters (Nolan and Yarossi Citation2011; Vistamehr, Kautz, and Neptune Citation2014).
4. Conclusions
In this preliminary study, the results indicate that the use of MecaFlex PD-AFO conducts to a significant increase in the VGRF impulse during gait. The latter suggests an improvement in: propulsion and grip. The next step of our study is to enlarge the population with the aim of generalizing the impact through the appropriate statistics.
References
- Benabid Y, Chettibi T, Aoussat A, Benfriha K. 2012. Design and implementation of orthosis to improve gait of patients with hemiplegia. Computer Method Biomech Biomed Eng. 15(Suppl 1):345–347.
- Faustini MC, Neptune RR, Crawford RH, Stanhope SJ. 2008. Manufacture of passive dynamic ankle–foot orthoses using selective laser sintering. IEEE Trans Biomed Eng. 55(2):784–790.
- Nolan KJ, Yarossi M. 2011. Preservation of the first rocker is related to increases in gait speed in individuals with hemiplegia and AFO. Clin Biomech. 26(6):655–660.
- Sawicki GS, Ferris DP. 2009. A pneumatically powered Knee-Ankle-Foot Orthosis (KAFO) with myoelectric activation and inhibition. J Neuroeng Rehabil. 6(1):23.
- Vistamehr A, Kautz SA, Neptune RR. 2014. The influence of solid ankle- foot-orthoses on forward propulsion and dynamic balance in healthy adults during walking. Clin Biomech. 29(5):583–589.