
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.1. Introduction
Spine surgery planning involves many decisions for which the surgeon has not enough information, and for which a dynamic model can be helpful. Research studies show a high variability in decision making in the planning of scoliosis surgery by experienced surgeons (Robitaille et al. Citation2007). That variability is problematic because this lack of information may cause complications for the patient, such as revision surgery or an increased limitation in spine mobility. Therefore, a biomechanical model for spine surgery planning can be useful in providing the surgeon with the information needed to propose the best treatment. In this context, intervertebral efforts represent an essential input in assisting diagnosis and subsequently guiding the surgical planning of scoliosis.
In this regard, we have created a biomechanical model based on clinical and experimental data, and on a multibody model of the upper body able to quantify the intervertebral efforts for idiopathic scoliotic adolescents in standing up position (statics) and during gait (dynamics) (Abedrabbo Citation2017).
Obviously, it is not easy to measure the effectiveness of this kind of tool, as the negative effects of a poor surgical planning, such as the degeneration of the intervertebral discs, only appear a number of years after spinal surgery. It is therefore not possible to prove - in the short term - that the results predicted by this approach will improve the quality of life of a particular patient. To circumvent this problem, and to avoid the use of invasive methods of measurement (Damm et al. Citation2016), this study proposes a retrospective analysis of twenty-two patients suffering from scoliosis (fifteen operated and seven non-operated) who were followed over several years.
Although this study will not allow us to estimate if the values obtained by our solution are close to reality, it will allow us to estimate if the predicted values (whether they are close to the real intervertebral forces or not) could help a surgeon to predict a potential problem to the patient.
In this context, the objective of this study consists in analysing if the degeneration of the discs could be correlated with the intervertebral lateral shear efforts predicted by our biomechanical model.
2. Methods
The data used for this analysis is based on a longitudinal study carried at the Université catholique de Louvain. The evolution of the spine deformation over the years is used to estimate the intervertebral degeneration.
2.1. Population and data
Twenty-two patients (fifteen operated and seven non-operated) suffering from idiopathic scoliosis (AIS), followed over several years (between four and ten years) have been analyzed.
The data used for this study are the following:
Patients masses. Used to estimate the mass distribution in our biomechanical model of the upper-body.
Bi-planar (coronal and sagittal) X-rays of patients, 6 months after surgery. Used to build the biomechanical model but also to estimate the initial deformation between the different intervertebral discs,
(Abedrabbo Citation2017).
Coronal X-rays of patients several years after surgery. Used to estimate the deformation between different intervertebral discs
2.2. Biomechanical model
Model Definition - Starting from the bi-planar X-rays data (3D Cartesian coordinates of each intervertebral disc reference points), the developed software automatically generates a 3D multibody representation of the spine. The model used for this study contains:
Eighteen rigid bodies representing the moving pelvis and the seventeen vertebrae. These bodies are interconnected via five articulations. (2 rotational and 3 translational joints);
Two moving bodies representing the wobbling masses of the abdominal cavity;
Four internal action/reaction forces, representing the main muscular groups acting in the back and abdomen.
Inputs and output of the model -The input data come from X-rays and a simplified vertical and lateral sinusoidal motion is used to emulate a realistic motion (gait). This motion is imposed to the pelvis to estimate the dynamic component of the intervertebral forces. This input is based on data obtained from previous studies, were the pelvis motion was measured experimentally for a smooth gait-type motion. The input time history is represented as follows ():
Figure 1. Imposed pelvis motion.
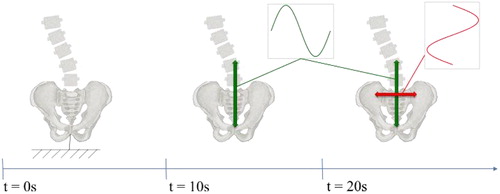
(t = 0 & t < 10 s) Static position (static forces),
(t = 10 & t < 20 s) Simplified Up/Down vertical motion,
(t = 20 & t < 30 s) Combined Up/Down and Left/Right lateral motion.
The main output are the maximal intervertebral shear forces along the spine during the entire simulation.
3. Results and discussion
Four possible scenarios have been found for each intervertebral disc, that can be highlighted:
Case 1: The model predicts a significant lateral force and, at the same time, there is a significant evolution in the degeneration angle: good results, the model could help such patients if used at the time of the planning.
Case 2: The model predicts a significant lateral force but there a minor evolution in the degeneration angle: weak results, it means that disc degeneration is not correlated to the computed lateral intervertebral force.
Case 3: The model predicts a minor lateral force but there is a significant evolution in the degeneration angle: not relevant results. It might mean two things; either the model was not able to predict a future increase in forces, or the deformation results from another cause.
Case 4: The model predicts a minor shear force and, at the same time, there is a minor evolution in the degeneration angle: relevant results, the model confirms the choice of the surgeon.
According to , the results obtained during this pre-clinical study are promising, since the model could improve the surgery of four patients if it was used at the moment of the surgery (about 18%). However, due to the size of the sample, it is not currently possible to take any definitive conclusions.
Table 1. Results classification: four possible scenarios.
There was just one case (4.5%) where the model predicted results that seems to be erroneous. The results obtained for this patient should be analysed more in details. Indeed, although our model has predicted a risk for the patient, the deformation was located in the adjacent levels. An explanation could be that the forces predicted by the model induce the deformation at another level, close to the predicted critical location.
This preliminary study has also allowed us to identify a threshold lateral shear force value of about 160 Newton. It seems that above that threshold, the risk of disc degeneration increases significantly. This value should be confirmed with more patients in the future.
4. Conclusions
There is not a bi-directional correlation between the intervertebral forces and the intervertebral disc degeneration. For some cases, lateral shear forces clearly induce intervertebral disc degeneration. However, there were several well-equilibrated patients with some degree of disc degeneration, whose origin is thus of a different nature.
Nevertheless, the results obtained in this study suggest that the model could improve the surgical planning in patients suffering from scoliosis. It is still necessary to analyse a larger population in order to confirm this observation; the sample-size used for this preliminary study is not sufficient. Nevertheless, given the conditions of this study, (non-calibrated X-rays and rather simplified motion input), the results are promising and recognized as such by physiotherapists and surgeons.
References
- Abedrabbo G. 2017. Quantification of intervertebral efforts using a multibody dynamics approach: application to scoliosis [PhD Thesis]. Louvain-la-Neuve, Belgium: Université catholique de Louvain.
- Damm P, Kutzner I, Bergmann G, Rohlmann A, Schmidt H. 2017. Comparison of in vivo measured loads in knee, hip and spinal implants during level walking. J Biomech. 51:128–132.
- Robitaille M, Aubin CE, Labelle H. 2007. Intra and interobserver variability of preoperative planning for surgical instrumentation in adolescent idiopathic scoliosis. Eur Spine J. 16(10):1604–1614.