
1. Introduction
Crouch gait is one of the most common gait deviations in cerebral palsy. When caused by short hamstrings, surgical lengthening may be indicated. Although effective this procedure may also be inefficient or iatrogenic on the pelvic tilt. Musculoskeletal modelling has been introduced to help lengthening decision (Arnold et al. Citation2006). We add to this approach clinical maximum hamstring length and machine learning in a procedure named SiMusCP (Desailly et al. Citation2012; Sebsadji et al. Citation2012). Except in MacWilliams et al. (Citation2016) and Laracca et al. (Citation2014) studies has only assessed the benefits of those approaches on series that has not been operated with knowledge of the recommendations prior to surgery. The purpose of this paper is to assess the contribution of the SiMusCP procedure to surgical decision making.
2. Methods
2.1. Population
Among a database of 190 children with cerebral palsy, operated, with at least a clinical gait analysis before and after surgery, those having had a SiMusCP procedure before and after surgery are included.
Patients with distal femoral osteotomy are excluded.
2.2. Surgical indication
Since July 2011 the surgeon was informed of every recommendations of the SiMusCP procedure. He then took freely his surgical decision taking into account also many other factors (physical examination, clinical gait analysis, electromyography, imagery, patient’s project, general condition …)
2.3. Data collection
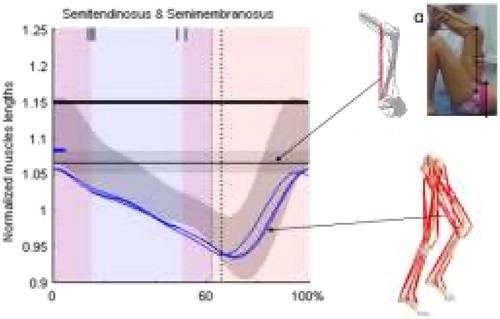
Data were recorded and processed as described in (Desailly et al. Citation2012; Sebsadji et al. Citation2012) ().
Figure 1. Illustration of the data inputted in the SiMusCP procedure. After a model personalisation, the functional hamstring length is modelled on the basis and of the clinical gait analysis measures and the clinical maximum hamstring length is computed using the clinical measurement α (bilateral popliteal angle). Those lengths are respectively compared to decision thresholds (the small bold blue hyphen and the horizontal bold line). If both are under those thresholds hamstring lengthening indication is proposed to the surgeon.
2.4. Data analysis
Concordance between the SiMusCP recommendations and the actual surgical decision is evaluated by Fisher exact test and odd ration computations. For all the hamstrings lengthening realized after July 2011 two groups are defined ‘indication’ and ‘contraindication’ depending on the recommendations of the algorithm. The kinematic outcomes of those two groups are compared regarding the knee flexion at initial contact (KFIC) and the mean pelvic tilt (PT) by t-tests.
3. Results and discussion
One hundred and twenty two patients (205 lower limbs) are included. Among them 102 lower limbs had a hamstring lengthening. Their KFIC are decreased from 43 ± 12° to 27 ± 10°
(p < 0.05), their PT are augmented 13 ± 6° to 18 ± 8° (p < 0.05) and their GDI are improved from 63 ± 9 to 70 ± 9 (<0.05).
The global series shows that hamstring lengthening gives good results on the KFIC while slightly worsening the pelvic tilt.
SiMusCP procedure is studied on the lower limbs operated after 2011. Among those 114 lower limbs, 46 had a hamstring lengthening. 68% of the recommendations were followed by the surgeon
(Fisher test <0.05; Odd ratio = 3.88) If the agreement between the recommendations and the actual surgeon’s decisions is good (68%) the reasons of the 32% of disagreement remain to be investigated.
The lower limbs with hamstring lengthening were either indicated or contraindicated by SiMusCP. The ‘indication’ group (n = 22) and the ‘contraindication’ (n = 24) group had different postoperative outcomes presented by and .
Figure 2. Individual knee flexion at initial contact and pelvic tilt outcomes for the ‘indication’ and ‘contraindication’ groups.
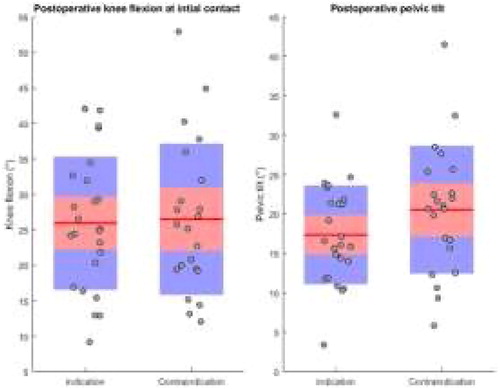
Table 1. Postoperative hamstring lengthening results on knee flexion at initial contact and pelvic tilt in degrees for the ‘indication’ and ‘contraindication’ groups.
Indicated or contraindicated by SiMusCP, the postoperative KFIC show no statistical difference. The indicated hamstring lengthnings do have postoperative pelvic tilt that are significantly lower than in the contraindicated group. SiMusCP recommend to operate the lower limbs that are less prone to suffer of an iatrogenic effect of the hamstring lengthening on the pelvic tilt.
4. Conclusions
The SiMusCP procedure recommendations were followed in 68% of the case. The patients operated in agreement with the recommendations had less postoperative pelvic tilt. The procedure gives beneficial information to the surgeon has it may help to prevent the side effects of the hamstring lengthening on the pelvic tilt.
Acknowledgements
The authors are grateful to the medical and technical staff of Fondation Ellen Poidatz for useful discussions and for recording the data used for this work.
Additional information
Funding
References
- Arnold AS, Liu MQ, Schwartz MH, Õunpuu S, Delp SL. 2006. The role of estimating muscle-tendon lengths and velocities of the hamstrings in the evaluation and treatment of crouch gait. Gait Posture. 23(3):273–281.
- Desailly E, Sebsadji A, Yepremian D, Hareb F, Khouri N. 2012. Simulation of muscle retraction in cerebral palsy. Validation of a decision support system for surgical lengthening of contractured muscles. Comput Methods Biomech Biomed Eng. 15(Suppl 1):263–265.
- Laracca E, Stewart C, Postans N, Roberts A. 2014. The effects of surgical lengthening of hamstring muscles in children with cerebral palsy: the consequences of pre-operative muscle length measurement. Gait Posture. 39(3):847–851.
- MacWilliams B.A, Stotts A.K, Carroll K.L, D’Astous J.L. 2016. Utilization and efficacy of computational gait analysis for hamstring lengthening surgery. Gait Posture. 49:394–397.
- Sebsadji A, Khouri N, Djemal K, Yepremian D, Hareb F, Hoppenot P, Desailly E. 2012. Description and classification of the effect of hamstrings lengthening in cerebral palsy children multi-site surgery. Comput Methods Biomech Biomed Eng. 15(Suppl 1):177–179.