
1. Introduction
In the case of an adolescent with Idiopathic Scoliosis (IS), a complex three-dimensional deformity of the spine was observed which affected the structural bones of the pelvis (Holewijn et al. Citation2017). To evaluate the incidence of this deformity and the influence of spinal fusion (which prevents the further development of spinal deformity), gait analysis was performed under different conditions (such as treadmill versus over-ground; imposed velocity versus free velocity) (Holewijn et al. Citation2017). However, using a treadmill influences kinematics: Staszkiewicz et al. (Citation2012) revealed differences between walking on a treadmill and walking over-ground in the case of healthy subjects. Walking on a treadmill causes the pelvis to make lower displacements in the transverse plane. Furthermore, this condition has been used to evaluate the influence of spinal fusion in the case of patients with IS (with imposed velocity) (Holewijn et al. Citation2017). The reduction of pelvic mobility in the transversal plane observed after spinal fusion could be exaggerated and influence the upper segments of the trunk. Therefore, for patients with IS, it seems interesting to evaluate the incidence of spinal fusion on such pelvic and spinal segments during walking over-ground conditions.
It seems that patients with IS use different strategies like changing the pattern of pelvic motion or changing the velocity of walking to minimize incidences of scoliosis (Holewijn et al. Citation2017). In healthy subjects, Feipel et al. (Citation2001) showed specific correlations between Range of Motion (RoM) of the lumbar spine and speeds. For patients with IS, correlations between the motion of the pelvis and walking velocity could be used to describe the influence of scoliosis and spinal fusion. Therefore, regarding walking over-ground and free speed, two questions are asked: (1) with similar walking speeds before/after spinal fusion, is there a reduction after spinal fusion in the kinematics of four spinal segments (neck, thorax, thoracic-pelvis and pelvis) in patients with IS? (2) Does this surgery reduce the correlation between walking velocity and the kinematics of the pelvis?
2. Methods
2.1. Population
Patients with IS (n = 17; 14 women and 3 men; mean age: 17.00 years (3.81); Cobb angle before fusion: 49.7° (12.8); Cobb angle after fusion: 17.24° (7.5)) enrolled in a clinical trial comparing gait data before and one year after spinal fusion. They were operated by the same orthopedic surgeon. A gait analysis was subject to medical follow-up. Patients gave informed consent form to used anonymous data. They were recruited from patients scheduled for a spinal fusion between January 2013 and December 2016. Asymptomatic subjects (n = 17; 10 women and 7 men; 19.63 years (0.81) were our control population.
2.2. Material and method
Subjects walk on a 10 m level ground walkway, at self-selected speed. From ‘Plug-in gait full body’ model applied on 31 retro reflective spherical markers (14 mm in diameter) captured with motion capture system (Vicon, Oxford Metrics, 100 Hz), gait cycles were defined as strides and kinematic data were explored. RoM on neck angles, thorax angles, lumbar angles (considered as thoracic-pelvis and computed as Holewijn et al. Citation2017), pelvis angles in each plane and gait velocity were computed for five gait cycles per subject. For each variable, data were averaged for each subject and condition. The sample size relates to the statistical power (90%) computed for RoM of pelvis mobility in coronal plane (patients before fusion and controls). All variables are presented as: mean (standard deviation). The following tests were used to establish the consequences of scoliosis on gait data (Statistica, V13, Dell, USA): Wilcoxon signed rank test for matched pairs (in case of patients), Mann-Whitney test (to compare patients and controls) and Spearman’s correlation. The accepted significance level was set at p ≤ 0.05.
3. Results and discussion
presents the comparison between the three populations. Regarding the patients, no difference was noticed between gait speed before (1.06 m s−1 (0.12)) or after spinal fusion (1.02 m s−1 (0.13)). The healthy population walked significantly faster (1.41 m s−1 (0.11)) than the patients. Only the kinematics of the pelvis was modified after spinal fusion whereas patients walked with similar velocities. In reference to (Staszkiewicz et al. Citation2012), the patients presented similar RoM for the neck, thorax, thorax-pelvis with a similar gait speed before and after fusion. As shown in , only correlations between velocity and RoM on the pelvis in transverse plane are significant for controls and patients before spinal fusion.
Figure 1. Correlations between each RoM and walking speed for each population. 1: sagittal; 2: frontal; 3: transverse. *: significant correlation.
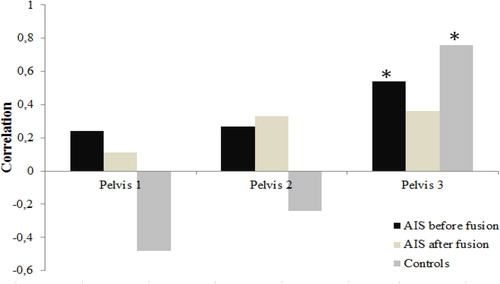
Table 1. RoM (°) on neck, thorax, thorax-pelvis (noticed T-Pel.) and pelvis. 1: sagittal; 2: frontal; 3: transversal.
Our approach evaluates the effect of spinal fusion on kinematics in the case of walking over-ground at self-selected speed. With a similar gait velocity before/after fusion, patients presented only lower RoM on the pelvis in the sagittal and transversal planes after fusion. We did not find an increase in pelvic mobility in the frontal plane as Holewijn et al. (Citation2017). The significant correlation between the velocity and mobility of the pelvis in the transverse plane could be associated with a new strategy with girdles. Patients walked at a lower speed than controls.
Spinal fusion could induce an increase in the incidence of lower back pain (Syczewska et al. Citation2010). Our results revealed lower pelvic tilt and no influence on pelvic obliquity after fusion. This result does not seem to be in phase with low back pains. Usually, exaggerated pelvic tilt or obliquity increases pains. Patients present a partial stiff gait (they restrict their movements on the pelvis): pains could depend on co-contractions on the lumbo-pelvic muscles. Several limitations can be pointed out. Firstly, we did not consider the length of spinal fusion. Secondly, only linear correlation was explored and was focused on the pelvis. Finally, co-contractions in the lumbo-pelvic muscles were not studied.
4. Conclusions
Patients with IS present lower pelvic mobility in sagittal and transverse planes after spinal fusion with similar walking velocity.
Acknowledgements
All patients included in this retrospective study. Ethics Committee of Angers for his ethical approval.
References
- Feipel V, De Mesmaeker T, Klein P, Rooze M. 2001. Three-dimensional kinematics of the lumbar spine during treadmill walking at different speed. Eur Spine J. 10(1):16–22.
- Holewijn RM, Kingma I, de Kleuver M, Schimmel JJP, Keijsers N. 2017. Spinal fusion limits upper body range of motion during gait without inducing compensatory mechanisms in adolescent idiopathic scoliosis patients. Gait Posture. 57:1–6.
- Staszkiewicz R, Chwała W, Forczek W, Laska J. 2012. Three-dimensional analysis of the pelvic and hip mobility during gait on a treadmill and on the ground. Acta Bioeng Biomech. 14(2):83–89.
- Syczewska M, Graff K, Kalinowska M, Szczerbik E, Domaniecki J. 2010. Does the gait pathology in scoliotic patients depend on the severity of spine deformity? Preliminary results. Acta Bioeng Biomech. 12(1):25–28.