
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.1. Introduction
Sternum is a flat bone composed of three parts: manubrium superiorly, xiphoid process inferiorly and the body in between (Selthofer et al. Citation2006). Manubrio-Sternal Joint (MSJ), also known as Louis’ Angle, is a synarthrosis joint. Manubrium and sternal body intersect with an angle of 165° to 175° between their posterior faces (intra-thoracic faces, Carrier et al. Citation2007). MSJ has implications in rheumatoid diseases and traumatic injuries. The potential MSJ degrees of freedom and range of motion during breathing and their relationships with ventilatory disease management stay controversial.
Recently, measurements of sternal angle on 12 asymptomatic subjects’ retrospective codified spiral-CT data (Beyer et al. Citation2017) showed MSJ variations. Subjects were on a supine position and conventional spirometry was added to monitor three states: Total Lung Capacity (TLC), Middle of Inspiratory Capacity (MIC) and Functional Residual Capacity (FRC). MSJ variations mean value from TLC to FRC was 4.4° ± 2.7°. The main limitation of this study is the invasive use of scanner that uses ionising rays.
Opto-Electronic Plethysmography (OEP) is a new non-invasive method of chest wall volume assessment based on optical computation of three-dimensional coordinates of markers fixed on the subjects’ trunk. OEP can be performed in any position (prone, supine, standing, sitting) without mouthpiece nor nose clip. OEP has been validated as an alternative to conventional spirometry. Difference between chest wall volume measured with OEP and spirometry was <1% according to Cala et al. OEP technique is suitable for acute functional respiratory examination. In the sitting position without backrest, a set of 86 markers is used to calculate total volume of the trunk. Six of these markers placed on different parts of the sternum can be used to determine MSJ displacement.
The aim of the present study is to provide a computational method based on OEP in order to quantify MSJ mobility associated with breath.
2. Methods
OEP is performed on three sportive males (age = 23 ± 0.5 years old, height = 1.84 ± 0.05 m, mass = 70 ± 2.5 kg) who are asymptomatic subjects (S1, S2, S3). 3D position of external markers is recorded by 8 infra-red emitting cameras (Vicon system, 100 Hz). Subjects are in a sitting position without backrest and are asked to perform five vital capacity manoeuvres. Total volume of the trunk was computed using variation of markers 3 D position and the Gauss-Ostrogradsky Theorem (Cala et al. Citation1996; Aliverti et al. Citation2000) Subtraction of the minimal volume (FRC) to the total volume gives the signal V(t) which corresponds to the lungs’ air flow.
Three markers are used to determine manubrium orientation in space: two placed on the median axis of the body at the upper extremity of manubrium (Mid1) and at the Louis’ Angle (Mid2), and one placed on the right first rib anterior extremity beneath clavicula (RA1). The same arrangement is used to determine the sternum orientation: two median markers at Louis’ Angle (Mid2) and lower extremity of the sternum body (Mid3) and one lateral on the second rib costal cartilage (RA2).
Median vectors (Mid1-Mid2 and Mid2-Mid3) are used as Z-axis. Cross product is used to generate two direct orthonormal vector fields: (
) attached to the manubrium orientation in space and (
) attached to the sternum orientation in space. X-axis points to the right and Y-axis points forward. Vector field attached to the sternum was considered as a reference and the vector field attached to the manubrium was mobile. Vector fields are linked by rotation matrix R:
The rotation matrix calculation with Newton-Euler method is composed of three successive rotations: rotation around
then around
and finally around
The resultant cardan angles are: θx (flexion/extension), θy (side bending) and θz (left and right rotation).
Experimental error of land mark position including motion of soft tissue was calculated with two orthonormal direct vector fields attached on coxal bones. Mean experimental error was 1,20° on θx. V(t), θx(t), θy(t), and θz(t) are analysed both on time domain using cross-correlation coefficient r and on frequency domain using a Fast Fourier Transform algorithm in order to differentiate noise and MSJ signal.
3. Results and discussion
θx(t) and V(t) signals present for each subject correlation on time domain (). Cross-correlation coefficients are greater than 0,8 with a phase signal equal to 0 ms (). Signals have similar curves in the frequency domain (). θx standard deviation had a mean value of 5.76° (). This indicates significant flexion and extension of the MSJ during breathing.
Figure 1. Time domain signals θx(t) and V(t).
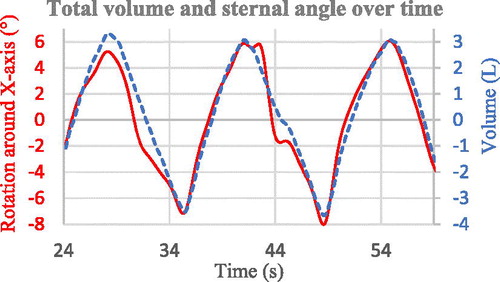
Figure 2. Frequency domain signals θx(t) and V(t).
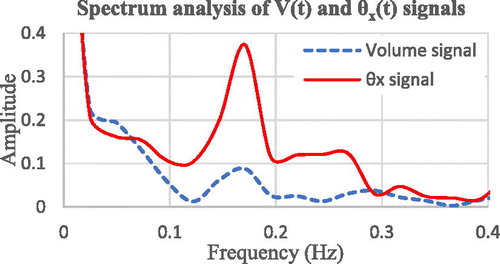
Table 1. Results for each subject.
Comparisons of θy(t) and θz(t) to V(t) show uncorrelated curves on both time and frequency domain. It indicates that variations are not related to breath and are made of noise.
During inspiration θx value increases. Manubrium rotates counter clockwise around X-axis, which corresponds to a backward inclination: Louis’ angle becomes more prominent. The opposite occurs during expiration: θx value decreases and the Louis’ angle becomes flatter. This result is in accordance with Beyer et al. conclusions.
4. Conclusion
This study shows that it is possible to measure MSJ mobility during breathing subject using non-invasive OEP method (Kaneko and Horie Citation2012). OEP assessment provides non ionising ray, reduces subject’s stress associated with conventional spirometry monitoring (nose clip and mouthpiece) and better explains the dynamic coordination (function of time) between MSJ and breath. The feasibility of this measurement is a first step for further studies that will concentrate on the possible link between that joint and pathologies like scoliosis, asthma or COPD. This could also provide new focusses about the influence of manual therapies on breath functions.
Acknowledgments
Authors would like to thank Roger, Christophe and Olivier Caporossi, Serge Pin, Laurent Stubbe and Jeanine Sanchez, ESO – Paris and the University of Reims-Champagne-Ardennes management.
References
- Aliverti A, Dellacá R, Pelosi P, Chiumello D, Pedotti A, Gattinoni L. 2000. Opto-electronic plethysmography in intensive care patients. Am J Respir Crit Care Med. 161(5):1546–1552.
- Beyer B, Feipel V, Sholukha V, Chèze L, Van Sint Jan S. 2017. In-vivo analysis of sternal angle, sternal and sternocostal kinematics in supine humans during breathing. J Biomech. 64:32–40.
- Cala SJ, Kenyon CM, Ferrigno G, Carnevali P, Aliverti A, Pedotti A, Macklem PT, Rochester DF. 1996. Chest wall and lung volume estimation by optical reflectance motion analysis. J Appl Physiol. 81(6):2680–2689.
- Carrier G, Fréchette É, Ugalde P, Deslauriers J. 2007. Correlative anatomy for the sternum and ribs, costovertebral angle, chest wall muscles and intercostal spaces, thoracic outlet. Thorac Surg Clin. 17(4):521–528.
- Kaneko H, Horie J. 2012. Breathing movements of the chest and abdominal wall in healthy subjects. Respir Care. 57(9):1442–1451.
- Selthofer R, Nikoli V, Mrela T, Radi R, Lek I, Rude I, Selthofer K. 2006. Morphometric analysis of the sternum. Coll Antropol. 30(4):43–47.