
1. Introduction
An aneurysm of the ascending aorta (AsAA) can progressively evolve over years and can involve an aortic dissection and/or rupture. The surgical replacement of the aneurysmal portion by a prosthesis remains the adopted treatment. Currently, surgical recommendations are based on the maximum diameter of the ascending aorta (Erbel et al. Citation2014). It is well known that this factor is not reliable (Duprey et al. Citation2016). Understanding the biomechanical properties of the aorta could lead to develop biomechanical criteria, and then to be more accurate in predicting the development of aortic aneurysm. In this framework, the aim of this work is to study the local patient specific elastic modulus distribution of the AsAA from biaxial tensile test.
2. Methods
Pathologic ascending aortic tissue samples (n = 20) were obtained from patients undergoing elective surgical repair of AsAA. The samples were grouped by the type of valve (tricuspid aortic valve (TAV) and bicuspid aortic valve (BAV)) ().
Table 1. Patient characteristics.
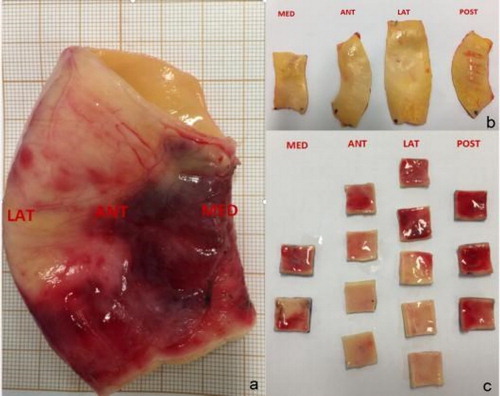
The biaxial tensile tests were performed within one hour of the resection of AsAA. All the aortic wall samples were partitioned related to medial (MED), posterior (POST), lateral (LAT), and anterior (ANT) quadrants (). Each AsAA sample was cut in square size (15 mm x 15 mm, n = 151) with marking the circumferential and longitudinal directions.
Figure 1. AsAA wall tissue. (a) Global human AsAA segment; (b) Sample pieces from each quadrant (intima view); (c) Subsequent processing for obtaining 15 mm x 15 mm specimens (adventitia view).
For each specimen, thickness was recorded at 5 locations in the tissue using a digimatic measuring machine (Litematic VL-50, Mitutoyo®) that provides a constant force thickness (±0.00001 mm). The average value of the measurements was used. The experiments were carried out by a biaxial tensile test machine (ElectroForce®). After being submerged in 32 °C spray of water, the specimens were subjected to a preconditioning protocol consisting five times of 5.5% displacement-controlled cycles. The stretch of the specimens were set up as a rate of 10 mm/min until rupture.
The maximum elastic modulus (EM) (Duprey et al. Citation2010) was obtained from each stress-strain curve of Young Modulus which is a parametre of stiffness.
3. Results and discussion
3.1. Result
The results of the EM related to different aortic regions are showed in .
Figure 2. (A)The Maximum Elastic Modulus for the longitudinal and circumferential directions for TAV (n = 103) and BAV (n = 48) samples for each quadrants. (B) The mean thickness of TAV (n = 103) and BAV (n = 48) for each quadrants.
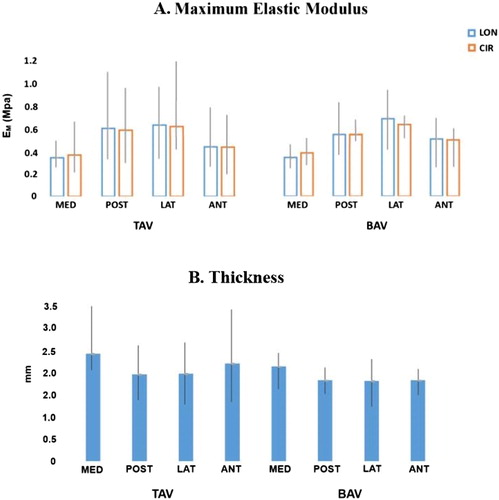
In general, the lateral quadrant (outer curvature) of the aorta shows a higher stiffness among all the four regions, roughly the double value of the medial quadrant (inner curvature). The longitudinal direction of the aorta allows more strain than the circumferential direction (TAV r = 0.8726, BAV r = 07159), except the medial quadrant showing the opposite result (TAV r = 0.0723, BAV r = 0.8854). There is no significant difference between tissue types in neither longitudinal (LON) nor circumferential (CIR) direction for the maximum elastic modulus (p = NS, t-test).
The thickness of TAV and BAV tissues did not show significant difference in the four regions of the AsAA wall ().
3.2. Discussion
It was expected to observe a regional variability in the thickness of the dilated samples corresponding to the change of mechanical properties caused by valve disease. However, among the ten AsAA tissues, there was no correlation between the regional thickness and mechanical properties (EM) of the expanded samples, neither TAV (r = -0.1527) nor BAV (r = -0.3001). Overall, in the ex-vivo study, the lateral of the aorta shows a higher stiffness. The longitudinal direction of the aorta is stiffer than the circumferential direction in the posterior, lateral, and anterior quadrants. On the contrary, in both TAV and BAV tissue types, the longitudinal direction of the medial quadrant shows the less stiffness.
Due to the limited number of AsAA samples, the mechanical properties and the thickness between the two valve types are not effectively emphasized. It is possible that these observations would be achieved with larger sample sizes. More patients will be included in the future study.
4. Conclusions
In this ex-vivo study we showed a local variability in the aortic stiffness for patients with AsAA without any link with local thickness.
Acknowledgements
We thank the association of “Bourgogne Coeur” for the financial support in the experiments.
References
- Choudhury N, Bouchot O, Rouleau L, Tremblay D, Cartier R, Butany J, Mongrain R, Leask R L. 2009. Local mechanical and structural properties of healthy and diseased human ascending aorta tissue. Cardiovasc Pathol. 18(2):83–91.
- Duprey A, Khanafer K, Schlicht M, Avril S, Williams D, Berguer R. 2010. In vitro characterisation of physiological and maximum elastic modulus of ascending thoracic aortic aneurysms using uniaxial tensile testing. Eur J Vas Endovas Surg. 39(6):700–707.
- Duprey A, Trabelsi O, Vola M, Favre J-P, Avril S. 2016. Biaxial rupture properties of ascending thoracic aortic aneurysms. Acta Biomater. 42:273–285.
- Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H, Evangelista A, Falk V, Frank H, Gaemperli O, et al. 2014. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J. 35(41):2873–2926.