
1. Introduction
Resuming activities of daily living after a lower limb amputation represents a challenge, especially because of the high risk of falling. Thus, rehabilitation initially focuses on stability. Despite its critical role in the rehabilitation, the clinical evaluation of stability is generally based on subjective assessments. Clinical scores, such as the two-minute walking test (2MWT), which measures the distance travelled by the patient in 2 minutes (Loiret et al. Citation2005), can be used to complement these subjective assessments but seem insufficient to assess stability during gait.
To overcome the lack of quantitative data, the instrumentation of clinical tests with wearable sensors, such as inertial measurement units (IMUs), was proposed (Bergamini et al. Citation2017). Stability – defined as step-to-step gait reproducibility and the capacity to minimize oscillations from the lower to upper levels of the body – can indeed be quantified using indices computed from upper body accelerations, like the improved harmonic ratio (Pasciuto et al. Citation2017) and attenuation coefficients (Paradisi et al. Citation2019). However, knowledge on these new indices and their use still need to be deepened.
The objective of this preliminary study is thus to explore the added value of quantifying these gait quality indices during 2MWT of people with transtibial amputation and to identify those that could be suitable for patients’ follow-up.
2. Methods
This study was granted ethical approval (CPP N°2018-A03477-48) and nine people with transtibial amputation who had completed their rehabilitation (1 female and 8 males and 1 female, age: 51.2 ± 10.5 years, mass: 78.6 ± 17.3 kg) gave their written informed consent prior to their participation. Participants were instrumented with three IMUs (MTw, Xsens, Netherlands, 100 s−1) located on the head at the occipital bone level, on the sternum and on the pelvis, at L3. Each participant then performed two successive 2MWT at their self-selected speed, starting from a standing static posture maintained for about 3 seconds.
Proper alignment of the IMUs with craniocaudal (CC), anteroposterior (AP), and mediolateral (ML) anatomical axes was ensured through a verticalization procedure during the initial static posture of each 2MWT (Bergamini et al. Citation2014). Only steady state strides were considered within each test, and two gait quality indices were computed for each stride.
The improved Harmonic Ratio (iHR) was computed for each of the 3 acceleration components measured at the pelvis level (Pasciuto et al. Citation2017); its computation is based on a spectral analysis of the acceleration and yields values between 0% (step-to-step asymmetry) and 100% (perfect step-to-step symmetry). The attenuation coefficients (AC) were computed between each level pair of the body (AC-PS, AC-PH, and AC-SH between pelvis/sternum, pelvis/head and sternum/head respectively), and for each acceleration component (Paradisi et al. Citation2019). Attenuation of the accelerations from lower to upper body levels yields positive coefficients, while amplification yield negative coefficients.
The medians and interquartile ranges of the twelve indices were computed over all strides for each 2MWT and each participant. The obtained values for the first 2MWT were used to describe the population. Then, the medians obtained at each repetition of the 2MWT were compared for each patient, so as to identify the most suitable indices for longitudinal follow-up.
A Shapiro-Wilk test was performed on the iHR and AC medians. According to the results of this test, paired t-tests or Wilcoxon signed-rank tests were used to identify indices with steady values across the 2MWT repetitions. The significance level was set to 0.05 for all statistical tests.
3. Results and discussion
3.1. Descriptive values for the studied population
provides the median iHR and AC achieved during the first 2MWT of all the participants (average of 71 strides per participant). A higher number of participants would be required to statistically characterize the population of transtibial amputees. However, the iHR values obtained are consistent with the literature, with values closer to those of asymptomatic population than people with transfemoral amputation (Pasciuto et al. Citation2017). Attenuations from pelvis to sternum in AP and ML directions were found to be prominent in transtibial amputees while amplifications of the accelerations were found from sternum to head, confirming results of the literature (Paradisi et al. Citation2019). Attenuations from pelvis to head were found to be lower in the current study, indicating a lower stability of the participants, which might be because some participants had only recently terminated their rehabilitation.
Table 1. Medians and interquartile ranges (IQR) of the median indices achieved during the first repetition of the 2MWT for each direction.
3.2. Identification of steady indices
For all of the twelve selected indices, no statistically significant difference was found between the repetitions of the 2MWT. An example is given in .
Figure 1. Comparison of the medians of AC-PS computed on the CC direction for the two 2MWT. Each point represents one participant. The line is the bisector.
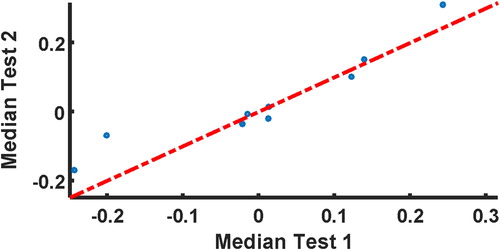
This seems to indicate (i) that a single repetition of the 2MWT is required to quantify stability using these indices, and (ii) that these indices are more suitable for the longitudinal follow-up of patients.
It should be noted that in some cases, there was no statistically significant difference detected due to high between-subjects variability. A higher number of participants is thus required to refine the statistics.
4. Conclusions
This preliminary study allowed to identify twelve indices quantifying stability that may be used for the longitudinal follow-up of patients with transtibial amputation during their rehabilitation. A higher number of patients is needed to confirm and refine these results, and to create a reference database for transtibial amputees. Future studies should focus on the repeatability of the indices in a between-session design, in order to determine the minimal detectable change by the selected indices. Eventually, a longitudinal study, from initial fitting of the prosthesis to rehabilitation discharge would allow to characterize stability evolution along the rehabilitation.
Acknowledgements
This study partly financed by the Fondation des Amputés de Guerre de France and the Université Franco-Italienne.
References
- Bergamini E, Ligorio G, Summa A, Vannozzi G, Cappozzo A, Sabatini AM. 2014. Estimating orientation using magnetic and inertial sensors and different sensor fusion approaches: Accuracy assessment in manual and locomotion tasks. Sensors (Basel)). 14(10):18625–18649.
- Bergamini E, Iosa M, Belluscio V, Morone G, Tramontano M, Vannozzi G. 2017. Multi-sensor assessment of dynamic balance during gait in patients with subacute stroke. J Biomech. 61:208–215.
- Loiret I, Paysant J, Martinet N, André J-M. 2005. Evaluation of amputees. Ann Readapt Med Phys. 48(6):307–316.
- Paradisi F, Di Stanislao E, Summa A, Brunelli S, Traballesi M, Vannozzi G. 2019. Upper body accelerations during level walking in transtibial amputees. Prosthet Orthot Int. 43(2):204–212.
- Pasciuto I, Bergamini E, Iosa M, Vannozzi G, Cappozzo A. 2017. Overcoming the limitations of the Harmonic Ratio for the reliable assessment of gait symmetry. J Biomech. 53:84–89.