
1. Introduction
With a prevalence of 4.87% in dogs, cranial cruciate ligament (LCC) rupture is the most common orthopedic involvement of the pelvic limbs (Witsberger et al. Citation2008). Repair techniques for these ruptures, using a synthetic intra-articular ligament, have limitations that are intrinsically linked to the materials used, which can influence the functionality of the in-situ system over time (Denny and Goodship 1980). A renewed interest has been initiated by the discovery of new medical grade fibers with interesting mechanical and biocompatible properties (such as UHMWPE fibers), that can be braided and used as a ligament reconstruction implant during rupture of the anterior cruciate ligament (ACL) in humans (Purchase et al. Citation2007). A gold standard for years, the interference screw is the preferred means of attachment associated with the use of these implants during ACL rupture. Numerous biomechanical studies carried out on human anatomical pieces have compared various axes and tunnel diameters in order to optimize these fixings (Aoki et al. 2019). The objective of this ex-vivo study will be to compare the biomechanical properties of two interference screw implantation techniques chosen as the fixation system for a synthetic UHMWPE implant used in the surgical treatment of LCC rupture in dogs.
2. Methods
2.1. Sample preparation protocol
Fourteen hindlimbs from 7 adult dogs 29 kg ± 2 kg (mean ± sd) were selected. Dogs were of similar size, without any stifle lesion observed and died from reasons unrelated to the focus of this study. Stifles were dissected to leave the tibia and femur intact. Each bone extremity was fixed with resin onto two supports.
2.2. Implantation of the UHMWPE ligament
Stifles were implanted with a UHMWPE ligament (Novalig®, Novetech Surgery, Monaco). An oblique tibial tunnel was drilled from the cranio-medial insertion of CCL. A femoral tunnel was drilled from the caudo-lateral femoral insertion. The ligament was passed through both tunnels ().
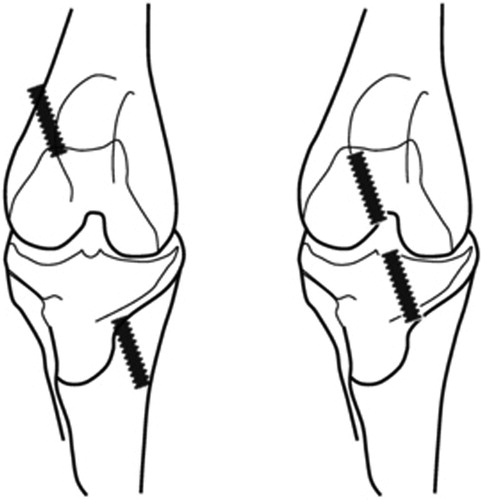
Figure 1. (a) Technique 1 “Out-In”: A first interference screw (diameter: 4.5 mm, 20 mm-long) was inserted from outside to inside the articulation from the distolateral femoral metaphysis. After straightening the ligament, a second interference screw was inserted from outside to inside the articulation from the proximo-medial tibia. (b) Technique 2 “In-Out”: This is the same technique as number one, but the interference screw was implanted from inside to outside the articulation from the intra articular space of the stifle towards the metaphysis of the proximal tibia and the distal femur.
2.3. Biomechanical testing
Static tensile tests of these two techniques were performed on the stifles using a traction system (AGS- X Shimadzu, Japan) with a pre-test of 20 mm/min traction until the load reached 10 N, thus straightening the system. The first static test consisted in a 1-mm/min traction until failure. Failure occurs if the displacement exceeds 15 mm. For the series of tests, the sampling rate for data acquisition was set at 10 Hz. A total of 14 experimental set-ups were randomly considered: 7 under the first surgical implantation technique and 7 under the second.
2.4. Data acquisition and processing
During tests, acquisitions of the data were carried out using the TrapeziumX software (Shimadzu, Japan). For each implantation technique, two measures were taken
The strength recorded at 3 mm (S3mm) of displacement of the cross traverse.
The maximum strength (Ms) and the displacement of the associated traverse stroke.
The mode of failure.
The data were then processed with Microsoft Excel. Statistical analyses were performed using non-parametric Mann-Whitney tests.
3. Results and discussion
No rupture of the set-up occurred. All the mechanical tests carried out reported a localized sliding exclusively in the tibial part. A measurement of the tensile strength was recorded at 3 mm displacement (S3mm). This displacement limit is equivalent to the acceptable limit of cranio-caudal amplitude of the movement of the tibia drawer, with respect to the post-operative controlled femur of an LCC reconstruction surgical technique (Loutzenheiser et al. Citation1995). The significant difference (S3mm) observed between the two implantation methods could be due to differences in bone density, depending on the implantation site of the interference screws. According to the theory of bone remodeling described by Wolff (1892), the interference screws implanted according to the "In-Out" technique are placed in the LCC insertion zone, which is thicker with denser sub-chondral bone in due to the much greater mechanical stresses borne by the articular surfaces. The essentially monocortical fixation of the interference screw implanted according to the "In-Out" technique is therefore carried out in the cortical and subchondral parts. These specific bone areas have better mechanical properties than the metaphyseal part, which is less exposed to mechanical stresses and seems to offer lower mechanical resistance when implanting the interference screws using the “Out-In” technique. In addition, the implantation of the interference screw according to the “In-Out” technique will act as wedge, owing to its conical shape, and limit the slip of the synthetic ligament more effectively while reducing the free part of the ligament in the intra-articular space. However, we know that the closer the fixation system is to the joint, the more solid the mounting (Scheffler et al. Citation2002; Bryan et al. Citation1996). Finally, a tensioning zone has been identified at the start of each of our mechanical tests. This displacement of the traverse stroke without linear increase in strength may be due to the tensioning of the fibers of the implant and a pre-tension of 10 N may not be sufficient and physiologically representative of the in-situ efforts of the implanted prosthesis when the dog is in a static position.
4. Conclusions
This study shows that in a synthetic ligamentoplasty assembly locked with two interference screws, those implanted “In-Out” allow better initial mechanical resistance (<3mm) of the LCC ligament reconstruction system than those implanted “Out- In”. The rupture mode is similar for the two implantation techniques, as a slip of the synthetic implant is observed between the walls of the tibial tunnel and the interference screw.
References
- Aoki A, Imade S, Uchio Y. 2019. Effect of the positional relationship between the interference screw and the tendon graft in the bone tunnel in ligament reconstruction. J Orthop Surg (Hong Kong). 27(1):2309499018822226.
- Bryan JM, Bach BR, Bush-Joseph CA, Fisher IM, Hsu KY. 1996. Comparison of “inside-out” and “outside-in” interference screw fixation for anterior cruciate ligament surgery in a bovine knee. Arthroscopy. 12(1):76–81.
- Denny HR, Goodship AE. 1980. Replacement of the anterior cruciate ligament with carbon fibre in the dog. J Small Anim Pract. 21(5):279–286.
- Loutzenheiser TD, Harryman DT, Yung S-W, France MP, Sidles JA. 1995. Optimizing arthroscopic knots. Arthroscopy. 11(2):199–206.
- Purchase R, Mason R, Hsu V, Rogers K, Gaughan JP, Torg J. 2007. Fourteen-year prospective results of a high-density polyethylene prosthetic anterior cruciate ligament reconstruction. J Long Term Eff Med Implant. 17(1):13–19.
- Scheffler SU, Südkamp NP, Göckenjan A, Hoffmann RFG, Weiler A. 2002. Biomechanical comparison of hamstring and patellar tendon graft anterior cruciate ligament reconstruction techniques: The impact of fixation level and fixation method under cyclic loading. Arthroscopy. 18(3):304–315.
- Witsberger TH, Armando Villamil J, Schultz LG, Hahn AW, Cook JL. 2008. Prevalence of and risk factors for hip dysplasia and cranial cruciate ligament deficiency in dogs. J Am Vet Med Assoc. 232 (12):1818–1824.
- Wolff J. 1892. Das gesetz der transformation der knochen. A Hirshwald. 1:1–152