
1. Introduction
Back pain and injuries are very prevalent in rhythmic gymnastics (Hutchinson Citation1999). The evaluation of the lumbar intervertebral stresses during the execution of rhythmic gymnastics movements could help identify which ones are the most likely leading to injuries. However, the recording of the spine kinematics during dynamic movements requires the use of linked-segment biomechanical model and is obtained through a multibody kinematics optimization (MKO) method. Several models are already available but none of them allow intervertebral motion in the thoracic spine. In the lumbar spine, different techniques are used to obtain the intervertebral motions, among which one is consisting in linearly constraining these intervertebral motions to the generalized coordinate representing the full lumbar lordosis (Christophy et al. Citation2012). However, the extreme range of motion of the spine during rhythmic gymnastics movements could be challenging when neglecting the thoracic spine intervertebral motion.
To investigate the potential contribution of the thoracic spine intervertebral motions, this study aimed at comparing the kinematics of the lumbar spine during rhythmic gymnastics movements with and without enabling the intervertebral thoracic spine motion.
2. Methods
2.1. Experimental data
Two rhythmic gymnasts (18 y/o, 165/169 cm, 60/63 kg), both competing at an international level, participated in this study. They were asked to perform the following rhythmic gymnastics movements: back and front walkovers (5 repetitions), rings with hand support (2), back splits without hand support (5), split leaps (3) and turning split leaps (5). Motion capture acquisitions were carried out using a 14-camera optoelectronic system. (Vicon system, hardware: Vero 1.3/2.2 cameras; Nexus 2 software; Oxford Metrics, UK) set at 200 Hz. The gymnasts were equipped with a total of 12 markers located around the pelvis, along the spine and on the thorax. Low dose biplanar radiographs in the EOS recommended standing upright posture were acquired (EOS system, EOS imaging, France) without removing the markers.
2.2. Musculoskeletal models
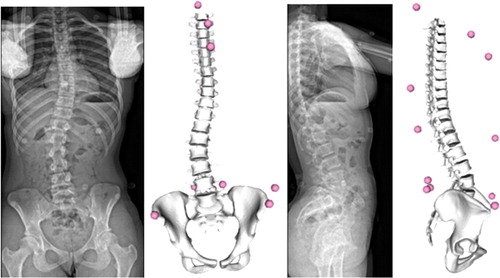
A personalised linked-segment model composed of the pelvis and the vertebrae from T1 to L5 was created based on the 3D reconstruction of the bones from the biplanar radiographs. Joints connecting the vertebrae were modelled as custom joints with six degrees of freedom (DoF). The reconstructed geometries were also used to determine the intervertebral joint centres, located at the centroid of the intervertebral discs (Bruno et al. Citation2015). A subject-specific spine curvature in neutral position () was obtained from the personalised joint centres and geometries formed. In addition, the reflective markers were also reconstructed on the same biplanar images which allowed for the personalisation of the marker positions in the model. The markers were linked to their closest body, except for those on the rib cage which were linked to T1.
Figure 1. Biplanar radiographs and personalised OpenSim model for subject 2.
Intervertebral joint motion on the lumbar spine was constrained to the full lumbar lordosis generalized coordinate, based on previous published work (Christophy et al. Citation2012). Extending this work to the thoracic bodies, linear constraints were added to the intervertebral thoracic joints in order to reduce the thoracic spine to a 3-DoF system driven by a thoracic kyphosis generalized coordinate. Constraints were adapted from (Gaume et al. Citation2020). This fully articulated spine model (FASM) was then duplicated and the thoracic mobility of the duplicated model was locked, resulting in a model close to (Christophy et al. Citation2012), but with subject-specific spine curvature. This second model will be referred to as the locked thoracic spine model (LTSM).
2.3. Data processing
Motion capture data were processed in parallel with the two models. Joint kinematics were computed by an inverse kinematics algorithm implemented in the OpenSim software. The comparison covered the lumbar lordosis, which was directly given by the generalized coordinate related to the lumbar spine, and the root mean squared error (RMSE) of the reconstructed markers with respect to their real coordinates in the motion capture reference frame. For each movement, RMSE was calculated for the 5 markers around the pelvis, the 7 markers across the torso and the whole marker set.
3. Results and discussion
Differences in the RMSE computed for both models are summarized in . For each subject, overall RMSE improved by 7.2 ± 1.8 mm for subject 1 and 2.5 ± 1.7 mm for subject 2 when running the MKO with the FASM.
Table 1. RMSE difference (LTSM minus FASM) for both subjects, averaged over the 22 movements.
More specifically, RMSE of the pelvis markers was improved by 3.4 mm and 1.8 mm, for subject 1 and subject 2, respectively, when allowing for mobility in the thoracic spine. Regarding RMSE of torso markers, a more important improvement of 10 mm and 4.5 mm was found for S1 and S2, respectively
Regarding the lumbar spine, the FASM resulted in smaller lumbar lordosis during the movements than the LTSM (differences of −10.4°±3 and −6.6°±4.3 for subject 1 and subject 2, respectively). This can be explained by the addition of 3 DoF in the FASM compared to the LTSM. Indeed, during the MKO with the FASM, the generalized coordinate of the lumbar lordosis mainly optimized the position of the markers on the lumbar spine, while thoracic kyphosis generalized coordinate rectified the position of the markers above. The movement for which thoracic mobility had the most impact on lumbar lordosis were rings with hand support for both subjects (-16° and −14° of flexion for subject 1 and subject 2, respectively).
Without any restriction on the range of motion of the lumbar kyphosis, its average amplitude was of 29° for subject 1 and 26° for subject 2, which is coherent with literature data (Morita et al. Citation2014). However, during back and front walkovers, this amplitude reached unphysiological values of 60.4° and 74.4° for S1 and S2, respectively.
4. Conclusions
This study showed the impact of thoracic mobility in musculoskeletal models on the spine kinematics. As expected, allowing movements along the thoracic spine led to a better overall RMSE. The resulting lumbar spine kinematics was also noticeably impacted, and a systematic reduction of the computed lordosis was found. Further research will focus on the validity of the predicted lumbar and thoracic motions with the fully articulated spine model.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
References
- Bruno AG, Bouxsein ML, Anderson DE. 2015. Development and validation of a musculoskeletal model of the fully articulated thoracolumbar spine and rib cage. J Biomech Eng. 137(8):81003.
- Christophy M, Faruk Senan NA, Lotz JC, O'Reilly OM. 2012. A musculoskeletal model for the lumbar spine. Biomech Model Mechanobiol. 11(1-2):19–34.
- Gaume M, Persohn S, Vergari C, Glorion C, Skalli W, Miladi L. 2020. Biomechanical cadaver study of proximal fixation in a minimally invasive bipolar construct. Spine Deform. 8(1):33–38.
- Hutchinson MR. 1999. Low back pain in elite rhythmic gymnasts. Med Sci Sports Exerc. 31(11):1686–1688.
- Morita D, Yukawa Y, Nakashima H, Ito K, Yoshida G, Machino M, Kanbara S, Iwase T, Kato F. 2014. Range of motion of thoracic spine in sagittal plane. Eur Spine J. 23(3):673–678.