
1. Introduction
Cerebral palsy (CP) is a neurological disease due to brain damage and it is the leading cause of pathological gaits in childhood. The Gross Motor Function Classification System (GMFCS) is commonly used to classify the degree of motor impairments (5 levels) together with their anatomical distribution (unilateral or bilateral CP) and type (spastic, ataxic or dyskinetic CP) (Rosenbaum Citation2003). Comorbidities like intellectual, visual and hearing disabilities usually co-exist with CP (De-Luca et al. Citation2012).
Several authors already studied the effects of the CP on the kinematics and the dynamics parameters of the musculo-skeletal system during gait. The GMFCS was demonstrated to be highly correlated with the profile and the authors always observed a decrease in the Range of Motion (ROM) of the joints compared to healthy subjects. This abnormal pattern locomotion could lead to increase energy consumption, gait instability and fatigue (Eek et al. Citation2017).
With the final aim of building an exoskeleton for rehabilitation purposes, we present for the first time a kinematic comparison of 2 true twins, one healthy and one with a cerebral palsy diagnosis to better understand the corrections which must be applied to recover a healthy gait. Our hypothesis is that the healthy child is the reference to be mimic by the CP child.
2. Methods
2.1. Subjects
Two true twin sisters were recruited for this study (age: 7 years old). The first one (H - size: 1.20 m - mass: 20 kg) is healthy and the second one (C - size: 1.05 m - mass: 17.6 kg) has spastic CP. The GMFCS is level II and C is able to walk independently with aid and can activate the ankle plantar flexors. She had dorsal selective rhizotomy and tendon lengthening surgery in the past 12 months at the knee and ankle and botulin toxin type A injections in the past 6 months.
The study was conducted in accordance with the declaration of Helsinki and was approved by the University of Toulouse ethical committee. The parents of the children signed and inform consent before the experiments.
2.2. Experimental setup
A motion capture system consisting of 13 cameras was used to register the position of a whole-body marker set of 48 markers placed on anatomical landmarks (Wu et al. Citation2002, Citation2005). The marker positions were sampled at 200 HZ and filtered with a 4-th order low-pass butterworth filter at 10 HZ. Twelve gait cycles for each side were analyzed for H and C. C held herself up with the right or left hand during the experiments.
2.3. Data reduction and analysis
The whole-body musculo-skeletal model in Maldonado et al. (Citation2018) was scaled with the Opensim software, using custom specification of the marker pairs, to obtain one model for each child. A maximum marker error (MME) around 2 cm were used to judge the quality of the scaling. The inverse kinematic process was performed in Opensim using custom marker weights, and only the gait cycles with less than 3 cm of MME were considered. The joint rotations of the lower limbs were computed at the hip (3D), the knee (1D) and the ankle (2D), according to ISB recommendations (Wu et al. Citation2002, Citation2005).
Significance of the parameters was assessed using t-tests with significance level of 0.05.
3. Results and discussion
summarizes the spatiotemporal parameters. There are significant differences in almost all of them between C and H. C has slower motion which is clearly evident by looking at the mean time (T), Double Support (DS) and Single Support (SS) phases. Here left DS is the DS before left SS, the opposite holds for the right DS. C walks with a larger DS phase compare to H to decrease her instability, while reducing the SS phase as well. The left DS phase is clearly shorter than the right one for both twins. The left swing phase (right SS%) of C lasts less than the right one because the left side is more affected by the spasticity as confirmed by medical observations. The stride length (SL) of C is shorter (28 cm less), and the CoM velocity (v) is slower also (almost half the one of H).
Table 1. Spatiotemporal parameters. *p > 0.05.
In the and , the hip flexion-extension and ankle dorsiflexion profiles were compared for H and C. The start of the swing phase is represented by the vertical line: the red one for H, the blue one for C.
Figure 1. Left hip flexion-extension.
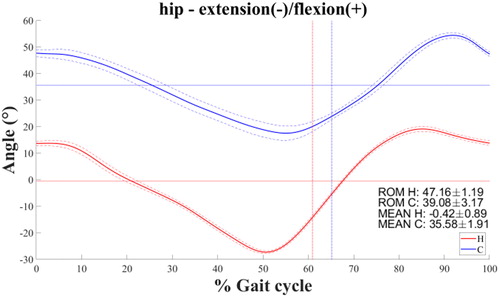
Figure 2. Right ankle planta-dorsiflexion.
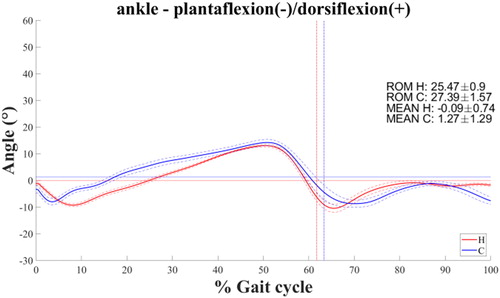
C has a typical crouch gait characterized by excessive hip and knee flexion and ankle dorsiflexion, especially in the stance phase. The hip orientation is expressed w.r.t. the pelvis and the anterior pelvis tilt of C was around 20° more than the one of H. Hip and knee flexions of C are stiffer (H-C – average ROM: 8.74°). The overall left side pattern of C is more flexed and tauter than the right one. This leads to left hip abduction more pronounced (H – average: 1.8° vs. C – average: 8.3°) together with compensatory motions at the trunk and pelvis like the higher clockwise rotation of the pelvis. The left ankle dorsiflexion of C is farther apart from the one of H compare to the right side (left |H-C| – average: 10.9° vs. right |H-C| – average: 1.4°).
The right hip adduction and internal rotation behaviour of C in the stance phase can be influenced by the higher right ankle eversion that pushes the leg inward. Moreover, both twins walk with eversion for almost the entire gait cycle. The hip, knee, and ankle angles of C resembles the one of H, but they are shifted and delayed.
Finally, the results showed that the angles patterns of C have higher standard deviations than the ones of H (H – average std: 0.96 vs C – average std: 1.54) because of the larger gait variability of C.
4. Conclusions
We investigated the kinematics of 2 twins of 7 years with the aim of further understand the gait pattern deviations that the cerebral palsy cause and start building one of the main pipelines for the design and evaluation of a lower limb exoskeleton. Significant spatiotemporal differences were observed. Except the right ankle plantarflexion and the left hip rotation, the joints kinematics were significantly far apart between both children. Indeed, the CP has a complex effect on the entire musculoskeletal system as previously observed (Armand et al. Citation2016). While this case study cannot be generalized, it can give us useful insights about the necessary gait corrections and controls to pursue with the realization of an adapted and personalized rehabilitation exoskeleton for C.
Additional information
Funding
References
- Armand S, Decoulon G, Bonnefoy-Mazure A. 2016. Gait analysis in children with cerebral palsy. EFORT Open Rev. 1(12):448–446.
- De-Luca MA, Ledbetter DH, Martin CL. 2012. Genetic insights into the causes and classification of the cerebral palsies. Lancet Neurol. 11:283–292.
- Eek MN, Zügner R, Stefansdottir I, Tranberg R. 2017. Kinematic gait pattern in children with cerebral palsy and leg length discrepancy: effects of an extra sole. Gait Posture. 55:150–156.
- Maldonado G, Soueres P, Watier B. 2018. Strategies of Parkour practitioners for executing soft precision landings. J Sports Sci. 36(22):2551–2557.
- Rosenbaum P. 2003. Cerebral palsy: what parents and doctors want to know. BMJ. 326(7396):970–974.
- Wu G, Siegler S, Allard P, Kirtley C, Leardini A, Rosenbaum D, Whittle M, D’Lima DD, Cristofolini L, Witte H, et al. 2002. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: ankle, hip, and spine. J Biomech. 35(4):543–548.
- Wu G, van der Helm FCT, Veeger HEJD, Makhsous M, Van Roy P, Anglin C, Nagels J, Karduna AR, McQuade K, Wang X, et al. 2005. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: shoulder, elbow, wrist and hand. J Biomech. 38(5):981–992.